










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Surgery
versão On-line ISSN 2078-5151
versão impressa ISSN 0038-2361
S. Afr. j. surg. vol.51 no.1 Cape Town Jan. 2013
http://dx.doi.org/10.7196/SAJS.1230
PAEDIATRIC SURGERY
DOI:10.7196/SAJS.1230
Paediatric blunt abdominal trauma - are we doing too many computed tomography scans?
M ArnoldI; S W MooreII
IMB ChB, FCPaed Surg. Division of Paediatric Surgery, Faculty of Medicine, Stellenbosch University, Parow, Cape Town
IIMB ChB, FRCS, MD. Division of Paediatric Surgery, Faculty of Medicine, Stellenbosch University, Parow, Cape Town
ABSTRACT
BACKGROUND: Blunt abdominal trauma in childhood contributes significantly to both morbidity and mortality. Selective non-operative management of blunt abdominal trauma in children depends on both diagnostic and clinical factors. Computed tomography (CT) scanning is widely used to facilitate better management. Increased availability of CT may, however, result in its overuse in the management of blunt abdominal trauma in children, which carries significant radiation exposure risks.
AIM: To evaluate the use and value of CT scanning in the overall management and outcome of blunt abdominal trauma in children in the Tygerberg Academic Hospital trauma unit, Parow, Cape Town, South Africa, before and after improved access to CT as a result of installation of a new rapid CT scanner in the trauma management area (previously the scanner had been 4 floors away).
METHODS: Patients aged 0 - 13 years who were referred with blunt abdominal trauma due to vehicle-related accidents before the introduction of the new CT scanner (group 1, n=66, November 2003 - March 2009) were compared with those seen in the 1-year period after the scanner was installed (group 2, n=37, April 2009 - April 2010). Details of clinical presentation, imaging results and their influence on management were retrospectively reviewed. A follow-up group was evaluated after stricter criteria for abdominal CT scanning (viz. prior evaluation by paediatric surgical personnel) were introduced (group 3, n=14, November 2011 - May 2012) to evaluate the impact of this clinical screening on the rate of negative scans.
RESULTS: There were 66 patients in group 1 and 37 in group 2. An apparent increase in CT use with increased availability was accompanied by a marked increase in negative CT scans (38.9% compared with 6.2%; p<0.006). Despite a slightly higher prevalence of associated injuries in group 2, as well as a slightly longer length of hospital stay, there was a similar prevalence of intra-abdominal injuries detected in positive scans in the two groups. In addition, rates of small-bowel perforation in the two groups were similar. The rate of negative scans in group 3 was 46.2% (6/13), but all except one of these patients had a severe brain injury preventing adequate clinical evaluation of intra-abdominal injury.
CONCLUSION: CT scanning for blunt abdominal trauma in children is essential in the presence of appropriate clinical indications. Ease of access probably increases availability, but the rate of negative scans may increase. Management guidelines should be in place to direct CT scanning to cases in which clinical examination and/or other modalities indicate a likelihood of intra-abdominal injury. The principle of 'as low (radiation) dose as reasonably achievable' (ALARA) should be adhered to because of the increased radiation exposure risks in children.
Trauma remains a major contributor to paediatric mortality and is the leading cause of death among children worldwide, particularly in Africa.[1] It has been described as 'the neglected disease of modern society',[2] and whereas childhood deaths from other causes continue to decline in many countries, trauma-related deaths are increasing. In South Africa, the trauma-related death rate in children was reported as being 1.5 - 3.8 times higher than that in the USA in 1990, the leading cause being vehicle-related accidents.[3]
Blunt abdominal trauma (BAT) is more frequent than penetrating abdominal trauma in children and may pose a diagnostic challenge. The diagnostic tool most commonly used in the assessment of the child with BAT is computed tomography (CT) scanning. Ease of access rather than clear clinical indications may tend to influence its use. In centres with easy access to CT scanning, the majority of children with suspected BAT will be given a CT scan. The question asked in this study was whether this approach is justified, or whether the use of CT scanning should be based on clear clinical indications.[3]
The reported advantages of routine CT scanning in children with BAT are that it facilitates the evaluation and triage of identified injuries and minimises negative abdominal exploration.[5] On the other hand, excessive use of medical imaging increases exposure to ionising radiation (a potential carcinogen) without yielding significant benefits to all patients,[6] and excessive use of CT can also negatively impact on healthcare costs. Few guidelines exist to aid in deciding when CT should be used.
