










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Science
versión On-line ISSN 1996-7489
versión impresa ISSN 0038-2353
S. Afr. j. sci. vol.118 no.9-10 Pretoria sep./oct. 2022
http://dx.doi.org/10.17159/sajs.2022/11480
REVIEW ARTICLE
Zero-tolerance drink-driving and road safety in South Africa: What are the options?
Anesh SukhaiI, II; Ashley van NiekerkI, II; Mohamed SeedatI, II
IInstitute for Social and Health Sciences, University of South Africa, Johannesburg, South Africa
IIMasculinity and Health Research Unit, University of South Africa and South African Medical Research Council, Cape Town, South Africa
ABSTRACT
SIGNIFICANCE: Alcohol is a major contributing factor to the burden of road traffic crashes and injuries in South Africa. There has been an increase in political interest and engagement on the issue of drink-driving in recent months following government restrictions on the sale and public consumption of alcohol during the COVID-19 lockdowns along with proposed zero-tolerance drink-driving legislation. In this paper, we critically examine global research and experiences with the adoption of zero-tolerance approaches to drink-driving along with key South African contextual considerations to provide evidence-based and contextually relevant recommendations for advancing zero-tolerance drink-driving legislation in the country. There is significant evidence to support the adoption of zero-tolerance legislation but at a blood alcohol concentration (BAC) threshold limit for the general driving population set at 0.02 g/100 mL (rather than the zero-BAC limit proposed through the Road Traffic Amendment Bill) to allow for variance in testing. Recommendations centre on the proposed legislation incorporating a gradualist approach and its location within a broader zero-tolerance approach that includes other complementary interventions to enable implementation.
: •The recommended blood alcohol level of 0.02 g/100 mL is lower than the best practice limit recommended by the World Health Organization of 0.05 g/100 mL, following consideration of the road safety and general alcohol consumption challenges in South Africa and evidence of success from other similar country contexts. •Broad principles and recommendations are presented to support the sustainable adoption of zero-tolerance drink-driving legislation in the country
Keywords: zero-tolerance, drink-driving, road safety, alcohol, South Africa
Introduction: Impetus for drink-driving legislative reform
The COVID-19 pandemic has renewed attention to alcohol-related harms in South Africa. Following a ban on the sale of alcohol at the commencement of a national lockdown on 27 March 2020, drastic reductions in alcohol-attributable hospital admissions were observed. Approximately 60% fewer injuries from road traffic crashes and assaults were reported at several health facilities during the first 2 weeks of the lockdown.1 Conversely, a surge in trauma cases and hospital admissions was noted following easing of the lockdown and a lifting of the alcohol ban on 1 June 2020.2,3 In a bid to free up hospital beds for potential COVID-19 patients during the first wave of the pandemic, sales and public consumption of alcohol was banned again from 13 July to 17 August 2020, and from 28 December 2020 to 1 February 2021.4 One week following the lifting of the last ban, spikes in trauma admissions were observed once again - for example, five Western Cape hospitals registered a combined increase of 105% in trauma cases.5
Alongside measures meant to contain the negative health outcomes of excessive alcohol use during the aforementioned periods, the Minister of Transport announced the prioritisation of the country's stalled 2015 Road Traffic Amendment Bill (in Government Gazette No. 43201 of 3 April 2020)6, as a legislative intervention to curtail drink-driving7. A key provision within the Bill makes it unlawful for a driver to test positive for any concentration of alcohol, which is a departure from the current legislation that provides for a blood alcohol concentration (BAC) in drivers of less than 0.05 g of alcohol per 100 mL, and less than 0.02 g per 100 mL in professional drivers.6
The renewed focus on legislative reform by the Ministry was also informed by a report on 'Driver intoxication and fatal crashes', which estimated that alcohol intoxication accounts for at least 27.1% of all driver-error fatal crashes in the country, with an estimated annual cost of ZAR18.2 billion.8 For a range of reasons related to how data are collected, the actual burden is also likely to be higher than that estimated.8
The above actions by government to restrict the sale and public consumption of alcohol during the COVID-19 lockdowns and the legislative reform by the Department of Transport reflect the heightened prioritisation of drink-driving on the country's political agenda as well as the growing political will in government to consider and adopt empirically produced information in policy and legislative decisions.6,7 As an attempt to deepen science-policy conversations and support an ethos of empirically based decision-making, we critically examined relevant literature on drink-driving and discuss good-practice interventions that may inform drink-driving zero-tolerance and other supportive measures in the country.
The international literature focused on adoption of zero-tolerance drink-driving legislation is still nascent; hence, we adopted a thematic approach to our literature review. We used Google, Google Scholar, PubMed, and ScienceDirect search engines to identify research publications, including peer-reviewed articles and grey literature related to "zero-tolerance" or "drink-driving" legislation effectiveness and the varying contextual dynamics that influence the outcome of legislative interventions.
