










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Science
versión On-line ISSN 1996-7489
versión impresa ISSN 0038-2353
S. Afr. j. sci. vol.117 no.11-12 Pretoria nov./dic. 2021
http://dx.doi.org/10.17159/sajs.2021/8354
RESEARCH ARTICLE
Self-esteem and antiretroviral therapy adherence among young people living with HIV: An exploratory serial mediation analysis
Patrick NyamaruzeI; Kaymarlin GovenderII; Richard G. CowdenIII
IDiscipline of Psychology, School of Applied Human Sciences, University of KwaZulu-Natal, Durban, South Africa
IIHealth Economics and HIV and AIDS Research Division, University of KwaZulu-Natal, Durban, South Africa
IIIDepartment of Psychology, University of the Free State, Bloemfontein, South Africa
ABSTRACT
Capitalising further on the benefits of antiretroviral therapy (ART) for individual treatment requires an improved understanding of the psychological processes that may affect optimal ART adherence among people living with HIV. We examined internalised HIV/AIDS-related stigma and body appreciation as mediators of the association between self-esteem and ART adherence among young people living with HIV (YPLHIV). A sample of 76 YPLHIV (Mage = 19.36, s.d.age = 2.56; male 56.58%) residing in an HIV hyperendemic region of South Africa completed self-report measures of self-esteem, internalised HIV/AIDS-related stigma, body appreciation, and ART adherence. Path-analytic mediation modelling was performed to test for direct and indirect effects linking self-esteem with ART adherence. Results of serial mediation analyses indicated that self-esteem and ART adherence were indirectly associated through a two-step path of internalised HIV/AIDS-related stigma and then body appreciation, as well as a one-step path through internalised HIV/AIDS-related stigma. The results provide preliminary support for internalised HIV/AIDS-related stigma and body appreciation as mechanisms underlying the association between self-esteem and ART adherence. Implications of the findings for promoting ART adherence among YPLHIV are discussed.
SIGNIFICANCE:
• Self-esteem and ART adherence were indirectly related through internalised HIV/AIDS-related stigma followed by body appreciation.
• Outcomes of intervention initiatives designed to promote ART adherence among young people living with HIV may be further improved by integrating components that target internalised HIV/AIDS-related stigma and body appreciation.
Keywords: adolescents, young adults, HIV, HIV/ AIDS stigma, body perceptions, medication adherence
Introduction
Increased availability and uptake of antiretroviral therapy (ART) among people living with HIV (PLHIV) have played an important role in the decline of new HIV infections.1 ART promotes viral suppression, improves physical and emotional well-being, and reduces mortality.2 In regions of HIV hyperendemicity where it has been particularly challenging to stay on track with global treatment and prevention targets, ART uptake represents a key avenue for reducing the burden of HIV. However, the benefits of ART for preventing and treating HIV may be undermined by treatment non-adherence, which can lead to impairments in psychosocial functioning (e.g. weakening of social relationships and loss of self-esteem resulting from periods of illness), increase risk of HIV transmission to non-infected sexual partners, and is a common cause of death among PLHIV.3,4 To advance health promotion initiatives designed to improve ART adherence, further research is needed to identify and better understand salient mechanisms underlying ART non-adherence in populations residing in HIV hyperendemic contexts and for which unique social-structural vulnerabilities exist.
The burden of the global HIV epidemic is highest among young people living in the countries within eastern and southern Africa.5 Alongside the social-structural issues (e.g. inadequate health infrastructure) that pose challenges to HIV testing and treatment-related behaviour of young people living in the eastern and southern African region6, the effectiveness of HIV treatment in promoting the health and longevity of this population is highly contingent on the individual choices young people make about treatment-related behaviour. Wide-ranging reasons for non-adherence to ART have been reported among young people. The more frequently identified patient-related factors include perceived or internalised HIV/AIDS-related stigma7, body image concerns8, forgetfulness, alcohol use, and depression9. Patient-related factors are closest in proximity to the individual, many of which appear amenable to change through targeted efforts that are directed towards harnessing and developing personal resources of young people living with HIV (YPLHIV). Although various psychological resources (e.g. self-efficacy, resilience) have been linked to better ART adherence10,11, one underexplored avenue that also has the potential to promote ART adherence among YPLHIV is self-esteem.
Self-esteem is an important inner resource encompassing an individual's overall positive evaluation of the self, including perceived competence and sense of worth.12 Self-esteem has been conceptualised as a protective factor that contributes to better health and well-being by buffering the impact of negative and stressful life experiences.13,14 Research involving young people has revealed that self-esteem is associated with lower health risk behaviour (e.g. fewer sexual partners15, lower alcohol use16), which suggests that those with higher self-esteem might be more inclined to make choices that support rather than degrade health and well-being (e.g. adhere to medication regimens).
Few studies have investigated the association between self-esteem and ART adherence, which is important for several reasons. First, negative self-evaluation and a low sense of self-worth may affect concentration and memory, both of which are associated with ART non-adherence.17 For example, impairment in prospective memory (i.e. remembering to perform a specific task in the future) has been associated with ART non-adherence.18 Second, lower self-esteem is linked to increased alcohol misuse and recreational substance use, which can impair judgement and may interfere with a person's ability to adhere to treatment.16 Third, high self-esteem can precipitate resilience-promoting psychological qualities (e.g. self-confidence) that may enhance medication adherence.13 To further examine the association between self-esteem and ART adherence, in the present study we tested for evidence of internalised HIV/AIDS-related stigma and body appreciation as serial mechanisms linking self-esteem and ART adherence in a sample of South African YPLHIV.
