










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Science
versión On-line ISSN 1996-7489
versión impresa ISSN 0038-2353
S. Afr. j. sci. vol.117 no.9-10 Pretoria sep./oct. 2021
http://dx.doi.org/10.17159/sajs.2021/8575
REVIEW ARTICLE
Meta-analysis of factors affecting prevalence estimates of HIV-associated neurocognitive disorder in sub-Saharan Africa
Martins C. NwekeI; Adaora J. OkemuoII; Ekezie M. UduonuII; Princewill I. UgwuIII; Chioma NwachukwuIII; Nombeko MshunqaneI
IDepartment of Physiotherapy, University of Pretoria, Pretoria, South Africa
IIDepartment of Medical Rehabilitation, University of Nigeria, Enugu, Nigeria
IIIDepartment of Physiology, University of Nigeria, Enugu, Nigeria
ABSTRACT
Successful treatment of HIV with anti-retroviral therapy (ART) is resulting in more people living with HIV-associated neurocognitive disorder (HAND). In sub-Saharan Africa, this calls for strategic planning and judicious allocation of scarce resources, which requires an accurate estimate of the prevalence of HAND. Estimates of the prevalence of HAND in sub-Saharan Africa vary greatly, between 18.8% and 88.3%. This variability may be explained by factors such as different diagnostic approach, neuromedical examination, ART status, sampling method, substance abuse, assessors' qualification, depression and outcome measure. Different methods of diagnosing HAND, different outcome measures and non-random sampling techniques make it almost impossible to accurately estimate the prevalence of HAND in sub-Saharan Africa, often resulting in overestimation of the burden of disease. Consumers of health research should consider certain study characteristics and exercise appropriate caution when interpreting burden of disease in sub-Saharan Africa, especially when pursuing policy shift. Underestimating the prevalence of HAND will certainly affect the capacity and speed of containment, while overestimating will draw unnecessary attention and result in the misallocation of scarce resources.
SIGNIFICANCE:
• The high prevalence of HAND in sub-Saharan Africa as estimated in this review calls for further research on the impact of HAND on activities of daily living and putative therapeutic modalities.
• We highlight which study characteristics should be critically checked when using prevalence estimates for the purpose of health policy and distribution of scarce resources in sub-Saharan Africa.
• By favouring certain factors, this review will guide HIV health researchers in which techniques should be used to estimate the burden of HAND. These factors may also apply to estimating the burden of other diseases in sub-Saharan Africa.
Keywords: HIV infection, neurocognitive disorder, prevalence, sub-Saharan Africa, study characteristics
Introduction
Human immunodeficiency virus (HIV)-associated neurocognitive disorder (HAND) is one of the most common neurological complications of HIV in the antiretroviral therapy (ART) era.1 The growing burden of HAND justifies a quintessential global response to address this important mental health challenge among people living with HIV (PLWHIV).2 Before ART was introduced in 1996, 20-30% of people with advanced HIV infection displayed symptoms of severe HAND3,4, with death occurring within 6 months5. In the ART era, the prevalence of HAND varies between 19% and 64%, averaging globally at about 50%.6-10 Without a doubt, widespread ART and early intensification with ART are associated with a remarkable drop in HIV-associated dementia.11 The prevalence of less severe but limiting forms of HAND has continued to increase.8,12 The rising prevalence of HAND is chiefly associated with HIV becoming a chronic disease because more people are surviving HIV with the use of ART13, often surviving into their late fifties14,15. The chronic nature of HIV has created new challenges for health policymakers and legislators.16 The neuropsychological complications associated with HIV need to be treated to secure a better well-being and adequate reintegration of PLWHIV into society. The symptoms of HAND include behavioural and cognitive difficulties such as memory loss, poor attention and concentration span, acalculia, poor information processing and inadequate multitasking resulting in poor executive function.17 Most PLWHIV contract the virus early in life, usually in their late thirties.18 Long-term treatment and inability to work may have severe economic consequences for many families. Impaired neurocognitive function further predisposes PLWHIV to low productivity, job losses, restricted social participation and poverty.19
The recent up-scaling of ART for PLWHIV in sub-Saharan Africa has been appreciable.20 Consequently, sub-Saharan African healthcare systems need to prepare for and address the surge of chronic complications of HIV such as HAND and accelerated ageing.20 This will provide a safe trajectory into older adulthood for PLWHIV -a privilege enjoyed by their HIV-seronegative counterparts. More than 50% of the global population of PLWHIV currently resides in sub-Saharan Africa despite comprising less than 10% of the world's population.21 To ensure a fair quality of life for PLWHIV in sub-Saharan Africa, insight and scholarship are needed for optimal allocation of limited resources. To achieve scholarship in strategic planning for PLWHIV, we need accurate and precise estimates of the prevalence of HAND in sub-Saharan Africa.22 Underestimating the prevalence of HAND may result in under-budgeting, whereas overestimating may impair the feasibility of such projects by deterring funding agencies. The prevalence of HAND in sub-Saharan Africa has been estimated in several studies11,23,24; however, conflicting findings may distort strategic planning.