Burden of alcohol-related harm and road safety
Excessive consumption of alcohol is common in South Africa.9 About one-third (31%) of South Africans aged 15 years and older consume alcohol. In terms of the volume consumed per drinker, the country ranks 6th highest globally.9 An estimated 4.6% of the population consume at harmful levels, 7.0% are afflicted with alcohol-related disorders, and 6.4% of deaths from all causes are attributable to alcohol.9 There is a clear socio-economic gradient to these deaths, with an overrepresentation of deaths from low socio-economic groups.10
The harmful use of alcohol has a considerable impact on South African society. For example, in a national survey, 65% of women reported physical, sexual, or emotional violence when their husbands or partners were reported to often be drunk.11 Alcohol intoxication also accounts for at least 27.1% of all driver-error attributed fatal crashes8, with a high overall road crash fatality rate of 25.9 deaths per 100 000 - about 1.5 times the global rate.12 Excessive drinking patterns are further evident in mortality statistics showing the average BAC of vehicle drivers at 0.16 g/100 mL - three times the legal threshold for driving of 0.05 g/100 mL.13 An estimated 10-12% of the country's gross domestic product (GDP) is spent on the consequences of alcohol harm.14
Alcohol increases the risks for crashes, injuries, and poor clinical and survival outcomes.15 The mechanisms through which alcohol modifies risk and outcomes are also well known. Alcohol impacts on driving performance through a deterioration in cognitive functioning and psychomotor skills, including divided attention, decreased visual functions and tracking, and a slower response to driving hazards.16 Judgement and memory are impacted, with drink-driving compromising safety assessments and choices related to the use of seatbelts or other protective devices, driving at excessive speeds, and other high-risk behaviours.17-19
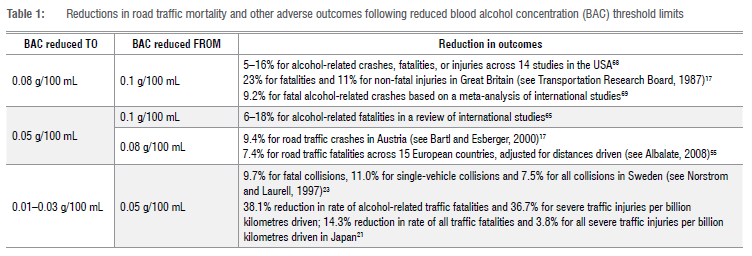
There is a dose-response relationship between BAC and road traffic fatalities. A meta-analysis from studies across the USA, Australia and New Zealand highlighted the odds of a fatal injury as 3.6 at 0.02 g/100 mL, increasing to 13.0 at 0.08 g/100 mL, and exponentially thereafter.20 Consistent with decreased driver performance and increased risk with increasing BACs, there is conversely a decrease in fatalities and other outcomes with reduced BAC threshold limits. Table 1 shows reductions at different BAC thresholds in different settings.
Studies, conducted mainly in high-income countries, also show some evidence for significant reductions in injury when BAC thresholds are reduced beyond the relatively low good practice threshold of 0.05 g/100 mL. In Japan, for example, there was a more than one-third reduction in the rate of both fatal and severe alcohol-related traffic injuries after a reduction in the BAC threshold from 0.05 g/100 mL to 0.01-0.03 g/100 mL.21 These results are consistent with research which shows that even very low concentrations of alcohol at 0.01-0.02 g/100 mL are associated with a deterioration in cognitive and visual functions, and attention and responses to driving hazards, including complex tasks.22,23
Socio-cultural and political context of alcohol use in South Africa
The patterns of alcohol consumption in South Africa as in other parts of the world may be understood from the perspective of prevailing cultural, religious and social norms.24-26 These influences are highlighted through a diversity of dominant patterns of alcohol consumption such as: an important traditional role in fostering friendships and celebrating important occasions by adults in rural communities25; recreational drinking in informal drinking establishments in marginalised urban community settings that lack positive social and recreational opportunities26; and consumption in more advantaged social and work 'event' settings with alcohol symbolising ideals of wealth and status24. The high level of problem drinking and dysfunctional coping in the country is also arguably underpinned historically through apartheid experiences and practices, including unregulated drinking in illegal establishments that perpetuated excessive drinking9,24; drinking within the context of high levels of social stresses from injustices by the apartheid regime27; and excessive drinking where alcohol was used as a currency for remuneration among indigenous workers under the notorious 'dop' system28. The enduring presence of alcohol in the country is also driven largely by a dominant liquor industry by way of its strong marketing forces and its negative influence on current efforts with legislative reform and social transformation, and the limited or inconsistent enforcement and prosecution responses such as with drink-driving offences.29
Legislative and policy responses to alcohol-related harm
The National Liquor Policy30, aligned with the World Health Organization (WHO)'s 2010 global strategy9, provides standards and guidelines for regulating the production, distribution, and consumption of alcohol as well as for the reduction of harmful alcohol use. The policy provides for reducing the maximum BAC limit for driving and regulates the serving of alcohol to intoxicated persons and the operating days and hours of alcohol outlets. In addition, the policy raises the legal drinking age from 18 to 21, requires the presentation of an ID by those appearing to be under 21, and disallows alcohol licences in areas not classified for entertainment or zoned by municipalities for alcohol trade such as petrol stations.30 These standards and guidelines, however, are limited in application, serving as policy recommendations for the amendment of the country's Liquor Act of 1993.31 Several other Bills of salience for public health promotion and the liquor industry, including the Control of Marketing of Alcoholic Beverages Bill of 2013 (focused on limiting public exposure to alcohol marketing through advertising and sponsorships) and the Liquor Amendment Bill of 2016 (based on the Liquor Policy of 2016), have been subject to considerable delays and stalling tactics.32-35 In 2020, industry and international pressure contributed to the repeal of an amendment to regulations related to health messages on container labels of alcoholic beverages.36
