










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.51 no.3 Cape Town Jan. 2013
TRAUMA
Firearm injuries to children in Cape Town, South Africa: Impact of the 2004 Firearms Control Act
N M CampbellI; J G ColvilleI; Y van der HeydeII; A B van AsIII
IMBBS, MRes, Trauma Department, Red Cross War Memorial Children's Hospital, Cape Town, South Africa
IIMB ChB, MMed, Trauma Department, Red Cross War Memorial Children's Hospital, Cape Town, South Africa
IIIMB ChB, FCS, MMEd, MBA, PhD, Trauma Department, Red Cross War Memorial Children's Hospital, Cape Town, South Africa
ABSTRACT
BACKGROUND: Before the introduction of the Firearms Control Act in 2004, the epidemiology of childhood firearm injuries from 1991 to 2001 in Cape Town, South Africa, was reported. This study analyses current data as a comparator to assess the impact of the Act.
METHODS: Firearm injuries seen at Red Cross War Memorial Children's Hospital, Cape Town, from 2001 to 2010 were retrospectively reviewed. Data recorded included the patients' folder numbers, gender, date of birth, age, date of presentation, date discharged and inpatient stay, firearm type, number of shots, circumstances, injury sites, injury type, treatment, resulting morbidities and survival. These data were compared with the 1991 - 2001 data.
RESULTS: One hundred and sixty-three children presented with firearm injuries during this period. The results showed a decrease in incidence from 2001 to 2010. Older children and males had a higher incidence than younger children and females. Most injuries were to an extremity and were unintentional. Mortality had reduced significantly from the previous study (6% to 2.6%), as did the total number of inpatient days (1 063 to 617).
CONCLUSIONS: Compared with the earlier study, this study showed a significant reduction in the number of children presenting with a firearm-related injury. Mortality and inpatient stay were also significantly reduced. The study shows the impact that the Firearms Control Act has had in terms of paediatric firearm-related injury and provides evidence that the medical profession can play an important role in reducing violence.
Violence and firearms are common features of South African society. The leading causes of death in this country are violence and homicide. Firearms are the leading external cause of non-natural deaths[1,2] and claimed approximately 15 000 lives in 2005.[3] Regrettably children are still being caught up in this epidemic, which is not unique to South Africa. In the USA, over a 10-year period between 1999 and 2010, one study identified 198 firearm injuries to children, with the majority being attributed to accidental causes.[4] It is clear that there is a link between availability of firearms and injuries to children, and that the only way of reducing these injuries is prevention through legislation.[5] In 2004 South Africa introduced legislation in the form of the Firearms Control Act (FCA).[6] The FCA made it more difficult to obtain a firearm, but in recent years the legislation has been coming under fire from opposition groups calling for its removal.
Research has previously been carried out into the epidemiology of firearm injuries in South Africa. A retrospective study from Red Cross War Memorial Children's Hospital (RXH), Cape Town, in 2004 looked at firearm injuries to children in the decade 1991 - 2001.[7] The study showed an annual increase in the number of firearm injuries to children throughout that period, highlighting an increasing problem. It concluded that reducing the availability of firearms could have a significant impact on the reduction of firearm injuries in children, and was to prove useful in supporting efforts to strengthen South Africa's national gun laws. The purpose of the present study (January 2001 - January 2011) was to identify the epidemiology of firearm injuries in children and review the clinical details of their presentation, treatment and outcomes. We then assessed the effect of the 2004 FCA by comparing the findings with those of the earlier study.
Methods
RXH provides secondary care for the local population and tertiary services for all hospitals in the Western Cape region (population 4.5 million), and has the only independent level 1 paediatric trauma unit in South Africa. The hospital provides services for children up to 12 years of age.
The Child Accident Prevention Foundation of Southern Africa (CAPFSA) was established in 1987, with the aim of preventing death and injury in South African children through research and lobbying. Since 1991, CAPFSA has kept a database of all patients seen at the RXH Trauma Unit. The database includes demographic information along with details of the cause of injury, age at injury, Injury Severity Score and outcome.
The CAPFSA database was used by two trained researchers to search for and retrieve data for all presentations coded as firearm injuries for the study period January 2001 - January 2011. Data recorded included the patients' names, hospital folder numbers, gender, date of birth, age at presentation, date of presentation, date discharged and total stay in hospital, admission details, type of firearm, number of shots received, circumstances of injury, injury sites, type of injury, surgical interventions, resulting morbidities and survival. To achieve continuity the collected data were then analysed in the same form as the initial paper, using a Microsoft Excel database, with simple analyses of means, ranges and percentages. In addition, data from the same period on the number of unnatural deaths in the population under 13 years of age were gathered from the University of Cape Town's Department of Forensic Medicine (Salt River Mortuary).