Self-esteem and internalised HIV/AIDS-related stigma
Internalised HIV/AIDS-related stigma refers to the negative perceptions and abasement of the self that may be endorsed by those diagnosed with HIV.19 It is characterised by self-denigrating thoughts (e.g. self-blame) and feelings (e.g. shame, guilt), as well as concealment of HIV status.20 Internalisation of stigma is not an inevitable response to possession of a stigmatised attribute21, but the risk of such increases when existing beliefs about one's self-worth and self-regard are low. In particular, low self-esteem is associated with a higher likelihood of acquiring identity standards from society, appropriating perspectives about the self from others, and evaluating the self negatively.22
Although few studies have directly investigated the impact of self-esteem on internalised HIV/AIDS-related stigma, existing research indicates that self-esteem may protect against the negative effects that perceived or experienced stigma can have on internalisation of HIV/AIDS-related stigma.23 Some findings suggest that positive changes in self-esteem (e.g. increased self-worth) can play a role in adaptive resistance to HIV/ AIDS-related stigma (e.g. open disclosure of HIV seropositive status to confront negative labelling).24 Other evidence points to the risk of internalising HIV/AIDS-related stigma when self-esteem is low, which could have negative downstream implications for health and well-being.25,26
Internalised HIV/AIDS-related stigma and body appreciation
Internalised HIV/AIDS-related stigma may be pronounced when PLHIV have physical attributes that are common markers of the disease.27 Previous studies have established a link between internalised HIV/AIDS-related stigma and body image28, with one study reporting that high stigma significantly lowered the probability of having a positive body image29. Even in the absence of visible body changes, self-deprecating psychological processes that are attributable to internalised HIV/AIDS-related stigma (e.g. feelings of shame and worthlessness) can impact negatively on the body image perceptions of PLHIV.30
Internalised HIV/AIDS-related stigma may affect different dimensions of body image, including body appreciation. Body appreciation is a component of positive body image that is conceptualised as being respectful, approving, and appreciative of the characteristics and health of one's body, regardless of shape, weight, and imperfections.31 Internalising social norms and discriminatory characterisations towards PLHIV may have a negative effect on how PLHIV view and appreciate their bodies.27 The negative implications of internalised HIV/AIDS-related stigma may be especially pronounced among YPLHIV, given the complex interplay of biopsychosocial processes that occur during the developmental transition from childhood to adulthood.6
Body appreciation and antiretroviral therapy adherence
A variety of physical and psychological complications commonly accompany HIV infection, including weight loss, skin lesions, depression, suicidal ideation, and body dissatisfaction.32,33 Research suggests that fear of bodily changes (e.g. weight loss) resulting from HIV and ART may be implicated in medication non-adherence.8 Although there are few direct links between body appreciation and adherence, there is some evidence that improving the perspectives of PLHIV about their body can lead to better health behaviour, including adherence to ART.34 Extensive evidence indicates that body appreciation is associated with an appreciation of diverse appearances and shapes31, better physical health, and higher levels of psychological well-being35. Efforts to promote body appreciation may have implications for ART adherence among PLHIV, especially among young people who tend to be particularly susceptible to the influence of bodily perceptions on positive health behaviour.36
The present study
In this study, we examine associations between self-esteem, internalised HIV/AIDS-related stigma, body appreciation, and ART adherence in YPLHIV who reside in an HIV hyperendemic country within the eastern and southern African region. Exploring these interrelationships could offer an improved understanding of mechanisms that are implicated in ART adherence, particularly those that could be targeted to promote adherence in seropositive young people. Thus, we used an integrative modelling approach to explore internalised HIV/AIDS-related stigma and body appreciation as serial mechanisms linking self-esteem and ART adherence among YPLHIV in the Durban area of KwaZulu-Natal, South Africa. To our knowledge, this is the first study examining body appreciation as a mediator of this association, particularly as a precursor to ART adherence. We hypothesised that self-esteem and ART adherence would be linked indirectly via a sequential path of internalised HIV/AIDS-related stigma followed by body appreciation.
Method
Participants
The sample comprised 76 (56.58% male) seropositive young people residing in the city of Durban, South Africa. Durban is located within the province of KwaZulu-Natal, which has the highest HIV prevalence rate in the country.37 Participants ranged from 15 to 24 years of age (Mage=19.36, s.d. = 2.56) and identified racially as African (82.89%) or coloured (17.11%). A majority of the sample had fulfilled high school equivalency requirements (67.11%) or completed post-secondary education (28.95%). A small proportion of the participants had not completed any formal education (3.95%). Almost half of the sample (52.63%) indicated that they had acquired HIV after birth from a source other than their mother (i.e. horizontal infection), and the remainder (47.37%) reported that they had been infected through mother-to-child transmission (i.e. vertical infection).