The installation of a new multi-slice, high-definition CT scanner directly adjacent to the trauma unit at Tygerberg Academic Hospital,
Parow, Cape Town, in 2009 (as opposed to much more difficult previous access 4 floors away) has shown considerable benefits, including ease of access, improved patient care, decreased patient transit time through the radiology suite, and speeding up of radiological diagnoses. However, its extensive use in children has raised some concern over potential overuse in BAT in this age group, especially in the light of long-term radiation and other risks.
This study set out to evaluate the overall value of CT scanning in the management and outcome of children subjected to this screening modality in the Tygerberg Hospital trauma unit before and after the installation of the new scanner at the beginning of 2009.
Method
We retrospectively reviewed paediatric patients (<13 years) with vehicle-related BAT managed at Tygerberg Academic Hospital (November 2003 - March 2009) with respect to abdominal imaging, clinical and radiological pathological findings and length of hospital stay. The hospital records of children seen over a 1-year period (2009/2010) after the improved access to CT ('post-trauma unit CT', group 2) were analysed and compared with those of patients admitted to the paediatric surgical services during the preceding 5½ years, when the scanner was 4 floors away ('pre-trauma unit CT', group 1). A further group of paediatric BAT patients presenting over a 7-month period after a change in policy regarding abdominal CT scan performance (viz. prior assessment by paediatric surgical personnel was required; group 3) was followed up to assess the impact of this 'rule' on the rate of negative CT scans.
Statistical evaluation
Fisher's exact and/or chi-square statistical tests for significance were performed where applicable. A p-value of <0.05 was regarded as statistically significant. Patient anonymity and confidentiality were protected.
Results
Of 103 patients admitted to the paediatric surgical services with BAT due to vehicle-related accidents during November 2003 -March 2009, 66 were seen in the 'pre-trauma unit CT' period (group 1) and 37 in the 'post-trauma unit CT' period (group 2). The number of patients scanned in group 2 (n=37) probably reflects an increase in CT use over the earlier years of the study.
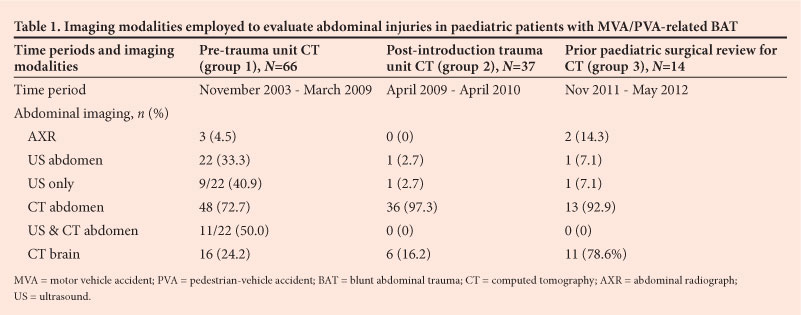
The imaging modalities employed to evaluate the patients' abdominal injuries are shown in Table 1. A decrease in the use of ultrasonography (from 33.3% to 2.7% of paediatric patients with BAT) and an increase in the use of CT scanning were observed, in keeping with current management protocols.
