










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Science
On-line version ISSN 1996-7489
Print version ISSN 0038-2353
S. Afr. j. sci. vol.118 n.5-6 Pretoria May./Jun. 2022
http://dx.doi.org/10.17159/sajs.2022/13323
RESEARCH ARTICLE
The intersection of age, sex, race and socioeconomic status in COVID-19 hospital admissions and deaths in South Africa
Waasila JassatI, II; Lovelyn OzougwuI; Shehnaz MunshiIII; Caroline MudaraI; Caroline VikaI; Tracy ArendseI; Maureen MashaI, II; Richard WelchI; Nevashan GovenderI; Joy EbonwuI; Michelle GroomeI, IV; Andre JosephV; Shabir A. MadhiVI, VII; Cheryl CohenI, III; Lucille BlumbergI, II
INational Institute for Communicable Diseases (NICD), National Health Laboratory Service (NHLS), Johannesburg, South Africa
IIRight to Care, Pretoria, South Africa
IIISchool of Public Health, University of the Witwatersrand, Johannesburg, South Africa
IVSchool of Pathology, University of the Witwatersrand, Johannesburg, South Africa
VLife Healthcare, Johannesburg, South Africa
VISouth African Medical Research Council (SAMRC) Vaccines and Infectious Diseases Analytics Research Unit, University of the Witwatersrand, Johannesburg, South Africa
VIIAfrican Leadership in Vaccinology Expertise (ALIVE), University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
Older age, male sex, and non-white race have been reported to be risk factors for COVID-19 mortality. Few studies have explored how these intersecting factors contribute to COVID-19 outcomes. This study aimed to compare demographic characteristics and trends in SARS-CoV-2 admissions and the health care they received. Hospital admission data were collected through DATCOV an active national COVID-19 surveillance programme. Descriptive analysis was used to compare admissions and deaths by age, sex, race, and health sector as a proxy for socio-economic status. COVID-19 mortality and healthcare utilisation were compared by race using random effect multivariable logistic regression models. On multivariable analysis, black African patients (adjusted OR [aOR] 1.3, 95% confidence interval [CI] 1.2, 1.3), coloured patients (aOR 1.2, 95% CI 1.1, 1.3), and patients of Indian descent (aOR 1.2, 95% CI 1.2, 1.3) had increased risk of in-hospital COVID-19 mortality compared to white patients; and admission in the public health sector (aOR 1.5, 95% CI 1.5, 1.6) was associated with increased risk of mortality compared to those in the private sector. There were higher percentages of COVID-19 hospitalised individuals treated in ICU, ventilated, and treated with supplemental oxygen in the private compared to the public sector. There were increased odds of non-white patients being treated in ICU or ventilated in the private sector, but decreased odds of black African patients being treated in ICU (aOR 0.5; 95% CI 0.4, 0.5) or ventilated (aOR 0.5; 95% CI 0.4, 0.6) compared to white patients in the public sector. These findings demonstrate the importance of collecting and analysing data on race and socio-economic status to ensure that disease control measures address the most vulnerable populations affected by COVID-19.
SIGNIFICANCE:
• These findings demonstrate the importance of collecting data on socio-economic status and race alongside age and sex, to identify the populations most vulnerable to COVID-19.
• This study allows a better understanding of the pre-existing inequalities that predispose some groups to poor disease outcomes and yet more limited access to health interventions.
• Interventions adapted for the most vulnerable populations are likely to be more effective.
• The national government must provide efficient and inclusive non-discriminatory health services, and urgently improve access to ICU, ventilation and oxygen in the public sector.
• Transformation of the healthcare system is long overdue, including narrowing the gap in resources between the private and public sectors.
Keywords: COVID-19, hospitalisation, mortality, race, age, sex, socio-economic status
Introduction
South Africa has experienced a high burden of COVID-19 and recorded over 3.6 million laboratory confirmed cases and 96 993 deaths as of 13 February 2022.1 The official reported COVID-19 cases and deaths are an underestimate as indicated by sero-surveys and alternative methods for analysing COVID-19 attributable deaths. A population-based sero-survey undertaken in Gauteng prior to the onset of the fourth COVID-19 wave that was dominated by the Omicron variant, reported that 68% of people not vaccinated against COVID-19 were sero-positive2, which implies that 10.5 million infections had taken place by then, compared with only 2.9 million cases being officially recorded as of 25 November 20213. Furthermore, the South Africa Medical Research Council estimated 298 879 excess deaths between 3 May 2020 and 13 February 2022 attributable to COVID-194, which is three-fold higher than the 96 993 recorded deaths since the start of the pandemic through to 13 February 2022.
The risks for severe COVID-19 disease are disproportionately born among different communities. Older age, male sex, minority race groups, and lower socio-economic status (SES) have been shown to be associated with severe COVID-19 disease and death.5-7 People from vulnerable racial and ethnic groups in many regions have been reported to be disproportionately affected by COVID-19, and have experienced increased risk of infection, hospitalisation and death.8-10 This risk has also been reported in South Africa from a study of a large cohort of hospitalised patients, which demonstrated that non-white race was associated with increased risk of COVID-19 mortality.11
Race and SES are an important predictor of inequality in South Africa. South Africa is an upper-middle-income country with the distinction of having the highest level of income inequality in the world.12 Black Africans, the unemployed, the less educated and female-headed households are most affected by poverty.12,13 Racial classification was introduced by the apartheid regime and remains entrenched in South African society, with four defined race groups. In 2011, South Africans classified themselves in the census, resulting in 2020 mid-year population estimates of 80.8% being black African, 8.8% as coloured, 2.6% as Indian descent and 7.8% as white ancestry.14
Race and SES have an impact on health burden globally and in South Africa. Racial/ethnic and SES disparities in health have been linked to higher risk of infectious diseases and poorer disease outcomes15, as well as reduced life expectancy and mortality16. South Africa has a significant burden of disease related to communicable and non-communicable disease, trauma, and injuries, with a disproportionate share borne by poor black Africans.17
An understanding of the relationship between race and other demographic characteristics with COVID-19 hospitalisation and mortality is important to effectively address the burden of disease among the most affected populations and to inform public health policy. In this study, we aimed to describe the trends and characteristics of SARS-CoV-2 admissions and the health care they received, and compare demographic characteristics of age, sex and race, as well as SES.