This retrospective review of a pros-pectively maintained database was analysed in a similar way to the retrospective database data reported in 2004.[7]
Results
Between 2001 and 2011, 163 children presented to the RXH Trauma Unit after being injured by a firearm. Data on age, gender and date of attendance were available for all 163 children; 16 had incomplete information regarding certain other aspects of their data.
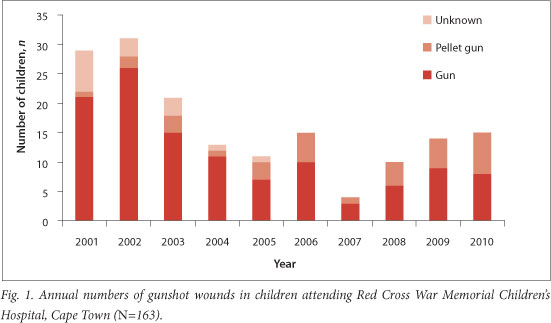
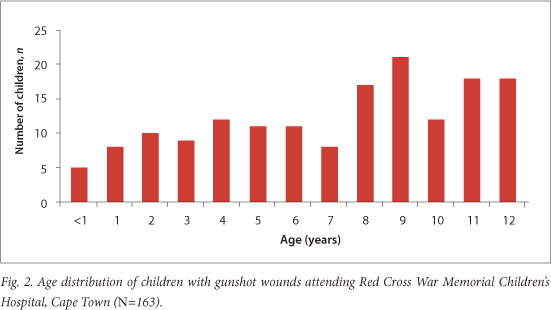
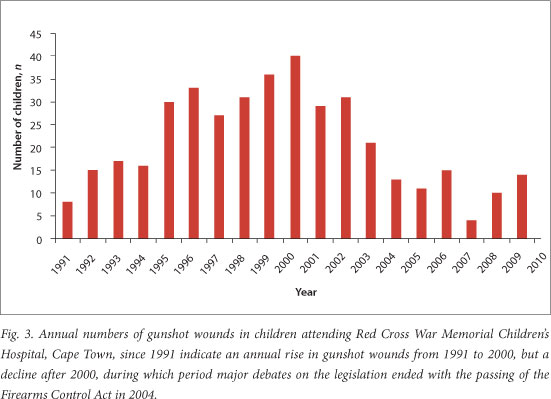
Fig. 1 shows annual attendances of patients with firearm injuries over the study period. It also distinguishes between the types of firearm used, i.e. gun or pellet gun. Fig. 2 illustrates the age distribution of the 163 children. The mean age was 7 years and 8 months. Fig. 3 shows the annual numbers of gunshot wounds in children attending RXH since 1991, indicating a rise in the number of children with gunshot injuries treated from 1991 to 2000 and a decline from 2001 to 2010.
Demographics
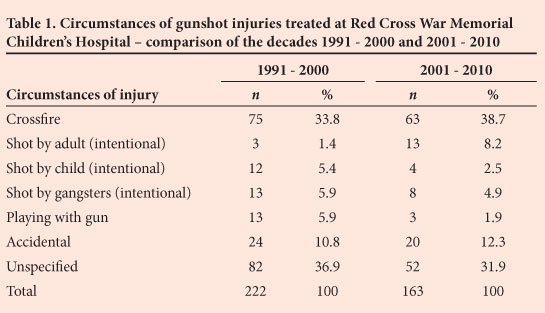
Sixty-one per cent of the children were male. The circumstances surrounding the firearm injuries for all children are shown in Table 1. The commonest circumstance was being caught in crossfire.
Injury patterns
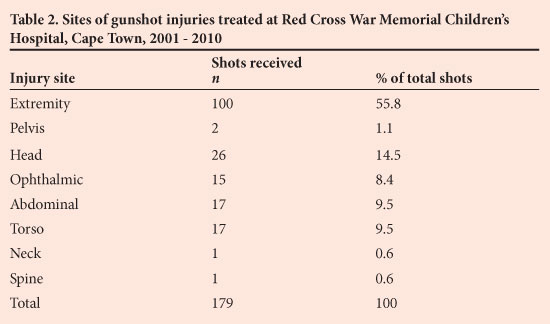
One hundred and forty-seven children were injured by 179 shots, of which 32 were from a pellet gun. One hundred and twenty-nine were shot once, 12 twice, 4 three times and 3 more than three times. The distribution of site of injury is shown in Table 2. Fifty-six per cent of injuries were to an extremity. Twenty-five of the 100 shots to an extremity resulted in an associated fracture. All the eye injuries were from a pellet gun. Of the 26 shots to the head, 12 were to the face, 5 were to the scalp and 8 were intracranial. One location on the head was unknown. The 26 shots to the head resulted in 14 isolated soft- tissue injuries and 11 soft-tissue injuries with fractures.
