










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Surgery
versión On-line ISSN 2078-5151
versión impresa ISSN 0038-2361
S. Afr. j. surg. vol.51 no.2 Cape Town ene. 2013
GENERAL SURGERY
Initial experience with laparoscopic splenectomy for immune thrombocytopenic purpura
L FerndaleI ; M NaidooI; S H BhailaII; S R ThomsonIII; F BassaIV
IFCS (SA). Department of Surgery, Faculty of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
IIMB ChB, FRCS (Glasg). Department of Surgery, Faculty of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
IIIChM, FRCS (Eng & Edin). Division of Gastroenterology, Faculty of Health Sciences, University of Cape Town, South Africa
IVFC Path (SA) (Haem), MMed. Department of Haematology, Faculty of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: Laparoscopic splenectomy has become the preferred method of splenectomy for refractory immune thrombocytopenic purpura (ITP). We present our experience with the introduction of laparoscopic splenectomy for ITP.
METHODS: Over a 2-year period, retrospective and prospective data were collected on all patients undergoing laparoscopic splenectomy for ITP at our institution. We analysed demographic data, peri-operative courses, platelet count responses and complications.
RESULTS: Twenty laparoscopic splenectomies were performed. There were 2 conversions to an open procedure. The average operating time was 100 minutes (range 30 - 170 minutes), and mean blood loss was 106 ml (range 50 - 200 ml). There were no deaths or major complications. The mean follow-up period was 7 months. Ninety-five per cent of patients had a complete or partial response to splenectomy.
CONCLUSION: Laparoscopic splenectomy can be introduced safely with an acceptable conversion rate, and is an effective treatment for ITP on short-term follow-up.
Immune thrombocytopenic purpura (ITP) is an immune-mediated disease characterised by thrombocytopenia, the degree of which determines the increased risk of bleeding.[1] It can be primary (idiopathic) or secondary. Secondary ITP can occur with systemic lupus erythematosus, chronic lymphocytic leukaemia, lymphoma, HIV infection and a variety of other disorders. Initial treatment is usually with corticosteroids, splenectomy being reserved for treatment failures.[2]
Laparoscopic splenectomy was first performed in 1991 and has since become the preferred method of splenectomy for refractory ITP.[3] Laparoscopic splenectomy compares favourably with open splenectomy with regard to postoperative pain, length of hospital stay and return to normal daily activity.[4-6]
We present our experience with the introduction of laparoscopic splenectomy at a referral institution to determine its safety and outcomes in ITP.
Methods
Data were collected retrospectively from February 2007 to June 2008 and prospectively from June 2008 to January 2009. All patients were referred for splenectomy by our haematology department following suboptimal response to steroids. Patients were given pneumococcal vaccine 2 weeks before surgery. Information collected included demographic data, pre-operative and postoperative platelet counts, preparation prior to surgery, intra-operative and postoperative course, and complications. Based- on the consensus reached by the International Working Group on ITP in Vicenza, Italy, in October 2007,[1] we defined a platelet count that failed to double and remained under 100x109/l as failure to respond, doubling of the platelet count, which nevertheless remained under 100x109/l, as partial response, and a platelet count over 100x109/l, resolution of clinical symptoms and no further need for steroid therapy as complete response.