Methods
Study design, setting and data source
This study was a cross-sectional analysis using data collected from DATCOV, a national active surveillance system for COVID-19 hospital admissions in South Africa, between 5 March 2020 and 8 January 2022. DATCOV contains data on all individuals who had a positive real-time reverse transcription polymerase chain reaction (rRT-PCR) assay for SARS-CoV-2 or a positive SARS-CoV-2 antigen test, with a confirmed duration of stay in hospital of one full day or longer, regardless of reason for admission. The case reporting form, adapted from the World Health Organization's COVID-19 case reporting tool, contains basic demographic data (age, sex, and race which was self-defined by the patient as black African, white, coloured, Indian ancestry or other race group); exposures such as occupation; potential risk factors such as obesity, comorbid diseases and pregnancy status; treatment and outcomes. Race information was missing in 156 061/439 448 (35.5%) of patients. The Human Research Ethics Committee (Medical) at the University of the Witwatersrand (Johannesburg, South Africa) approved the project protocol as part of a national surveillance programme (M160667).
Data analysis
The wave periods were defined from the week South Africa crossed a weekly incidence risk of 30 cases per 100 000 persons at the start and end of the waves.18
• Pre-wave 1: week 10 (2020) - week 23 (2020) [5 March - 6 June 2020]
• Wave 1: week 24 (2020) - week 34 (2020) [7 June - 22 August 2020]
• Post-wave 1: week 35 (2020) - week 46 (2020) [23 August - 14 November 2020]
• Wave 2: week 47 (2020) - week 5 (2021) [15 November 2020 - 6 February 2021]
• Post-wave 2: week 6 (2021) - week 18 (2021) [7 February - 8 May 2021]
• Wave 3: week 19 (2021) - week 37 (2021) [9 May - 18 September 2021]
• Post-wave 3: week 38 (2021) - week 46 (2021) [19 September - 20 November 2021]
• Wave 4: week 47 (2021) - week 3 (2022) [21 November 2021 - 22 January 2022]
In addition, periods were combined to create four distinct wave periods that corresponded to the periods during which SARS-CoV-2 variants circulated: D614G in the first wave, Beta in the second wave, Delta in the third wave and Omicron in the fourth wave.
COVID-19 in-hospital mortality was defined as a death related to COVID-19 that occurred during the hospital stay and excluded deaths that occurred because of other causes or after discharge from hospital. Case-fatality risk was calculated among individuals with in-hospital outcome, i.e. COVID-19 deaths divided by COVID-19 deaths plus COVID-19 discharges, excluding individuals who were still admitted in hospital at the time of analysis. For the calculation of cumulative incidence, Stats SA mid-year population estimates for 2020 were utilised.14
Categorical variables were presented as frequencies and percentages, while continuous variables such as age were expressed as median and interquartile range (IQR). Chi-square and Kruskal-Wallis tests were used to compare proportions and median difference where appropriate.
Multivariable logistic regression analysis was performed to identify (1) the potential factors associated with COVID-19 in-hospital mortality and (2) the odds of being treated in ICU and ventilated, by race. Age, sex, race, presence of a comorbidity (hypertension, diabetes, chronic cardiac disease, chronic pulmonary disease and asthma, chronic renal disease, malignancy in the past 5 years, obesity, HIV, and past and current tuberculosis), health sector, province and wave period were considered as potential risk factors for COVID-19 in-hospital mortality. Socio-economic variables were not collected. Health sector of admission was used as a proxy for SES, with people admitted in public sector hospitals considered to be from lower SES and people admitted in private sector hospitals assumed to be from higher SES. There is strong alignment of individuals with higher SES being employed and able to afford medical insurance and seek private hospital care, while those of lower SES who are unable to afford private medical insurance are not able to access private hospital care. We assessed all variables that were significant with a p-value of less than 0.2 in the univariate analysis and excluded non-significant factors (p>0.05) with manual backward elimination. Statistical analyses were performed using STATA software version 16 (Stata Corp®, College Station, Texas, USA).
Results
Between 5 March 2020 and 8 January 2022, 386 171 admissions and 91 180 deaths were reported from 646 hospitals in South Africa.
Admission trends
The median age of hospitalised COVID-19 cases was 53 (38-65) years, which was similar among black African patients, coloured patients and patients of Indian descent, but higher among white patients (median age: 61 [IQR 50-73] years; p<0.001) (Table 1). Most COVID-19 hospitalised patients were in the 40-59-year age group =160 172, 36.5%), whilst only 5.9% (n=25 999) were in the <20-year age group (p<0.001). COVID-19 admissions were highest amongst the 40-59-year age group in patients of Indian descent (44.2%), coloured patients (39.6%), and black African patients (35.7%), while the highest percentage of admissions among white patients was in the 60-79-year (40.9%) age group. Overall, there were more admissions among female patients (55.4%) than male patients (p<0.001); however, the trend was reversed with more admissions amongst male patients in those of Indian descent (55.4%) and white ancestry (54.2%). Among 282 496 patients with known race, the cumulative number of COVID-19 hospitalisations was 215 539 (76.3%) among black African patients, 32 672 (11.6%) in white patients, 19 784 (7.0%) among coloured patients and 14 501 (5.1%) in patients of Indian descent.
The number (and percentage) of admissions with no reported comorbidities was 6235 (43.0%) among those of Indian descent and 13 112 (40.1%) of white ancestry, compared with 4 663 (23.6%) among coloured and 60 317 (28.0%) among black African patients. Hypertension (115 032; 26.4%) and diabetes (74 544; 17.1%) were the most prevalent comorbidities amongst all race groups, but comorbidities with high prevalence in black patients were HIV (19 939; 9.3%) and current TB (1176; 1.1%); in white patients were malignancy (383; 1.2%) and obesity (2532; 8.1%); and in patients of Indian descent was chronic cardiac disease (676; 4.7%).
The highest number of COVID-19 hospitalisations was reported during the third wave dominated by the Delta variant (147 582), followed by the second wave which was dominated by the Beta variant (105 985), the first wave which was due to the wild-type virus (71 410) and, finally, the fourth wave (42 746) which was dominated by the Omicron variant.
