










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Science
versión On-line ISSN 1996-7489
versión impresa ISSN 0038-2353
S. Afr. j. sci. vol.117 no.11-12 Pretoria nov./dic. 2021
http://dx.doi.org/10.17159/sajs.2021/9328
RESEARCH ARTICLE
Determination of alcohols in hand sanitisers: Are off-the-shelf hand sanitisers what they claim to be?
Abdullahi A. Yusuf
Social Insects Research Group, Department of Zoology and Entomology, University of Pretoria, Pretoria, South Africa
ABSTRACT
Transmission of SARS-CoV-2 - the causative agent of COVID-19 - can be prevented through non-pharmaceutical interventions such as observing proper hand hygiene using alcohol-based hand rubs/sanitisers (ABHRs) as recommended by the WHO and local health authorities. However, this recommendation has led to high demand for ABHRs and proliferation of sub-standard products, which do not contain the recommended amount of alcohol. Fifty products of different origins and formulations obtained off-the-shelf and in public places in and around Pretoria (South Africa) were analysed for their alcohol content using gas chromatography. Ethanol was the most common alcohol used in the products, followed by isopropanol. Only 21 (42%) of the products analysed contained at least 70% alcohol; of these only 14 (28%) met the WHO recommended 80±5% alcohol content to have a virucidal effect on SARS-CoV-2. Of the 41 commercial off-the-shelf products analysed, 27 (66%) contained less than 70% alcohol in comparison to 13% of homemade products. Only 18% of gel products contained 70% alcohol, compared with 47% for liquid-based products. Most of the products did not contain the appropriate or correct declaration as recommended by the South African National Standards (SANS 289 and 490). The proliferation of substandard ABHRs is of great public health concern and calls for stricter regulations and enforcement in order to protect consumers, their rights and well-being during and post the COVID-19 pandemic period. However, in the interim, formulation of ABHRs using the WHO guidelines should be mandatory, as such formulations, when made correctly, do have the required virucidal effect against SARS-CoV-2.
SIGNIFICANCE:
• Commercial, off-the-shelf and public hand sanitisers were analysed to determine whether they contained enough alcohol to be efficacious virucides as recommended by the WHO.
• The majority of the products analysed were substandard, did not contain the recommended amount of alcohols and were not labelled correctly according to local and international standards.
• Homemade products conformed to a greater degree to the WHO standards for alcohol-based hand sanitisers. It is evident from these results that there is a need to monitor the manufacture of off-the-shelf products to ensure compliance and to assure consumers that products offer the required protection against SARS-CoV-2.
Keywords: alcohol contents, ABHRs, COVID-19, SARS-CoV-2, homemade hand sanitisers, gas chromatography
Introduction
In December 2019, an infectious disease named COVID-19 caused by a novel coronavirus (SARS-CoV-2)1 was first identified in Wuhan, Hubei Province, China2. By the beginning of 2020, COVID-19 had rapidly spread around the world, leading to it being declared a pandemic by the World Health Organization (WHO) on 11 March 2020. By December 2020, a year later, global COVID-19 cases had reached 65 million, with 1.5 million deaths, of which 800 000 and 21 000 cases and deaths were from South Africa, respectively2 - making South Africa among the countries with the highest per capita number of COVID-19 cases. Interrupting the chain of virus transmission using non-pharmaceutical interventions such as observing physical distancing, wearing of a face mask and maintaining good hand hygiene (washing hands with soap or the use of alcohol-based hand rubs/sanitisers (ABHR)) as recommended by the WHO and