Outcome
Admission data were available for 147 children in the study group. Forty-seven were sent home without admission, 81 were admitted to the Trauma Unit, 15 were admitted to the Intensive Care Unit (ICU), and 3 died before being admitted. One child was transferred to another hospital on arrival.
Surgical procedures
Forty-seven patients (32.0% of 147) required a surgical procedure: 31 of these involved debridement of the wound, 7 patients had a laparotomy, and 18 procedures involved removal of a bullet. The majority of the procedures took place under local anaesthesia. Other procedures performed included 2 craniotomies, 8 bowel repairs and 2 plastic surgery reconstructions.
Hospital and ICU stay
Fifteen children were admitted to the ICU. Five had been shot in the abdomen, 5 in the head, 2 in the torso, 2 in an extremity and 1 in the spine.
Firearm victims took up a total of 617 inpatient days in hospital as a direct result of their injury. Shots to the abdomen accounted for 169 days, shots to an extremity for 130 days, shots to the head for 143 days, ophthalmic injuries for 11 days, pelvic injuries for 11 days, spinal injuries for 104 days, and shots to the torso for 49 days.
Morbidity
Only one of the 15 patients with ophthalmic injuries had reduced visual acuity.
This was the only morbidity resulting from a pellet gun injury. Four patients sustained peripheral nerve injuries: 1 brachial plexus injury, 1 ulnar nerve palsy, 1 radial nerve palsy and 1 perineal nerve palsy. One patient suffered from cranial nerve palsy. One patient developed a small-bowel obstruction requiring surgical intervention. Four patients suffered severe long-term physical effects of their injury: 1 became paraplegic following a gunshot to the cervical spine, 2 had widespread brain damage due to intracranial injuries, and another with intracranial injury became hemiplegic and died 2 years later from pneumonia.
Deaths
There were 3 hospital deaths. Two patients died after gunshots to the head and 1 from exsanguinating haemorrhage after an injury to the femoral artery in the thigh.
Mortuary data
The data set for the study period was completed from information gathered at the Department of Forensic Medicine (Salt River Mortuary) on numbers of unnatural deaths in children under 13 years of age. A total of 3 034 children died during this period, 33 as a result of gunshot-related injuries. Of the children who died of a gunshot wound, 30 died before they could reach hospital. Of these 30, 19 had an isolated gunshot wound to the head, 7 a single gunshot to the chest, and 1 a single gunshot to the abdomen. Three children died after multiple gunshots. A total of 193 children children were shot during the study period (163 admissions to hospital and 30 to the mortuary).
Discussion
The 1991 - 2001 study highlighted numerous determinants of gunshot wounds in children. This study, and numerous others, show that countries with permissive attitudes to gun control have higher rates of paediatric injuries and deaths due to firearms than countries with stricter legislation.[5,8,9] In a recent study in the USA, children aged 5 - 14 years of age living in states with high levels of gun ownership were 16 times more likely to die from unintentional firearm injury than children living in states with low levels of gun ownership.[8] Since the earlier Cape
Town study, and as a result of significant mobilisation of civil society via the 'anti-gun lobby', the South African government's stance on firearms has become stricter, with the aim of reducing firearm-related injuries and deaths. The FCA makes it much more difficult for civilians to acquire a gun. This seems to have had the intended effect of reducing the number of firearms in the general population. One of the aims of our present study was to analyse the impact this legislation has had on paediatric firearm-related injuries.
The earlier Cape Town study[7] showed an increase in the rate of firearm injuries in children over the decade, the figure peaking in the year 2000. Our study shows a decline in total firearm injuries in children from 2001, coinciding with changes in government opinion after 2000 and the legislation introduced in 2004 and demonstrating that strengthening firearm legislation can reduce firearm-related injury. Research in the US supports this conclusion, showing that unintentional firearm-related deaths among children have fallen steadily in that country due to stricter child access prevention laws.[9]
We also found that the proportion of firearm injuries caused by guns as opposed to pellet guns decreased significantly over the 10-year study period, as shown in Fig. 1, although the number of injuries caused by pellet guns remained fairly constant. For example, 7 of the 15 wounds in children attending RXH in 2010 were inflicted by pellet guns, as opposed to 1 out of 29 in 2001. The firearm legislation introduced does not affect ease of acquiring a pellet gun, so numbers of injuries caused by pellet guns would be expected to remain fairly constant, with injuries from guns decreasing as a result of the legislation. The previous study did not distinguish between guns and pellet guns, but this distinction is important because type of firearm affects prognosis. No deaths in our series were caused by pellet guns, and only one pellet gun injury resulted in long-term morbidity (loss of visual acuity after an ophthalmic injury).