Measures
Rosenberg Self-Esteem Scale
The Rosenberg Self-Esteem Scale (RSES)12 is a 10-item measure of self-respect and self-acceptance. Items (e.g. 'I feel that I am a person of worth, at least on an equal plane with others') are rated using a four-point response scale (1 = Strongly disagree; 4 = Strongly agree), half of which are reverse scored. In this study, responses to all items were aggregated for a total raw score (range: 10 to 40). Findings of various studies support the construct validity of the RSES.38,39 Estimated internal consistency reported for the RSES in prior research has been >0.80.40
Internalised AIDS-Related Stigma Scale
The Internalised AIDS-Related Stigma Scale (IA-RSS)41 consists of six items that were adapted from the AIDS-Related Stigma Scale42 to measure negative self-perceptions and self-abasement about being a person living with HIV. Items (e.g. 'I hide my HIV status from others') are rated on a dichotomous response scale (0 = Disagree; 1 = Agree) and are summed for a total score ranging from 0 to 6. Higher scores indicate greater internalised HIV/AIDS-related stigma. Support for the construct validity of the IA-RSS has been evidenced through associations with indicators of mental health and well-being (e.g. depression, quality of life).19 Prior research involving samples of South Africans have revealed internal consistency values of >0.73 for the IA-RSS.41
Body Appreciation Scale-2
The Body Appreciation Scale-2 (BAS-2)43 contains 10 items that measure a person's perceptions of their body (e.g. acceptance, appreciation, inner positivity) and attention towards their body's needs through the adoption of healthy behaviours.43 Participants rate the items (e.g. 'I feel good about my body') using a five-point response scale (1 = Never; 5 = Always). Item responses are summed for a total score ranging from 10 to 50. Higher scores indicate greater levels of body appreciation. The BAS-2 has been cross-culturally validated in samples from diverse countries (e.g. China, England).44,45 Previous studies have reported internal consistency values of >0.80 for women and men44, and evidence supports the convergent, incremental, and discriminant validity of the BAS-243.
Morisky Medication Adherence Questionnaire
The Morisky Medication Adherence Questionnaire (MMAS-8)46 comprises eight items that assess patient adherence to medication for chronic conditions. The first seven items (e.g. 'When you feel like your symptoms are under control, do you sometimes stop taking your medicine') are rated using a dichotomous response format (0 = Yes; 1 = No). A five-point response format is used to rate the final item (e.g. 'How often do you have difficulty remembering to take all your medicine'), which is transformed to a dichotomous score prior to aggregation of item responses (0 = A; 1 = B-E). In this study, participants completed the MMAS-8 by referencing their adherence to ART medication. We aggregated responses to each of the MMAS-8 items for a total score ranging from 0 to 8, with higher scores reflecting greater adherence to ART. Evidence supports the psychometric utility of the MMAS-8 as a valid and reliable measure of medication adherence46, including ART adherence47. Previous research has reported internal consistency values of >0.75 for the MMAS-8, and the findings of several studies support the construct validity of the measure.46,48
Procedure
Ethical approval for this study was granted by the Humanities and Social Sciences Research Ethics Committee of the University of KwaZulu-Natal (HSS/0522/018D). Written permission was acquired from a local HIV youth centre to access YPLHIV who received ART from the organisation. A purposive, convenience sampling approach was used to recruit participants. Specifically, YPLHIV who presented at the youth centre to collect their monthly medication were invited by a team of researchers to participate in this study. Interested individuals were directed to a private administrative office where they were initially given details about the study purpose, the participation procedures, and ethical considerations (e.g. anonymity, confidentiality). Those who agreed to participate were invited to provide their written informed consent. With the assistance of the nurses at the youth centre, parents and legal guardians of potential participants below 18 years were informed of the research. Written parental consent was obtained on behalf of all legal minors who indicated their interest in participating. Written assent was also obtained from legal minors. The measures were administered in English, which participants completed in an office provided by the youth centre. The research team was present and available to address any questions or issues that arose during the course of the subjects' participation.
Results
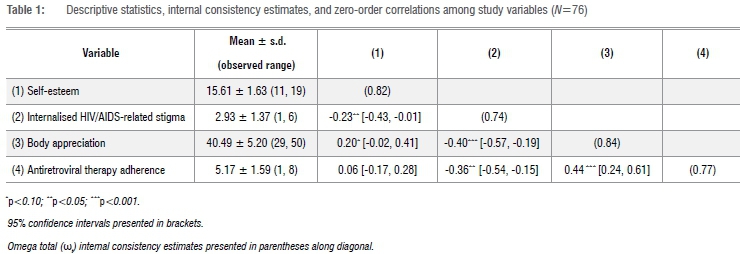
Statistical processing was performed using R.49 Study variables were initially screened for gross univariate and multivariate outliers. Standardised values for all variables were within acceptable limits (i.e. z < |3.29|)50, indicating there were no univariate outlier concerns. Mahalanobis distance (x2 (4) = 18.47, p<0.001) did not reveal any multivariate outliers (all D2values <11.92). Univariate skewness (max. = |0.86|) and kurtosis (max. = |0.76|) values indicated that all variables were approximately normal in distribution. Descriptive statistics, internal consistency estimates, and zero-order correlations among the study variables are reported in Table 1. Omega total (wt) estimates of internal consistency for all measures were >0.74. Self-esteem evidenced a small negative association with internalised HIV/AIDS-related stigma and a small positive association with body appreciation, but its association with ART adherence was negligible. Moderate negative associations were found linking internalised HIV/AIDS-related stigma with both body appreciation and ART adherence. There was a moderate positive association between body appreciation and ART adherence.
