










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.51 n.2 Cape Town Jan. 2013
GENERAL SURGERY
Ten-year survival of patients with oesophageal squamous cell carcinoma
W HuI; Y LiangIII ; S ZhangIV; Y HuV; J LiuII
IBS. Department of Thoracic Surgery, First Affiliated Hospital of Zhengzhou University, Zhengzhou, People's Republic of China
IIMD. Department of Thoracic Surgery, First Affiliated Hospital of Zhengzhou University, Zhengzhou, People's Republic of China
IIIBS Department of Pediatrics, Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, People's Republic of China
IVBS. Department of Thoracic Oncology, Cancer Centre, Sun Yat-sen University, Guangzhou, People's Republic of China
VMD. Department of Thoracic Oncology, Cancer Centre, Sun Yat-sen University, Guangzhou, People's Republic of China
ABSTRACT
OBJECTIVES: The standard predictive factors of actuarial survival such as T and N stage become less important as patients live for more than 10 years after treatment of cancer. Reports of actual 10-year survivors of oesophageal squamous cell carcinoma (SCC) are rare, and demographic and clinicopathological factors associated with 10-year survival have not been well documented. In this research we evaluated factors predictive of actual, as opposed to actuarial, 10-year survival.
METHODS: We retrospectively analysed 1 046 patients who had undergone oesophagectomy for oesophageal SCC. The demographic and clinicopathological characteristics of patients who were alive more than 10 years after oesophagectomy and those of patients who had died were compared.
RESULTS: Univariate analysis showed that 18 factors differed significantly between the two groups. Based on logistic regression analysis, factors associated with 10-year survival were younger age, female gender, absence of dysphagia, a left transthoracic surgical approach, lower pathological T stage, and fewer metastatic lymph nodes.
CONCLUSION: The independent positive predictors of actual as opposed to actuarial 10-year survival are younger age, female gender, absence of dysphagia, lower pathological T stage, and fewer metastatic lymph nodes.
Squamous cell carcinoma (SCC) accounts for most malignant oesophageal tumours in China, in contrast to predominance of adenocarcinoma in the Western world.[1] The outcome for patients with oesophageal SCC continues to be poor, with 5-year survival rates ranging from 26.2% to 49.4%[2-7] and 10-year survival rates ranging from 8% to 36.1%.[3,5,6] However, all these survival rates are estimated ones. Reports of actual 10-year survivors of oesophageal SCC are rare. According to the recent literature, many demographic and clinicopathological factors are associated with survival after surgical resection of oesophageal SCC. However, since long-term survival is unusual, the prevalence of these factors in actual 10-year survivors has not been well documented. The standard factors associated with improved actuarial survival, such as T and N stage, will differ from those associated with actual 10-year survival. We sought to review and describe our two institutions' experience with oesophagectomy for oesophageal SCC in order to identify factors associated with actual, as opposed to actuarial, 10-year survival.
Materials and methods
Study cohort
This retrospective study was approved by the ethics committee of the First Affiliated Hospital of Zhengzhou University and Sun Yat-sen University Cancer Centre, People's Republic of China. The records of all patients who had undergone oesophagectomy for oesophageal SCC at the Cancer Centre were identified. We- excluded patients with carcinoma of the cervical oesophagus and gastro-oesophageal junction, and those who underwent surgical exploration without oesophagectomy. We also excluded patients who were still alive but had survived for less than 10 years. Finally, we divided the 1 046 patients we had identified into those who were alive more than 10 years after oesophagectomy and those who had died within 10 years of oesophagectomy.
Surgical procedure
Surgical procedures included primary tumour resection and lymph node dissection. The most commonly used surgical approaches included the left transthoracic procedure, the Ivor-Lewis approach, and the cervico-thoraco-abdominal procedure. The left transthoracic and Ivor-Lewis procedures with anastomosis of the upper chest were performed for all tumours of the lower third of the oesophagus and some tumours of the middle third. The cervico-thoraco-abdominal procedure was used for all tumours of the upper third of the oesophagus and some tumours of the middle third. Extensive lymph node dissection in the posterior mediastinum and abdomen was systematically performed, but cervical lymphadenectomy was not. For patients with cervical anastomosis, the lymph nodes exposed in the cervical incision were dissected. All resected specimens were submitted for pathological examination. A pathological diagnosis was made for primary tumours and lymph nodes, which were separately labelled by the surgeons. The lymph nodes examined included those- embedded in the en bloc specimen, which were not labelled but were identified by the pathologists.