Fig. 3 shows the number of gunshot wounds in children presenting to RXH from the start of the initial study in 1991 to the end of the present study in 2010. There has been a decrease in incidence after the changes in government opinion in 2000 and the introduction of the FCA in 2004.
The majority of children injured by firearms were males, caught in crossfire close to their own homes. This correlates with the findings of the earlier study. Fig. 2 shows an increase in the incidence of firearm injury with increasing age. The previous study[7] and others[4,5,10] concluded that the majority of children suffered unintentional injury (caught in crossfire, hurt when playing with a gun, accidental shots). It was suggested that the fact that the majority of injuries were unintentional demonstrates that ease of access to guns made a major contribution to the incidence of gunshot wounds in children.
Numerous studies have suggested that the older children are, the more likely they are to be injured by a firearm, with the vast majority of gunshot wounds occurring in the age group 13 - 19 years.[11,12] As our study had a cut-off age of 12, we were limited with regard to this comparison; however, we did find an increase in incidence with age. Studies done before the introduction of the legislation showed an increasing number of gunshot wounds among children younger than 13 years.[11,12] This could have been due to an increase in the incidence of accidental injuries or an increase in the number of children being caught in crossfire.
Lack of information or conflicting information in the patient's history often made it difficult to gather complete data on the circumstances of the shooting. However, our results suggest that the majority of children injured by firearms were caught in crossfire; accidental shootings also made a large contribution. The fact that the majority of children sustained only one gunshot wound supports data suggesting that most were shot unintentionally.
The majority of shots were received to an extremity, corresponding with findings from the previous study and other studies.[7,13] Twenty-five per cent of gunshot wounds to an extremity resulted in an associated fracture, compared with 39% in the previous 10 years. There were no vascular injuries associated with these fractures. Over the more recent 10-year period, no children with gunshot wounds in an extremity developed a localised skin infection.
Forty-seven patients (32.0%) required a surgical procedure, compared with 54% in the previous study. The majority of these operations involved bullet removal, under local or general anaesthesia. The majority of surgical procedures on the head or abdomen were done under general anaesthesia.
Outcomes
The majority of admissions to the ICU were of patients with head injuries, organ damage or spinal injuries, similar to the previous study. Furthermore, the majority of children who were not admitted received soft-tissue injuries only, usually to an extremity, or were shot by pellet guns.
The total of 617 inpatient days demonstrates the burden firearm injuries in children potentially places on resources at RXH - and this figure does not include outpatient visits for treatment of these injuries. Many studies have highlighted the cost of firearm injuries in children and indicate it to be significant.[14,15] In comparison to the previous study, the number of inpatient days has fallen by a significant 40%. The mortality rate of 2% shows a significant decrease from the 6% in the previous study. Additionally, the data show a significant decrease in gunshot-related injuries in children since the year 2000. This reduction can in part be explained by the effects of the legislation. In 1994 there were 3.5 million licensed firearms in the hands of 2.4 million individuals, with approximately 1 500 new gun licence applications submitted daily.[16] Applications peaked at the time of the first democratic elections in 1994: 236 033 new gun licences were issued that year.[17] Although there are now 3.7 million licensed firearms, the rate of firearm applications has gradually declined.[18] In the 7-year period after the introduction of the FCA in 2004, fewer than 300 000 new firearm licence applications have been received. Applications do not represent approvals; a 20 - 30% refusal rate can be expected (unpublished communication, Central Firearms Registry, 6 October 2011). The result in practical terms is that gun ownership levels have dropped significantly in South Africa over the past decade, with a dramatic reduction in the number of licences granted each month.
Our study population included 12 children with physical complications (8.2%), similar to the prevalence of complications in the previous 10 years. However, psychological and emotional complications also have to be taken into account. These effects have been analysed by Garbarino et al.,[19] who found that emotional complications can be as devastating as physical ones.