national health agencies remain the primary prevention options, especially given the slow pace of vaccination and the emergence of genetic variants of SARS-CoV-2. The recommendation that good hand hygiene should be practised led to stockpiling and hoarding of emergency supplies of hand sanitisers around the world - a phenomenon termed 'pandemic pantries' that resulted in the disappearance of these products from supermarket shelves.3 After the rush, and with easing of lockdown restrictions, the return to work, and legislation that made the provision of hand sanitisers at public places mandatory, many manufacturers, including chemical industries, breweries and perfumeries, began producing ABHRs.4 This demand drove the global hand sanitiser market valued at USD2.7 billion in 2019 up to USD3.3 billion in 2020, which is projected to reach USD13.7 billion by 2027.5 In South Africa, production facilities for the raw materials needed to make hand sanitisers experienced a nearly 400% increase in demand, opening the door to the introduction of substandard products, exploitation (inflated prices) and corruption leading to estimated overpricing to the level of ZAR66 million.6
The effectiveness of an ABHR depends on the type of alcohol it contains, the concentration and quantity applied to hands as well as the duration of exposure.7 ABHRs typically contain isopropyl alcohol (isopropanol), ethyl alcohol (ethanol), n-propanol or a combination of these alcohols.8 However, the two formulations recommended by the WHO are: Formulation I containing 80±5 % ethanol (v/v) and Formulation II containing 75±5 % isopropanol.9 Thus far, only ABHR formulations containing alcohols in the recommended concentrations by the WHO are shown to be effective against enveloped viruses including SARS-CoV-2.10-12 As effectiveness of an ABHR depends on its alcohol content, quality control is essential in order to maintain the integrity of the product and ensure that consumers are paying for and using products that have virucidal activity against COVID-19. It is therefore important to have easy and rapid methods to detect alcohols in ABHRs as well as to determine the alcohol content in commercial off-the-shelf ABHR products to ensure that the consumer is receiving an effective product. Hence, this study was undertaken with the following questions. Do the ABHRs sold or formulated in South Africa and those available in public places contain the required alcohol content to qualify as virucides? Are there differences between formulations (liquids and gels) in their alcohol content? Lastly, are ABHRs labelled appropriately as required by WHO and local standards set out in the South African National Standards SANS 289:2016 guide?13 To answer these questions, a rapid and reproducible gas chromatographic method was used to determine the alcohol content of both off-the-shelf and homemade liquid- and gel-based ABHRs found and used in different public places in Pretoria. The findings here are discussed in the context of COVID-19 prevention and beyond.
Materials and methods
Alcohol-based hand sanitisers
Commercially available liquid- and gel-based ABHRs hereafter 'off the shelf' were purchased from stores or sampled from hand sanitising points at public places (schools, offices, shopping malls, restaurants, places of worship) in and around Pretoria, Gauteng Province, South Africa. Another set of ABHRs that were made based on WHO recommendations for hand rubs using locally available ingredients at home by persons or in the laboratory for the daily use of personnel (hereafter referred to as 'homemade') were solicited from and provided by volunteers. The ABHRs were sampled directly from the container (in the case of those purchased) or collected in 1.5-mL sterile Eppendorf tubes. Overall, 50 ABHR products were analysed, of which 38 were liquids, 11 were gels and 1 was a spray-based formulation.