Follow-up
A follow-up examination was generally carried out every 3 months in the first year, every 4 months in the second year, and twice a year thereafter. Patients with specific symptoms were examined sooner. Routine follow-up included physical examination, blood biochemical analysis, tumour markers (carcino-embryonic antigen, SCC antigen), a computed tomography scan, oesophagography, ultrasonography and endoscopy. The median duration of follow-up for the patients who were alive was 12 years.
Data retrieved
Patient demographic and clinicopathological characteristics included age, gender, tumour location, severity of dysphagia, weight loss, co-morbidity, a history of smoking and/or alcohol abuse, a family history of any cancer, neo-adjuvant treatment, pathological complete response, surgical approach, completeness of resection, pathological T stage, pathological N stage, histological grade, number of metastatic lymph nodes, number of resected lymph nodes, adjuvant treatment and length of survival. Tumour, node and metastasis descriptors and the staging classification used for this analysis were those defined in the 7th edition of the American Joint Committee on Cancer StagingManual.[8]
Statistical analysis
Statistical analysis was done using SPSS version 17.0 (SPSS, Chicago, Illinois, USA) statistical software. Continuous variables were compared using an independent samples t-test. Mean values were described as mean ± standard deviation. Pearson's chi-square test was used to determine the significance of differences between groups for dichotomous variables. Logistic regression was used to compare the 10-year survival group with the non-10-year survival group in order to identify factors associated with long-term survival. A _p-value of <0.05 was considered statistically significant. Survival time was measured from the date of surgery to the date of death or last follow-up.
Results
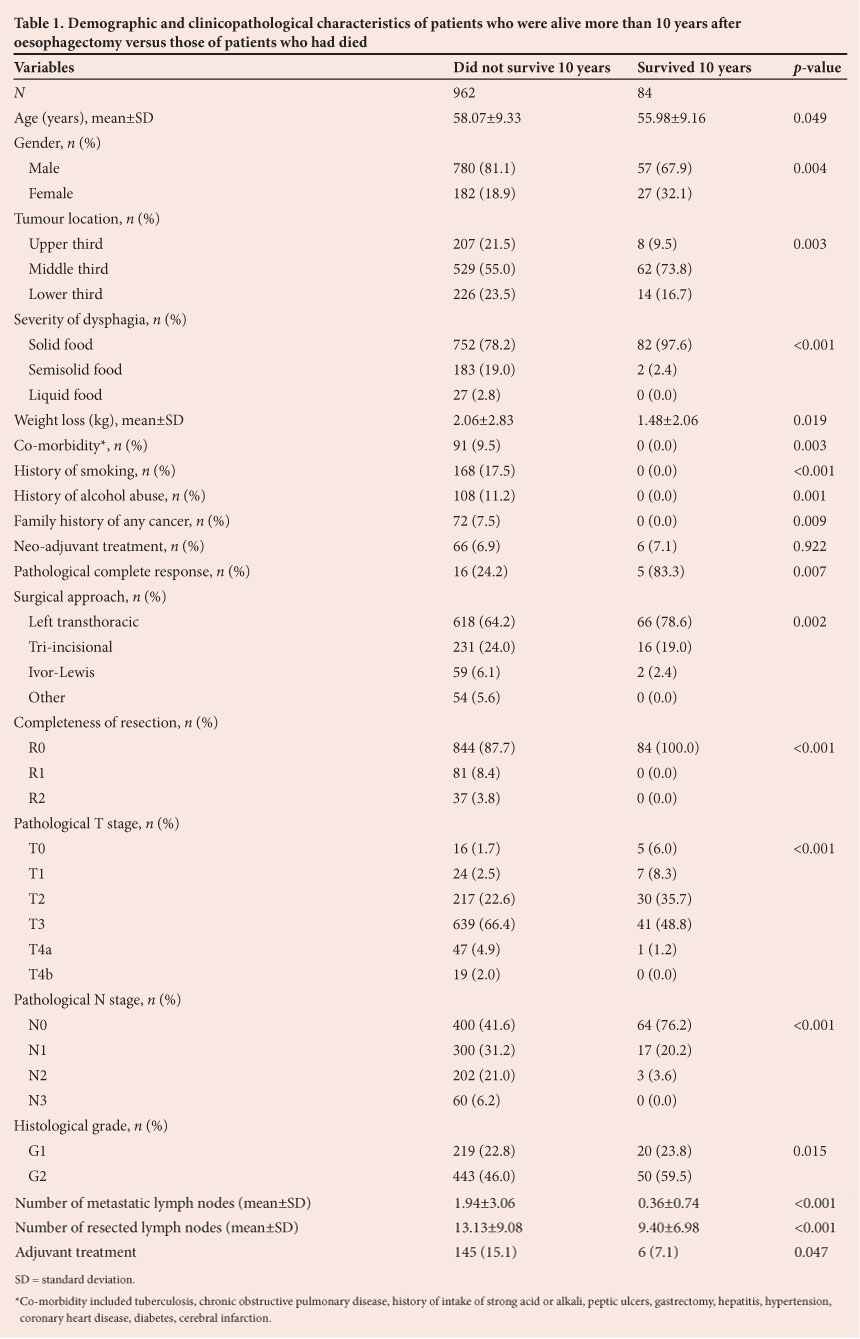
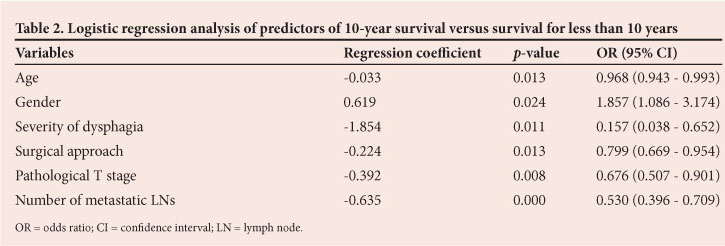
We identified 1 046 patients who had undergone oesophagectomy for SCC. Of these, 84 (8.0%) were actual 10-year survivors. Table 1 sets out their characteristics and those of patients who did not survive for 10 years. Univariate analysis showed that there were significant differences between the two groups with regard to all the variables except neo-adjuvant treatment. Of the entire series, 72 patients (6.9%) underwent neo-adjuvant therapy, and the rate of pathological complete response was 29.2%. Although there was no significant difference between the two groups with regard to the proportion receiving neo-adjuvant therapy, the pathological complete response rate for the 10-year survivor group was higher than that for the group who did not survive for 10 years. There was no patient with co-morbidity, a history of smoking or alcohol abuse, a family history of any cancer or non-R0 resection (R0 resection being defined as resection with negative margins) among the 10-year survivors. Logistic regression analysis showed significant factors associated with actual 10-year survival to be younger age, female gender, absence of dysphagia, a left transthoracic surgical approach, lower pathological T stage, and fewer metastatic lymph nodes (Table 2).