Hence, there is need for a meta-analysis of the prevalence estimates of HAND in sub-Saharan Africa. Aside from our meta-analysis of HAND prevalence estimates, we explored the effect of different study characteristics such as diagnostic criteria, outcome measures, ART status and duration, assessors' qualifications, assessment of neuropsychological confounds and other factors on prevalence estimates. Researchers should be able to evaluate the quality of a study based on outcome measure used, the assessor's qualification, sampling technique and other study characteristics.22 The assessment of outcomes constitutes an important domain in clinical practice, and influences the success of strategic plans and treatment.25 We reviewed all published estimates of HAND in sub-Saharan Africa.
Materials and methods
Design
This is a systematic review of observation studies including retrospective surveys, cross-sectional studies and cohort studies, focussing on the effects of different outcome measures and assessors on prevalence estimates in sub-Saharan Africa. The protocol was structured using a hybrid of the preferred reporting items for systematic review and meta-analysis (PRISMA) checklist and the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guideline.26,27 The protocol was registered with Open Science Framework: https://osf.io/vb52y.28
Eligibility criteria
Study characteristics
This review included observational studies of epidemiological design written in English, irrespective of sample size and test statistics. Studies had to have been conducted in sub-Saharan Africa.
Participants: This review only included studies in which participants were diagnosed with HAND by a physician or trained person using instruments such as the international HIV dementia scale (IHDS), HIV dementia scale (HDS), Montreal Cognitive Assessment Scale, or neuropsychological battery tests. We included studies irrespective of whether neuropsychological confounds were assessed or whether activities of daily living were evaluated.
Intervention: Not applicable. This is a systematic review of epidemiological studies reporting prevalence of HAND in the sub-Saharan African region.
Control: We included studies irrespective of whether the study had a control group.
Outcomes: For each study, we assessed the estimated prevalence of HAND, sampling method, sub-Saharan African region, measuring instrument and assessors' qualification, neuromedical exam, depression screening, alcohol dependence and substance abuse.
Inclusion criteria
1. Studies conducted among PLWHIV in sub-Saharan Africa reporting prevalence of HAND
2. Studies conducted in which assessment tool and/or assessor's qualification was stated
3. Studies conducted between 2009 and 2019
Exclusion criteria
1. Studies conducted among PLWHIV in sub-Saharan Africa but not reporting on prevalence of HAND
2. Studies conducted in which assessment tool and/or assessor's qualification was not stated
3. Studies conducted before 2009
Information sources and search strategy
We searched the literature using several combinations of search terms from medical subject headings (MeSH), and keywords in the title, abstract and/or text of the articles. First, we did a pilot search in PubMed to establish the face sensitivity of the search strategy. The PubMed pilot search included various MeSH terms and keywords/free text terms generated from articles that were key to the research question. We conducted the pilot search using several combinations of the search terms. The most sensitive and specific terms were chosen and reported. The terms were adapted to the syntax and subject headings of the remaining databases. Finally, we searched the following databases: PubMed, MEDLINE, Academic Search Complete, CINAHL and PsycINFO. We also searched the reference lists of identified observational and review articles for relevant studies.
Study records and data management
We exported all literature search results into EndNote 8 and removed all duplicate articles. We screened all bibliographic records in EndNote 8 and then selected articles that met the inclusion criteria. We developed, piloted and refined screening forms that included eligibility questions to aid in the screening process.