The highest percentage of total admissions among black African patients was in the first (61 389/106 326; 57.7%) and fourth waves (22 904/42 746; 53.6%); among white patients in the third wave (17 509/157 205; 11.1%), among coloured patients in the third wave (7716/157 205; 4.9%) and among those of Indian descent in the second wave (5033/132 899; 3.8%). In the fourth wave, coloured patients, white patients and those of Indian descent accounted for a lower percentage of total admissions than for the prior three waves (p<0.001), whereas black African patients accounted for a higher percentage of total admissions in the fourth wave compared to the second and third waves (p<0.001).
The percentage of total admissions per wave decreased from the first to third wave among black African individuals and increased from the third to fourth wave (Figure 1). The percentage of total admissions per wave increased from the first to third wave among coloured people, people of Indian descent and white people, and then decreased from the third to fourth wave. The percentage of total admissions in which race was unknown increased with each wave.

Incidence of COVID-19 admissions and deaths
The incidence of COVID-19 admissions (per 100 000 persons) increased with age. While the overall incidence was higher in female (526.8) than male (417.0) individuals, it was higher in female individuals <60 years and in male individuals >60 years (Table 2). The incidence of admissions was highest among people of Indian descent (940.4) and was 446.9 in black African people, 376.5 in coloured people and 697.7 in white people. The incidence of admissions was higher in female than male individuals among black African and coloured people, and higher in male individuals among those of Indian descent and white ancestry.
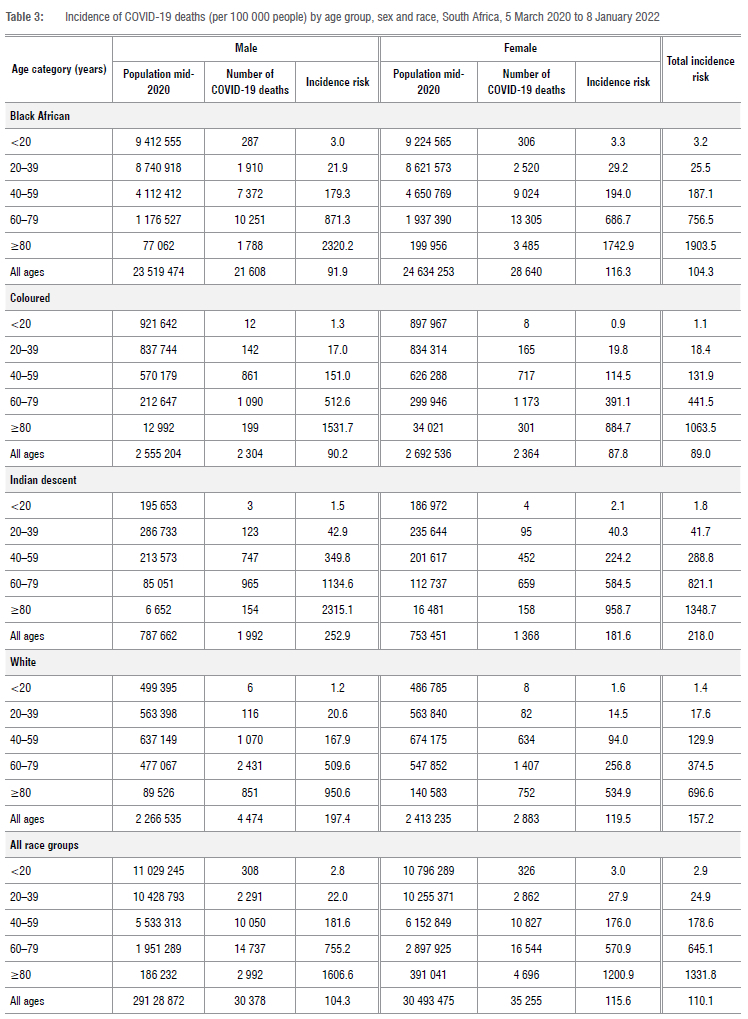
The incidence risk of in-hospital COVID-19 deaths (per 100 000 persons) increased with age (Table 3). While overall incidence was higher in female (115.6) than male patients (104.3), it was higher in female patients <40 years and in male patients >40 years. Incidence of deaths was highest among patients of Indian descent (218.0), followed by white patients (157.2), black African patients (104.3), and coloured patients (89.0). Overall, in the 20-79-year age group, incidence of COVID-19 deaths was highest in those of Indian descent, whilst being highest among black African patients in the <20-year and >80-year age groups.
Factors associated with mortality
On multivariable analysis, black African (adjusted odds ratio [aOR] 1.3, 95% confidence interval [CI] 1.2, 1.3), coloured (aOR 1.2, 95% CI 1.1, 1.3), Indian descent (aOR 1.2, 95% CI 1.2, 1.3) and patients of other races (aOR 1.4, 95% CI 1.4, 1.5) had increased risk of inhospital COVID-19 mortality compared to white patients. Furthermore, admission in the public health sector (aOR 1.5, 95% CI 1.5, 1.6) was associated with increased risk of mortality compared with admission to the private sector (Table 4). Other factors associated with in-hospital mortality were ages of 20-39 years (aOR 3.1, 95% CI 2.7, 3.6), 40-59 years aOR 8.6, 95% CI 7.4, 9.9), 60-79 years (aOR 19.4, 95% CI 16.8, 22.2) and >80 years (aOR 35.2, 95% CI 30.6, 40.6) compared to <20 years; male sex (aOR 1.3, 95% CI 1.3, 1.4); hypertension (aOR 1.1, 95% CI 1.0, 1.1), diabetes (aOR 1.4, 95% CI 1.3, 1.4), chronic cardiac disease (aOR 1.2, 95% CI 1.1, 1.3), chronic kidney disease (aOR 1.6, 95% CI 1.5, 1.7), malignancy (aOR 1.6, 95% CI 1.4, 1.9), HIV (aOR 1.3, 95% CI 1.2, 1.4), current TB (aOR 1.4, 95% CI 1.2, 1.6), and current and past TB (aOR 1.4, 95% CI 1.2, 1.6) compared to no history of or current TB. Also, being hospitalised in the Eastern Cape (aOR 1.9, 95% CI 1.8, 2.0), Free State (aOR 1.3, 95% CI 1.3, 1.4), Gauteng (aOR 1.4, 95%CI 1.4, 1.5), KwaZulu-Natal (aOR 1.5, 95% CI 1.4, 1.6), Limpopo (aOR 1.7, 95% CI 1.6, 1.9), Mpumalanga (aOR 1.4, 95% CI 1.3, 1.5), North West (aOR 1.2, 95% CI 1.0, 1.2) and Northern Cape (aOR 1.4, 95% CI 1.3, 1.6) was associated with higher in-hospital mortality compared with hospitalisation in the Western Cape. Individuals also had higher risk of mortality if admitted during the second wave (aOR 1.5, 95% CI 1.4, 1.5) or third wave (aOR 1.3, 95% CI 1.3, 1.4), but lower risk of mortality if admitted during the fourth wave (aOR 0.4, 95% CI 0.3, 0.4) compared with admission during the first wave. Factors associated with COVID-19 mortality amongst respective race groups are presented in Supplementary table 1.