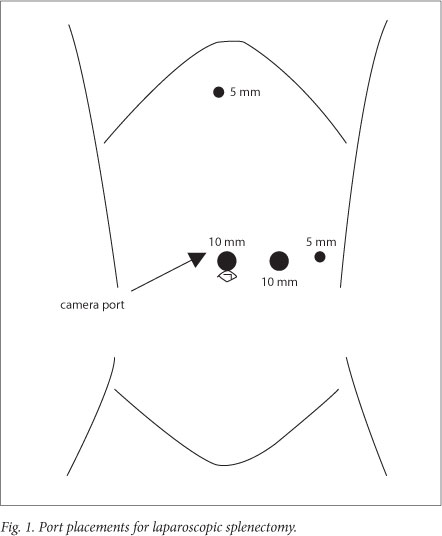
The surgery was performed at Inkosi Albert Luthuli Central Hospital, Durban, KwaZulu-Natal, by two surgeons with extensive experience in laparoscopic cholecystectomy and the use of energy devices for dissection and vessel sealing. Patients were positioned either supine with a slight right lateral tilt or in the right lateral position. Initial entry was achieved under direct vision using the open Hasson technique or an optical port. We used 4 ports, positioned as shown in Fig. 1. Upon entering the abdomen, any adhesions in the left upper quadrant were taken down. The short gastric vessels were divided using either an ultrasonic dissector or a vessel-sealing device. The splenic artery was identified and divided either between clips or using the vessel-sealing device. The spleen was mobilised fully, after which the hilum was divided using the vessel-sealing device. The spleen was inserted into an Endobag, broken up using swab-holding forceps, and removed from the abdomen through the supra-umbilical incision. The sheath and the skin were closed using absorbable sutures. Postoperatively, patients were allowed to eat a normal meal once fully awake and discharged the next day if they were well. Platelet- counts were checked at each follow-up visit. The postoperative platelet counts recorded were from the last follow-up visit, a mean of 7 months after the surgery.
Results
The data on 20 patients were collected retrospectively for 12 patients and prospectively for 8, and are summarised in Table 1. The majority were females in their late twenties. Two patients required conversion to an open procedure because of hilar bleeding that was difficult to control laparoscopically. This occurred early in the series. Blood loss was negligible and the mean splenic weight was 20 g above the upper limit of normal.

The mean pre-operative and postoperative platelet counts were 34x109/l and 287x109/l, respectively. Their distribution is shown in Fig. 2. Eighteen patients had a complete response, 1 did not respond, and 1 had a partial response. Mean hospital stay was 4- days (range 3 - 7 days) and mean follow-up was 7 months (range 1 - 19 months). There were no deaths and no major complications. One patient complained of left-sided chest pain; a chest radiograph and electrocardiogram were normal, and the pain resolved spontaneously after 1 week.

Discussion
The decision to treat ITP is based on the platelet count and the degree of bleeding. Generally treatment is commenced when the platelet count falls below 30x109/l. Corticosteroids are the backbone of initial treatment and are initially effective in 50 - 80% of cases. However, when the dose of steroids is reduced or when treatment is stopped, remission is sustained in only 10 - 30% of cases. Splenectomy is the traditional second-line treatment for patients who do not respond to steroids or relapse after their withdrawal. Complete or partial remission occurs in more than two-thirds of patients who undergo splenectomy, but the relapse rate is 15 - 25%.[2]
This study shows that laparoscopic splenectomy can be performed safely and effectively in appropriately selected patients with ITP.
The two surgeons performing the laparoscopic splenectomies had considerable experience with routine laparoscopic operations and open splenectomy prior to embarking on the introduction of the procedure. That their skill set was adequate to develop the performance of laparoscopic splenectomy safely is attested to by their low conversion rate (10%), which is lower than the 33% reported for the first 15 patients in one the earliest studies implementing the technique. These authors went on to show a 9% conversion rate in their subsequent 35 patients.[7] Other studies addressing the learning curve for laparoscopic splenectomy found that 15 - 25 cases[8-11] are required to become proficient. Compared with both laparoscopic and open splenectomy series, blood loss in our hands was minimal.[5,7]
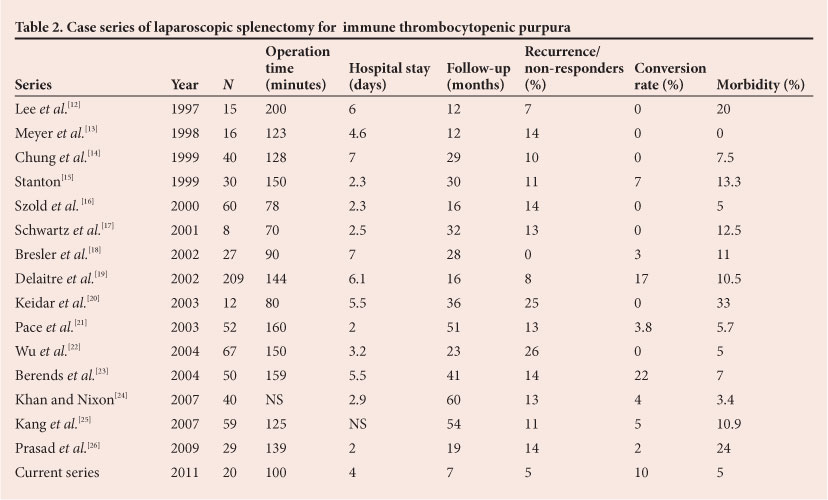
Table 2 lists the cohort series reporting on laparoscopic splenectomy for ITP. A marked heterogeneity is evident. Eight of the studies report on less than 50 cases, and only 1 reports on more than 100. Six of the studies had no conversions, while 2 were at the other extreme with 20% requiring open surgery. It appears that once the learning curve has been overcome, a rate of less than 5% should be the norm. There is marked variability in operating time, with the largest series of over 200 patients having an average time of over 2 hours. Only 4 studies had an operating time of less than our mean of 100 minutes. The follow-up period in our study was short, and the higher recurrence rates generally occurring in- series with longer follow-up are a better reflection of the duration of the operation's efficacy. The morbidity data are generally poorly defined, but as in our series laparoscopic splenectomy is generally free from major complications.