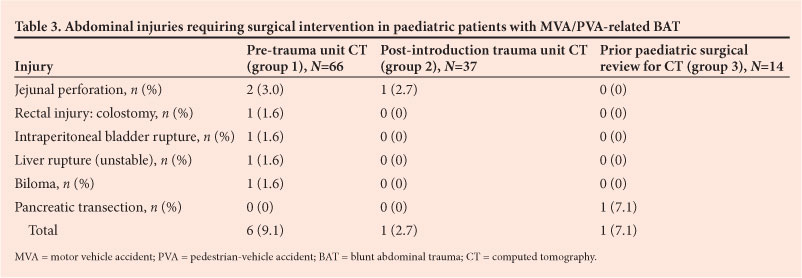
A slightly higher incidence of associated injuries was observed in group 2, as well as slightly longer hospital stay (Table 2). The rates of hollow muscular organ perforation (mostly small bowel) in the two groups were similar (Table 3). Only one of the total of 7 patients who required surgery did not have abdominal CT; this patient had bladder rupture that was managed laparoscopically after ultrasonography. One patient with a jejunal perforation at surgery had free fluid reported on the CT scan with no signs of solid organ injury.
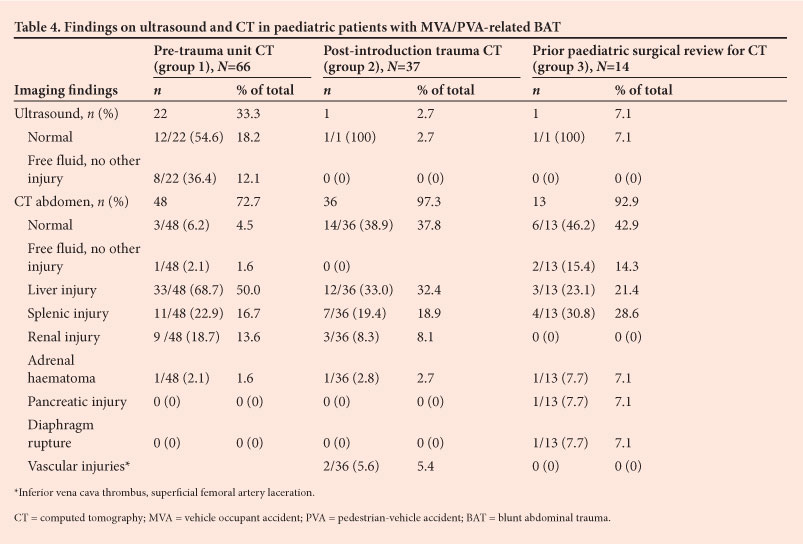
Nevertheless, the prevalences of intra-abdominal injuries detected on CT differed because of a high rate of negative CT scans (38.9% v. 6.2%; p=0.006) after improved access to CT (Table 4).
This was unrelated to concomitant scanning for associated head injuries, which may influence patient selection (i.e. 24.2% and 16.2% of groups 1 and 2, respectively, required CT brain scanning). Looking at the positive abdominal CT scans only (45 in group 1 and 22 in group 2), the prevalences of intra-abdominal injuries in the two groups were similar (24 - 32% splenic injuries and 73 -55% hepatic injuries in groups 1 and 2, respectively).
In group 3, the rate of negative scans was 46.2% (6/13), but all except 1 of these patients had a severe brain injury.
Discussion
Selective non-operative management of BAT has become standard practice in paediatric patients,[3,7,8] with a 90 - 95% success rate in children with blunt solid organ injuries.[7,9] Management of these patients depends heavily on diagnosis and therefore on the improved accuracy of modern imaging modalities, with CT representing the gold standard.[8] It is fully accepted that abdominal CT imaging for BAT underlies the success of selective non-operative management in children, with a negative predictive value of abdominal CT for intra-abdominal injuries exceeding 99% in paediatric patients.[10] CT is particularly useful in situations where the patient is unable to respond and serious injuries may be missed (e.g. head injury). Some would therefore even recommend routine CT scanning of the injured child because of the advantages in evaluating and triaging identified injuries as well as minimising negative abdominal exploration.[5] However, one must bear in mind that abdominal exploration is not often needed, with only 5 - 10% of children proceeding to abdominal exploration. In addition, decisions regarding emergency surgical intervention are only based on clinical grounds (a haemodynamically unstable patient) and not on radiological findings. Timing of special investigations is also an important factor. In this study, CT scans were frequently performed in completely stable children referred from peripheral health institutions more than 24 hours after injury, when scans are unlikely to make a difference in active management in the absence of clinical indications.