Discussion
Oesophageal squamous cell carcinoma is associated with short median survival and low cure rates. It is important to understand risk factors in subsets of patients with long-term survival. The standard factors such as T and N stage, which are predictive of- actuarial survival, become less important as patients live longer. We therefore evaluated other factors that might predict survival for more than 10 years.
We reviewed the recent literature and found three studies on predictors of survival after surgical resection of oesophageal SCC with large sample sizes. Li et al. analysed 605 patients[5] and found a 10-year overall survival rate of 8%, a figure consistent with our findings. The independent prognostic factors identified by multivariate analysis were number of metastatic lymph nodes, histological grade, tumour location, depth of invasion and vascular invasion.[51 Chen et al. reported on 1 715 patients with oesophageal SCC who underwent extended oesophagectomy with three-field lymph node dissection. The actuarial 10-year overall survival rate was 36.1%. Univariate and multivariate analyses showed that age of 60 years or more, male gender, tumours more than 5 cm long, poorly differentiated histology, T4 tumours, presence of vascular cancer thrombus in the surgical specimen, lymph node positivity, 3 or more positive lymph nodes, and disease stage II or higher were negative prognostic factors for overall survival.[3] Multivariate analysis of 1 553 patients by Yuequan et al. showed that independent prognostic factors were tumour size, histological grade, pathological stage, and a family history of oesophageal cancer.[2]
It has not been determined whether long-term survival in oesophageal SSC is primarily influenced by patient characteristics or tumour biology. Age as a prognostic factor is controversial.[3,9] We found that there were more younger patients in the 10-year survivor group, and age was identified as a significant factor associated with actual 10-year survival based on logistic regression analysis. However, Turkyilmaz et al. compared survival rates for patients aged 40 years or less and over 40 years, and found that younger patients did not have improved 5-year survival compared with their older counterparts.[9]
Many researchers, including ourselves, have demonstrated female gender to be a positive prognostic factor for overall survival,[3,10-12] although Cincibuch et al. concluded that female gender was an independent indicator of poor prognosis.[10] However, it should be noted that patients in that study were treated with chemoradiation, not surgery, and patients with adenocarcinoma were included.[10]
We found, as have other investigators,[12,13] that dysphagia was negatively correlated with long-term survival. This is likely to be because dysphagia usually implies relatively late-stage disease. We included pathological T stage[3,5,7,14,15] and the number of metastatic lymph nodes[2,3,5,14,16-20] among the factors that might affect prognosis, as others have confirmed their impact.