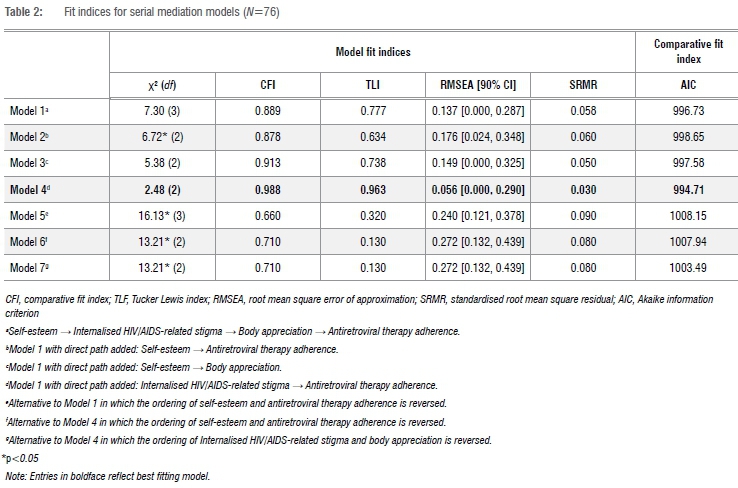
Path modelling procedures were performed using maximum likelihood estimation with robust standard errors. Evidence of mediation was tested using a global approach, which involves determining mediation effects after first establishing adequacy of model fit. Following existing recommendations51,52, model fit was evaluated using a combination of absolute, incremental, and residual-based fit indices. Specifically, we report the chi-square goodness-of-fit statistic (and its associated p-value), the comparative fit index, the Tucker Lewis index, the standardised root mean square residual, and the root mean square error of approximation. Along with the statistical significance of the chi-square test statistic (p>0.05), values of >0.90 for comparative fit index and Tucker Lewis index and values <0.10 for root mean square error of approximation and standardised root mean square residual were used as benchmarks to guide our evaluation of model fit.53,54 We also report the Akaike information criterion to allow comparisons between estimated models, with lower Akaike information criterion values indicative of a more favourable level of fit.55 Based on our theorising that internalised HIV/AIDS-related stigma and body appreciation would be serial mediators linking self-esteem with medication adherence, we began with the most parsimonious baseline full mediation model in which the association between self-esteem (X) and ART adherence (Y) was specified to occur via internalised HIV/AIDS-related stigma (M1) and then body appreciation (M2). Additional paths were sequentially integrated into subsequent models to determine whether less restrictive models were favoured over those that were more parsimonious. Because model estimation was based on cross-sectional data, a series of conceptually viable alternative models was also estimated.
Fit indices for all mediation path models are reported in Table 2. The baseline full mediation model (Model 1) in which internalised HIV/AIDS-related stigma and body appreciation were specified as serial mediators linking self-esteem with ART adherence evidenced an unsatisfactory level of fit. Inclusion of a direct effect between self-esteem and ART adherence (Model 2) worsened model fit. Although model fit improved when a path was added to Model 1 linking self-esteem with body appreciation (Model 3), there remained an unsatisfactory level of fit to the data. A substantial improvement in model fit was found by adding a path to Model 1 linking internalised HIV/AIDS-related stigma with ART adherence (Model 4). All model fit indices indicated that Model 4 had a satisfactory level of fit to the data and was identified as the best fitting model. We proceeded with comparing all alternative models to Model 4.
We compared Model 4 to variations of Models 1 and 4 in which the order of self-esteem and ART adherence was inverted (Models 5 and 6), as well as an alternative to Model 4 in which the order of internalised HIV/ AIDS-related stigma and body appreciation was interchanged (Model 7). Fit indices revealed that each of these alternative models had an unsatisfactory level of fit to the data. Akaike information criterion values also supported a superior level of fit for Model 4, which we retained as the best fitting model.
The standardised path coefficients for Model 4 are reported in Figure 1. There was a small negative association between self-esteem and internalised HIV/AIDS-related stigma. Internalised HIV/AIDS-related stigma evidenced a moderate negative association with body appreciation and a small negative association with ART adherence. A moderate positive association was found between body appreciation and ART adherence. Taken together, the findings are consistent with indirect-only mediation and suggest that self-esteem is indirectly associated with ART adherence via internalised HIV/AIDS-related stigma and body appreciation.
Discussion
The purpose of this study was to examine associations between self-esteem, internalised HIV/AIDS-related stigma, body appreciation, and ART adherence in a sample of YPLHIV in order to acquire further insight into potential pathways for promoting ART adherence among young people. As hypothesised, the results revealed that self-esteem and ART adherence were linked indirectly via a sequential path of internalised HIV/AIDS-related stigma followed by body appreciation. There was also evidence of a one-step indirect effect linking self-esteem with ART adherence via internalised HIV/AIDS-related stigma, although such an effect did not emerge for body appreciation. Overall, the results offer support for internalised HIV/AIDS-related stigma and body appreciation as mechanisms underlying the association between self-esteem and ART adherence.
The finding that self-esteem is not directly associated with ART adherence is consistent with a broader body of research on the mechanisms (e.g. counselling, social support) underlying the association between self-esteem and medication adherence.56 Evidence of a two-step indirect effect suggests that the sequential path of internalised HIV/AIDS-related stigma and then body appreciation represents one mechanism that accounts for the association between self-esteem and ART adherence. This sequential pathway can be interpreted in the context of existing conceptual models that highlight the role of low self-esteem in precipitating health risk behaviour. Conceptualising self-esteem within the framework of identity theory57, both the initial distress of receiving an HIV-seropositive diagnosis and the ongoing experience of living with HIV have the potential to disrupt the process of self-verification. Disturbances to self-verification can lead to a depletion of self-esteem, thereby reducing the capacity of self-esteem to operate as a buffer against stressors that emerge.21 Among YPLHIV, low self-esteem may increase vulnerability to internalised HIV/AIDS-related stigma that arises out of the self-deprecating consequences of evaluating the self against stigmatising social norms (e.g. promiscuity) about HIV.22 Internalisation of HIV/AIDS-related stigma is associated with fear of developing identifiable markers of the disease (e.g. lipodystrophy), which can heighten a person's sensitivity to bodily changes and increase bodily shame.29 Previous research has found that the psychological sequalae of body image disturbance (e.g. depression) can have negative implications for ART adherence8, suggesting that similar mechanisms may be involved in the association between body appreciation and ART adherence.