There appeared to be an increase in CT use during the period represented by group 2, along with increased accessibility. This increase also raised concern because of the high rate of negative scans (38.9% compared with 6.2%; p<0.006) observed after improved access to CT in our unit. This would suggest a lowered threshold for indications for CT scanning (possibly even in the absence of clinical signs) and even a shift towards more liberal use in the minds of the attending doctors.
Despite a slightly higher incidence of associated injuries in group 2, as well as a slightly longer length of hospital stay (Table 1), the rates of intra-abdominal injuries detected on positive CT scans were similar in the two groups (Table 4). This finding suggests that the increased or routine use of CT did not necessarily improve the rate of detection of blunt abdominal injuries. On the other hand, the rate of negative scans clearly increased significantly (p<0.006) with ease of access. Although this analysis demonstrates the overall trend, the asymmetrical nature of the three groups needs to be borne in mind.
Seven children with BAT required surgery during the period of the study, but CT was only influential in decision making in 6 of them, as one did not have an abdominal scan. In this particular case, bladder rupture was suspected on ultrasonography and confirmed and treated on subsequent laparoscopy! There was also no major difference in rates of small-bowel perforation between the two groups (Table 2). In one patient with a jejunal perforation, only free fluid was seen on CT, with no signs of solid organ injury or free air.
It must be emphasised that careful clinical review of BAT patients remains a mandatory aspect of management. This must be carried out even when there is no radiological evidence of injury on the CT scan, due to the possibility of missed injuries to hollow viscera[11] or secondary bleeding.
Although a trauma unit-based CT scanner is probably every trauma doctor's dream, it is not without possible risks, especially in children. Recent publications[12-16] have drawn attention to the fact that the benefits of CT scanning are offset by the very high radiation dose a modern CT scan represents to a child, with the lifetime radiation risk being proportional to age.[17] It is now well accepted that small children are up to 10 times more sensitive to radiation than adults. The risk is increased not only by their longer life expectancy but also by possible radiation overdose due to copying of adult-orientated protocols (an adult CT scan gives approximately 10 - 20 mGy radiation).[16] This could be even higher if multiphase CT scanning is employed or the CT settings are not adjusted for child-appropriate radiation levels (~5 mGy[16]). Children have been shown to be more sensitive to the long-term effects of radiation because of an increased number of rapidly dividing cells in conjunction with longer life expectancy.[14,18] There is some debate as to the degree of increased risk of cancer mortality related to CT scanning in a child. Currently the risk of developing a serious cancer (e.g. thyroid carcinoma or leukaemia) from a single CT scan has been calculated to be as high as 1 in 1 000, with an even higher risk in infants.[12] As this estimation of radiation exposure is extrapolated from nuclear bomb survivors, and CT has only been in clinical use for 30 years, no long-term data are currently available to indicate how accurate it is.[16,18]
However, it would seem reasonable to advocate judicious use and careful management of CT scans in paediatric BAT. The apparent risks, although largely unproven, are sufficient to cause concern and should lead to careful evaluation of the routine use of CT scanning in paediatric BAT. Guidelines should include avoiding CT scans where clinical judgement or another imaging modality can be used, and avoiding repeat scans unless clinically indicated. Where a CT scan is clinically indicated, there seems to be support for the principle of 'as low (radiation dose) as reasonably achievable' (ALARA)[16] when performing CT in children, by adjusting the dose to the patient's size and age.18,1 Decreasing the radiation dose has been shown not to influence diagnostic accuracy negatively, and theoretically decreases the cancer risk without increasing the rate of missed injuries.[19]