Health services characteristics of cases of COVID-19 admissions
Overall, there were more admissions in the public sector (232 615; 52.9%) than in the private sector (206 833; 47.1%) (p<0.001; Table 5). Furthermore, people of Indian descent (10 880; 75.0%) (p<0.001) and white people (25 862; 79.2%) (p<0.001) were more likely to be hospitalised in the private sector than in the public sector. Compared to other race groups, a lower percentage of black African patients were treated in ICU (9.0%) (p<0.001), in high care (8.2%) (p<0.001) or were ventilated (5.1%) (p<0.001), whilst a higher percentage of white patients were treated with supplemental oxygen (61.6%) (p<0.0001).
Overall, there was a higher percentage of individuals treated in ICU in the private (45 792/206 833; 22.1%) compared to the public sector (12 550/232 615; 5.4%), across all age groups >20 years (p<0.001 for all); and across all race groups (p<0.001 for all) (Table 6). The percentage treated in ICU was highest among individuals aged 40-59 years in the public sector (4760; 6.4%) and among 60-79 years in the private sector (17 171; 29.3%). The lowest percentage of people treated in ICU were black African, in both the public (8435; 5.3%) and private sectors (10 982; 19.4%) (p<0.001 for both). The highest percentage treated in ICU in the public and private sectors were people of Indian descent (10.1% and 24.4%) and white people (8.8% and 23.3%).
There was a higher percentage of individuals ventilated in the private (19 800/206 833; 9.6%) compared to the public sector (7818/232 615; 3.4%) overall and across all age groups >20 years (p<0.001 for all). A higher percentage of individuals were ventilated in the private sector across all race groups (p<0.001 for all) except for those of Indian descent for whom a similar percentage were ventilated in public and private sectors (Table 6). In the public sector, the lowest percentage of patients ventilated were black African (6213; 3.9%) and the highest percentages were those of Indian descent (308; 8.5%) and white (477; 7.0%). In the private sector, the lowest percentage of patients ventilated were black African (4833; 8.5%) and those of Indian descent (924; 8.5%) and the highest percentage ventilated were coloured (956; 10.7%).
There was a higher percentage of individuals who received supplemental oxygen in the private (95 703/206 833; 46.3%) compared to the public sector (87 023/232 615; 37.4%), overall and across all age groups >20 years (p<0.001 for all) (Table 6). In the public sector, the lowest percentage of patients who received supplemental oxygen were black African (73 800; 46.4%) and the highest percentage who received supplemental oxygen were those of Indian descent (2096; 57.9%).
In the private sector, the lowest percentage of patients who received supplemental oxygen were black African (24 658; 43.6%) and the highest percentage who received supplemental oxygen were white (16 374; 63.3%).
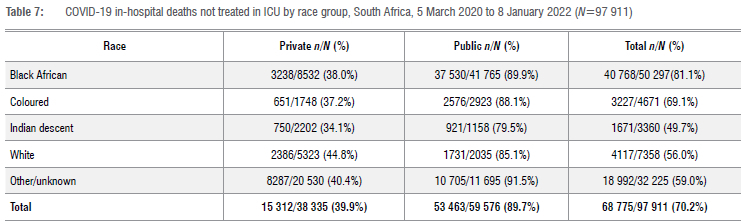
Of all the COVID-19 patients who died in hospital, 68 775/97 911 (70.2%) were not treated in ICU, which differed by sector: 39.9% in the private sector and 89.7% in the public sector were not treated in ICU (Table 7). There was also a difference by race group, with black African (3238; 38.0%) and white (2386; 44.8%) decedents having the highest percentage of non-ICU treatment in the private sector; and black African (37 530; 89.9%) highest in the public sector.
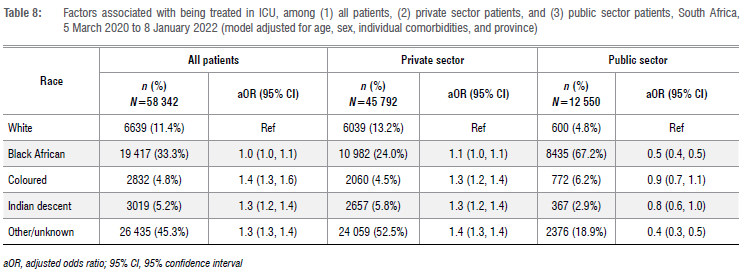
On multivariate analysis, adjusting for age, sex, individual comorbidities and province, in the private sector, there were increased odds of being treated in ICU for black African (aOR 1.1; 95% CI 1.0, 1.1) and coloured (aOR 1.3; 95% CI 1.2, 1.4) patients and patients of Indian descent (aOR 1.3; 95% CI 1.2, 1.4) compared to white patients. In contrast, in the public sector, there were decreased odds of being treated in ICU for black African patients (aOR 0.5; 95% CI 0.4, 0.5) compared to white patients (Table 8). Similar trends were observed for ventilation of patients (Table 9).