Specific measures on restricting drink-driving are included in the National Road Traffic Act of 1996 with proposed amendments to adopt a zero-BAC limit through the Road Traffic Amendment Bill.6 Regulation and enforcement are prioritised in the National Road Safety Strategy 2016-2030, which also focuses on the high levels of involvement of alcohol in traffic crashes, the weakness of law enforcement, and the prosecution of intoxicated drivers.37 Initiatives in South Africa have aligned with the WHO's SAFER initiative38 that features the five most cost-effective priority interventions for reducing the harmful use of alcohol. These interventions, which also impact drink-driving to varying degrees, include: strengthened restrictions on alcohol availability; enforcement of drink-driving countermeasures; access to screening, brief counselling interventions and treatment; bans or restrictions on alcohol advertising, sponsorship and promotion; and raised prices on alcohol through excise taxes and pricing policies.38 Following WHO's SAFER recommendations, specific initiatives have been proposed for South Africa, including: reducing BAC threshold limits for drivers to 0.02 g/100 mL; increasing police enforcement, especially through breath testing; testing for BAC after serious vehicle collisions; and fitting ignition locks to vehicles of persons convicted of drink-driving.28,39
However, a review of key policy initiatives between 1994 and 2009 (on restrictions to alcohol advertising and counter-advertising; regulation of retail sales of alcohol; alcohol taxation; and controls on alcohol packaging) show alcohol policy development in the country as fragmented and uncoordinated.39 Two specific initiatives are flagged as having been most successful from a public health perspective, namely increased excise taxes on alcohol and banning of 'papsakke' (or cheap wine sold in non-resealable foil bags). Their success is attributed to, among other factors, the clear recognition of the problem, provision of policy alternatives, alignment between political and other stakeholder interests along with a committed bureaucracy, and the adoption of evidence-based strategies. In the case of banning 'papsakke', the consensus between a range of civic, corporate, health promotion and state stakeholders and a series of World Health Assembly resolutions, global strategies and regional action plans provided important leverage for policy reform. In the case of raising alcohol excise taxes, the adoption of international benchmarks and cost-benefit evidence were important empirical resources for promoting public health interests and to countering opposition by the liquor industry, which tended to raise the spectre of job and economic losses.39
Zero-tolerance laws on drink-driving
Globally, zero-tolerance laws have been applied to driving under the influence of alcohol and other psychoactive drugs, including illicit drugs, prescription drugs and psychoactive substances.40 Drink-driving laws may make it unlawful to operate a motor vehicle in excess of a specified BAC limit, or may institute a zero-tolerance approach that makes it unlawful to operate a motor vehicle with any amount of alcohol in the body.40 However, many countries that assume zero-tolerance laws - for example, Brazil and Chile - include a margin of tolerance, usually in the range of 0.02-0.03 g/100 mL to accommodate challenges in the detection of very low levels of alcohol using breath testing equipment.41-45 In some states in the USA, zero-tolerance laws focused on young or inexperienced drivers with very low alcohol thresholds, usually at a BAC of 0.02 g/100 mL.46,47 Available data based on studies from the USA and Australia show that zero-tolerance laws account for reductions of 9-24% for fatal crashes and 4-17% for a combination of all crashes.46
The 2018 Global Survey on Alcohol and Health reports on seven countries (Afghanistan, Maldives, Mauritania, Saudi Arabia, Somalia, Sudan and Yemen) with a total ban on alcohol use for all drivers, and 13 countries (for example, Australia and New Zealand) with zero-tolerance for young/novice drivers only.48 The 4th Global Status Report on Road Safety of 2018, indicates that 136 of 175 countries have drink-driving laws with specified BAC threshold limits of which only six countries (Brazil, Hungary, Paraguay, Slovakia, Uruguay and Vietnam) have BAC threshold limits at zero.12 However, countries like Brazil and Chile also provide for a margin of tolerance in their legislation. In total, 90 countries (including the six mentioned above) have a BAC limit not exceeding 0.05 g/100 mL for the general population. Specifically, 55 countries have their maximum BAC limit at 0.05 g/100 mL, 19 countries at 0.03-0.04 g/100 mL and 10 countries at 0.01-0.02 g/100 mL. In Africa, six countries have their maximum BAC limit set at 0.05 g/100 mL (Botswana, Burkina Faso, Eritrea, Guinea Bissau, Mauritius and Nigeria), two countries at 0.03-0.04 g/100 mL (South Africa and Eswatini) and one country at 0.01-0.02 g/100 mL (Mali).12
Studies on zero-tolerance laws that apply to all drivers and that are salient to South Africa have been undertaken mainly in South American countries, including Brazil41-43, Chile44, and Uruguay45. Brazil implemented its zero-tolerance traffic law in 2008, lowering the BAC limit for drivers from 0.06 to 0.02 g/100 mL41-43, driven largely by the need to increase the deterrence effect of legislation and the perceived risk of sanctions for drink-driving49. A time series analysis for Sao Paulo state and capital city for the period 2001-2010, indicated significant reductions for the rate of traffic fatalities (-7.2% and -16.0% for the State and capital, respectively) and for the rate of non-fatal traffic injuries (-1.8 and -2.3% for the State and capital, respectively).49 The stronger effect observed for the capital city in relation to the State was attributed to the relatively higher levels of enforcement.49 A time series analysis for Rio de Janeiro did not indicate a statistically significant reduction in road traffic mortality rates 9 years after implementation, but disaggregated findings showed significant reductions in fatality rates for vulnerable road users including pedestrians aged ≥20 years and among cyclists and motorcyclists aged ≥60 years.42 In Chile, a zero-tolerance law was enacted in 2012, lowering the BAC threshold for drivers from 0.05 to 0.03 g/100 mL.44 A study that adjusted for a range of confounders showed a 15% decrease in alcohol‐related car crashes and an 11% reduction in injuries 3 years after enactment.44 Uruguay implemented a phased reduction in its BAC threshold from 0.08 g/100 mL before the implementation of its law in 2007 to 0.05 g/100 mL in November 2008, 0.03 g/100 mL in March 2009, and finally a zero limit BAC in January 2016.45,50 Significant reductions in fatal crashes were found at both 12 and 24 months following implementation of the zero-limit law in January 2016 (21% and 14%, respectively), although reductions in moderate/severe injuries over both time periods were not significant. The findings show that decreases in thresholds, even at low levels from 0.03g/100 mL to zero BAC, are effective in reducing road traffic injuries and deaths.