Although our data in this study are retrospective in nature, it appears that routine or increased use of CT scans in children with BAT does not appear to improve the diagnostic yield of intra-abdominal injuries significantly. Furthermore, the possible side-effects mitigate against overuse. Parents should also be informed of the relative risks of the radiation exposure and the expected benefits of the scan, and the issue of informed consent has been raised by some.[20]
Regular review of clinical parameters remains the mainstay of selected non-operative management of BAT in children. There are as yet few data comparing clinical outcome and costs of primary use of CT as opposed to combining serial clinical examinations with ultrasound and use of biochemical measurements. For example, elevated transaminase enzymes have a reported sensitivity of up to 100% (depending on time elapsed since injury)[21,22] for intra-abdominal injury in BAT. A small study found serial ultrasound scans in conjunction with clinical assessments to have over 97% accuracy in effecting appropriate diagnosis and facilitating surgical decision making in children with BAT.[23] CT could then be used as a possible secondary investigation only as indicated. In this scenario, sonography of the abdomen and retroperitoneum to look for intra-abdominal injury in the otherwise stable patient needs to be differentiated from focused abdominal sonography in trauma (FAST), which is known to have a low sensitivity for intra-abdominal injuries and is only aimed at identifying sources of haemorrhage in unstable patients requiring urgent laparotomy/ thoracotomy.[24] Indications for CT should include cases in which the clinical and/or sonographic parameters suggest intra-abdominal injury, or the patient's response may be compromised (e.g. head injury) (Table 5). In stable paediatric BAT patients without head injury, serial clinical examinations by suitably trained clinicians should play a far bigger role in management, particularly when there is low clinical suspicion of an intra-abdominal injury. In admissions after 24 hours from the time of injury, a CT scan is probably only indicated in the presence of ongoing clinical signs or abnormal ultrasound findings. However, clinicians need to be aware that with or without definitive imaging, regular clinical review in BAT patients is mandated.
Conclusion
Although we strongly support the use of CT scanning in children with BAT where clinically indicated, we feel that it should be limited to patients with agreed clinical indications.
Secondly, in order to decrease radiation exposure to children with BAT, CT should not be relied on as the first-line imaging modality exclusively, but should rather be used for greater anatomical accuracy where clinical examination and/or other modalities indicate likely intra-abdominal pathology. Further evaluation of the primary use of serial ultrasound scans as a diagnostic imaging modality in stable children with BAT is recommended.
Thirdly, when CT is required, the machine settings should be adjusted to allow 'as low (radiation dose) as reasonably achievable' (ALARA) to minimise radiation risks.
References
1. Afukaar FK, Antwi P, Ofosu-Amaah S. Pattern of road traffic injuries in Ghana: Implications for control. Inj Control Saf Promot 2003;10(1-2):69-76. [http://dx.doi.org/10.1076/icsp.10.1.69.141071] [ Links ]
2. Bener A, El-Rufaie OE, Al-Suweidi NE. Pediatric injuries in an Arabian Gulf country. Inj Prev 1996;3(3):224-226. [http://dx.doi.org/10.1136/ip.3.3.2241] [ Links ]
3. Cywes S, Kibel SM, Bass DH, et al. Paediatric trauma care: Review article. S Afr Med J 1990;78(7):413-418. [ Links ]
4. Shapiro MJ, Krausz C, Durham RM, Mazuski JE. Overuse of splenic scoring and computed tomographic scans. J Trauma 1999;47(4):651-658. [http://dx.doi.org/10.1097/00005373-199910000-000081] [ Links ]
5. Strohm PC, Uhl M, Hauschild O, et al. What is the value of the whole body spiral CT in the primary radiological imaging of severely injured children? Z Orthop Unfall 2008;146(1):38-43. [ Links ]