Although they were not identified by us as independent predictors of actual 10-year survival, the impact of tumour location,[5,21,22] weight loss,[9,12,23] completeness of resection[21] and histological grade[2,3,5,20,22] on prognosis has been proven by other investigators.
We found no patients with co-morbidity, a history of smoking or alcohol abuse, or a family history of any cancer in the 10-year survivor group. Although logistic regression analysis did not identify these as significant factors associated with actual 10-year survival, we considered this an important finding. Other investigators have found these to be negative prognostic factors with regard to overall survival.[2,13,24-26]
The left transthoracic surgical approach was identified as a significant factor associated with actual 10-year survival in our study, but other researchers have found that type of oesophagectomy had no prognostic impact.[27] We are unable to explain this finding adequately, although according to traditional practice Chinese surgeons are likely to select that approach in patients with lower-third disease, earlier stage or fewer metastatic lymph nodes. This result was probably impacted on by other relevant factors.
Several researchers found that a higher resected lymph node count favourably influenced survival.[28,29] We had a counterintuitive result in this regard, with fewer resected lymph nodes in the 10-year survivor group - however, this is not to say that the fewer lymph nodes resected, the better the prognosis. There are two possible explanations for this phenomenon. First, the number of resected lymph nodes in itself had no effect on actual 10-year survival. Other research has also indicated that the number of resected lymph nodes had no prognostic impact.[27] Second, there were relatively more patients with earlier stage and relatively few with enlarged lymph nodes in the 10-year survivor group.
Considerable controversy remains with regard to improved long-term survival associated with neo-adjuvant treatment[12,27,30] and adjuvant treatment.*[3,12] Although no significant difference between our two groups was evident when the proportions receiving neo-adjuvant therapy were compared, the pathological complete response rate was higher in the 10-year survivor group than in those with shorter survival. Pathological complete response has been considered a stronger predictor of long-term survival than neo-adjuvant treatment itself.[4,23,30,31] Chen et al. found that postoperative radiation therapy improved overall survival for patients with poor disease-related prognostic factors (positive nodal disease, three or more positive lymph nodes, stage III/IV disease, and large or deeply invasive tumour).13 However, adjuvant treatment failed to predict long-term survival in our research.
The limitations of the current study included its retrospective format, which meant that comparison between 10-year survivors and those who did not survive for 10 years was subject to selection bias. In addition, the study spanned many years and therapeutic modalities have evolved over time, with increasing use of neo-adjuvant and adjuvant treatment. Owing to lack of detailed data on pathological characteristics, we also could not investigate the impact of vascular, perineural and extracapsular invasion on prognosis. Finally, the study excluded patients who underwent oesophagectomy after April 2001 and were still alive, because they had survived for less than 10 years.
In conclusion, the independent positive predictors of actual 10-year survival were younger age, female gender, absence of dysphagia, lower pathological T stage and fewer metastatic lymph nodes.
Acknowledgments. The authors thank all the patients included in this research.
Authorship. J Liu, W Hu and Y Liang designed the study. J Liu, W Hu, S Zhang and Y Hu acquired the data, which W Hu and Y Liang analysed. W Hu and Y Liang wrote the article, which all authors reviewed.