The contextual information available in the research reported for Brazil and Chile highlighted the nature of the sanctions with increased BAC limits, by the severity of injuries involved, and by the extent of recidivism. In Brazil, for example, the zero-tolerance law provided for fines, introduction of demerit points and licence suspension of up to 12 months for BACs up to 0.02g/100 mL, and, at higher levels, drivers could be criminally prosecuted with prison sentences from 6 months to 3 years.51 In Chile, large-scale citizen advocacy following a case of a child killed by a car driven by a heavily intoxicated driver, prompted increased sanctions to include prison sentences.52,53 Evaluation outcomes for Chile point to the effectiveness of the second law in sustaining reductions in alcohol-related crashes and injuries.53 Both laws, however, did not have an impact on alcohol intake among drivers who drove with a very high BAC (above the 90th quantile of BAC distribution).53 Strict enforcement was shown to be critical in supporting the zero-tolerance legislation in these settings, which share key social and traffic similarities to South Africa, and elsewhere.17,54,55
Following current empirically produced evidence, the WHO and others recommend that the best practice for BAC threshold limits, at present, is 0.05 g/100 mL for the general driving population and 0.02 g/100 mL for young and novice drivers.12,55 The 0.05 g/100 mL for the general driving population is supported by substantial experimental research showing a considerable increase in crash risk at the 0.05 g/100 mL threshold and higher compared to sober drivers.56,57 Young and novice drivers are even more susceptible to impairment from low levels of alcohol with a greater risk of crash involvement, which relates to their developing skills, experience and maturity. For example, compared to sober drivers and at 0.08 g/100 mL, drivers aged 15-19 years were 87 times more likely to be involved in a road traffic crash compared to drivers over 30 years who had a 16 times higher risk at the same BAC (Leskovsek et al., 2018).17
Journeying towards zero tolerance
From this thematically focused review, we make two observations: first, very few countries have adopted strict zero-tolerance legislation on drink-driving; and, second, most of the emerging research on zero tolerance legislation has been undertaken mainly in Latin American countries that share many similarities with South Africa. Brazil, for example, is also an upper-middle-income economy and shares similar contextual challenges relating to an entrenched culture of drinking and availability of cheap alcohol54, generally low levels of road traffic enforcement54, and weak policies and legislation for the social control of alcohol consumption51. The finding from Brazil on zero-tolerance legislation being protective of pedestrians42, is of especial importance given the extent of pedestrian vulnerability in South Africa. More than half the pedestrian victims of both fatal and non-fatal injuries, in various settings, have been shown to be alcohol related; pedestrians, are shown to be three times more likely to die in a crash when drivers are intoxicated.8
Further to the large burden of alcohol-related road traffic crashes and injuries in the country, South Africa is plagued by a range of challenges in the road traffic environment, including high levels of risky road user behaviours, low levels of enforcement, and generally inadequate road safety responses. High levels of travel exposure, elevated pedestrian vulnerability due to a general lack of safe pedestrian-related infrastructure, and the influences of a dominant alcohol industry advocating for easy access to alcohol exacerbate risks in the road environment. Following the available research on the adoption of zero-tolerance drink-driving legislation and in considering other evidence-based drink-driving practices from middle- and high-income countries with good road safety track records, there is therefore support for lowering of the BAC threshold for drink-driving in South Africa.
However, Brazil's action on drink-driving, for example, began with a presidential decree for zero-tolerance for any level of blood alcohol while driving. The zero-BAC limit was, in this instance, not adopted as there were constraints on its workability; for instance, the detection of small amounts of alcohol in the breath of motorists who may have used products such as mouthwash posed challenges to the no-drink driving measures.54 In addition, as evidenced by the adoption of zero-tolerance legislation in the Latin American countries reviewed above, a higher burden on state resources may also be expected from increased enforcement, prosecutions and contestations with the adoption of zero-alcohol legislation in South Africa, a critical issue in the current resource-strained climate of the country. Accordingly, a zero-tolerance approach that incorporates a drink-driving law with a BAC threshold limit for the general driving population at 0.02 g/100 mL (rather than the immediate zero-BAC limit proposed through the Road Traffic Amendment Bill) is argued to be more feasible. A reduced threshold to 0.02 g/100 mL is also consistent with submissions made at the recent public hearing on the Road Traffic Amendment Bill by the Automobile Association (AA), South African Medical Research Council (SAMRC), and the Southern African Alcohol Policy Alliance (SAAPA). The SAMRC and SAAPA support the implementation of administrative sanctions for BACs between 0.02 g/100 mL and 0.05g/100 mL, and criminal sanctions for higher BACs.58
As described earlier, a large proportion of the South African population is implicated in the harmful and excessive use of alcohol. Long-standing historical, cultural and social norms serve to maintain and normalise high alcohol consumption patterns.24-26 Given the entrenched culture of alcohol consumption and misuse, a gradualist approach, sensitive to the above context, would be more appropriate to enable and sustain behaviour change. This gradualist, broader zero-tolerance approach is premised on mobilising public acceptance for legislative measures. Public engagement and consent, and broad social contracting between government and the public are all critical for legislative adoption and implementation (see Vannoni59 for an elaboration on the concept of gradualism along with the mediating role of public opinion on policy change). For example, as demonstrated in Brazil42 and Chile44, a series of awareness campaigns was undertaken before implementation, and in Uruguay45, a phased strategy was used to reduce BAC thresholds.