Taken together, the two-step indirect effect found in this study suggests that YPLHIV who receive support to reduce or protect against internalised HIV/AIDS-related stigma may benefit by experiencing higher levels of body appreciation, which in turn could lead to better ART adherence.
A unique contribution of this study to the evidence on ART adherence among YPLHIV is the inclusion of body appreciation as a sequential mechanism through which self-esteem and ART adherence are linked. A previous study highlighted the importance of identifying mechanisms by which internalised HIV/AIDS-related stigma is associated with ART adherence to enhance the efficacy of treatment approaches for improving treatment adherence.58 Based on the findings of this study, other intrapersonal (e.g. depression) and interpersonal (e.g. social support) factors that could affect ART adherence among YPLHIV should be targeted alongside body appreciation issues to promote ART adherence.
The finding of a two-step indirect effect via internalised HIV/AIDS-related stigma and then body appreciation was supplemented by a one-step indirect effect via internalised HIV/AIDS-related stigma, which aligns with prior research involving self-esteem, internalised stigma, and medication adherence.23 Considering the findings of this study did not support a one-step mediating effect for body appreciation, internalised HIV/AIDS-related stigma appears to play a key role in linking self-esteem and ART adherence. Should the availability of resources for promoting ART adherence be limited by infrastructure or economic constraints, treatment approaches targeting ART adherence might consider prioritising internalised HIV/AIDS-related stigma over body appreciation.
Practical implications
Although longitudinal evidence is needed to build on this study, the findings suggest that intervention initiatives targeting internalised HIV/ AIDS-related stigma and body appreciation may offer viable pathways for improving ART adherence. Several standalone interventions have successfully addressed internalised HIV/AIDS-related stigma and body appreciation in isolation. Cognitive-behavioural therapy approaches have been effective at reducing internalised HIV/AIDS-related stigma by challenging maladaptive patterns of thinking and building internal self-regulatory resources (e.g. coping skills) to manage stigma.59 Fitness training interventions60 have been successful at improving body image perceptions (including body appreciation and satisfaction with body functionality) and generalised self-efficacy by encouraging people to focus more on the functionality of their body and less on their appearance. Many of these standalone approaches could be integrated into interventions that incorporate other key components (e.g. social support) to provide a multi-pronged and more comprehensive approach to targeting ART adherence decisions and behaviours among YPLHIV.
Limitations and future research directions
The findings of this study offer additional insight into the mechanisms underlying the association between self-esteem and ART adherence, but there are several limitations to acknowledge. First, the cross-sectional nature of the data limits our ability to establish causal inferences and draw definitive conclusions about directionality. Although several models were compared to identify the best fitting model from the alternatives, longitudinal studies are needed to establish the directionality and causal pathways linking the variables included in this study. Second, the sample comprised a small, relatively homogeneous group of black African YPLHIV who were recruited from a single source located in a populous urban setting. Coupled with the purposive convenience sampling approach that was used to recruit participants, caution should be applied in generalising the findings to other populations of PLHIV. Additional research is needed to determine the replicability of the findings in specific populations, particularly among vulnerable young key populations. Third, effect estimates ranged from small to moderate61, and it is possible that the findings of this study are confounded by the omission of relevant variables that might exert a stronger mediating effect on the association between self-esteem and ART adherence (e.g. self-efficacy, autonomous motivation). Future studies might consider integrating additional variables into modelling procedures to explore the relative strength of alternative indirect mechanisms that link self-esteem with ART adherence. Along similar lines, further research is needed to identify other factors that may affect a person's experiences of bodily changes, attitude towards living with HIV, and ART adherence behaviour (e.g. socio-demographic factors, mode of HIV infection, length of time since HIV-seropositive diagnosis). Fourth, the findings should also be considered alongside the small sample of participants in this study. HIV remains a highly stigmatised health condition in South Africa and is a sensitive topic for many young people who often have concerns about the possible consequences of participating in research on HIV, including discrimination and having their HIV status further exposed.62 Only 63% of the YPLHIV who were approached consented to participate in this study, with many offering the aforementioned concerns as reasons for declining to participate.
Conclusion
In summary, the findings of the current cross-sectional study provide preliminary evidence of both one-step (through internalised HIV/ AIDS-related stigma) and two-step (through internalised HIV/AIDS-related stigma and then body appreciation) indirect effects linking self-esteem and ART adherence among YPLHIV. Notwithstanding the need to determine whether the results reported herein replicate in other key populations by employing more sophisticated methodological approaches, the findings raise the intriguing possibility of promoting ART adherence in young people through targeted intervention initiatives that seek to resolve internalised HIV/AIDS-related stigma and improve body appreciation.
Acknowledgements
We acknowledge the young participants in this study, without whom the study would not have been possible. We also thank the staff of the HIV youth centre who assisted us in gaining access to the respondents.
Competing interests
We have no competing interests to declare.
Authors' contributions
PN.: Conceptualisation; methodology; data collection; writing - the initial draft. K.G.: Conceptualisation; student supervision; critical revisions; R.G.C.: Conceptualisation; methodology; data analysis; data curation; student supervision; writing - revisions.
