










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.51 n.2 Cape Town Jan. 2013
CASE REPORT
Post-traumatic diaphragmatic hernias - importance of basic radiographic investigations
E Mansoor
MB ChB cum laude. Department of Cardiothoracic Surgery, Inkosi Albert Luthuli Central Hospital and University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
This case presentation highlights important principles in the management of post-traumatic diaphragmatic hernia. A suggestive history should prompt early diagnosis even if the patient appears well. The chest radiograph, although not pathognomonic, is extremely useful in the detection of diaphragmatic hernia if accurately interpreted. Herniated bowel is at high risk of strangulation, especially in the presence of a 'ribbon sign'. Delayed operative intervention can prove fatal.
The chest radiograph is the single most important investigation required when a post-traumatic diaphragmatic hernia is suspected. A delay while waiting for further special investigations often translates into morbidity and mortality.
Case report
A 57-year-old man had a history of blunt abdominal trauma sustained several years previously in a motor vehicle accident. He complained of progressive non-radiating abdominal pain in the left upper quadrant, vomiting and constipation, which had been present for a week before admission.
On clinical examination he was noted to be in poor general condition. Haemodynamic parameters were within normal limits. Abdominal examination revealed mild left upper quadrant tenderness and no peritonitis. No bowel sounds were audible in the left hemithorax.
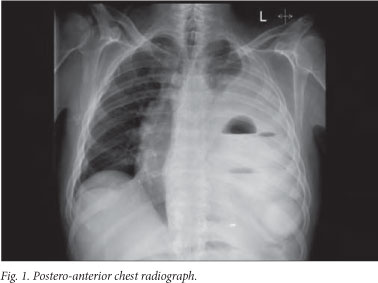
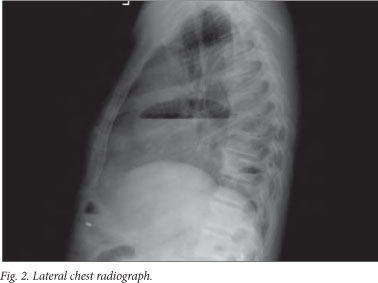
The postero-anterior chest radiograph (Fig. 1) showed an obscured left hemidiaphragm, air/fluid levels in the left hemi- thorax, pleural space occupation and old fractures of left ribs 8 - 9. The lateral film (Fig. 2) suggested the presence of a dilated bowel segment above the diaphragmatic margin. No free sub-diaphragmatic air was present. A subsequent barium study showed an incarcerated loop of large bowel in a 'ribbon-like' contour (Fig. 3) and dilated small bowel in the left chest (Fig. 4). The passage of barium through the colon was relatively unimpeded. Arterial blood gas analysis allayed suspicions of strangulated bowel.


Diagnosis of a delayed post-traumatic diaphragmatic hernia with partial bowel obstruction was made. Surgery was undertaken as soon as the investigations were concluded.
The hernia was approached via a left posterolateral thoracotomy and the pleural space was entered through the 7th intercostal space. The contents of the hernia included mainly large bowel, small bowel and its associated mesentery. The hernial mass was adherent to a cortex-free left lower lobe. Only a moderate amount of turbid fluid was present in the pleural space.
Reduction of the herniated contents and definition of the hernial neck were facilitated by a midline laparotomy. Ischaemia of the large bowel and mesentery was noted. A colonic perforation was present at the splenic flexure, with gross faecal contamination of the peritoneal cavity. The respective colonic segment from transverse colon to splenic flexure and mesentery was resected.
The diaphragmatic defect was repaired primarily with interrupted 'O' nylon sutures in the prescribed manner. After thorough irrigation of the abdomen and thorax via their respective incisions, the cavities were closed in the routine fashion.
Intra-operative haemodynamic instability warranted transfer of the patient to the intensive care unit, where he later died of sepsis.
Discussion
The importance of prompt recognition of the many radiological features of diaphragmatic hernias cannot be over-emphasised.
Study of basic chest radiographs in the anteroposterior and lateral views can yield a great deal of valuable information - 30 -62% sensitivity rates have been reported.[1] The following signs are highly suggestive of a hernia:[2-4]
- an elevated hemidiaphragm
- distortion or obscuring of the diaphragmatic margin
- bowel shadows or air/fluid levels above the diaphragm
- intrathoracic presence of the nasogastric tube
- associated pleural collection, lung collapse and contra-lateral mediastinal shift.
Herniation of intra-abdominal contents into the chest may be particularly difficult to identify on contrast studies. The relationship of the respective positions of the hernia and diaphragm needs to be actively examined. I propose that a 'ribbon sign' suggests the presence of a loop of incarcerated torted bowel. Subsequent strangulation and perforation is the natural history.[5] Herniation of other abdominal structures is likely to co-exist. Pleural collections are not specific to strangulated bowel, but increase the likelihood of its presence. Fluid leaking from oedematous bowel drains directly into the pleural space. This has prognostic implications, so surgery must be performed as a matter of urgency even if the patient appears well.
Computed tomography often does not add additional information to that gained from a combination of the chest radiograph and contrast study. Furthermore, costs and availability may preclude its routine use in the South African setting. 'Hourglass', 'dependent viscera', 'diaphragmatic discontinuity', 'dangling diaphragm' and 'collar' signs have been extensively described in the radiological literature.[3,4]
Diaphragmatic hernias are associated with significant morbidity and mortality. A high index of suspicion must be maintained, and speedy decision making is imperative. Radiological investigations, such as the chest radiograph and contrast examinations, serve as useful adjuncts. Delayed diagnosis and the condition of the hernia contents at operation influence prognosis.
REFERENCES
1. Al-Refaie RE, Awad E, Mokbel EM. Blunt traumatic diaphragmatic rupture: a retrospective observational study of 46 patients. Interact Cardiovasc Thorac Surg 2009;9(1):45-49. [http://dx.doi.org/10.1510/icvts.2008.1983331] [ Links ]
2. Purdy MR. Large-bowel obstruction as a result of traumatic diaphragmatic hernia. S Afr Med J 2007;97(3):180-181. [ Links ]
3. lochum S, Ludig T, Walter F, Sebbag H, Grosdidier G, Blum AG. Imaging of diaphragmatic injury: A diagnostic challenge? Radiographics 2002;22:S103-S118. [ Links ]
4. Sliker CW. Imaging of diaphragmatic injuries. Radiol Clin North Am 2006;44(2):199-211. [http://dx.doi.org/10.1016/j.rcl.2005.10.003] [ Links ]
5. Schulman A, Fataar S, Alheit B. Obstruction-strangulation of post-traumatic diaphragmatic hernia - delayed diagnosis and fatal outcome. S Afr Med J 1965;68(1):39-44. [ Links ]
 Corresponding author:
Corresponding author:
E Mansoor
(dremansoor@gmail.com)