REFERENCES
1. Younes M, Henson DE, Ertan A, Miller CC. Incidence and survival trends of esophageal carcinoma in the United States: Racial and gender differences by histological type. Scand J Gastroenterol 2002;37(12):1359-1365. [http://dx.doi.org/10.1080/003655202762671215] [ Links ]
2. Yuequan J, Shifeng C, Bing Z. Prognostic factors and family history for survival of esophageal squamous cell carcinoma patients after surgery. Ann Thorac Surg 2010;90(3):908-913. [http://dx.doi.org/10.1016/j.athoracsur.2010.05.060] [ Links ]
3. Chen J, Zhu J, Pan J, et al. Postoperative radiotherapy improved survival of poor prognostic squamous cell carcinoma esophagus. Ann Thorac Surg 2010;90(2):435-442. [http://dx.doi.org/10.1016/j.athoracsur.2010.04.002] [ Links ]
4. Yong EL, Han XP, Watson DI, et al. Outcome following surgery for squamous cell carcinoma of the oesophagus. ANZ J Surg 2009;79(10):724-728. [http://dx.doi.org/10.1111/j.1445-2197.2009.05058.x] [ Links ]
5. Li H, Zhang Q, Xu L, et al. Factors predictive of prognosis after esophagectomy for squamous cell cancer. J Thorac Cardiovasc Surg 2009;137(1):55-59. [http://dx.doi.org/10.1016/j.jtcvs.2008.05.024]
6. Zhang DK, Su XD, Long H, et al. Surgical treatment and prognosis in patients with squamous cell carcinoma of thoracic oesophagus [Chinese]. Zhonghua Wai Ke Za Zhi 2008;46(17):1333-1336. [ Links ]
7. Morita M, Yoshida R, Ikeda K, et al. Advances in esophageal cancer surgery in Japan: An analysis of 1000 consecutive patients treated at a single institute. Surgery 2008;143(4):499-508. [http://dx.doi.org/10.1016/j.surg.2007.12.007] [ Links ]
8. Edge SB, Byrd DR, Compton CC, et al. AJCC Cancer Staging Manual. 7th ed. New York: Springer, 2009. [ Links ]
9. Turkyilmaz A, Eroglu A, Subasi M, Karaoglanoglu N. Clinicopathological features and prognosis of esophageal cancer in young patients: Is there a difference in outcome? Dis Esophagus 2009;22(3):211-215. [http://dx.doi.org/10.1111/j.1442-2050.2008.00890.x] [ Links ]
10. Cincibuch J, Neoral C, Aujeský R, et al. Prognostic factors in patients with oesophageal carcinoma treated with chemoradiation: Single center experience. Hepatogastroenterology 2010;57(102-103):1145-1149. [ Links ]
11. Tong DK, Law S, Kwong DL, et al. Histological regression of squamous esophageal carcinoma assessed by percentage of residual viable cells after neoadjuvant chemoradiation is an important prognostic factor. Ann Surg Oncol 2010;17(8):2184-2192. [http://dx.doi.org/10.1245/s10434-010-0995-2] [ Links ]
12. Mariette C, Taillier G, Van Seuningen I, Triboulet JP. Factors affecting postoperative course and survival after en bloc resection for esophageal carcinoma. Ann Thorac Surg 2004;78(4):1177-1183. [http://dx.doi.org/10.1016/j.athoracsur.2004.02.068] [ Links ]
13. Lin CS, Chang SC, Wei YH, et al. Prognostic variables in thoracic esophageal squamous cell carcinoma. Ann Thorac Surg 2009;87(4):1056-1065. [http://dx.doi.org/10.1016/j.athoracsur.2008.11.051] [ Links ]
14. Hu Y, Zheng B, Rong TH, et al. Prognostic analysis of the patients with stage-III oesophageal squamous cell carcinoma after radical oesophagectomy. Chin J Cancer 2010;29(2):178-183. [ Links ]
15. Ren HZ, Pan GQ, Wang JS, et al. Reduced stratifin expression can serve as an independent prognostic factor for poor survival in patients with esophageal squamous cell carcinoma. Dig Dis Sci 2010;55(9):2552-2560. [http://dx.doi.org/10.1007/s10620-009-1065-0] [ Links ]
16. Kobayashi T, Teruya M, Kishiki T, et al. Inflammation-based prognostic score and number of lymph node metastases are independent prognostic factors in esophageal squamous cell carcinoma. Dig Surg 2010;27(3):232-237. [http://dx.doi.org/10.1159/000276910] [ Links ]