Gas chromatographic analysis of alcohols in ABHRs
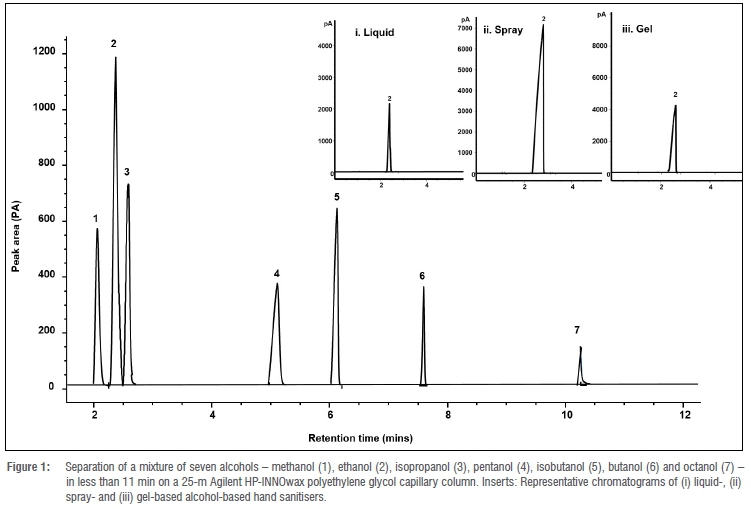
For the analysis, a 6890 Agilent gas chromatograph fitted with a flame ionisation detector and an Agilent HP-INNOWax polyethylene glycol (model number Agilent 19091N-102) column (25 m x 200 μm x 0.20 μm) was used. Samples were injected in the split mode with a split ratio of 30:1 at 140 °C and a pressure of 24.14 psi. The temperature of the flame ionisation detector was set at 200 °C, the flow rates for hydrogen, air and nitrogen were set at 40, 150 and 25 mL/min, respectively, and that of the carrier gas helium was set at 1.4 mL/min. The oven was programmed as follows: 35 °C for 1 min, increased by 5 ° per min to 40 °C, held for 1 min ramped at 15 °C to 75 °C with a 1 min hold and finally increased at 25 °C per min to 220 °C. To validate the method, a mixture of seven alcohols containing methanol, ethanol, isopropanol, pentanol, isobutanol, butanol and octanol was analysed. Thereafter, 1 μL of each ABHR was analysed on the gas chromatograph and the alcohol content quantified using an external calibration curve made up of either ethanol or isopropanol (the two main alcohols recommended by the WHO for use in ABHRs) in the range of 10-100% (v/v). The concentration of either ethanol or isopropanol was determined using the equation of the trend line , The equation of the trend line y=mx+c, where y = measured peak intensity of alcohol, m = gradient, x = unknown concentration of alcohol and c = intercept. As a reference and quality control standard check, a 91% ethanol standard was analysed with each batch of samples. All samples were analysed in duplicate and the composition of alcohols presented as mean proportions ± standard errors. Comparisons between ABHR formulation types and sources were made using a chi-square (X2) test of proportions using the Proc FREQ command in the statistical software SAS version 9.4 (SAS Inc, USA).
Results
Direct method for analysing alcohols in ABHRs
Using a direct gas chromatographic method for the analysis of alcohols in ABHRs, a mixture of seven alcohols was separated in less than 11 min (Figure 1). The two main alcohols used in ABHRs, ethanol and isopropanol, eluted from the column at 2.430 min and 2.530 min, respectively (Figure 2a and 2b).
Calibration curves prepared for both alcohols containing 10-100% (v/v) show a strong fit with coefficient of determination fi2-values of 0.999 and 0.992 for ethanol and isopropanol, respectively (Figure 2c and 2d). The 91% ethanol reference standard consistently had peak intensities with a mean of 114 716±190 over ten runs.