References
1. UNAIDS. 90-90-90: An ambitious treatment target to help end the AIDS epidemic [document on the Internet]. c2017 [cited 2020 Feb 10]. Available from: https://www.unaids.org/sites/default/files/sub_landing/90-90-90_en.pdf [ Links ]
2. Schaecher KL. The importance of treatment adherence in HIV. Am J Manag Care. 2013;19:S231-S237. [ Links ]
3. Nachega JB, Marconi VC, Van Zyl GU, Gardner EM, Preiser W, Hong SY et al. HIV treatment adherence, drug resistance, virologic failure: Evolving concepts. Infect Disord Drug Targets. 2011;11:167-174. https://doi.org/10.2174/187152611795589663 [ Links ]
4. Adejumo OA, Malee KM, Ryscavage P Hunter SJ, Taiwo BO. Contemporary issues on the epidemiology and antiretroviral adherence of HIV-infected adolescents in sub-Saharan Africa: A narrative review. J Int AIDS Soc. 2015;18(1):1-19. https://doi.org/10.7448/ias.18.L20049 [ Links ]
5. Govender K, Masebo WG, Nyamaruze P Cowden RG, Schunter BT, Bains A. HIV prevention in adolescents and young people in the Eastern and Southern African Region: A review of key challenges impeding actions for an effective response. Open AIDS J. 2018;12:53-67. https://doi.org/10.2174/1874613601812010053 [ Links ]
6. Cowden RG, Tucker LA, Govender K. Conceptual pathways to HIV risk in Eastern and Southern Africa: An integrative perspective on the development of young people in contexts of social-structural vulnerability. In: Govender K, Poku NK, editors. Preventing HIV among young people in Eastern and Southern Africa. New York: Routledge; 2020. p. 31-47. https://doi.org/10.4324/9780429462818-4 [ Links ]
7. Mutumba M, Bauermeister JA, Musiime V Byaruhanga J, Francis K, Snow RC, et al. Psychosocial challenges and strategies for coping with HIV among adolescents in Uganda: A qualitative study. AIDS Patient Care STDS. 2015;29:86-94. https://doi.org/10.1089/apc.2014.0222 [ Links ]
8. Blashill AJ, Goshe BM, Robbins GK, Mayer KH, Safren SA. Body image disturbance and health behaviors among sexual minority men living with HIV. Health Psychol. 2014; 33:677-80. https://doi.org/10.1037/hea0000081 [ Links ]
9. Shubber Z, Mills EJ, Nachega JB, Vreeman R, Freitas M, Bock P et al. Patient-reported barriers to adherence to antiretroviral therapy: A systematic review and meta-analysis. PLoS Med. 2016;13, e1002183. https://doi.org/10.1371/journal.pmed.1002183 [ Links ]
10. Henriksen IO, Ran0yen I, Indredavik MS, Stenseng F. The role of self-esteem in the development of psychiatric problems: A three-year prospective study in a clinical sample of adolescents. Child Adolesc Psychiatry Ment Health. 2017;11:68. https://doi.org/10.1186/s13034-017-0207-y [ Links ]
11. Zhang L, Li X, Lin Z, Jacques-Tiura AJ, Xu J, Zhou Y et al. Side effects, adherence self-efficacy, and adherence to antiretroviral treatment: A mediation analysis in a Chinese sample. AIDS Care. 2016;28:919-926. https://doi.org/10.1080/09540121.2015.1124984 [ Links ]
12. Rosenberg M. Society and adolescent child. Princeton, NJ: Princeton University Press; 1965. [ Links ]
13. Mann MM, Hosman CM, Schaalma HP, De Vries NK. Self-esteem in a broad-spectrum approach for mental health promotion. Health Educ Res. 2004;19:357-372. https://doi.org/10.1093/her/cyg041 [ Links ]
14. Hagen R, Havnen A, Hjemdal O, Kennair LE, Ryum T, Solem S. Protective and vulnerability factors in self-esteem: The role of metacognitions, brooding, and resilience. Front Psychol. 2020;11:1447. https://doi.org/10.3389/fpsyg.2020.01447 [ Links ]
15. Enejoh V, Pharr J, Mavegam BO, Olutola A, Karick H, Ezeanolue EE. Impact of self esteem on risky sexual behaviors among Nigerian adolescents. AIDS Care. 2016;28:672-676. https://doi.org/10.1080/09540121.2015.1120853 [ Links ]
16. Sileo KM, Kizito W, Wanyenze RK, Chemusto H, Reed E, Stockman JK, et al. Substance use and its effect on antiretroviral treatment adherence among male fisherfolk living with HIV/AIDS in Uganda. PLoS ONE. 2019;14(6), e0216892. https://doi.org/10.1371/journal.pone.0216892 [ Links ]
17. Zogg JB, Woods SPP Sauceda JA, Wiebe JS, Simoni JM. The role of prospective memory in medication adherence: A review of an emerging literature. J Behav Med. 2012;35:47-62. https://doi.org/10.1007/s10865-011-9341-9 [ Links ]
18. Poquette AJ, Moore DJ, Gouaux B, Morgan EE, Grant I, Woods SP, et al. Prospective memory and antiretroviral medication non-adherence in HIV: An analysis of ongoing task delay length using the memory for intentions screening test. J Int Neuropsychol Soc. 2013;19(2):155-161. https://doi.org/10.1017/S1355617712001051 [ Links ]
19. Tsai AC, Bangsberg DR, Bwana M, Haberer JE, Frongillo EA, Muzoora C, et al. How does antiretroviral treatment attenuate the stigma of HIV? Evidence from a cohort study in rural Uganda. AIDS Behav. 2013;17:2725-2731. https://doi.org/10.1007/s10461-013-0503-3 [ Links ]