Selection process
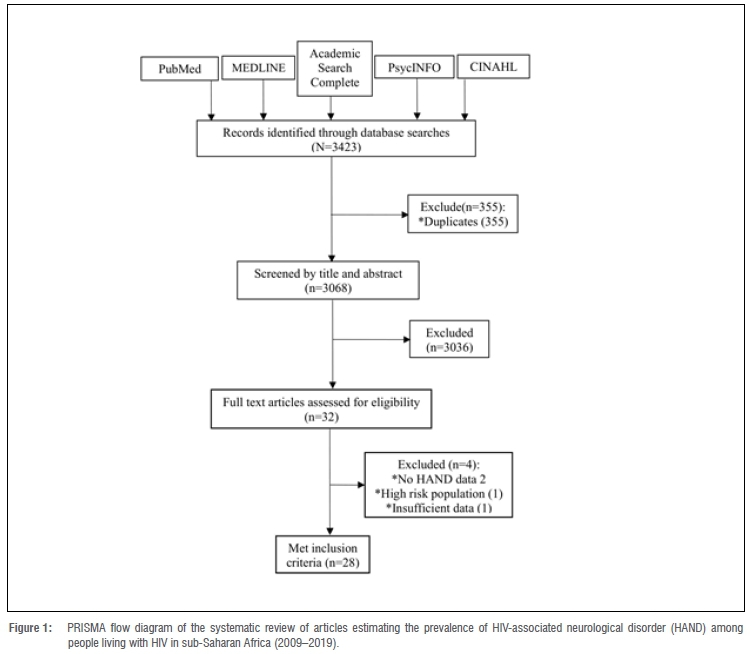
Initially, one author screened all the articles to identify those that met the inclusion criteria. The rest of the authors then applied the exclusion criteria simultaneously to the database. Any conflicts were then resolved until all authors agreed on the articles to be included. The primary author (MCN) critically cross-checked the initial screening results and read through the full texts of the selected studies for further screening to ensure that the eligibility criteria were met. We emailed the authors of selected studies to clarify issues that impacted on the selection of an article. Details of the flow of studies throughout the selection process, along with the reasons for exclusion, are presented using a PRISMA diagram (Figure 1).
Data collection process
Quality appraisal and risk of bias assessment
We assessed the quality and risk of bias of each article using the quality assessment checklist for prevalence studies adapted from Hoy et al.29 The checklist examines the appropriateness and adequacy of methodology, study design, participant recruitment, data collection, data analysis and presentation of findings. It is suitable for appraising most studies reporting prevalence. The tool contains 10 items/ questions with the 10th item being the summary score. Studies were classified as unclear when there was not enough information to evaluate the risk of bias. All the authors independently assessed the risk of bias, and the primary author (MCN) collated the results.
Data items
Data collected from each article were: authors' affiliations, participants' characteristics, inclusion criteria, exclusion criteria, study sample size, sampling methods, diagnostic criteria/method of assessment, ART status, duration on ART, country, region, instrument used, the assessors' qualification/experience, neuropsychological confounds and results/conclusions.
Data synthesis and assessment of heterogeneity
We used a random-effect model of meta-analysis to estimate the pooled prevalence estimates of HAND, as well as estimates for different measuring instruments and categories of assessors.30,31 Measures of heterogeneity, i.e. study characteristics, were sorted by year of publication and are presented in an evidence table (Table 1). Measure of heterogeneity, the Cochrane's Q statistics, and I2 were computed in line with Higgins and Thompson32. The I2-value was interpreted in line with the Cochrane Handbook for Systematic Reviews of Intervention as follows: 0-10% might indicate low heterogeneity, 30-60% may represent moderate heterogeneity, 50-90% may represent substantial heterogeneity, and 75-100% may indicate considerable heterogeneity.33
Ethical consideration
This review is related to a clinical trial approved by the Research Ethics Committee of the Faculty of Health Sciences, University of Pretoria (ethics reference number: 152/2020), which complies with the ICH-GCP guidelines and the US Federal wide Assurance.
Data analysis
The pooled prevalence of HAND was estimated using MedCalc. The effects of study characteristics on prevalence estimates of HAND were explored using SPSS version 2, with a set at 0.05. First, we tested the effect of each study characteristic on prevalence using an independent test or ANOVA, and then repeated the test while adjusting for all significant covariates using univariate analysis. To differentiate statistical significance from epidemiological significance, an increase or decrease in prevalence by >7% was termed epidemiologically significant. A covariate was deemed significant if it accounted for a variation in prevalence of >7%. We calculated the burden of HAND by multiplying the number of PLWHIV in sub-Saharan Africa by the estimated prevalence of HAND (with 95% confidence intervals [CIs]).34 We obtained the number of adults with HIV in sub-Saharan Africa (25.6 million) from the 2018 UNAIDS report.35
Results
Review profile
We identified 3423 records. After removing duplicates, 3068 records remained. After screening all the titles and abstracts, we excluded 3036 irrelevant records, leaving 32 records for full-text review. Of the 32 full texts, 4 publications were excluded. Ultimately, our review included 28 articles involving 9315 participants from 12 countries (Figure 1). Of these 28 articles, 24 were found in PubMed, 2 in Academic Search Complete, and 1 each from MEDLINE and PsycINFO. The sample sizes in each study varied from 5 536 to 247137. More than half (61%) of the sample population were from East Africa; 39% of the studies were conducted in East Africa, 10 (35.7%) in Southern Africa and 7 (25%) in West Africa. Seventeen studies (71%) used non-probability sampling methods. All studies included adult participants, with a mean age of approximately 38±7 years. The ratio of women to men was approximately 2:1. Most of the participants had formal education (>7years of formal education).