Alcohols and their composition in ABHRs
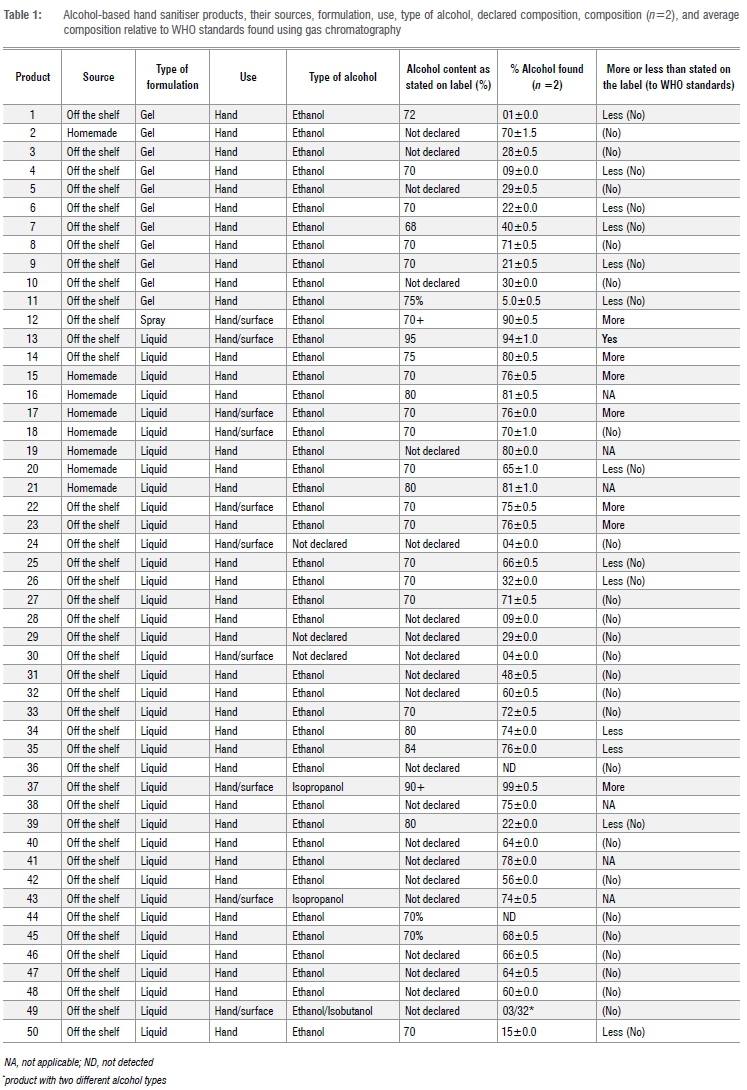
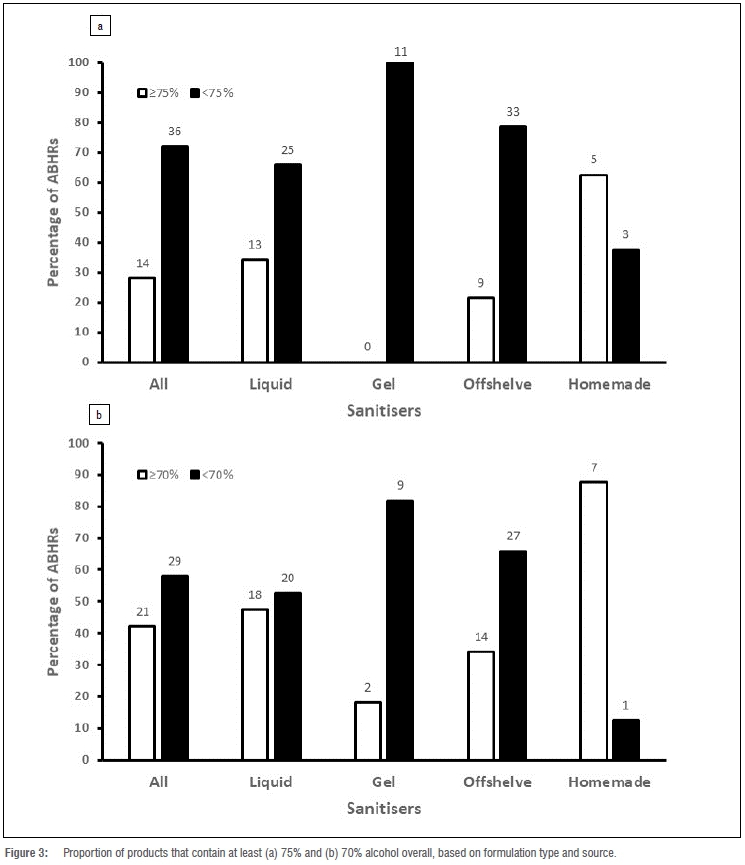
Ethanol was the main alcohol found in the ABHRs with the exception of products 37 and 43 which contained isopropanol, and product 49 with a combination of isobutanol and ethanol (Table 1). Methanol was not detected in any of the ABHRs. Only 14 (28%) of the 50 ABHRs analysed contained >75% alcohol (Figure 3a, Table 1). Looking at alcohol composition by formulation type, only 13 (34%) of the 28 liquids and the only spray-based formulation (product 12) contained >75% alcohol (Figure 3a, Table 1). Comparing the alcohol composition of ABHRs based on their sources (homemade vs off the shelf), 63% of homemade ABHRs met the >75% alcohol content criterion whilst only 21% of the off-the-shelf ABHRs met this criterion (X2=5.798, d.f.=1, p=0.0160, Figure 3a).