20. Quinn DM. Issue introduction: Identity concealment: Multilevel predictors, moderators, and consequences. J Soc Issues. 2017;73:230-239. https://doi.org/10.1111/josi.12213 [ Links ]
21. Crocker J, Quinn DM. Social stigma and the self: Meanings, situations, and self-esteem. In: Heatherton TF, Kleck RE, Hebl MR, Hull JG, editors. The social psychology of stigma. New York: Guilford Press; 2000. p. 153-183. [ Links ]
22. Brown JD, Dutton KA, Cook KE. From the top down: Self-esteem and self-evaluation. Cogn Emot. 2001;15:615-31. https://doi.org/10.1080/02699930126063 [ Links ]
23. Visser M, Sipsma H. The experience of HIV-related stigma in South Africa. In: Liamputtong P editor. Stigma, discrimination and living with HIV/AIDS stigma, discrimination and living with HIV/AIDS. Dordrecht: Springer; 2013. p. 205-227. https://doi.org/10.1007/978-94-007-6324-1_12 [ Links ]
24. Goudge J, Ngoma B, Manderson L, Schneider H. Stigma, identity and resistance among people living with HIV in South Africa. SAHARA J. 2009;6(3):94-104. https://doi.org/10.1080/17290376.2009.9724937 [ Links ]
25. Bernier A, Benmoussa A, Hilali MK, Henry E, Otis J, Loukid M, et al. Self-esteem and HIV infection in Morocco: Associated factors among people living with HIV - Results from a community-based study. Community Ment Health J. 2019;55(8):1402-1410. https://doi.org/10.1007/s10597-019-00394-9 [ Links ]
26. Pantelic M, Shenderovich Y, Cluver L, Boyes M. Predictors of internalised HIV-related stigma: A systematic review of studies in sub-Saharan Africa. Health Psychol. Rev. 2015;9(4):469-490. https://doi.org/10.1080/17437199.2014.996243 [ Links ]
27. Varas-Díaz N, Toro-Alfonso J, Serrano-García I. My body, my stigma: Body interpretations in a sample of people living with HIV/AIDS in Puerto Rico. Qual Rep. 2005;10:122-142. https://doi.org/10.1177/1049732304272059 [ Links ]
28. Zeng C, Li L, Hong YA, Zhang H, Babbitt AW, Liu C, et al. A structural equation model of perceived and internalized stigma, depression, and suicidal status among people living with HIV/AIDS. BMC Public Health. 2018;18:138. https://doi.org/10.1186/s12889-018-5053-1 [ Links ]
29. Palmer AK, Duncan KC, Ayalew B, Zhang W, Tzemis D, Lima V et al. "The way I see it": The effect of stigma and depression on self-perceived body image among HIV-positive individuals on treatment in British Columbia, Canada. AIDS Care. 2011;23:1456-1466. https://doi.org/10.1080/09540121.2011.565021 [ Links ]
30. Chapman E. Conceptualisation of the body for people living with HIV: Issues of touch and contamination. Sociol Health Illn. 2000;22:840-857. https://doi.org/10.1111/1467-9566.00233 [ Links ]
31. Tylka TL, Wood-Barcalow NL. What is and what is not positive body image? Conceptual foundations and construct definition. Body Image. 2015;14:118-129. https://doi.org/10.1016/j.bodyim.2015.04.001 [ Links ]
32. Nyamaruze P Govender K. "I like the way I am, but I feel like I could get a little bit bigger": Perceptions of body image among adolescents and youth living with HIV in Durban, South Africa. PLoS ONE. 2020;15, e0227583. https://doi.org/10.1371/journal.pone.0227583 [ Links ]
33. Bankole KO, Bakare MO, Edet BE, Igwe MN, Ewa AU, Bankole IA, et al. Psychological complications associated with HIV/AIDS infection among children in South-South Nigeria, sub-Saharan Africa. Cogent Med. 2017;4(1):1372869. https://doi.org/10.1080/2331205X.2017.1372869 [ Links ]
34. Lamb KM, Nogg KA, Safren SA, Blashill AJ. Mechanism of change in cognitive behavioral therapy for body image and self-care on ART adherence among sexual minority men living with HIV. AIDS Behav. 2018;22:2711-2717. https://doi.org/10.1007/s10461-018-2143-0 [ Links ]
35. Gillen MM. Associations between positive body image and indicators of men's and women's mental and physical health. Body Image. 2015;13:67-74. https://doi.org/10.1016/j.bodyim.2015.01.002 [ Links ]
36. Meland E, Haugland S, Breidablik HJ. Body image and perceived health in adolescence. Health Educ Res. 2007;22:342-350. https://doi.org/10.1093/her/cyl085 [ Links ]
37. Ramjee G, Sartorius B, Morris N, Wand H, Reddy T, Yssel JD, et al. A decade of sustained geographic spread of HIV infections among women in Durban, South Africa. BMC Infect Dis. 2019;19(1):1-9. https://doi.org/10.1186/s12879-019-4080-6 [ Links ]
38. Westaway MS, Jordaan ER, Tsai J. Investigating the psychometric properties of the Rosenberg self-esteem scale for South African residents of greater Pretoria. Eval Health Prof. 2015;38:181-199. https://doi.org/10.1177/0163278713504214 [ Links ]
39. Supple AJ, Su J, Plunkett SW, Peterson GW, Bush KR. Factor structure of the Rosenberg Self-Esteem Scale. J Cross-Cult Psychol. 2013;44:748-764. https://doi.org/10.1177/0022022112468942 [ Links ]
40. Ugoji FN. Determinants of risky sexual behaviours among secondary school students in Delta State Nigeria. Int J Adolesc Youth. 2014;19:408-418. https://doi.org/10.1080/02673843.2012.751040 [ Links ]