It is also recommended that the proposed legislation be nested within a broader zero-tolerance approach and include a range of other complementary interventions including measures relating to enforcement, education, awareness-raising, and harm reduction (see Siegfried and Parry60 for a review of the effectiveness of alcohol control policies, including those targeting drink-driving). This integration would allow for a holistic synergised approach to addressing drink-driving in the country, consistent with a multiple and systems-oriented approach that is generally advocated for addressing road traffic crashes and injuries.61
The integration of complementary interventions may also be phased, consistent with a gradualist approach, for example, by province or municipality to initially allow for testing and refining of implementation strategies and comprehending contextual nuances. Such an approach with a preparatory phase would allow for an incremental approach to the introduction of enforcement measures, and timely introduction of education, awareness and harm reduction measures to complement the legislative intervention.62 Psychoeducational interventions are crucial for obtaining public support and for preparing those most affected by stricter enforcement. Education-type interventions provide important opportunities for behavioural modification, skills transfer and counselling support, especially for the rehabilitation of offenders.63,64 Harm reduction strategies may include designated-driver and safe-ride-home schemes that provide alternatives to drink-driving.9,65
Legislative provisions may allow for the fitment of alcohol ignition interlocks, effective for first-time and repeat offenders.66 These devices are installed within the vehicle and require the driver to provide an alcohol-negative breath specimen to start the vehicle.63 A graduated licensing system by age and/or experience with zero-BAC laws for young and novice drivers, along with other risk-reducing measures such as a ban on late-night driving and on the carrying of passengers could be key in light of the potential protection benefits for this group. Such measures, implemented within graduated driver licensing systems, have been shown to be highly effective, with a Cochrane review indicating a median decrease of 31% in population crash rates among 16-year-old drivers.67 Sanctions may include a combination of fines, demerit points, licence suspension and revocation, and referral for rehabilitation for BACs of 0.02-0.05 g/100 mL. Sanctions may also be implemented in ways that are cognisant of BAC, severity of injuries, and extent of recidivism, as demonstrated in Brazil and Chile. Finally, interventions that are directed at the structural and upstream drivers of excessive alcohol consumption should also be considered, and include attention to the interrelated influences of socio-economic deprivation, mental health conditions, substance abuse, and addiction.9,28 The provision of safe, reliable and affordable public transportation options would also play an important role in keeping inebriated users off the roads.
Conclusion
Zero-tolerance drink-driving legislation is an important public health oriented opportunity for the control of alcohol-related harm in South Africa, especially given the protracted delays and stalling of key alcohol control legislation proposed over the past few decades. In addition, the adoption of zero-tolerance drink-driving legislation (at a reduced threshold of 0.02 g/100 mL) based on a gradualist approach and implemented within a broader zero tolerance approach, along with favourable support from the Department of Transport, offers a critical window of opportunity for addressing drink-driving and advancing road safety in the country. It would also be beneficial to align the proposed gradualist and broader zero-tolerance approach with the country's broader human rights and developmental agenda to allow for synergistic benefits. The realisation of a vision of no drink-driving is also contingent on the adoption of empirical evidence, enabling organisational arrangements, and multiple strategies that embrace the behavioural, environmental, socio-cultural and economic determinants of road safety.
Competing interests
We have no competing interests to declare.
Author contributions'
A.S. prepared the initial draft of the manuscript; A.S., A.v.N. and M.S. were involved with subsequent revisions and development of the manuscript.
References
1.Reuter H, Jenkins LS, De Jong M, Reid S, Vonk M. Prohibiting alcohol sales during the coronavirus disease 2019 pandemic has positive effects on health services in South Africa. Afr J Prim Health Care Fam Med. 2020;12(1), Art. #2528. https://doi.org/10.4102/phcfm.v12i1.2528 [ Links ]
2.Gaye D. Alcohol must be better regulated, not prohibited, MRC tells MPs [webpage on the Internet]. c2020 [cited 2022 Aug 06]. Available from: https://ewn.co.za/2020/07/16/alcohol-must-be-better-regulated-not-prohibited-mrc-tells-mps [ Links ]
3.Winde A. Statement by Premier Alan Winde at his weekly Digital Press Conference [webpage on the Internet]. c2020 [cited 2022 Aug 06]. Available from: https://www.westerncape.gov.za/news/statement-premier-alan-winde-his-weekly-digital-press-conference [ Links ]
4.The Presidency, Republic of South Africa. President Cyril Ramaphosa: Speeches [webpage on the Internet]. c2020 [cited 2021 Feb 28]. Available from: http://www.thepresidency.gov.za/speeches/president-cyril-ramaphosa [ Links ]