In summary, we believe this study has shown that laparoscopic splenectomy can be introduced safely and effectively by surgeons who have had good exposure to routine laparoscopic operations. It should be considered the preferred option for splenectomy for ITP.
REFERENCES
1. Rodeghiero F, Stasi R, Gernsheimer T. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: Report from the international working group. Blood 2009;113(11):2386-2393. [http://dx.doi.org/10.1182/blood-2008-07-162503] [ Links ]
2. Bromberg M. Immune thrombocytopenic purpura: The changing therapeutic landscape. N Engl J Med 2006;355(16):1643-1645. [http://dx.doi.org/10.1056/NEJMp068169] [ Links ]
3. Delaitre B, Maignien B, Icard P. Laparoscopic splenectomy. Br J Surg 1992;79(12):1334. [http://dx.doi.org/10.1182/blood-2008-07-162503] [ Links ]
4. Cordera F, Long KH, Nagorney D, et al. Open vs. laparoscopic splenectomy for idiopathic thrombocytopenic purpura: Clinical and economic analysis. Surgery 2003;134(1):45-52. [[http://dx.doi.org/10.1067/msy.2003.204] [ Links ]
5. Park A, Marcaccio M, Sternbach M, et al. Laparoscopic vs. open splenectomy. Arch Surg 1999;134(11):1263-1269. [http://dx.doi.org/10.1001/archsurg.134.11.1263] [ Links ]
6. Winslow ER, Brunt LM. Perioperative outcomes of laparoscopic vs. open splenectomy: A meta-analysis with emphasis on complications. Surgery 2003;134(4):647-655. [http://dx.doi.org/10.1016/S0039-6060(03)00312-X] [ Links ]
7. Rege RV, Merriam LT, Joehl RJ. Laparoscopic splenectomy. Surg Clin North Am 1996;76(3):459-468. [http://dx.doi.org/10.1016/S0039-6109(05)70453-9] [ Links ]
8. Cusick R, Waldhausen J. The learning curve associated with pediatric laparoscopic splenectomy. Am J Surg 2001;181(5):393-397. [http://dx.doi.org/10.1016/S0002-9610(01)00609-2] [ Links ]
9. Peters M, Camacho D, Ojeda H, et al. Defining the learning curve for laparoscopic splenectomy for immune thrombocytopenic purpura. Am J Surg 2004;188 (5):522-525. [http://dx.doi.org/10.1016/j.amjsurg.2004.07.026] [ Links ]
10. Rege R, Joehl R. A learning curve for laparoscopic splenectomy at an academic institution. J Surg Res 1999;81(1):27-32. [http://dx.doi.org/10.1006/jsre.1998.5485] [ Links ]
11. Nursal T, Ezer A, Belli S, et al. Reaching proficiency in laparoscopic splenectomy. World J Gastroenterol 2009;15(32):4005-4008. [http://dx.doi.org/10.3748/wjg.15.4005] [ Links ]
12. Lee W, Kim B. Laparoscopic splenectomy for chronic idiopathic thrombocytopenic purpura. Surgical Laparoscopy and Endoscopy 1997;7(3):209-212. [http://dx.doi.org/10.1097/00019509-199706000-00006] [ Links ]
13. Meyer G, Wichmann M, Rau H, et al. Laparoscopic splenectomy for idiopathic thrombocytopenic purpura. Surg Endosc 1998;12(11):1348-1352. [http://dx.doi.org/10.1007/s004649900854] [ Links ]
14. Chung C, Lee W, Choi J, et al. Laparoscopic splenectomy for immune thrombocytopenic purpura - long term result of 40 laparoscopic splenectomies. Yonsei Med J 1999;40(6):578-582. [ Links ]
