










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Surgery
versión On-line ISSN 2078-5151
versión impresa ISSN 0038-2361
S. Afr. j. surg. vol.51 no.4 Cape Town ene. 2013
CASE REPORT
Salmonella thyroiditis: A case report and review of the literature
A Maraj; A Kiss; T E Luvhengo
Department of General Surgery, Chris Hani Baragwanath Academic Hospital and University of Witwatersrand, Johannesburg, South Africa
ABSTRACT
Thyroid abscesses are rare, and Staphylococcus aureus is the main causative organism. Abscesses caused by other organisms are even rarer. This report describes a case of Salmonella thyroiditis in an HIV-positive patient. Fine-needle aspiration cytology was performed and Salmonella sp. were cultured. The patient was successfully treated with antibiotics and incision and drainage.
Thyroid abscesses caused by Salmonella are rare. The main causative organism is usually Staphylococcus aureus.[1] HIV infection has reached epidemic proportions in South Africa.[2] Patients with HIV may present with rare conditions such as cytomegalovirus intestinal perforations[3] or upper gastrointestinal tract bleeding secondary to Kaposi's sarcoma.[4]Salmonella infection typically involves the hepatobiliary system, bones, joints and soft tissue. Infection of the thyroid gland is rare, and when it occurs in immunocompromised patients it is associated with high mortality.[1] We present a case of Salmonella thyroiditis in an HIVpositive patient who was successfully treated with antibiotics and incision and drainage. Such rare conditions should be considered when managing HIV-positive patients.
The reasons why infective thyroiditis is rare include the following: (i) thyroid colloid material contains antibacterial properties; (ii) the thyroid gland receives a high blood flow; (iii) storage of excess iodine in the thryroid is protective against infections; (iv) in hyperthyroid states, phagocytes have an increased physiological ability to destroy bacteria; and (v) thyroid hormones have antibacterial roles.[5,6]
Case report
A 48-year-old HIV-positive woman on highly active antiretroviral therapy (HAART) presented with a 1-year history of an anterior neck mass that had increased markedly in size over the preceding 3 months. She also complained of pain, palpitations, sweating and loss of weight. She had compressive symptoms as evidenced by difficulty in breathing and dysphagia, and her voice was hoarse.
On examination she had a normal heart rate and was apyrexial. There was a 12.2 cm x 11.7 cm x 11 cm anterior mass on the left side of her neck (Fig. 1). The mass moved up on swallowing. It was tender, smooth, well defined and fluctuant, and there was retrosternal extension. The trachea was deviated to the right and there were palpable submental and cervical lymph nodes. The right side was normal. All results of blood tests were normal except for a C-reactive protein level of 60 mg/l and a haemoglobin concentration of 7.5 g/l.

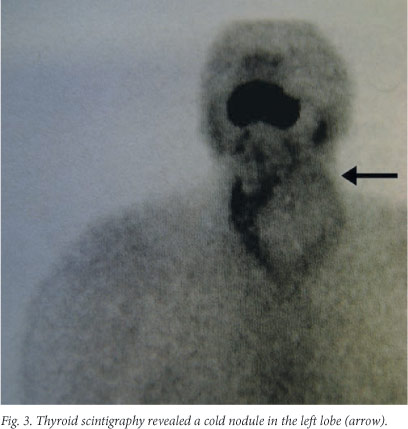
Tracheal deviation and retrosternal extension were confirmed on the chest radiograph (Fig. 2). Findings on ultrasound examination suggested a thyroid abscess. A computed tomography scan of the neck revealed a complex mass arising from the left thyroid lobe with compression of the surrounding structures but no infiltration of the vessels. There were multiple submental and posterior cervical lymph nodes. Thyroid scintigraphy revealed a cold nodule in the left lobe (Fig. 3).

