










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151
Print version ISSN 0038-2361
S. Afr. j. surg. vol.51 n.1 Cape Town Jan. 2013
http://dx.doi.org/10.7196/SAJS.1357
HEAD AND NECK SURGERY
DOI:10.7196/SAJS.1357
Does sentinel lymph node biopsy have a role in node-positive head and neck squamous carcinoma?
O EdkinsI; C HofmeyrII; J J FaganIII
IMB BCh, FCORL (SA), MMed (Otol). Division of Otolaryngology, University of Cape Town
IIMB ChB, FCORL (SA). Division of Otolaryngology, University of Cape Town
IIIMB ChB, FCS (SA), MMed (Otol). Division of Otolaryngology, University of Cape Town
ABSTRACT
OBJECTIVES/HYPOTHESIS: The objective of the study was to determine whether sentinel lymph node biopsy (SLNB) can be used to reduce clinical overstaging of cervical nodes in head and neck squamous cell carcinoma (SCC) in a developing world setting.
STUDY DESIGN: Sentinel and echelon lymph nodes were identified by means of a combination of lymphoscintigraphy, gamma probe and blue dye staining. They were analysed histologically and their pathological status was compared with the rest of the neck dissection specimen to determine diagnostic accuracy in patients with T1-4 N0-3 SCC of the oral cavity or oropharynx undergoing primary surgical resection and neck dissection.
RESULTS: Thirty-three patients were included in the study, 13 in the node-negative (N0) and 20 in the node-positive (N+) group. In the clinically N0 group the sensitivity of SLNB was 100% and the negative predictive value (NPV) 100%. In the clinically N+ group the sensitivity was 71% and the NPV 60% for staging the nodal status of the neck.
CONCLUSION: The accuracy of SLNB in the clinically N+ neck is too low for SLNB to be a means of avoiding comprehensive neck dissection.
LEVEL OF EVIDENCE: 2B.
Cervical adenopathy in patients with squamous cell carcinoma (SCC) of the upper aerodigestive tract is assumed to represent nodal metastasis and is treated with therapeutic neck dissection.[1] Overstaging of the neck leads to overtreatment by modified neck dissection. In southern Africa and the developing world, the accuracy of clinical staging of cervical adenopathy in head and neck cancer may be confounded by the high prevalence of other causes of lymphadenopathy such as HIV, tuberculosis and untreated upper respiratory and dental infections. De Waal et al. reported a false-positive rate of 32% for the clinically node-positive (N+) neck when comparing clinical staging with pathological analysis in a study done in Cape Town.[2]
Sentinel lymph node biopsy (SLNB) has been employed for the node-negative (N0) neck to avoid unnecessary elective neck dissection (END).[1,3-6] However, no studies have been reported on the use of SLNB to distinguish between inflammatory and metastatic adenopathy in the clinically N+ neck as a means of avoiding unnecessary therapeutic neck dissection.
Aim of the study
The aim of the study was to determine whether SLNB can be used to reduce clinical overstaging of the cervical nodes in head and neck SCC in a developing world setting, and hence reduce the number of unnecessary comprehensive neck dissections done in clinically N+ but pathologically N0 necks.
Materials and methods
A cohort study of patients with T1-4 N0-3 SCC of the oral cavity and oropharynx undergoing primary resection and neck dissection was conducted at Groote Schuur Hospital, Cape Town, between March 2004 and May 2009. Tumours had to be accessible for transoral peritumoural injection. Pregnant and lactating patients were excluded, as were those who had undergone previous surgery or radiotherapy to the neck. SLNB findings did not alter the surgical management of the neck or the primary tumour. The study was approved by the University of Cape Town Ethics Committee.
Lymphoscintigraphy was done in the Department of Nuclear Medicine. Peritumoural injection of 99mTc-labelled human serum albumin (Nanocoll) was immediately followed by saline mouthwash to prevent pooling or swallowing of the residual radioactivity. Continuous-flow lymphoscintigraphy was performed for 30 minutes with a static film, 15 and 30 minutes after the injection. Sentinel lymph nodes (SLNs) detected on lymphoscintigraphy were marked on the skin using a radioactive tracer. In the operating theatre and after induction of general anaesthesia, 1 - 2 ml of methylene blue dye was injected into the mucosa and submucosa surrounding the primary tumour. The neck was explored using standard neck dissection approaches. SLNs and echelon lymph nodes (ELNs) were identified using gamma probe localisation and by identifying blue-stained lymphatics and lymph nodes. In some cases the primary tumour was removed before the neck was explored; this facilitated SLNB where shine-through of radioactivity from the primary tumour interfered with location of the SLN. The SLNs and ELNs were excised. Ex vivo radioactivity, colour and anatomical level of the nodes in the neck were recorded. Each node was sent for histological analysis in 10% formalin. Neck dissection and removal of the primary tumour were then completed.