When the minimum alcohol composition was lowered to 70%, only 21 (42%) of the 50 ABHRs met this criterion, of which 18 (47%) and 2 (18%) are liquid and gel formulations, respectively (X2=7.268, d.f.=1, p=0.0070, Figure 3b). Only 14 (34%) of the off-the-shelf ABHRs contained at least 70% alcohol and 7 of the 8 homemade ABHRs (88%) met this criterion (X2=7.810, d.f.= 1, p=0.0052, Figure 3b).
Declaration and appropriate labelling
All the ABHRs analysed, with the exception of products 24, 29 and 30, had labels on which the type of alcohol(s) they contained were declared (Table 1). However, only 29 (58%) of the 50 products gave an indication of the composition of alcohols they contained (Table 1). Of these, 16 products (55%) did not contain the amount of alcohol as declared on the labels (Table 1). One product (product 37) which had isopropanol as its main component, contained up to 99%, which is above the recommended 70±5% for isopropanol-based ABHRs.
Discussion
A reproducible and direct method capable of detecting and separating the most commonly used alcohols in less than 11 min was used for the analysis of alcohols in hand sanitisers. This gas chromatographic method reduces analysis time and the need for complex sample preparation and offers the potential to increase throughput. Gas chromatography has previously been used for the determination of alcohols in ABHRs and application notes and methods such as those by Dhandapani14 and Berardi et al.15 are available. However, in these methods, alcohols, especially ethanol and isopropanol, were detected only after 4 minutes and were not directly sampled, hence increasing analysis time and the potential of introducing contaminants during sample preparation. Other analytical methods used for the determination of alcohols in ABHRs include Fourier transformed infrared spectroscopy for gel-based hand sanitisers.16
Most of the products analysed contained ethanol as their active ingredient, with only two found to contain isopropanol and one product contained a mixture of ethanol and isobutanol. Ethanol was the preferred alcohol over propanols for ABHR formulations because of its superior virucidal activity and its skin tolerance.17,18
A vast majority of the products analysed did not contain alcohols in the compositions recommended by the WHO (80±5 v/v% for ethanol and 70±5 v/v% for isopropanol).9 Most also did not contain the required 70% ethanol recommended by the US Centers for Disease Control and Prevention (CDC). Because alcohol content and concentrations are imperative3,7 for a sanitiser to have virucidal activity, these findings suggest that there is widespread lack of adherence to the required composition.
It is also noteworthy that only WHO Formulations I, II, and variations thereof have been tested and found to be effective against SARS-CoV-2.11 According to the WHO, an ABHR is 'an alcohol-containing preparation (liquid, gel or foam) designed for application to the hands to inactivate microorganisms and/or temporarily suppress their growth'9. Such preparations may contain one or more alcohols, and other active ingredients with excipients and humectants.19 Considering this definition, and putting it in the context of the findings here, most of the products analysed do not qualify as ABHRs, but rather are cosmetics15 because only products containing 70-95% alcohol have been shown to be able to denature the lipid and protein membranes of microorganisms20. It is only at 80% and 75%, respectively, for ethanol and isopropanol, that ABHRs are effective against emerging coronaviruses including SARS-CoV-2.10,11 The findings here also corroborate earlier warnings by Korsten and de Bruinn6 on the presence of fake hand sanitisers in the South African market and the need for South Africans to be protected against them.