Neuro-psychiatric disorder was assessed and excluded in 19 (68%) studies. Comprehensive neuropsychological assessment was carried out in 10 (35.7%) studies, 14 (53.6%) studies used IHDS, 2 (7.1%) employed HDS, and 1 each employed a combination of IHDS and Montreal Cognitive Assessment Scale and a community screening interview for dementia. We noted that different studies used different definitions and criteria to diagnose HAND. Six studies used the 2007 Frascati criteria, with three of them being East African studies. Sixteen (57%) studies diagnosed HAND if participants had <10 on IHDS/HDS, with most being East African studies. Four (14.3%) studies used the Global Deficit Score. One study from Kenya used an aggregate score derived from the Montreal Cognitive Assessment Scale and IHDS. In terms of methodological quality, risk of bias assessment revealed that all studies had a low risk of bias (Table 1). Of the 28 studies included in this review, 6 reported prevalence of depression, with the prevalence of depression being significantly higher (35.6%) in studies in which depression was associated with HAND than those in which the prevalence of depression (14.3%) was not associated with HAND. In 13 (46.4%) studies, depression was excluded or the rate was not associated with HAND, as opposed to 11 studies in which depression was included or rate was not associated with HAND. Four studies reported level of alcohol use. Mogambery et al.38 reported that higher alcohol use (42.5%) was protective of HAND as opposed to studies that reported low levels of alcohol use (13.5%) which found no association between prevalence of HAND and alcohol use. Of the studies that did not outrightly exclude participants with substance abuse, only three reported rate of substance abuse, which was not associated with HAND (Table 1).
Prevalence and burden of HAND in sub-Saharan Africa
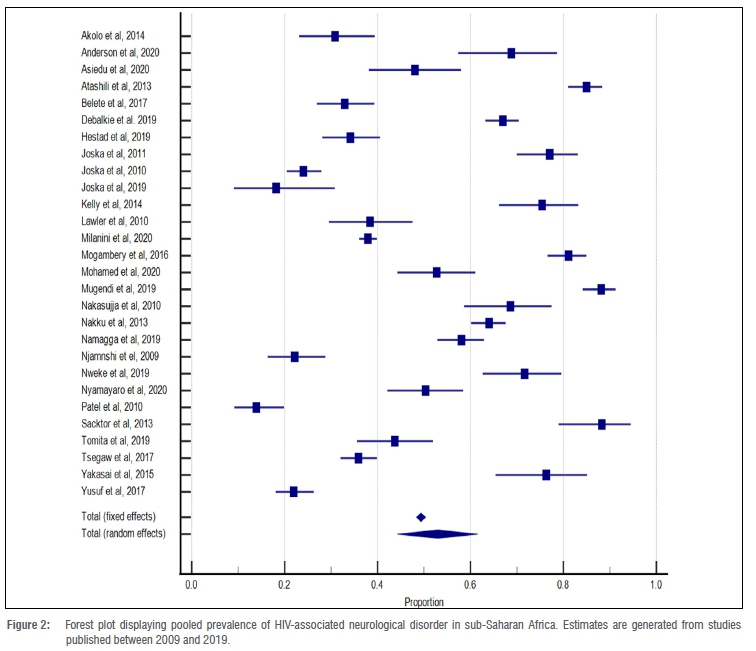
The prevalence of HAND in sub-Saharan Africa varies greatly between 14% (9.2 to 19.9%)39 and 88% (79.0 to 94.5%)40. With a considerable degree of heterogeneity, the pooled prevalence was pegged at 53% (CI=44.3 to 61.5%; I2=98.5). Thirteen (46%) of the studies reported prevalence rates higher than the summary prevalence (Figure 2). The estimated burden of HAND in sub-Saharan Africa was 1356.8 million (m) (CI: 1134.08-1574.4 m). The prevalence of HAND in East Africa, West Africa and Southern Africa was 66.7 m (CI: 35.0-98.4 m), 49.6 m (CI: 23.6-75.6 m) and 48.4 m (CI: 22.5-74.4 m), respectively.