Clinical details relating to tumour site, clinical stage, and levels of clinically palpable nodes were recorded. The numbers of radioactive-only nodes, blue-only nodes and nodes that were both radioactive and blue-stained, radiation counts of each node, background radioactivity and anatomical levels of the nodes were all documented. The time interval between isotope injection and surgery, the length of time for SLNB, the lymph node basins explored and any technical difficulties were also noted. Histopathological data recorded related to pathological stage (TNM), tumour thickness, status of the SLNs and nodal status of the rest of the neck dissection specimens.
Results
Thirty-three patients were available for analysis. The results are outlined in Table 1. The mean age was 58 years (range 42 - 89 years), with a male/female ratio of 2.3:1. Both the N0 and N+ groups included T1-4 primary tumours; the N+ group comprised N1-3 patients. Three patients underwent lymphoscintigraphy the afternoon before surgery and the remainder immediately before surgery. The mean time interval between injection and surgery was 233 minutes (range 91 - 1 185 minutes). The volume of peritumoural injection of 99mTc-labelled human serum albumin varied with primary tumour size and ranged from 0.2 ml to 0.6 ml (mean 0.37 ml); the dosage was 29.0 - 66.0 MBq (mean 47.2 MBq).
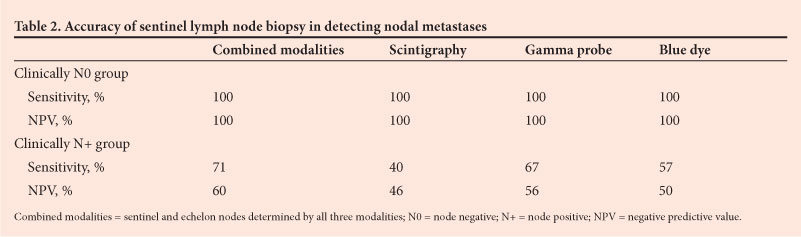
The sensitivity and negative predictive value (NPV) of SLNB as predictor of N-stage of the lymph node basin were calculated separately for the N0 and N+ patient groups. The accuracy in detecting sentinel and echelon nodes in each group was determined for each individual diagnostic modality alone and for a combination of the modalities (Table 2). The N0 group comprised 13 patients, 12 of whom had undergone ipsilateral and 1 bilateral END (14 neck dissections). In the N+ group there were 20 patients, of whom 10 had undergone ipsilateral and 10 bilateral modified radical neck dissections (30 neck dissections).
In the clinically N0 necks, combined lymphoscintigraphy, gamma probe and blue dye yielded sensitivity in identifying the sentinel nodes of 100% and an NPV of 100%. It follows that the methodology and technical expertise of lymphoscintigraphy and intra-operative identification of the SLNs were accurate and were not a confounding factor for the results achieved for N+ necks. In the clinically N+ group the sensitivities of the individual modalities to identify the 16 necks with metastases were 40% (scintigraphy), 67% (gamma probe) and 57% (blue dye), and the combined sensitivity and NPV for the three modalities used were 71% and 60%, respectively.
Discussion
The principal reason for conducting our study was the concern that 32% of neck dissection specimens for clinically N+ necks in our unit were pathologically N0, and the patients had therefore been subjected to an unnecessary comprehensive neck dissection.[2] A theoretical problem of employing SLNB for the pathologically N+ neck is that when a lymph node contains metastatic carcinoma, lymphatic flow may be blocked in that lymphatic channel or node and the tracer or dye may be diverted past the true first echelon node(s) to a 'false SN'.[7] The question therefore was whether SLNB in the N+ neck was sufficiently accurate to exclude cervical nodal metastases.
The reasoning behind SLNB is that the sentinel node is the first lymph node in a nodal basin that receives lymphatic drainage from a malignant tumour, and therefore theoretically is the first node to contain lymphatic metastasis; if a sentinel node is found to be free of metastatic disease, it can be inferred that the metastatic status of the remainder of the nodal basin will be negative. The lymphatic drainage of the breast and other regions of the body is relatively ordered.[7,8] SLNB using radioactive isotope, dye or combinations thereof is the standard of care in many centres for patients with N0 cutaneous malignant melanoma and breast carcinoma.[1] However, the drainage pathways in the head and neck are more complex and less predictable. Skip lesions may also occur, e.g. with SCC of the oral tongue and the floor of the mouth, which may 'fast track' to level IV, 'bypassing' levels I - III.[1,5,9,10]
SLNB has a high degree of sensitivity, and is reliable and reproducible in N0 oral and oropharyngeal SCC.[1,4,11] Reported sensitivity ranges from 89% to 100%, with false-negative rates of 0 - 12.5%.[1] In a meta-analysis of 19 studies, Paleri et al. reported an overall sensitivity of 0.926 (95% confidence interval 0.852 -0.964).[11] This concurs with the 100% sensitivity achieved for the clinically N0 group in our study. Despite the high sensitivity, to our knowledge there are no randomised controlled trials (RCTs) that compare SLNB with END in terms of patient outcome, rates of local recurrence or survival.[5] SLNB in head and neck SCC therefore remains a limited tool pending outcomes of RCTs.[1,5] There is also said to be a significant learning curve associated with SLNB, and it has been suggested that the technique be standardised.[5,11] It has also been suggested that its use should be restricted to early-stage (T1/2 N0) SCC of the oral cavity and oropharynx.[5
In the clinically N+ group, 4/20 patients were pathologically N0 despite having clinically palpable lymph nodes; 20% of patients in this group had therefore undergone unnecessary neck dissections owing to the presumed clinical evidence of nodal metastases. The pre-operative clinical staging in these patients was T2N1, T3N1, T3N2b and T4N2c. Histologically the palpable nodes were generally reactive lymph nodes. Patients had not been routinely tested for HIV and there was no histological evidence of tuberculosis.