5.Githawu M. Winde upset as trauma cases spike after lifting of alcohol ban [webpage on the Internet]. c2021 [cited 2022 Aug 06]. Available from: https://www.iol.co.za/capeargus/news/winde-upset-as-trauma-cases-spike-after-lifting-of-alcohol-ban-a52e3f23-eb73-4b85-b292-e547d95ac9b3 [ Links ]
6.South African Government. National Road Traffic Amendment Bill b7-2020 [document on the Internet]. c2020 [cited 2022 Aug 06]. Available from: https://www.gov.za/documents/national-road-traffic-amendment-bill-b7-2020-29-may-2020-0000# [ Links ]
7.The Citizen. Mbalula talks tough on new regulations - Motorists will have to drive '100% sober' [webpage on the Internet]. c2021 [cited 2022 Aug 06]. Available from: https://citizen.co.za/news/south-africa/government/2425146/mbalula-talks-tough-on-new-regulations-motorists-will-have-to-drive-100-sober/ [ Links ]
8.Govender R, Sukhai A, Van Niekerk A. Driver intoxication and fatal crashes in South Africa: Alcohol as a risk factor for fatal crashes and fatalities, 2016 to 2018 [document on the Internet]. c2020 [cited 2022 Aug 06]. Available from: https://www.rtmc.co.za/images/rtmc/docs/research_dev_rep/Driver%20intoxication%20and%20fatal%20crashes%20Report%20-%20March_2020.pdf [ Links ]
9.World Health Organization. Global status report on alcohol and health 2018 [document on the Internet]. c2018 [cited 2022 Aug 06]. Available from: https://apps.who.int/iris/handle/10665/274603 [ Links ]
10.Probst C, Parry CDH, Wittchen HU, Rehm J. The socioeconomic profile of alcohol-attributable mortality in South Africa: A modelling study. BMC Med. 2018;16(1):97. https://doi.org/10.1186/s12916-018-1080-0 [ Links ]
11.South African Department of Health, Statistics South Africa, South African Medical Research Council, ICF. South Africa Demographic and Health Survey 2016 [document on the Internet]. c2019 [cited 2022 Aug 06]. Available from: https://dhsprogram.com/publications/publication-fr337-dhs-final-reports.cfm [ Links ]
12.World Health Organization. Global Status Report on Road Safety 2018 [document on the Internet]. c2018 [cited 2022 Aug 06]. Available from: https://apps.who.int/iris/rest/bitstreams/1164010/retrieve [ Links ]
13.MRC-UNISA Crime, Violence and Injury Lead Programme. A profile of fatal injuries in South Africa. 7th Annual report of the National Injury Mortality Surveillance System 2005. Cape Town: Crime, Violence and Injury Lead Programme; South African Medical Research Council and University of South Africa; 2017. [ Links ]
14.Matzopoulos RG, Truen S, Bowman B, Corrigall J. The cost of harmful alcohol use in South Africa. S Afr Med J. 2014;104(2):127-132. https://doi.org/10.7196/samj.7644 [ Links ]
15.Ogden EJ, Moskowitz H. Effects of alcohol and other drugs on driver performance. Traffic Inj Prev. 2004;5(3):185-198. https://doi.org/10.1080/15389580490465201 [ Links ]
16.Zhao X, Zhang X, Rong J. Study of the effects of alcohol on drivers and driving performance on straight road. Math Probl Eng. 2014;2014:1-9. https://doi.org/10.1155/2014/607652 [ Links ]
17.Smailović E, Pešić D, Markovic N, Antić B, Lipovac K. The effects of a change in permissible blood alcohol concentration limit on involving drink-driving in road accidents. Transp Res Procedia. 2020;45:201-209. https://doi.org/10.1016/j.trpro.2020.03.008 [ Links ]
18.European Road Safety Observatory (ERSO). Alcohol 2015 [document on the Internet]. No date [cited 2020 Sep 26]. Available from: https://ec.europa.eu/transport/road_safety/sites/roadsafety/files/erso-synthesis-2015-alcohol-detail_en.pdf [ Links ]
19.Sukhai A, Seedat M, Jordaan E, Jackson D. A city-level study of aggressive road behaviours: Magnitude, and predictors and implications for traffic safety. S Afr J Psychol. 2005;35(2):244-269. https://doi.org/10.1177/008124630503500206 [ Links ]
20.Taylor B, Rehm J. The relationship between alcohol consumption and fatal motor vehicle injury: High risk at low alcohol levels. Alcohol Clin Exp Res. 2012;36(10):1827-1834. https://doi.org/10.1111/j.1530-0277.2012.01785.x [ Links ]
21.Nagata T, Setoguchi S, Hemenway D, Perry MJ. Effectiveness of a law to reduce alcohol-impaired driving in Japan. Inj Prev. 2008;14(1):19-23. https://doi.org/10.1136/ip.2007.015719 [ Links ]
22.Moskowitz H, Burns MM, Williams AF. Skills performance at low blood alcohol levels. J Stud Alcohol. 1985;46(6):482-485. https://doi.org/10.15288/jsa.1985.46.482 [ Links ]
23.Heng K, Hargarten S, Layde P, Craven A, Zhu S. Moderate alcohol intake and motor vehicle crashes: The conflict between health advantage and at-risk use. Alcohol Alcohol. 2006;41(4):451-454. https://doi.org/10.1093/alcalc/agh258 [ Links ]
24.Mail & Guardian. Effects of alcohol consumption in South Africa: From the cradle to the grave [webpage on the Internet]. c2017 [cited 2021 Feb 01]. Available from: https://mg.co.za/article/2017-10-27-00-effects-of-alcohol-consumption-in-south-africa-from-the-cradle-to-the-grave/ [ Links ]
25.Setlalentoa B, Pisa P, Thekisho G, Ryke E, Loots DT. The social aspects of alcohol misuse/abuse in South Africa. South Afr J Clin Nutr. 2010;23(3suppl1):S11-S15. https://doi.org/10.1080/16070658.2010.11734296 [ Links ]
26.Puljević C, Learmonth D. Substance abuse prevention in Cape Town's peri-urban settlements: Local health trainers' perspectives. Health Psychol Behav Med. 2014;2(1):183-197. https://doi.org/10.1080/21642850.2013.878659 [ Links ]
27.BBC News. Coronavirus and South Africa's toxic relationship with alcohol [webpage on the Internet]. c2020 [cited 2021 Feb 01]. Available from: https://www.bbc.com/news/world-africa-53699712#:~:text=South%20Africa's%20coronavirus%20crisis%3A&text=Our%20unhealthy%20relationship%20with%20alcohol,of%20the%20pandemic%2C%20in%20March.&text=%22What%20happened%20with%20the%20unbanning,%2Drelated%20trauma%20and%20fatalities.%22 [ Links ]