Fine-needle aspiration cytology (FNAC) performed under ultrasound guidance was diagnostic of infection by Salmonella sp. and negative for acid-fast bacilli. The organism was sensitive to cefotaxime, ceftriaxone and ciprofloxacin. Incision and drainage was done, and a tissue sample sent for microscopy and blood culture confirmed a Salmonella infection sensitive to cefotaxime, ceftriaxone and ciprofloxacin. The culture was also negative for acid-fast bacilli and therefore confirmed the FNAC results. The patient was treated with 1 g ceftriaxone intravenously twice daily for 2 weeks. Repeat FNAC a month later was negative.
Discussion
Thyroid abscesses account for 0.1% of all diseases of the thyroid gland.[1] Factors predisposing to thyroid abscesses include immunosuppressive states such as HIV infection or diabetes.[1] Our patient was HIV-positive and in an advanced stage of the disease, with a CD4+ count of 67 cells/|il despite being on HAART.
S. aureus is the main organism causing thyroid abscesses.[1] However, the abscess in our patient was caused by a Salmonella sp. infection. Various serotypes of Salmonella have been implicated, as follows: Salmonella enteritidis,[1,7] S. typhimurium,[1,8] S. choleraesuis,[1] S. paratyphi A[1] and S. brandenburg.[1]
Before 2003 only 14 cases of Salmonella thyroiditis had been reported worldwide.[1] Sporadic cases have been reported since then. Although the majority of patients present with a history of diarrhoea,[8] our patient did not include this in her history.
Fever and neck swelling and tenderness are reported as the most common symptoms of Salmonella thyroiditis.[1,7,8] Other symptoms may be due to hypothyroidism or hyperthyroidism.[7] Compressive symptoms may also be present, suggesting a malignant lesion of the thyroid gland.[9] Our patient had difficulty in breathing, stridor, hoarseness and dysphagia and was euthyroid. The findings necessitated FNAC, which was diagnostic of a Salmonella sp. infection. In an earlier report, Igler and colleagues also relied on FNAC to diagnose Salmonella infection.[7] However, we proceeded to perform incision and drainage because our patient was acutely symptomatic and needed relief of her compressive symptoms.
Conclusion
Although thyroid abscesses are rare, they need to be considered when an HIV-positive patient presents with a painful anterior neck mass. As these patients may have features suggestive of thyroid malignancy, FNAC should be done. The mainstays of treatment for Salmonella thyroid abscess are antibiotics and incision and drainage.
REFERENCES
1. Wasana S. Thyroid abscess caused by Salmonella group C infection. Chiang Mai Medical Bulletin 2003;42(3):113-119. [ Links ]
2. Connolly C, Shisana O, Colvin M, Stoker D. Epidemiology of HIV in South Africa - results of a national, community-based survey. S Afr Med J 2004; 4(11):776-781. [http://dx.doi.org/10.1186/1476-072X-10-61] [ Links ]
3. Braun J, Schumpelick V. Surgical problems in AIDS. Zentralbl Chir 1990;115(2):65-76. [ Links ]
4. Lew EA, Dieterich DT. Severe hemorrhage caused by gastrointestinal Kaposi's syndrome in patients with acquired immunodeficiency syndrome: Treatment with endoscopic injection sclerotherapy. Am J Gastroenterol 1992;87(10):1471-1474. [ Links ]
5. Khan EM, Haque I, Pandey R, et al. Tuberculosis of the thyroid gland: A clinicopathological profile of four cases and review of the literature. Aust N Z J Surg 1993;63(10):807-810. [ Links ]
6. Bulbuloglu E, Ciralik H, Okur E, Özdemir G, Ezberci F, Cetinkaya A. Tuberculosis of the thyroid gland: Review of the literature. World J Surg 2006;30(2):149-155. [http://dx.doi.org/10.1007/s00268-005-0139-1] [ Links ]
7. Igler C, Zahn T, Muller D. Thyroid abscess caused by Salmonella enteritidis. Dtsch Med Wochenschr 1991;116(18):695-698. [ Links ]
8. Gudipati S, Westblom TU. Salmonellosis initially seen as a thyroid abscess. Head Neck 1991;13(2):153-155. [http://dx.doi.org/10.1002/hed.2880130212] [ Links ]
9. Lala AK, Perakath B, Nair A, Lalitha MK. Salmonella thyroid abscess mimicking thyroid carcinoma. Indian Journal of Otolaryngology and Head and Neck Surgery 1996;48(4):337-338. [http://dx.doi.org/10.1007/BF03048678] [ Links ]
 Correspondence:
Correspondence:
T E Luvhengo
(thifhelimbilu.luvhengo@wits.ac.za)