15. Stanton C. Laparoscopic splenectomy for idiopathic thrombocytopenic purpura: A five-year experience. Surg Endosc 1999;13(11):1083-1086. [http://dx.doi.org/10.1007/s004649901178] [ Links ]
16. Szold A, Schwartz J, Abu-Abeid S, et al. Laparoscopic splenectomies for idiopathic thrombocytopenic purpura: Experience of sixty cases. Am J Hematol 2000;63(1):7-10. [http://dx.doi.org/10.1002/(SICI)1096-8652(200001)63:1<7::AID-AJH2>3.0.CO;2-1] [ Links ]
17. Schwartz J, Eldor A, Szold A. Laparoscopic splenectomy in patients with refractory or relapsing thombotic thrombocytopenic purpura. Arch Surg 2001;136(11):1236-1238. [http://dx.doi.org/10.1001/archsurg.136.11.1236] [ Links ]
18. Bresler L, Guerci A, Brunaud L, et al. Laparoscopic splenectomy for idiopathic thrombocytopenic purpura: Outcome and long term results. World J Surg 2002;26(1):111-114. [http://dx.doi.org/10.1007/s00268-001-0190-5] [ Links ]
19. Delaitre B, Blezel E, Samama G, et al. Laparoscopic splenectomy for idiopathic thrombocytopenic purpura. Surg Laparosc Endosc Percutan Tech 2002;12(6):412-419. [http://dx.doi.org/10.1097/00129689-200212000-00005] [ Links ]
20. Keidar A, Sagi B, Szold A. Laparoscopic splenectomy for immune thrombocytopenic purpura in patients with severe refractory thrombocytopenia. Pathophysiology of Haemostasis and Thrombosis 2003;33(2):116-119. [http://dx.doi.org/10.1159/000073856] [ Links ]
21. Pace D, Chiasson P, Schlachta C, et al. Laparoscopic splenectomy for idiopathic thrombocytopenic purpura. Long-term follow-up data. Surg Endosc 2003;17(1):95-98. [http://dx.doi.org/10.1007/s00464-002-8805-y] [ Links ]
22. Wu J, Lai I, Yuan R, et al. Laparoscopic splenectomy for idiopathic thrombocytopenic purpura. Am J Surg 2004;187(6):720-723. [http://dx.doi.org/10.1016/j.amjsurg.2003.11.032] [ Links ]
23. Berends F, Schep N, Cuesta M, et al. Hematological long term results of laparoscopic splenectomy for patients with idiopathic thrombocytopenic purpura. Surg Endosc 2004;18(5):766-770. [http://dx.doi.org/10.1007/s00464-003-9140-7] [ Links ]
24. Khan L, Nixon S. Laparoscopic splenectomy is a better treatment for adult ITP than steroids - it should be used earlier in patient management: Conclusions of a ten-year follow-up study. Surgeon 2007;5(1):3-4,6-8. [http://dx.doi.org/10.1016/S1479-666X(07)80105-3] [ Links ]
25. Kang C, Lee J, Kim K, et al. Long-term follow-up of laparoscopic splenectomy in patients with immune thrombocytopenic purpura. J Korean Med Sci 2007;22(3):420-424. [http://dx.doi.org/10.3346/jkms.2007.22.3.420] [ Links ]
26. Prasad S, Harman R, Henderson R, et al. Laparoscopic splenectomy and the treatment outcomes for idiopathic thrombocytopaenic purpura at North Shore Hospital. N Z Med J 2009;122(1297):38-48. [ Links ]
 Corresponding author:
Corresponding author:
L Ferndale
(lucienferndale@gmail.com)


{kind=link}