Discussion
While the associations of age, sex and race with risk of COVID-19 mortality have been well established, our study reveals insights into the intersection of age, gender, race, and SES (using health sector of admission as a proxy) with COVID-19 mortality in South Africa. We propose that the COVID-19 mortality disparities revealed in this study were due to multiple intersecting risk factors affecting COVID-19 exposure, susceptibility to infection, and differences in access to care, as reported in other studies.19,20 These risk factors have underlying structural and social determinants which the World Health Organization defines as 'the conditions in which people are born, grow, work, live, and age and people's access to power, money and resources'21. Attributing poor clinical outcomes in vulnerable race groups solely to genetics and biological differences has historically been responsible for marginalising their health needs.
Higher risk of mortality among non-white patients
The risk for in-hospital COVID-19 death was increased in individuals of non-white race. Systematic reviews have confirmed the higher risk of mortality among black, Asian and minority ethnicities (BAME) even after adjusting for confounders such as age, sex and comorbidities.6,8,9 Even in low- and middle-income countries (LMIC), non-white people with COVID-19 who were admitted to hospital had significantly higher risk of mortality.22 This disparity in COVID-19 deaths by race was present in our study among all age groups, and even among younger individuals who have low risk of COVID-19 mortality overall, non-white individuals exhibited higher mortality rates than white individuals, similar to another study23.
There is currently little evidence that genetics, immunology or blood groups explain the racial and ethnic disparities in COVID-19 infection and severity.23 Angiotensin-converting enzyme 2 (ACE2) appears elevated in African Americans23 and Asians24, which could place them at higher risk for COVID-19 severe disease.
Higher prevalence of comorbid disease may play a role in the increased severity of COVID-19 among non-white individuals.25,26 BAME populations have a disproportionate burden of diabetes, cardiovascular disease, asthma, HIV, morbid obesity, liver disease, and kidney disease.19,23,26-29 The risk of comorbidities results from generations of exposure to racial inequities, environmental hazards, and social factors such as food insecurity, which result in changes in the microbiome and localised inflammation, and contribute to the development of long-term stress, which results in compromised immunity, thus increasing the risk for comorbidities and perpetuating adverse health outcomes.19,20,23,30
We found a sex differential in mortality rates, with incidence of mortality higher in female individuals <40 years and in male individuals >40 years. Increased oestrogen in female individuals is associated with improved immune function and reduced risk of viral infections compared to male individuals.24 Severe COVID-19 disease in male individuals could be explained by androgen regulation of expression of both ACE2 and TMPRSS2, an endothelial cell surface protein that is involved in the viral entry and spread of SARS-CoV-2.23,24
In other studies, the overall male to female mortality sex ratio was not equal at all ages31 and in one study was significantly higher among women, particularly in the 40-49-year age group32. The observed sex differences are complex, and intersectional analyses are required to understand risk factors that change with both sex and age, including differences in occupation, lifestyle (including smoking and alcohol use), comorbidities and health seeking behaviour, amongst others.24,31,32 We need to consider the impact of gender and its social and cultural characteristics rather than only the biology of sex.
In our study, even within race groups, the risk for mortality differed by age and sex. Race-specific risk estimates are likely not fixed in men and women or by age group, requiring statistical analysis stratified by effect modifiers rather than adjusting for them in regression models.33 The gendered disparities in COVID-19 is another important point of consideration given the multiple intersecting layers of oppression and marginalisation amongst women, especially black African women. During the pandemic, women in South Africa, especially women of colour, struggled to find shelter as they tackled poverty, unemployment, gender-based violence and food insecurity. In the USA, 'non-white' women have borne the greatest burden of COVID-19 disease and the socio-economic consequences of the pandemic.30
Higher mortality in young in LMIC
The risk of mortality increased with age, but there were proportionately more COVID-19 deaths reported among young people in South Africa compared to those in high income countries (HIC). Globally, deaths in individuals younger than 70 years accounted for 13% of all deaths in HIC and 63% in LMIC.34 In our analysis, 67% of deaths were in people younger than 70 years. The COVID-19 mortality rate for those aged 70-79 is 12.6 times the rate for those aged 50-59 in HIC, 3.5 times in LMIC and 1.8 times in our study. This pattern holds overall as well as separately for male and female mortality rates.34 The probability of a COVID-19 patient dying at age 40-49 years in a developing country is statistically similar to dying at age 60-69 in a rich country.35 This difference is only partly related to differences in population age structure. Poorer outcomes in developing countries are driven by a higher prevalence of comorbid conditions, and by challenges in access to hospitals and critical care.35
Socio-economic status
Higher COVID-19 mortality in non-white groups may be attributable to increased risk of infection amongst these communities.25,28 Our data revealed that most hospital admissions occurred amongst non-white people of working age - reflecting historical patterns of disadvantage that remain today. Admissions incidence was highest among working age individuals in non-white groups, and in older individuals among white people. Admissions were higher in female individuals in black and coloured groups, and higher in male individuals in Indian and white groups. A higher percentage of total admissions in the first wave were among black people, who may have been most severely hit in the early part of the pandemic due to employment in essential services, while other race groups were better able to shield and adopt measures for prevention and isolation, and access health services. In South African national blood service sero-surveys, sero-prevalence has been reported to be consistently higher among black African individuals.36 Socio-economic factors among non-white groups - including poverty; unemployment; poor housing conditions; living in larger, multigenerational households; low level of education; as well as higher burden of underlying comorbidities; and poor access to health services - place them at increased risk for COVID-19 infection and death.8,11,22,25,27,29,37 Frontline workers in South Africa are mostly women and mostly non-white and, as in other settings, have less opportunity to work from home, and have increased risk of exposure to SARS-CoV-2 through work and commuting using public transport.25
Healthcare access
Inequality in access to health care may also be driving increased COVID-19 infection and mortality rates.9 Fewer black African people and more white people and those of Indian descent were admitted in the private sector, reflecting health insurance coverage by race group in South Africa, which was 10% in black, 17% in coloured, 52% in Indian and 73% in white groups.38 In the USA, minorities are also less likely to have health insurance, resulting in reduced healthcare access.28
Almost half (47%) of all admissions were in the private sector, despite only 16% of the population having access to medical insurance and private health care. This might be due to lower thresholds for admission in the private sector and to limited bed availability in the public sector, but is unlikely to be due to patients in the public sector having lower risk of severe disease requiring hospitalisation.