The sensitivities of scintigraphy (40%), gamma probe (67%), blue dye (57%) and the combination of the three techniques (71%) to accurately stage the necks in terms of nodal metastases in the clinically N+ group were inadequate to direct surgeons on whether to proceed to comprehensive neck dissection. Our results in clinically N0 necks indicate that the poor accuracy of SLNB in these necks was not due to technical issues or a 'learning curve' associated with the procedure, but reflects inadequacy of SLNB as a staging tool in the clinically N+ neck.
Conclusions
Despite confounding causes responsible for cervical lympha-denopathy in the developing world setting, SLNB cannot be relied upon to direct the therapeutic approach in the clinically N+ neck in patients with mucosal SCC of the head and neck.
Financial disclosure. The research in this article was funded through a research grant from the ENT Society of South Africa.
Conflicts of interest. None.
Presented at the 4th International Conference on Sentinel Node Biopsy and Radioguided Head and Neck Surgery, Copenhagen, Denmark, May 2010, and the South African ENT Congress, Drakensberg, October 2010.
Acknowledgements. Dr T Kotze, Dr R Steyn and Mrs G Boltman of the Department of Nuclear Medicine, Groote Schuur Hospital.
References
1. Devaney KO, Rinaldo A, Rodrigo JP, Ferlito A. Sentinel node biopsy and head and neck tumors - where do we stand today? Head Neck 2006;28(12):1122-1131. [http://dx.doi.org/10.1002/hed.20443] [ Links ]
2. De Waal PJ, Fagan JJ, Isaacs S. Pre- and intra-operative staging of the neck in a developing world practice. J Laryngol Otol 2003;117(12):976-978. [http://dx.doi.org/10.1258/002221503322683876] [ Links ]
3. Hoft S, Maune S, Muhle C, et al. Sentinel lymph-node biopsy in head and neck cancer. Br J Cancer 2004;91(1):124-128. [http://dx.doi.org/10.1038/sj.bjc.6601877]
4. Kosuda S, Kusano S, Kohno N, et al. Feasibility and cost-effectiveness of sentinel lymph node radiolocalization in stage N0 head and neck cancer. Arch Otolaryngol Head Neck Surg 2003;129(10):1105-1109. [http://dx.doi.org/10.1001/archotol.129.10.1105] [ Links ]
5. Kuriakose MA, Trivedi NP. Sentinel node biopsy in head and neck squamous cell carcinoma. Curr Opin Otolaryngol Head Neck Surg 2009;17(2):100-110. [http://dx.doi.org/10.1097/MOO.0b013e3283293631]
6. Taylor RJ, Wahl RL, Sharma PK, et al. Sentinel node localization in oral cavity and oropharynx squamous cell cancer. Arch Otolaryngol Head Neck Surg 2001;127(8):970-974. [ Links ]
7. Nieuwenhuis EJ, Pijpers R, Castelijns JA, Snow GB. Lymphoscintigraphic details of sentinel lymph node detection in 82 patients with squamous cell carcinoma of the oral cavity and oropharynx. Nucl Med Commun 2003;24(6):651-656. [http://dx.doi.org/10.1097/00006231-200306000-00006] [ Links ]
8. Willis AI, Ridge JA. Discordant lymphatic drainage patterns revealed by serial lymphoscintigraphy in cutaneous head and neck malignancies. Head Neck 2007;29(11):979-985. [http://dx.doi.org/10.1002/hed.20631] [ Links ]
9. Alex JC. The application of sentinel node radiolocalization to solid tumors of the head and neck: a 10-year experience. Laryngoscope 2004;114(1):2-19. [http:// dx.doi.org/10.1097/00005537-200401000-00002] [ Links ]
10. Byers RM, Weber RS, Andrews T, McGill D, Kare R, Wolf P. Frequency and therapeutic implications of 'skip metastases' in the neck from squamous carcinoma of the oral tongue. Head Neck 1997;19(1):14-19. [http://dx.doi.org/10.1002/(SICI)1097-0347(199701)19:1<14::AID-HED3>3.0.CO;2-Y] [ Links ]
11. Paleri V, Rees G, Arullendran P, Shoaib T, Krishman S. Sentinel node biopsy in squamous cell cancer of the oral cavity and oral pharynx: A diagnostic meta- analysis. Head Neck 2005;27(9):739-747. [http://dx.doi.org/10.1002/hed.20228] [ Links ]
 Corresponding author:
Corresponding author:
O Edkins
(o.edkins@uct.ac.za)


{kind=link}
{kind=link}