Effects of study characteristics on prevalence of HAND in sub-Saharan Africa
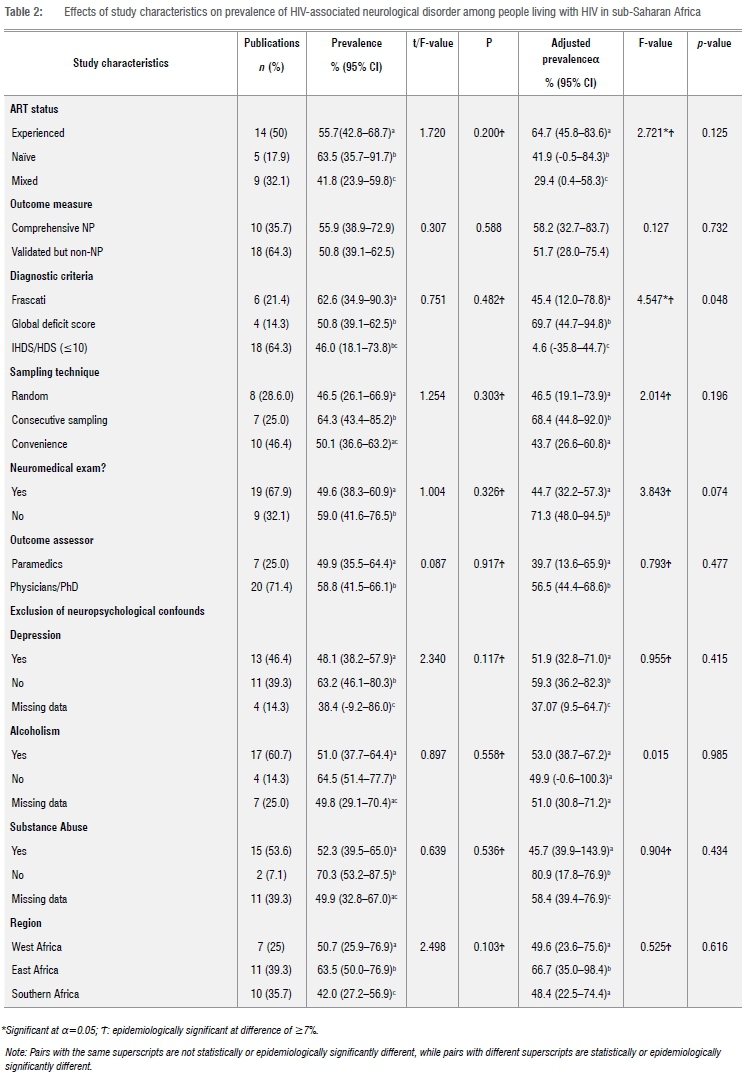
Our data were normally distributed (Shapiro-Wilk statistic=0.940; p=0.111), hence we used parametric statistics. Table 2 shows the effects of study characteristics on the prevalence estimates of HAND in sub-Saharan Africa.
Epidemiologically, studies from East Africa reported significantly higher prevalence estimates of HAND ((66.7 (CI: 35.0-98.4)) compared to studies from Southern Africa and West Africa. Studies that utilised random sampling recorded an epidemiologically significantly lower rate ((46.5% (CI: 26.1-66.9)) compared with studies that used consecutive sampling ((68.4 (CI: 44.8-92.0)). Epidemiologically, similar prevalence estimates of HAND were obtained using comprehensive neuropsychological tests and validated composite measures. Nineteen (68%) studies diagnosed HAND using a neuromedical exam. Prevalence estimates of HAND were significantly lower (44.7% (CI: 32.2-57.3)) in studies with neuromedical exam compared to studies without neuromedical exam (71.3% (CI: 48.094.5)). Epidemiologically higher prevalence estimates of HAND were reported in studies in which physicians/PhD holders were the outcome assessors (58.8%) than those studies with paramedics (49.6%). A large proportion of studies did not exclude neuropsychological confounds such as depression (79%), alcohol use (57%) and substance abuse (61%). We classified studies into two categories: (1) studies in which neuropsychological confound(s) were excluded or potential confounds were not associated with HAND prevalence estimates and (2) studies that included neuropsychological confound(s) which were associated with HAND prevalence estimate. Studies that excluded depression and substance abuse reported epidemiologically lower prevalence estimates of HAND (51.9% and 45.7%, respectively) than studies that included depression and substance abuse (p<0.05) (Table 2).
Discussion
The estimated prevalence of HAND in sub-Saharan Africa in this review was approximately 53% (CI: 44.3-61.5%). Unfortunately, none of the reviewed studies assessed for self-report of difficulty in cognitive ability as part of the criteria for diagnosing HAND. It is likely that use of diagnostic criteria void of a patient's perspective of the symptom may have resulted in exaggerated prevalence estimates.34,41 Given that the false positive rate can exceed 20%.41,42 We estimate the prevalence of HAND to be pegged at 33%. Our prevalence estimates are 10% higher than estimates obtained in a similar study conducted 7 years ago.43 This increase reflects the widespread use of ART in sub-Saharan Africa and indicates that asymptomatic and mild cognitive impairment are common amongst PLWHIV.