In general, more liquid-based formulations were found to contain alcohols meeting the criteria for ABHRs in comparison to gel-based products. One reason for this is that liquid-based ABHR formulations are much easier to make in comparison to gel-based ones. For the former, ingredients are mixed based on volume per volume (v/v), while in the latter ingredients are measured based on weight per weight (w/w). Although gel-based ABHRs are preferred due to their ease of use on hands and the presence of residual ingredients21 such as perfumes. The efficacy of gel-based ABHRs is shrouded in controversy, with some studies showing no difference in their virucidal effect in comparison to those of liquid and foams22 and some indicating that they are less efficient23. Aside from the alcohol contents and presence of residuals, the type and viscosity of the gel3 used in the formulation also affects the delivery of the active ingredients in the required amounts, thus affecting virucidal activity. Even though making liquid-based formulations is easier, most of the off-the-shelf products analysed did not meet the criteria for ABHRs in comparison to homemade ABHRs that were formulated according to the WHO guidelines.9 The production and sale of products that do not qualify as ABHRs in South Africa could be traced to several factors, including shortages of sanitising products experienced prior to the national lockdown resulting from the declaration of the state of disaster. These shortages and demands from consumers saw hoarding and an increase in prices. The increase in prices then led to the opening up of a market niche (valued in millions of rands) that made many companies, including non-chemical, pharmaceutical, and breweries, turn to producing ABHRs. In addition, ethanol - the most preferred alcohol in available products -is not cheap; hence cutting corners through reducing its composition by 10-20% translates into an increase in profit margins.
Correct labelling and declaration of contents for ABHRs are required in accordance with standards set by WHO and local regulatory agencies. Unfortunately, of the 50 products analysed, more than half did not declare their contents or made declarations that were inaccurate. In South Africa, the South African National Standards SANS 289 stipulates that labels on pre-packaged products should include its identity, name, place and business of the manufacturer, packer, distributor, importer/ retailer and net quantity.13 Likewise, SANS guide 490 clearly stipulated similar requirements on disinfectant alcohol-based hand rub products.24 Practices involving non-declaration of contents and selling of products that are not of the required standard are infringing on consumer rights and are in contravention of the South African Consumer Protection Act 68 of 2008, which provides for fair, accessible products of high national and international standards. In addition, substandard ABHRs create a false sense of security about the efficaciousness of the products.
Conclusion
A direct rapid and reproducible gas chromatography method for the determination of alcohols in hand-based sanitisers that can be used for the quality control of ABHRs was developed and optimised. Most of the commercial alcohol-based products sold and made available to consumers in public places are sub-standard and do not contain the required amount of alcohol to be classified as effective virucides, especially against SARS-CoV-2, the causative agent of COVID-19. The presence of products that do not qualify as ABHRs, and are not appropriately labelled, on the market as well as in public places, poses a great risk to consumers in the wake of preventative measures against COVID-19, more so because hand hygiene and disinfection remains one of the most (if not the only) effective measure for mitigating the spread of the disease available at this time. Thus, using sub-standard products exposes the population unknowingly to the virus by increasing the chances of transmission through contaminated surfaces. There is therefore a need to put in place quality control measures, especially at the manufacturing, wholesale and retail levels to ensure that the consumer gets good-quality ABHRs that qualify as virucides, and which are appropriately labelled. Added to this is the need to test ABHRs and any product sold as such for its virucidal effect to confirm its efficacy. For now, in the absence of appropriate quality control measures, preparing ABHRs using the WHO guide for local formulations remains a better alternative to purchasing off-the-shelf products that are mostly sub-standard.
Acknowledgements
Thanks to volunteers who supplied hand sanitiser products and to colleagues for fruitful discussions on the idea to analyse hand sanitisers. Special thanks to Prof. Robin Crewe and Prof. Christian Pirk for reviewing an earlier version of the manuscript. Funding was provided for in part
by the South African National Research Foundation grant for Y-rated researchers, SARChI Chair in Mathematical Models and Methods in Bioengineering and Biosciences (M3B2) and the Alexander von Humboldt Foundation equipment grants. Views expressed in this article do not necessarily reflect the views of the funding bodies.