17. Liu YP, Ma L, Wang SJ, et al. Prognostic value of lymph node metastases and lymph node ratio in oesophageal squamous cell carcinoma. Eur J Surg Oncol 2010;36(2):155-159. [http://dx.doi.org/10.1016/j.ejso.2009.09.005] [ Links ]
18. Shimada H, Okazumi S, Shiratori T, et al. Impact of lymph node involvement in T2 or T3 thoracic oesophageal squamous cell carcinoma. Hepatogastroenterology 2009;56(93):1039-1043. [ Links ]
19. Zhang HL, Chen LQ, Liu RL, et al. The number of lymph node metastases influences survival and International Union Against Cancer tumor-node-metastasis classification for esophageal squamous cell carcinoma. Dis Esophagus 2010;23(1):53-58. [http://dx.doi.org/10.1111/j.1442-2050.2009.00971.x] [ Links ]
20. Liu W, Hao XS, Fan Q, et al. Cox proportional hazard model analysis of prognosis in patients with carcinoma of oesophagus and gastric cardia after radical resection [Chinese]. Zhonghua Zhong Liu Za Zhi 2008;30(12):921-925. [ Links ]
21. Ruol A, Castoro C, Portale G, et al. Trends in management and prognosis for esophageal cancer surgery: Twenty-five years of experience at a single institution. Arch Surg 2009;144(3):247-254. [http://dx.doi.org/10.1001/archsurg.2008.574] [ Links ]
22. Rice TW, Rusch VW, Ishwaran H, et al. Cancer of the esophagus and esophagogastric junction: Data-driven staging for the seventh edition of the American Joint Committee on Cancer/International Union Against Cancer Cancer Staging Manuals. Cancer 2010;116(16):3763-3773. [http://dx.doi.org/10.1002/cncr.25146] [ Links ]
23. Blanchard P, Quero L, Hennequin C. Prognostic and predictive factors of oesophageal carcinoma [French]. Bull Cancer 2009;96(4):379-389. [http://dx.doi.org/10.1684/bdc.2008.0778] [ Links ]
24. Pultrum BB, Bosch DJ, Nijsten MW, et al. Extended esophagectomy in elderly patients with esophageal cancer: Minor effect of age alone in determining the postoperative course and survival. Ann Surg Oncol 2010;17(6):1572-1580. [http://dx.doi.org/10.1245/s10434-010-0966-7] [ Links ]
25. Siewert JR, Ott K. Are squamous and adenocarcinomas of the esophagus the same disease? Semin Radiat Oncol 2007;17(1):38-44. [http://dx.doi.org/10.1016/j.semradonc.2006.09.007] [ Links ]
26. Gao Y, Hu N, Han X, et al. Family history of cancer and risk for oesophageal and gastric cancer in Shanxi, China. BMC Cancer 2009;9:269. [http://dx.doi.org/10.1186/1471-2407-9-269] [ Links ]
27. Vallböhmer D, Hölscher AH, DeMeester S, et al. A multicenter study of survival after neoadjuvant radiotherapy/chemotherapy and esophagectomy for ypT0N0M0R0 oesophageal cancer. Ann Surg 2010;252(5):744-749. [http://dx.doi.org/10.1097/SLA.0b013e3181fb8dde] [ Links ]
28. Peyre CG, Hagen JA, DeMeester SR, et al. The number of lymph nodes removed predicts survival in esophageal cancer: An international study on the impact of extent of surgical resection. Ann Surg 2008;248(4):549-556. [http://dx.doi.org/10.1097/SLA.0b013e318188c474] [ Links ]
29. Altorki NK, Zhou XK, Stiles B, et al. Total number of resected lymph nodes predicts survival in esophageal cancer. Ann Surg 2008;248(2):221-226. [http://dx.doi.org/10.1097/SLA.0b013e31817bbe59] [ Links ]
30. Courrech Staal EF, Aleman BM, Boot H, et al. Systematic review of the benefits and risks of neoadjuvant chemoradiation for oesophageal cancer. Br J Surg 2010;97(10):1482-1496. [http://dx.doi.org/10.1002/bjs.7175] [ Links ]
31. Kersting S, Konopke R, Dittert D, et al. Who profits from neoadjuvant radiochemotherapy for locally advanced esophageal carcinoma? J Gastroenterol Hepatol 2009;24(5):886-895. [http://dx.doi.org/10.1111/j.1440-1746.2008.05732.x] [ Links ]
 Correspondence:
Correspondence:
J Liu
(liujingeng888@163.com)


{kind=link}
{kind=link}