The prevalence of HAND seems to be higher among ART experienced PLWHIV compared to ART naïve individuals.14,15 ART naïve PLWHIV showed a higher prevalence of HAND compared to PLWHIV in a mixed ART group, suggesting that duration of use of ART is an important factor influencing the prevalence of HAND and the severity of symptoms. This is consistent with the findings of Habib et al.43 in which individuals on ART for >6 months achieved a lower prevalence of dementia. We included studies from 2009 to 2019 only, and no cases of acute HAND were diagnosed in any of these studies, suggesting that ART has been successful in combating severe forms of neurocognitive impairment among PLWHIV in sub-Saharan Africa. In other words, non-use of ART among ART-naïve PLWHIV is a risk for HAND, while longer duration of ART is a risk for mild forms of HAND among ART-experienced PLWHIV.14,15 Interestingly, we found an inverse relationship between the prevalence of HAND and the prevalence of HIV. In sub-Saharan Africa, Southern Africa has the highest prevalence of HIV, followed by Eastern Africa and then West Africa. Our review suggests that East Africa had the largest burden of HAND, followed by West Africa and then Southern Africa. This may be due to the South African HIV care system being more effective than those of East and West Africa44,45 or due to a larger proportion of PLWHIV in South Africa being on ART46.
Our findings also suggest that the prevalence estimates of HAND were associated with sampling technique. Studies that used consecutive sampling generated significantly higher prevalence estimates compared to studies that employed random sampling. Estimating prevalence using non-probability sampling may be prone to a type-1 error due to selection bias47, and may have contributed to the wide prevalence gap across studies. We suggest that policymakers cautiously interpret studies that employ non-probability sampling, especially when using such evidence for strategic planning. Random sampling is the gold standard procedure for selecting participants for medical research.48
Several measures, ranging from generic to disease-specific measures, are used to assess neurocognitive disorder among PLWHIV. These include the popular mini-mental state exam48, the HDS49, community screening interview for dementia50, IHDS29, and several combinations of neuropsychological tests such as Hopkins verbal learning test revised, Wechsler adult intelligence scale III symbol search, grooved pegboard, colour trails 2, Wechsler memory scale III spatial span and controlled oral word association test11. In this review, cognitive measures included IHDS, HDS, community screening interview for dementia, Montreal Cognitive Assessment Scale and multidomain neuropsychological tests. Consistent with the literature9,51, we found that studies using comprehensive multidomain neuropsychological battery tests delivered higher prevalence estimates of HAND. Neuropsychological tests are generally more sensitive than composite measures such as IHDS and HDS.51,52 Generally, HAND is diagnosed with a IHDS/HDS score less than 10. We found that prevalence estimates of HAND were statistically and epidemiologically lower in studies that used the Frascati criteria and Global Deficit Score compared to studies that relied on IHDS/HDS score alone. This suggests that the Frascati criteria are stricter and more specific than the IHDS/HDS score.39,53 Neuropsychological tests are the gold standard for assessing HAND, especially when the Frascati criteria are fulfilled.54 The Frascati criteria seems to be gaining wide utility in clinical research across sub-Saharan Africa40,55; however, use of composite measures remains the norm amongst clinical researchers in the region56. This may be due to battery tests being expensive and health professionals not being skilled in administering these tests to diagnose HAND.57,58 Our findings suggest that the Frascati criteria may be more sensitive, generating higher prevalence estimates than the Global Deficit Score. Based on this review, we recommend comprehensive neuropsychological screening and application of the Frascati criteria to diagnose HAND for improved sensitivity as well as reduced false positive rate, especially when planning treatment.
We found that studies that conducted neuromedical exams and screened for depression generated significantly lower prevalence estimates. This is consistent with the findings of Belete et al.59 and Lawler et al.6 who maintain that neurological and neuropsychiatric confounds, such as depression and a positive history of psychiatric disorder, constitute major bias and often result in exaggerated prevalence estimates. Non-exclusion of neuropsychological confounds such as depression, substance abuse or lack of neurological and/or medical examination may also result in false positive diagnoses. We recommend compulsory neuromedical examination as well as screening for exclusion of putative neuropsychological confounds such as depression, alcoholism and substance abuse. Employing the Frascati criteria may also help to eliminate confounding variables.4 The Frascati criteria were developed in 2007 to allow for uniformity in the diagnosis of HAND. These criteria involve neuropsychological testing across various cognitive domains. Activities of daily living and ruling out other potential factors/causes for cognitive decline are also part of the diagnostic criteria.16 Our review reveals a grey area of controversy: whether alcohol use is protective of, or a risk for HAND. Studies by Debalkie Animut et al.44 and Patel et al.40 concluded that alcohol use is a significant predictor of HAND prevalence in a population. Interestingly, an important study38 that found a high rate of alcohol use achieved a reciprocal association between alcohol use and the prevalence of HAND. It is possible that alcohol use in this population negatively influenced ART use (adherence), which might protect against mild forms of HAND.60 We found that studies with more highly qualified and experienced assessors resulted in higher prevalence estimates of HAND, possibly due to physicians or assessors with a PhD being less likely to miss a diagnosis. This shows that the qualification or experience of outcome assessors is an important consideration when screening for HAND in clinical research across sub-Saharan Africa.