Competing interests
I have no competing interests to declare.
References
1. Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;383:727-733. https://doi.org/10.1056/nejmoa2001017 [ Links ]
2. Center for Systems Science and Engineering (CSSE) Johns Hopkins University. Coronavirus COVID-19 global cases [webpage on the Internet]. c2020 [cited 2021 Oct 20]. Available from: https://coronavirus.jhu.edu/map.html [ Links ]
3. Berardi A, Perinelli DR, Merchant HA, Bisharat L, Bashetia IA, Bonacucina G, et al. Hand sanitisers amid CoViD-19: A critical review of alcohol-based products on the market and formulation approaches to respond to increasing demand. Int J Pherm. 2020;584, Art. #119431. https://doi.org/10.1016/j.ijpharm.2020.119431 [ Links ]
4. Bomgardner MM, Mullin R, Scott A. Stepping up to the hand sanitizer shortage. C&EN Global Enterprise. 2020;98(11):12. https://doi.org/10.1021/cen-09811-buscon1 [ Links ]
5. Grand View Research. Hand sanitiser market size, share and trend analysis report by product (gel, foam, liquid), by distribution channel (hypermarket & supermarket, drug store, speciality, store, online), by region, and segment forecasts, 2020-2027 [webpage on the Internet]. c2020 [cited 2020 Nov 23]. Available from: https://www.grandviewresearch.com/industry-analysis/hand-sanitizer-market [ Links ]
6. Korsten L, de Bruinn W. South Africans aren't being protected from fake sanitisers: what needs to be done. The Conversation. 2020 October 20. Available from: https://theconversation.com/south-africans-arent-being-protected-from-fake-sanitisers-what-needs-to-be-done-148128 [ Links ]
7. Todd ECD, Michaels BS, Holah J, Smith D, Greig JD, Bartleson CA. Outbreaks where food workers have been implicated in the spread of foodborne disease. Part 10: Alcohol-based antiseptics for hand disinfection and a comparison of their effectiveness with soaps. J Food Prot. 2010;73:2128-2140. https://doi.org/104315/0362-028X-73.11.2128 [ Links ]
8. Boyce JM, Pittet D. Guideline for hand hygiene in health-care settings: Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Infect Control Hosp Epidemiol. 2002;23:S3-S40. https://doi.org/10.1086/503164 [ Links ]
9. World Health Organization (WHO). Guide to local production: WHO-recommended handrub formulations. WHO/IER/PSP/2010.5 [webpage on the Internet]. c2010 [cited 2020 Nov 23]. Available from: https://www.who.int/publications/i/item/WHO-IER-PSP-2010.5 [ Links ]
10. Siddharta A, Pfaender S, Vielle NJ, Dijkman R, Friesland M, Becker B, et al. Virucidal activity of World Health Organization-recommended formulations against enveloped viruses, including Zika, Ebola, and emerging coronaviruses. J Infect Dis. 2017;215(6):902-906. https://doi.org/10.1093/infdis/jix046 [ Links ]
11. Kratzel A, Todt D, V'kovski P Steiner S, Gultom M, Thao T, et al. Inactivation of Severe Acute Respiratory Syndrome Coronavirus 2 by WHO-recommended hand rub formulations and alcohols. Emerg Infect Dis. 2020;26(7):1592-1595. https://dx.doi.org/10.3201/eid2607.200915 [ Links ]
12. Leslie RA, Zhou S, David RM. Inactivation of SARS-CoV-2 by commercially available alcohol-based hand sanitizers. Am J Infect Control. 2021;49(3):401-402. https://doi.org/10.1016/j.ajic.2020.08.020 [ Links ]