41. Kalichman SC, Simbayi LC, Cloete A, Mthembu PP, Mkhonta RN, Ginindza T. Measuring AIDS stigmas in people living with HIV/AIDS: The Internalized AIDS Related Stigma Scale. AIDS Care. 2009;21:87-93. https://doi.org/10.1080/09540120802032627 [ Links ]
42. Kalichman SC, Simbayi LC, Jooste S, Toefy Y Cain D, Cherry C, et al. Development of a brief scale to measure AIDS-related stigma in South Africa. AIDS Behav. 2005;9:135-143. https://doi.org/10.1007/s10461-005-3895-x [ Links ]
43. Tylka TL, Wood-Barcalow NL. The Body Appreciation Scale-2: Item refinement and psychometric evaluation. Body Image. 2015;12:53-67. https://doi.org/10.1016/j.bodyim.2014.09.006 [ Links ]
44. Halliwell E, Jarman H, Tylka T, Slater A. Adapting the Body Appreciation Scale-2 for children: A psychometric analysis of the BAS-2C. Body Image. 2017;21:97-102. https://doi.org/10.1016/j.bodyim.2017.03.005 [ Links ]
45. Swami V Ng SK, Barron D. Translation and psychometric evaluation of a standard Chinese version of the Body Appreciation Scale-2. Body Image. 2016;18:23-26. https://doi.org/10.1016/j.bodyim.2016.04.005 [ Links ]
46. Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. 2008;10:348-354. https://doi.org/10.1111/j.1751-7176.2008.07572.x [ Links ]
47. Saal W, Kagee A. The applicability of the Theory of Planned Behaviour in predicting adherence to ART among a South African sample. J Health Psychol. 2012;17:362-370. https://doi.org/10.1177/1359105311416875 [ Links ]
48. De las Cuevas C, PeñateW. Psychometric properties of the eight-item Morisky Medication Adherence Scale (MMAS-8) in a psychiatric outpatient setting. Int J Clin Health Psychol. 2015;15(2):121-129. https://doi.org/10.1016/j.ijchp.2014.11.003 [ Links ]
49. R Core Team. R: A language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2019. Available from: https://www.R-project.org/ [ Links ]
50. Tabachnick BG, Fidell LS. Using multivariate statistics. 6th ed. Boston, MA: Pearson; 2013. [ Links ]
51. Mueller RO, Hancock GR. Best practices in structural equation modeling. In: Osborne JW, editor. Best practices in quantitative methods. Thousand Oaks, CA: SAGE; 2008. p. 488-510. https://doi.org/10.4135/9781412995627.d38 [ Links ]
52. Worthington RL, Whittaker TA. Scale development research: A content analysis and recommendations for best practices. Couns Psychol. 2006;34:806-838. https://doi.org/10.1177/0011000006288127 [ Links ]
53. Hopwood CJ, Donnellan MB. How should the internal structure of personality inventories be evaluated? Pers Soc Psychol Rev. 2010;14:332-346. https://doi.org/10.1177/1088868310361240 [ Links ]
54. Weston R, Gore Jr PA. A brief guide to structural equation modeling. Couns Psychol. 2006;34:719-751. https://doi.org/10.1177/0011000006286345 [ Links ]
55. Burnham KP Anderson DR, Huyvaert KP. AIC model selection and multimodel inference in behavioral ecology: Some background, observations, and comparisons. Behav Ecol Sociobiol. 2011;65:23-35. https://doi.org/10.1007/s00265-010-1029-6 [ Links ]
56. Hussain S, Malik A, Hussain Z. A randomized controlled intervention trial: Effect of counselling on treatment adherence and self-esteem of women patients receiving tuberculosis treatment. Open Med. 2016;3:27-33. https://doi.org/10.2174/1874220301603010027 [ Links ]
57. Cast AD, Burke PJ. A theory of self-esteem. Soc Forces. 2002;80:1041-1068. https://doi.org/10.1353/sof.2002.0003 [ Links ]
58. Helms CB, Turan JM, Atkins G, Kempf MC, Clay OJ, Raper JL, et al. Interpersonal mechanisms contributing to the association between HIV-related internalized stigma and medication adherence. AIDS Behav. 2017;21:238-247. https://doi.org/10.1007/s10461-016-1320-2 [ Links ]
59. Tshabalala J, Visser M. Developing a cognitive behavioural therapy model to assist women to deal with HIV and stigma. S Afr J Psychol. 2011;41:17-28. https://doi.org/10.1177/008124631104100103 [ Links ]
60. Bassett RL, Ginis KA. Risky business: The effects of an individualized health information intervention on health risk perceptions and leisure time physical activity among people with spinal cord injury. Disabil Health J. 2011;4:165-176. https://doi.org/10.1016/j.dhjo.2010.12.001 [ Links ]
61. Cohen J. Statistical power analysis. Curr Dir Psychol Sci. 1992;1(3):98-101. https://doi.org/10.1111/1467-8721.ep10768783 [ Links ]
62. DiClemente RJ, Sales JM, Borek N. Barriers to adolescents' participation in HIV biomedical prevention research. J Acquir Immune Defic Syndr. 2010;54:S12-S17. https://doi.org/10.1097/QAI.0b013e3181e1e2c0 [ Links ]
 Correspondence:
Correspondence:
Patrick Nyamaruze
Email: nyamruzepatrick@yahoo.com
Received: 18 May 2020
Revised: 09 July 2021
Accepted: 22 July 2021
Published: 29 Nov. 2021
Editors: Pascal Bessong, Sandiswa Mbewana
Funding: None


{kind=link}
{kind=link}
{kind=link}