28.Parry CD. South Africa: Alcohol today. Addiction. 2005;100(4):426-429. https://doi.org/10.1111/j.1360-0443.2005.01015.x [ Links ]
29.Seedat M, Van Niekerk A, Jewkes R, Suffla S, Ratele K. Violence and injuries in South Africa: Prioritising an agenda for prevention. Lancet. 2009;374(9694):1022. https://doi.org/10.1016/S0140-6736(09)60948-X [ Links ]
30.Department of Trade and Industry Republic of South Africa. Final National Liquor Policy 2016 [document on the Internet]. c2016 [cited 2022 Aug 06]. Available from: https://www.gov.za/sites/default/files/gcis_document/201609/40321gon1208.pdf [ Links ]
31.South African Government. National Liquor Act 2003 [document on the Internet]. c2004 [cited 2022 Aug 06]. Available from: https://www.gov.za/documents/liquor-act#:~:text=to%20provide%20for%20essential%20national,provide%20for%20matters%20connected%20therewith [ Links ]
32.Parry C, London L, Myers B. Delays in South Africa's plans to ban alcohol advertising. Lancet. 2014;383(9933):1972. https://doi.org/10.1016/S0140-6736(14)60954-5 [ Links ]
33.Parry C. Toughen the law: One drink is too many if you're driving [webpage on the Internet]. c2019 [cited 2022 Aug 06]. Available from: https://www.dailymaverick.co.za/article/2019-10-24-toughen-the-law-one-drink-is-too-many-if-youre-driving/ [ Links ]
34.Dlamini B. Statement by the Minister of Social Development, Ms Bathabile Dlamini during a media briefing on the Control of Marketing of Alcohol Beverages Bill [document on the Internet]. c2013 [cited 2022 Aug 06]. Available from: https://www.gov.za/statement-minister-social-development-ms-bathabile-dlamini-during-media-briefing-control-marketing [ Links ]
35.The Citizen. Government urged to expedite Liquor Amendment Bill [webpage on the Internet]. c2021 [cited 2022 Aug 06]. Available from: https://citizen.co.za/news/south-africa/2417487/government-urged-to-expedite-liquor-amendment-bill/ [ Links ]
36.South African Department of Health. Repeal of Amendment to Regulations Relating to Health Messages on Container Labels of Alcoholic Beverages, Government Notice No. 1143 of 2020 [document on the Internet]. c2020 [cited 2022 Aug 06]. Available from: https://www.greengazette.co.za/notices/foodstuffs-cosmetics-and-disinfectants-act-54-1972-repeal-of-amendment-to-regulations-relating-to-health-messages-on-container-labels-of-alcoholic-beverages_20201026-GGN-43844-01143 [ Links ]
37.South African Department of Transport. National Road Safety Strategy 2016-2030 [document on the Internet]. No date [cited 2022 Aug 06]. Available from: https://www.gov.za/sites/default/files/gcis_document/201708/strategicplansnationalroadsafetystrategy2016to2030.pdf [ Links ]
38.World Health Organization. Safer: A world free from alcohol related harms [document on the Internet]. c2018 [cited 2022 Aug 06]. Available from: https://apps.who.int/iris/handle/10665/329931 [ Links ]
39.Parry CD. Alcohol policy in South Africa: A review of policy development processes between 1994 and 2009. Addiction. 2010;105(8):1340-1345. https://doi.org/10.1111/j.1360-0443.2010.03003.x [ Links ]
40.World Health Organization. Drug use and road safety: A policy brief [document on the Internet]. c2016 [cited 2022 Aug 06]. Available from: https://apps.who.int/iris/handle/10665/249533 [ Links ]
41.Volpe FM, Ladeira RM, Fantoni R. Evaluating the Brazilian zero tolerance drinking and driving law: Time series analyses of traffic-related mortality in three major cities. Traffic Inj Prev. 2017;18(4):337-343. https://doi.org/10.1080/15389588.2016.1214869 [ Links ]
42.Jomar RT, Ramos DO, Fonseca VAO, Junger WL. Effect of the zero-tolerance drinking and driving law on mortality due to road traffic accidents according to the type of victim, sex, and age in Rio de Janeiro, Brazil: An interrupted time series study. Traffic Inj Prev. 2019;20(3):227-232. https://doi.org/10.1080/15389588.2019.1576035 [ Links ]
43.Andreuccetti G, Carvalho HB, Cherpitel CJ, Ye Y, Ponce JC, Kahn T, et al. Reducing the legal blood alcohol concentration limit for driving in developing countries: A time for change? Results and implications derived from a time-series analysis (2001-10) conducted in Brazil. Addiction. 2011;106(12):2124-2131. https://doi.org/10.1111/j.1360-0443.2011.03521.x [ Links ]
44.Otero S, Rau T. The effects of drinking and driving laws on car crashes, injuries, and deaths: Evidence from Chile. Accid Anal Prev. 2017;106:262-274. https://doi.org/10.1016/j.aap.2017.05.031 [ Links ]
45.Davenport S, Robbins M, Cerdá M, Rivera-Aguirre A, Kilmer B. Assessment of the impact of implementation of a zero blood alcohol concentration law in Uruguay on moderate/severe injury and fatal crashes: A quasi-experimental study. Addiction. 2021;116(5):1054-1062. https://doi.org/10.1111/add.15231 [ Links ]
46.Shults RA, Elder RW, Sleet DA, Nichols JL, Alao MO, Carande-Kulis VG, et al. Reviews of evidence regarding interventions to reduce alcohol-impaired driving. Am J Prev Med. 2001;21(4 Suppl):66-88. https://doi.org/10.1016/s0749-3797(01)00381-6 [ Links ]
47.National Academies of Sciences, Engineering, and Medicine. Getting to zero alcohol-impaired driving fatalities: A comprehensive approach to a persistent problem. Washington DC: US National Academies Press; 2018. https://doi.org/10.17226/24951 [ Links ]
48.World Health Organization. Global health observatory: Legal BAC limits by country [webpage on the Internet]. c2018 [cited 2019 May 08]. Available from: http://apps.who.int/gho/data/view.main.54600 [ Links ]