13. South African Bureau of Standards (SABS). South African National Standard. Labelling requirements for prepackaged products (prepackages) and general requirements for the sale of goods subject to legal metrology control. SANS 298: 2016 Edition 1.06. Pretoria: South African Bureau of Standards (SABS) Standards Division; 2016. [ Links ]
14. Dhandapani R. Fast analysis of alcohol based hand sanitisers by gas chromatography. Phenomenex [webpage on the Internet]. c2020 [cited 2020 Dec 10]. Available from: https://phenomenex.blog/2020/03/31/alcohol-based-sanitizers/ [ Links ]
15. Berardi A, Cenci-Goga B, Grispoldi L, Cossignani L, Perinelli DR. Analysis of commercial hand sanitisers amid COVID-19: Are we getting the products that we need? AAPS Pharm Sci Tech. 2020;21, Art. #286. https://doi.org/10.1208/s12249-020-01818-6 [ Links ]
16. Fernando SF, Brito L, Pimetel MF, Leal LB. Determination of ethanol in gel hand sanitisers using mid and near infrared spectroscopy. J Braz Chem Soc. 2020;31(9):1759-1763. http://dx.doi.org/10.21577/0103-5053.20200115 [ Links ]
17. Cartner T, Brand N, Tian K, Saud A, Carr T, Stapleton R et al. Effect of different alcohols on stratum corneum kallikrein 5 and phospholipase A2 together with epidermal keratinocytes and skin irritation. Int J Cosmetic Sci. 2017;39:188-196. https://doi.org/10.1111/ics.12364 [ Links ]
18. Tarka R Gutkowska K, Nitsch-Osuch A. Assessment of tolerability and acceptability of an alcohol-based hand rub according to a WHO protocol and using apparatus tests. Antimicrob Resist Infect Control. 2019;8, Art. #191. https://doi.org/10.1186/s13756-019-0646-8 [ Links ]
19. Gold NA, Mirza TM, Avva U. Alcohol sanitizer. StatPearls Publishing [webpage on the Internet]. c2020 [cited 2020 Nov 20]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513254/ [ Links ]
20. Jia Jing JL, Thong PY Rajendran JC, McCarthy JR, Tharmalingam N, Madheswaran T. Hand sanitizers: A review on formulation aspects, adverse effects, and regulations. Int J Environ Res Public Health. 2020;17(9), Art. #3326. https://doi.org/10.3390/ijerph17093326 [ Links ]
21. Kampf G, Kramer A, Suchomel M. Lack of sustained efficacy for alcohol-based surgical hand rubs containing 'residual active ingredients' according to EN 12791. J Hosp Infec. 2017;95:163-168. http://dx.doi.org/10.1016/j.jhin.2016.11.001 [ Links ]
22. Larson EL, Cohen BV Baxter KA. Analysis of alcohol-based hand sanitizer delivery systems: Efficacy of foam, gel, and wipes against influenza A (H1N1)) virus on hands. Am J Infect Control. 2012;40:806-809. https://doi.org/10.1016/j.ajic.2011.10.016 [ Links ]
23. Kramer A, Rudolph R Kampf G, Pittet D. Limited efficacy of alcohol-based hand gels. Lancet. 2002;359:1489-1490. https://doi.org/10.1016/S0140-6736(02)08426-X [ Links ]
24. South African Bureau of Standards (SABS). South African National Standard disinfectant alcohol-based handrub. SANS 490: 2013 Edition 1.1 Amdt 1. Pretoria; South Africa Bureau of Standards (SABS) Standards Division; 2013. Available from: https://ctfa.co.za/wp-content/uploads/2020/04/SANS490_disinfectant-hand-rub-Standards_Development.pdf [ Links ]
 Correspondence:
Correspondence:
Abdullahi Yusuf
Email: abdullahi.yusuf@up.ac.za
Received: 16 Dec. 2020
Revised: 24 June 2021
Accepted: 05 July 2021
Published: 29 Nov. 2021
Editor: Priscilla Baker
Funding: South African National Research Foundation, Alexander von Humboldt Foundation


{kind=link}
{kind=link}
{kind=link}
{kind=link}