Conclusions
Prevalence of HAND in sub-Saharan Africa is high and widespread, with HAND being most prevalent in East Africa. In sub-Saharan Africa, HAND is estimated under circumstances that differ: using different diagnostic approaches, different degrees of neuromedical examination, across people with different ART status, different sampling methods, assessment of substance abuse, assessors' qualification, depression and different outcome measures. These variables, in this order, account for different prevalence estimates of HAND reported in different studies. We recommend that estimating the prevalence of HAND should be standardised, favouring the use of Frascati criteria and multidomain comprehensive neuropsychological screening, neuromedical examination, factoring in of ART status and duration, random sampling technique, assessing and excluding current history of substance abuse and depression, and inter-professional collaboration with at least one of the assessors being a physician or PhD graduate. Importantly, policymakers should consider study characteristics when interpreting prevalence estimates for strategic planning and policymaking.
Acknowledgements
We acknowledge the Health Promotion, Molecular Therapy and Rehabilitation initiative, University of Nigeria, Enugu, for the motivation to conduct this review. We extend our sincere gratitude to Dr Tosh Cheryl of the Faculty of Health Sciences, University of Ibadan, for editing this manuscript.
Competing interests
We have no competing interests to declare.
Authors' contributions
M.C.N. who is a funded PhD student under the supervision of N.M. conceived the idea and wrote the study protocol. Independent screening was undertaken by A.J.O., E.M.U., and C.N. Differences were resolved in consultation with M.C.N. Data extraction was independently carried out by A.J.O., E.M.U., C.N. and P.I.U., while M.C.N. serves as the data curator. M.C.N. together with A.J.O., C.N., and P.I.U. wrote the initial draft of the manuscript. All the authors revised the initial draft of the manuscript and approved the final draft.
References
1. Sanmarti M, Ibáñez L, Huertas S, Badenes D, Dalmau D, Slevin M. HIV-associated neurocognitive disorders. J Mol Psychiatry. 2014;2(1):371-379. https://doi.org/10.1186/2049-9256-2-2 [ Links ]
2. Bougea A, Spantideas N, Galanis P Gkekas G, Thomaides T. Optimal treatment of HIV-associated neurocognitive disorders: Myths and reality. Ther Adv Infect Dis. 2019;6(8):1-9. https://doi.org/10.1177/2049936119838228 [ Links ]
3. Ahmad MY Mustafa IG. Prevalence and correlates of HIV-associated neurocognitive disorders in Northwestern Nigeria. Neurol Res Int. 2015;2015, Art. #486960. https://doi.org/10.1155/2015/486960 [ Links ]
4. Antinori A, Trotta MP Lorenzini P Torti C, Gianotti N, Maggiolo F, et al. Virological response to salvage therapy in HIV-infected persons carrying the reverse transcriptase K65R mutation. Antiviral Ther. 2007;12(8):1175-1183. [ Links ]
5. Ances BM, Ellis RJ. Dementia and neurocognitive disorders due to HIV-1 infection. Semin Neurol. 2007;27(1):86-92. https://doi.org/10.1055/s-2006-956759 [ Links ]
6. Lawler K, Mosepele M, Ratcliffe S, Seloilive E, Steele K, Nthobatsang R, et al. Neurocognitive impairment among HIV positive individuals in Botswana: A pilot study. J Int AIDS Soc. 2010;13(1):15. https://doi.org/10.1186/1758-2652-13-15 [ Links ]
7. Atashili J, Gaynes BN, Pence BW, Tayong G, Kats D, O'Donnell JK. Prevalence, characteristics and correlates of a positive-dementia screen in patients on antiretroviral therapy in Bamenda, Cameroon: A cross-sectional study. BMC Neurol. 2013;13:86. https://doi.org/10.1186/1471-2377-13-86 [ Links ]
8. Sacktor N, Skolasky RL, Seaberg E, Munro C, Becker JT, Martin E. Prevalence of HIV-associated neurocognitive disorders in the Multicenter AIDS Cohort Study. Neurology. 2016;86(4):334-340. https://doi.org/10.1212/WNL.0000000000002277 [ Links ]
9. Kelly CM, Van Oosterhout JJ, Ngwalo C, Stewart RC, Benjamin L, Robertson KR, et al. HIV associated neurocognitive disorders (HAND) in Malawian adults and effect on adherence to combination anti-retroviral therapy: A cross sectional study. PLoS ONE. 2014;9(6), e98962. https://doi.org/10.1371/journal.pone.0098962 [ Links ]