A lower proportion of patients in the public sector were treated in ICU, ventilated or treated with supplemental oxygen, which reflects inequity of resources between the public and private sectors, including hospital beds, healthcare workers and equipment such as oxygen and ventilators. In South Africa, the average spend in the private sector was six times higher than that in the public sector.39 Higher expenditure affords more healthcare specialists, hospitals, and expensive medicines and technology. A comparison of the quality of healthcare systems of 48 countries found that the South African private sector ranked sixth while the public sector ranked eighth from the bottom.40
There were also differences in treatment in ICU and ventilation by race and health sector. There was less inequality in treatment in the private sector where non-white groups with highest risk of mortality were most likely to be treated in ICU or ventilated. In the public sector, however, black African patients were less likely to have been treated in ICU and ventilated compared to white patients, despite having higher risk of mortality than white patients. The inequality could be due to black patients more likely accessing care in rural district hospitals that had no ICU or ventilators available. Of concern, this finding suggests possible rationing of care that unfairly disadvantaged black people in the public sector. In Brazil, ICU access was also considered to explain differences in mortality by ethnicity, with white patient more likely to be admitted to ICU than non-white patients.22
In South Africa, 47% of individuals in the 2018 general household survey reported facing constraints in access to health services, which showed bias towards the poor (63%) compared to the non-poor (36%).41 Black South Africans, living in rural areas, with lower education levels, being unemployed and poor, were least likely to report access and experienced long distances to the nearest healthcare facilities.41 The inequitable distribution of resources has an impact on 'the timeliness, range and quality of services provided to users' in public healthcare facilities.41 Even in HICs like the USA, African Americans and Latin Americans had lower levels of access to a health provider20, social and economic barriers to testing42, varying medication prescriptions28, and lower quality care for COVID-1929.
Race and racism
Race and SES were important determinants of access to health care during apartheid when health systems were fragmented and discriminatory; but racial differences continue to impact access to health care today.38 The consequences of structural inequality disproportionately affect vulnerable groups, who experience discrimination based on their race, gender, and SES. The pandemic has exposed pre-pandemic inequalities that illustrate multiple barriers to health care and historically disadvantaged groups remain most impacted by COVID-19.30 In addition, the relationship between structural inequality and COVID-19 disease susceptibility and severity are bidirectional; the impact of the pandemic within these communities has worsened inequities in education, housing, employment, income, and access to quality health care.43
Some argue that 'racism, not race, drives inequity' in COVID-19 infection and outcomes.43 The biomedical risk factors and social determinants that disproportionately influence COVID-19 morbidity and mortality within BAME communities, are linked partly to structural racism.29,37,44 'These processes are complex and systemic, underpinned by unequal power relations and beliefs, and operating at individual, community, and organisational levels, resulting in stigmatisation, discrimination, and marginalisation of ethnic minorities'6.
Limitations
This analysis had several limitations. Firstly, data quality in a surveillance system is dependent on the information submitted by healthcare facilities. Fields with the highest proportion of incomplete data included race (36%) and comorbidities (25-32%). The proportion with missing race information was similar to the 39% reported in a study in Brazil22, and the 26% in a large UK data set42. Analysis was restricted to those with complete data. It is possible that there were differences amongst those who were excluded with unknown race. Secondly, DATCOV does not collect socio-economic data on income, education, occupation, household size, etc. and so we were limited to examining SES using health sector of admissions as a proxy. We were therefore unable to take a nuanced approach to inferring associations of COVID-19 mortality with inequality. It is also possible that some patients with medical aid were admitted in the public sector and some without medical aid were admitted in the private sector; however, these are likely to be small numbers and should not affect analysis. Therefore, sector of admission is likely to be a robust proxy for SES. In addition, race in this analysis may serve as a proxy for SES rather than as a risk factor in itself. Thirdly, the hospital surveillance system has incomplete data on reason for admission and includes patients with COVID-19 symptoms and those who tested positive for SARS-CoV-2 incidentally when admitted for other reasons. There could have been changes over time in the criteria and thresholds for hospitalisation which could have influenced the analysis of treatment in ICU or with ventilation, but it is likely that these changes over time were similar across race groups. Fourthly, our analysis did not include out-of-hospital mortality, which probably underestimates the true impact of COVID-19, as healthcare access would likely be more constrained among patients who are not hospitalised, as was demonstrated in Brazil.22
Conclusion
This study adds to the evidence of inequalities in South Africa, revealing how different intersecting systems (age, sex, race, SES) influence healthcare utilisation and health outcomes for people with COVID-19. These findings demonstrate the importance of collecting and analysing data on SES alongside race data.45 This will ensure that disease control measures address the most marginalised groups affected by COVID-19.32 Public health efforts should be targeted towards vulnerable populations, taking into consideration the pre-existing inequities that predispose them to have poor disease outcomes and yet have more limited access to health interventions.44 The findings should also inform government efforts to provide inclusive non-discriminatory health services, and urgently improve access to ICU, ventilation and oxygen in the public sector.
Acknowledgements
We acknowledge the National Institute for Communicable Diseases (NICD) team responsible for reporting test, case and hospitalisation data. We are grateful to the laboratory staff, clinicians and data teams in all public and private sector hospitals throughout the country who report cases and hospitalisation data, and who are acknowledged and listed as the DATCOV author group: https://www.nicd.ac.za/diseases-a-z-index/covid-19/surveillance-reports/daily-hospital-surveillance-datcov-report/
Competing interests
We have no competing interests to declare.
Authors' contributions
W.J. and S.M. contributed to the literature search. W.J., L.B., C.C., L.O. and C.M. contributed to study design and refining methods of analysis. L.O., W.J. and R.W. contributed to data analysis, and creation of tables and figures. W.J., L.O. and S.M. contributed to data interpretation and writing the initial draft. W.J. drafted the initial manuscript and all other coauthors contributed scientific inputs equally towards the interpretation of the findings and the final draft of the manuscript. W.J., L.O., R.W. and C.M. verified the underlying data.