49.Andreuccetti G, Carvalho H, Leyton V. Evidence-based drinking and driving policies in Brazil: Using evidence to guide policy changes. In: Proceedings of the 20th International Council on Alcohol, Drugs and Traffic Safety Conference; 2013 August 25-28; Brisbane Convention and Exhibition Centre, Australia. Brisbane: International Conference on Alcohol, Drugs and Traffic Safety; 2013. [ Links ]
50.EFE. Uruguay bans drinking and driving [webpage on the Internet]. c2015 [cited 2022 Aug 06]. Available from: https://www.efe.com/efe/english/life/uruguay-bans-drinking-and-driving/50000263-2799581#:~:text=Uruguayan%20President%20Tabare%20Vazquez%20signed,the%20wheel%20after%20consuming%20alcohol.&text=The%20law%20will%20take%20effect%20early%20next%20month [ Links ]
51.Campos VR, de Souza e Silva R, Duailibi S, dos Santos JF, Laranjeira R, Pinsky I. The effect of the new traffic law on drinking and driving in São Paulo, Brazil. Accid Anal Prev. 2013;50:622-627. https://doi.org/10.1016/j.aap.2012.06.011 [ Links ]
52.Nistal-Nuño B. Impact of a new law to reduce the legal blood alcohol concentration limit - A Poisson regression analysis and descriptive approach. J Res Health Sci. 2017;17(1), e00374. https://doi.org/10.26226/morressier.57108e32d462b80290b4ad74 [ Links ]
53.García-Echalar A, Rau T. The effects of increasing penalties in drunk driving laws - Evidence from Chile. Int J Environ Res Public Health. 2020;17(21):8103. https://doi.org/10.3390/ijerph17218103 [ Links ]
54.Jurberg C. Brazil targets drink driving on the road to fewer deaths. Bull World Health Organ. 2011;89(7):474-475. https://doi.org/10.2471/BLT.11.020711 [ Links ]
55.Haghpanahan H, Lewsey J, Mackay DF, McIntosh E, Pell J, Jones A, et al. An evaluation of the effects of lowering blood alcohol concentration limits for drivers on the rates of road traffic accidents and alcohol consumption: A natural experiment. Lancet. 2019;393(10169):321-329. https://doi.org/10.1016/S0140-6736(18)32850-2 [ Links ]
56.Voas RB, Torres P, Romano E, Lacey JH. Alcohol-related risk of driver fatalities: An update using 2007 data. J Stud Alcohol Drugs. 2012;73(3):341-350. https://doi.org/10.15288/jsad.2012.73.341 [ Links ]
57.Zador PL, Krawchuk SA, Voas RB. Alcohol-related relative risk of driver fatalities and driver involvement in fatal crashes in relation to driver age and gender: An update using 1996 data. J Stud Alcohol. 2000;61(3):387-395. https://doi.org/10.15288/jsa.2000.61.387 [ Links ]
58.Parliamentary Monitoring Group. National Road Traffic Amendment Bill: Public hearings [document on the Internet]. c2021 [cited 2022 May 20]. Available from: https://pmg.org.za/bill/942/ [ Links ]
59.Vannoni M. Punctuated gradualism: Policy images, public opinion and policy change in tobacco control [doctoral thesis]. London: University College London; 2017. [ Links ]
60.Siegfried N, Parry C. Do alcohol control policies work? An umbrella review and quality assessment of systematic reviews of alcohol control interventions (2006-2017). PLoS ONE. 2019;14(4), e0214865. https://doi.org/10.1371/journal.pone.0214865 [ Links ]
61.World Health Organization, World Bank. World report on road traffic injury prevention [document on the Internet]. c2004 [cited 2022 Aug 06]. Available from: https://www.who.int/publications-detail-redirect/world-report-on-road-traffic-injury-prevention [ Links ]
62.Elder RW, Shults RA, Sleet DA, Nichols JL, Thompson RS, Rajab W, et al. Effectiveness of mass media campaigns for reducing drinking and driving and alcohol-involved crashes: A systematic review. Am J Prev Med. 2004;27(1):57-65. https://doi.org/10.1016/j.amepre.2004.03.002 [ Links ]
63.Wells-Parker E, Bangert-Drowns R, McMillen R, Williams M. Final results from a meta-analysis of remedial interventions with drink/drive offenders. Addiction. 1995;90(7):907-926. https://doi.org/10.1046/j.1360-0443.1995.9079074.x [ Links ]
64.McKnight AJ, Tippetts AS. Accident prevention versus recidivism prevention courses for repeat traffic offenders. Accid Anal Prev. 1997;29(1):25-31. https://doi.org/10.1016/s0001-4575(96)00058-9 [ Links ]
65.Fell JC, Scolese J, Achoki T, Burks C, Goldberg A, DeJong W. The effectiveness of alternative transportation programs in reducing impaired driving: A literature review and synthesis. J Safety Res. 2020;75:128-139. https://doi.org/10.1016/j.jsr.2020.09.001 [ Links ]
66.Burton R, Henn C, Lavoie D, O'Connor R, Perkins C, Sweeney K, et al. A rapid evidence review of the effectiveness and cost-effectiveness of alcohol control policies: An English perspective. Lancet. 2017;389(10078):1558-1580. https://doi.org/10.1016/S0140-6736(16)32420-5 [ Links ]
67.Russell KF, Vandermeer B, Hartling L. Graduated driver licensing for reducing motor vehicle crashes among young drivers. Cochrane Database Syst Rev. 2011;(10), CD003300. https://doi.org/10.1002/14651858.CD003300.pub3 [ Links ]
68.Fell JC, Voas RB. The effectiveness of reducing illegal blood alcohol concentration (BAC) limits for driving: Evidence for lowering the limit to .05 BAC. J Safety Res. 2006;37(3):233-243. https://doi.org/10.1016/j.jsr.2005.07.006 [ Links ]
69.Fell JC, Scherer M. Estimation of the potential effectiveness of lowering the blood alcohol concentration (BAC) limit for driving from 0.08 to 0.05 grams per deciliter in the United States. Alcohol Clin Exp Res. 2017;41(12):2128-2139. https://doi.org/10.1111/acer [ Links ]
 Correspondence:
Correspondence:
Anesh Sukhai
Email: anesh.sukhai@gmail.com
Received: 17 June 2021
Revised: 03 June 2022
Accepted: 13 June 2022
Published: 29 Sep. 2022
Editor: Floretta Boonzaier
Funding: University of South Africa, South African Medical Research Council


{kind=link}