Conclusions
The previous study concluded that the government should introduce legislation to reduce gun ownership in an attempt to reduce the number of children who sustain firearm-related injuries.[7] New legislation has now been introduced, and the present study demonstrates its effects. The number of children presenting with firearm injuries has fallen significantly, as has the number of deaths. The cost saved by RXH alone is significant, with inpatient days being reduced by 40%. These figures highlight the success of the FCA and provide evidence for the important role civil society can play in reducing gun-related violence through legislation.
Acknowledgements
Our thanks to the staff at CAPFSA and the records staff at RXH for their help in the production of this paper, and to Adele Kirsten for reviewing the paper and for firearm-related data.
REFERENCES
1. South African Medical Research Council. A profile of fatal injuries in South Africa: 7th Annual Report of the National Injury Mortality Surveillance System. Cape Town: MRC, 2005. [ Links ]
2. Matthews T. Facts about firearm injuries and fatalities among children in Cape Town. MPhil thesis, University of Cape Town, 2010. [ Links ]
3. Allard B, Burch VC. The cost of treating serious abdominal firearm-related injuries in South Africa. S Afr Med J 2005;95(8):591-594. [ Links ]
4. Senger C, Keijzer R, Smith G, Muensterer OJ. Pediatric firearm injuries: A 10-year single-center experience of 194 patients. J Pediatr Surg 2011;46(5):927-932. [http://dx.doi.org/10.1016/j.jpedsurg.2011.02.032] [ Links ]
5. Naidoo S, Van As AB. Vulnerability of children to gunshot trauma in violence-prone environment: The case of South Africa. Afr J Paediatr Surg 2011;8(1):101-104. [ Links ]
6. Firearms Control Act 2000. http://www.capegateway.gov.za/Text/2003/firearms_control_act_60_of_2000.pdf (accessed 20 June 2011). [ Links ]
7. Hutt J, Van As AB, Wallis A, Numanoglu A, Millar AJW, Rode H. Gunshot wounds in children: Epidemiology and outcome. African Safety Promotion 2004;2(2):4-15. [http://dx.doi.org/10.4314/asp.v2i2.31606] [ Links ]
8. Miller M, Azrael D, Hemenway D. Firearm availability and unintentional firearm deaths, suicide and homicide among 5-14 year olds. J Trauma 2002;52(2):267-274. [http://dx.doi.org/10.1097/00005373-200202000-00011] [ Links ]
9. Webster DW, Starnes M. Reexamining the association between child access prevention gun laws and unintentional shooting deaths of children. Pediatrics 2000;106(6):1466-1469. [http://dx.doi.org/10.1542/peds.106.6.1466] [ Links ]
10. Jackman JA, Farah MM, Kellermann AL, Simon HK. Seeing is believing: What do boys do when they find a real gun? Pediatrics 2001;107(6):1247-1250. [http://dx.doi.org/10.1542/peds.107.6.1247] [ Links ]
11. Wigton A. Firearm-related injuries and deaths among children and adolescents in Cape Town. S Afr Med J 1999;89(4):407-410. [ Links ]
12. Hadley GP, Mars M. Gunshot injuries in infants and children in KwaZulu-Natal -an emerging epidemic? S Afr Med J 1998;88(4):444-447. [ Links ]
13. Barlow B, Niemirska M, Gandhi RP. Ten years' experience with pediatric gunshot wounds. J Pediatr Surg 1982;28(3):306-308. [http://dx.doi.org/10.1016/S0022-3468(82)80469-7] [ Links ]
14. Allard D, Burch VC. The cost of treating serious abdominal firearm-related injuries in South Africa. S Afr Med J 2005;95(8):591-594. [ Links ]
15. Cook PJ, Lawrence BA, Ludwig J, Miller TR. The medical costs of gunshot injuries in the United States. JAMA 1999;282(5):447-454. [http://dx.doi.org/10.1001/jama.282.5.447] [ Links ]
16. Chetty R, ed. Firearm Use and Distribution in South Africa. Pretoria: National Secretariat for Safety and Security, National Crime Prevention Centre, 2000. [ Links ]
17. Kirsten A. A Nation without Guns? The Story of Gun Free South Africa. Durban: University of KwaZulu-Natal Press, 2008. [ Links ]
18. Shung-King M, Proudlock P, Michelson L. From Fieldwork to Facts to Firearm Control. Cape Town: Children's Institute, University of Cape Town, 2005. [ Links ]
19. Garbarino J, Bradshaw CP, Vorrasi JA. Mitigating the effects of gun violence on children and youth. Future Child 2002;12(2):72. [http://dx.doi.org/10.2307/1602739] [ Links ]
 Correspondence:
Correspondence:
N M Campbell
(n.m.campbell@ncl.ac.uk)