References
1. South African Department of Health. COVID-19 statistics in SA [webpage on the Internet]. No date [cited 2022 Feb 14]. Available from: https://www.health.gov.za/covid19/index.html [ Links ]
2. Madhi SA, Kwatra G, Myers JE, Jassat W, Dhar N, Mukendi CK, et al. South African population immunity and severe Covid-19 with Omicron variant [preprint]. medRxiv. 2021.12.20.21268096. https://doi.org/10.1101/2021.12.20.21268096 [ Links ]
3. South African Department of Health. COVID-19 statistics in SA [webpage on the Internet]. No date [updated 2021 Nov 25; cited 2022 Feb 14]. Available from: https://sacoronavirus.co.za/2021/11/25/update-on-covid-19-thursday-25-november-2021/ [ Links ]
4. South African Medical Research Council. Estimated number of excess natural deaths and death rates by province and metro, South Africa 2020/2021 (all ages) [webpage on the Internet]. No date [cited 2022 Feb 14]. Available from: https://www.samrc.ac.za./reports/report-weekly-deaths-south-africa [ Links ]
5. Nguyen NT, Chinn J, Ferrante MD, Kirby KA, Hohmann SF, Amin A. Male gender is a predictor of higher mortality in hospitalized adults with COVID-19. PLoS ONE. 2021;16, e0254066. https://doi.org/10.1371/journal.pone.0254066 [ Links ]
6. Sze S, Pan D, Nevill CR, Gray LJ, Martin CA, Nazareth J, et al. Ethnicity and clinical outcomes in COVID-19: A systematic review and meta-analysis. eClinicalMedicine. 2020;29, Art. #100630. https://doi.org/10.1016/j.eclinm.2020.100630 [ Links ]
7. Sasson I. Age and COVID-19 mortality: A comparison of Gompertz doubling time across countries and causes of death. Demogr Res. 2021;44:379-396. https://doi.org/10.4054/DemRes.2021.44.16 [ Links ]
8. Khanijahani A, Iezadi S, Gholipour K, Azami Aghdash S, Naghibi D. A systematic review of racial/ethnic and socioeconomic disparities in COVID-19. Int J Equity Health. 2021;20:248. https://doi.org/10.1186/s12939-021-01582-4 [ Links ]
9. Mackey K, Ayers CK, Kondo KK, Saha S, Advani SM, Young S, et al. Racial and ethnic disparities in COVID-19-related infections, hospitalizations, and deaths: A systematic review. Ann Intern Med. 2021;174(3):362-373. https://doi.org/10.7326/M20-6306 [ Links ]
10. Gershengorn HB, Patel S, Shukla B, Warde PR, Bhatia M, Parekh D, et al. Association of race and ethnicity with COVID-19 test positivity and hospitalization is mediated by socioeconomic factors. Ann Am Thorac Soc. 2021;18(8):1326-1334. https://doi.org/10.1513/AnnalsATS.202011-1448OC [ Links ]
11. Jassat W, Cohen C, Tempia S, Masha M, Goldstein S, Kufa T, et al. Risk factors for COVID-19-related in-hospital mortality in a high HIV and tuberculosis prevalence setting in South Africa: A cohort study. Lancet HIV. 2021;8:e554-e567. https://doi.org/10.1016/S2352-3018(21)00151-X [ Links ]
12. Statistics South Africa. Inequality trends in South Africa: A multidimensional diagnostic of inequality. Pretoria: Statistics South Africa, 2019. Available from: https://www.statssa.gov.za/publications/Report-03-10-19/Report-03-10-192017.pdf [ Links ]
13. Morudu P Kollamparambil U. Health shocks, medical insurance and household vulnerability: Evidence from South Africa. PLoS ONE. 2020;15, e0228034. https://doi.org/10.1371/journal.pone.0228034 [ Links ]
14. Statistics South Africa. Mid-year population estimates, 2020. Statistical release PO302. Pretoria: Statistics South Africa; 2021. Available from: http://www.statssa.gov.za/publications/P0302/P03022020.pdf [ Links ]
15. De Glanville WA, Thomas LF, Cook EAJ, De C. Bronsvoort BM, Wamae NC, Kariuki S, et al. Household socio-economic position and individual infectious disease risk in rural Kenya. Sci Rep. 2019;9:2972. https://doi.org/10.1038/s41598-019-39375-z [ Links ]
16. Marmot M. Social determinants of health inequalities. Lancet. 2005;365(9464):1099-1 104. https://doi.org/10.1016/S0140-6736(05)71146-6 [ Links ]
17. Coovadia H, Jewkes R, Barron P Sanders D, McIntyre D. The health and health system of South Africa: Historical roots of current public health challenges. Lancet. 2009;374:817-834. https://doi.org/10.1016/S0140-6736(09)60951-X [ Links ]
18. National Institute for Communicable Diseases (NICD). Proposed definition of COVID-19 wave in South Africa. Communicable Diseases Communiqué. 2021 Nov;20(11). Available from: https://www.nicd.ac.za/wp-content/uploads/2021/11/Proposed-definition-of-COVID-19-wave-in-South-Africa.pdf [ Links ]
19. Raine S, Liu A, Mintz J, Wahood W, Huntley K, Hazulla F. Racial and ethnic disparities in COVID-19 outcomes: Social determination of health. Int J Environ Res Public Health. 2020;17:8115. https://doi.org/10.3390/ijerph17218115 [ Links ]
20. Ruprecht MM, Wang X, Johnson AK, Xu J, Felt D. Evidence of social and structural COVID-19 disparities by sexual orientation, gender identity, and race/ethnicity in an urban environment. J Urban Health. 2021;98:27-40. https://doi.org/10.1007/s11524-020-00497-9 [ Links ]
21. World Health Organization (WHO). COVID-19 and the social determinants of health and health equity: Evidence brief. Geneva: WHO; 2021. Available from: https://www.who.int/publications/i/item/9789240038387 [ Links ]
22. Baqui P, Bica I, Marra V, Ercole A, Van der Schaar M. Ethnic and regional variations in hospital mortality from COVID-19 in Brazil: A cross-sectional observational study. Lancet Glob Health. 2020;8, e1018-26. https://doi.org/10.1016/S2214-109X(20)30285-0 [ Links ]