6. Korley FK, Pham JC, KirschTD. Use of advanced radiology during visits to US emergency departments for injury-related conditions, 1998-2007. JAMA 2010;304(13):1465-1471. [http://dx.doi.org/10.1001/jama.2010.14081] [ Links ]
7. Davies DA, Pearl RH, Ein SH, et al. Management of blunt splenic injury in children: Evolution of the nonoperative approach. J Pediatr Surg 2009;44(5):1005-1008. [ Links ]
8. Gaines BA. Intra-abdominal solid organ injury in children: Diagnosis and treatment. J Trauma 2009;67(2 Suppl):S135-139. [http://dx.doi.org/10.1097/TA.0b013e3181adc17a1]
9. Myers JG, Dent DL, Stewart RM, et al. Blunt splenic injuries: Dedicated trauma surgeons can achieve a high rate of nonoperative success in patients of all ages. J Trauma 2000;48(5):801-805. [http://dx.doi.org/10.1097/00005373-200005000-00002]
10. Hom J. The risk of intra-abdominal injuries in pediatric patients with stable blunt abdominal trauma and negative abdominal computed tomography. Acad Emerg Med 2010;17(5):469-475. [http://dx.doi.org/10.1111/j.1553-2712.2010.00737] [ Links ]
11. Kim HC, Shin HC, Park SJ, et al. Traumatic bowel perforation: analysis of CT findings according to the perforation site and the elapsed time since accident. Clin Imaging 2004;28(5):334-339. [http://dx.doi.org/10.1016/S0899-7071(03)00244-4]
12. Brenner D, Elliston C, Hall E, Berdon W. Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR Am J Roentgenol 2001;176(2):289-296. [ Links ]
13. Chodick G, Ronckers CM, Shalev V, Ron E. Excess lifetime cancer mortality risk attributable to radiation exposure from computed tomography examinations in children. Isr Med Assoc J 2007;9(8):584-587. [ Links ]
14. Vock P. CT radiation exposure in children: Consequences of the American discussion for Europe. Radiologe 2002;42(9):697-702. [http://dx.doi.org/10.1007/s00117-002-0812-4] [ Links ]
15. Stein SC, Hurst RW, Sonnad SS. Meta-analysis of cranial CT scans in children. A mathematical model to predict radiation-induced tumors. Pediatr Neurosurg 2008;44(6):448-457. [http://dx.doi.org/10.1159/000172967] [ Links ]
16. Scaife ER, Rollins MD. Managing radiation risk in the evaluation of the pediatric trauma patient. Semin Pediatr Surg 2010;19(4):252-256. [http://dx.doi.org/10.1053/j.sempedsurg.2010.06.004Links ] Arial, Helvetica, sans-serif" size="2">]
17. Hall EJ. Radiation biology for pediatric radiologists. Pediatr Radiol 2009;39:Suppl 1,S57 -S64. [http://dx.doi.org/10.1007/s00247-008-1027-2] [ Links ]
18. Mattix KD, Tataria M, Holmes J, et al. Pediatric pancreatic trauma: Predictors of nonoperative management failure and associated outcomes. J Pediatr Surg 2007;42(2):340-344. [http://dx.doi.org/10.1016/j.jpedsurg.2006.10.006] [ Links ]
19. Arrangoiz R, Opreanu RC, Mosher BD, et al. Reduction of radiation dose in pediatric brain CT is not associated with missed injuries or delayed diagnosis. Am Surg 2010;76(11):1255-1259. [ Links ]
20. Karsli T, Kalra MK, Self JL, et al. What physicians think about the need for informed consent for communicating the risk of cancer from low-dose radiation. Pediatr Radiol 2009;39(9):917-925. [http://dx.doi.org/10.1007/s00247-009-1307-5] [ Links ]
21. Hennes HM, Smith DS, Schneider K, et al. Elevated liver transaminase levels in children with blunt abdominal trauma: A predictor of liver injury. Pediatrics 1990;86(1):87-90. [ Links ]
22. Karaduman D, Sarioglu-Buke A, Kilic I, Gurses E. The role of elevated liver transaminase levels in children with blunt abdominal trauma. Injury 2003;34(4):249-252. [http://dx.doi.org/10.1016/S0020-1383(02)00188-2]
23. Retzlaff T, Hirsch W, Till H, Rolle U. Is sonography reliable for the diagnosis of pediatric blunt abdominal trauma? J Pediatr Surg 2010;45(5):912-915. [http://dx.doi.org/10.1016/j.jpedsurg.2010.02.020] [ Links ]
24. Soundappan SV, Holland AJ, Cass DT, Lam A. Diagnostic accuracy of surgeon-performed focused abdominal sonography (FAST) in blunt paediatric trauma. Injury 2005;36(8):970-975. [http://dx.doi.org/10.1016/j.injury.2005.02.026] [ Links ]
 Corresponding author:
Corresponding author:
S W Moore
(swm@sun.ac.za)


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}