23. Carethers JM. Insights into disparities observed with COVID-19. J Internal Med. 2021;289:463-473. https://doi.org/10.1111/joim.13199 [ Links ]
24. Kopel J, Perisetti A, Roghani A, Aziz M, Gajendran M, Goyal H. Racial and gender-based differences in COVID-19. Front Public Health. 2020;8:418. https://doi.org/10.3389/fpubh.2020.00418 [ Links ]
25. Acosta AM, Garg S, Pham H, Whitaker M, Anglin O, O'Halloran A, et al. Racial and ethnic disparities in rates of COVID-19-associated hospitalization, intensive care unit admission, and in-hospital death in the United States from March 2020 to February 2021. JAMA Netw Open. 2021;1;4(10), e2130479. https://doi.org/10.1001/jamanetworkopen.2021.30479 [ Links ]
26. Laurencin CT, McClinton A. The COVID-19 pandemic: A call to action to identify and address racial and ethnic disparities. J Racial Ethn Health Disparities. 2020;7(3):398-402. https://doi.org/10.1007/s40615-020-00756-0 [ Links ]
27. Hooper MW, Nápoles AM, Pérez-Stable EJ. COVID-19 and racial/ethnic disparities. JAMA. 2020;323(24):2466-2467. https://doi.org/10.1001/jama.2020.8598 [ Links ]
28. Bhala N, Curry G, Martineau AR, Agyemang C, Bhopal R. Sharpening the global focus on ethnicity and race in the time of COVID-19. Lancet. 2020;395(10238):1673-1676. https://doi.org/10.1016/S0140-6736(20)31102-8 [ Links ]
29. Tai DBG, Shah A, Doubeni CA, Sia IG, Wieland ML. The disproportionate impact of COVID-19 on racial and ethnic minorities in the United States. Clin Infect Dis. 2021;72(4):703-706. https://doi.org/10.1093/cid/ciaa815 [ Links ]
30. Obinna DN. Confronting disparities: Race, ethnicity, and immigrant status as intersectional determinants in the COVID-19 era. Health Educ Behav. 2021;48(4):397-403. https://doi.org/10.1177/10901981211011581 [ Links ]
31. Bhopal S, Bhopal R. Sex differential in COVID-19 mortality varies markedly by age. Lancet. 2020;396:532-533. https://doi.org/10.1016/S0140-6736(20)31748-7 [ Links ]
32. Dehingia N, Raj A. Sex differences in COVID-19 case fatality: Do we know enough? Lancet Glob Health. 2021;9(1):e14-e15. https://doi.org/10.1016/S2214-109X(20)30464-2 [ Links ]
33. Islam N, Khunti K, Dambha-Miller H, Kawachi I, Marmot M. COVID-19 mortality: A complex interplay of sex, gender, and ethnicity. Eur J Public Health. 2020;30(5):847-848. https://doi.org/10.1093/eurpub/ckaa150 [ Links ]
34. Demombynes G. COVID-19 Age-mortality curves are flatter in developing countries. Policy research working paper 9313. Washington DC: World Bank Group; 2020. https://doi.org/10.1596/1813-9450-9313 [ Links ]
35. Chauvin JP, Fowler A, Herrera LN. The younger age profile of COVID-19 deaths in developing countries. IDB Working Paper Series IDP-WP-1154. Washington DC: Inter-American Development Bank; 2020. http://dx.doi.org/10.18235/0002879 [ Links ]
36. Sykes W, Mhlanga L, Swanevelder R, Glatt TN, Grebe E, Coleman C, et al. Prevalence of anti-SARS-CoV-2 antibodies among blood donors in Northern Cape, KwaZulu-Natal, Eastern Cape, and Free State provinces of South Africa in January 2021 [preprint]. Research Square. 2021 Feb 12:rs.3.rs-233375. https://doi.org/10.21203/rs.3.rs-233375/v1 [ Links ]
37. Figueroa JF, Wadhera RK, Mehtsun WT, Riley K, Phelan J, Jha AK. Association of race, ethnicity, and community-level factors with COVID-19 cases and deaths across U.S. counties. Healthcare. 2021;9:100495. https://doi.org/10.1016/j.hjdsi.2020.100495 [ Links ]
38. Mhlanga D, Garidzirai R. The influence of racial differences in the demand for healthcare in South Africa: A case of public healthcare. Int J Environ Res Public Health. 2020;17,5043. https://doi.org/10.3390/ijerph17145043 [ Links ]
39. Mclntyre D, Doherty J, Ataguba J. Healthcare financing and expenditure: Post-1994 progress and remaining challenges. In: Van Rensburg H, editor. Health and healthcare in South Africa. Pretoria: Van Schaik; 2012. p. 433-482. [ Links ]
40. Monitor Group. Health Systems Comparison Project. Cambridge: Mimeo; 2008. [ Links ]
41. Burger R, Christian C. Access to health care in post-apartheid South Africa: Availability, affordability, acceptability. Health Econ Policy Law. 2020;15:43-55. https://doi.org/10.1017/S1744133118000300 [ Links ]
42. Mathur R, Rentsch CT, Morton CE, Hulme WJ, Schultze A, OpenSAFELY Collaborative. Ethnic differences in SARS-CoV-2 infection and COVID-19-related hospitalisation, intensive care unit admission, and death in 17 million adults in England: An observational cohort study using the OpenSAFELY platform [with erratum 2021 May 6]. Lancet. 2021;397(10286):1711-1724. https://doi.org/10.1016/S0140-6736(21)00634-6 [ Links ]
43. Khazanchi R, Evans CT, Marcelin JR. Racism, not race, drives inequity across the COVID-19 continuum. JAMA Netw Open. 2020;3(9), e2019933. https://doi.org/10.1001/jamanetworkopen.2020.19933 [ Links ]
44. Ford CL. Commentary: Addressing inequities in the era of COVID-19. The pandemic and the urgent need for critical race theory. Family Commun Health. 2020;43(3):184-186. https://doi.org/10.1097/FCH.0000000000000266 [ Links ]
45. Chowkwanyun M, Reed AL. Racial health disparities and COVID-19 - Caution and context. N Engl J Med. 2021;383(3):201-203. https://doi.org/10.1056/NEJMp2012910 [ Links ]
 Correspondence:
Correspondence:
Waasila Jassat
Email:waasilaj@nicd.ac.za
Received: 21 Feb. 2022
Revised: 08 Apr. 2022
Accepted: 13 Apr. 2022
Published: 31 May 2022
Editor: Pascal Bessong
Funding: None


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}