10. Van Wijk C. Screening for HIV-associated neurocognitive disorders (HANDs) in South Africa: A caution against uncritical use of comparative data from other developing countries. S Afr J HIV Med. 2013;14(1):17-19. https://doi.org/10.7196/sajhivmed.855 [ Links ]
11. Yakasai AM, Gudaji MJ, Muhammad H, Ibrahim A, Owolabi LF, Ibrahim DA, et al. Prevalence and correlates of HIV-Associated Neurocognitive Disorders (HAND) in Northwestern Nigeria. Neurol Res Int. 2015:1-9. https://doi.org/10.1155/2015/486960 [ Links ]
12. Heaton RK, Franklin DR, Ellis RJ, McCutchan JA, Letendre SL, Leblanc S, et al. HIV-associated neurocognitive disorders before and during the era of combination antiretroviral therapy: Differences in rates, nature, and predictors. J Neurovirol; 2011;17(1):3-16. https://doi.org/10.1007/s13365-010-0006-1 [ Links ]
13. Deeks SG, Lewin SR, Havlir DV. The end of AIDS: HIV infection as a chronic disease. Lancet. 2013;382(9903):1525-1533. https://doi.org/10.1016/S0140-6736(13)61809-7 [ Links ]
14. US Centers for Disease Control and Prevention (CDC). HIV surveillance report vol. 29: Diagnoses of HIV infection in the United States and dependent areas, 2017. Atlanta, GA: CDC; 2018. Available from: http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html [ Links ]
15. UNAIDS. AIDSinfo [webpage on the Internet]. No date [cited 2019 Dec 17]. Available from: https://aidsinfo.unaids.org/ [ Links ]
16. Gates TM, Cysique LA, Siefried KJ, Chaganti J, Moffat KJ, Brew BJ. Maraviroc-intensified combined antiretroviral therapy improves cognition in virally suppressed HIV-associated neurocognitive disorder. AIDS. 2016;30(4):591- 600. https://doi.org/10.1097/QAD.0000000000000951 [ Links ]
17. Modi G, Mochan A, Modi M. Neurological manifestations of HIV. In: Okware SI, editor. Advances in HIV and AIDS control. London: IntechOpen; 2018. https://doi.org/10.5772/intechopen.80054 [ Links ]
18. Hall MD. Age transmissions in European HIV transmission pairs uncovered with viral sequence data. Paper presented at: Conference on Retroviruses and Opportunistic Infections (CROI 2018); 2018 March 4-7; Boston, MA, USA. Abstract 960. [ Links ]
19. Alford K, Vera JH. Cognitive impairment in people living with HIV in the ART era: A review. Br Med Bull. 2018;127(1):55-68. https://doi.org/10.1093/bmb/ldy019 [ Links ]
20. Wing EJ. The aging population with HIV infection. Trans Am Clin Climatol Assoc. 2017;128:131-144. [ Links ]
21. Nweke MC, Nombeko M, Govender N, Akinpelu AO. Physiologic effects of physical activity on cognitive function in people living with HIV: A systematic review of intervention and observational studies. Afr J Physical Activity Health Sci. 2021;27(1):1-22. [ Links ]
22. Ward MM. Disease prevalence and incidence using administrative data: Some assembly required. J Rheumatol. 2013;40(8):1241-1243. https://doi.org/10.3899/jrheum.130675 [ Links ]
23. Namagga JK, Rukundo GZ, Voss JG. Prevalence and risk factors of HIV-associated neurocognitive disorders in Rural Southwestern Uganda. J Assoc Nurses AIDS Care. 2019;30(5):531-538. https://doi.org/10.1097/JNC.0000000000000036 [ Links ]
24. Achappa B, Madi D, Bhaskaran U, Ramapuram JT, Rao S. Adherence to antiretroviral therapy in sub-Saharan Africa and North America: A meta-analysis. North Am J Med Sci. 2013;5(3):220-223. https://doi.org/10.4103/1947-2714.109196 [ Links ]
25. Kampstra P. Beanplot: A boxplot alternative for visual comparison of distributions. J Stat Softw. 2008;28(1)1-9. https://doi.org/10.18637/jss.v028.c01 [ Links ]
26. Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ. 2015;349:g7647. https://doi.org/10.1136/bmj.g7647 [ Links ]
27. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: A proposal for reporting Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008-2012. https://doi.org/10.1001/jama.283.15.2008 [ Links ]
28. Nweke MC, Ekezie UM, Chioma N, Adaora O, Ugwu PIMM. Effects of variability in outcome measure and outcome assessors on the prevalence of HAND in sub-Saharan Africa [preregistered protocol]. OSF; 2020. https://doi.org/10.17605/OSF.IO/VB52Y [ Links ]
29. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177-188. https://doi.org/10.1016/0197-2456(86)90046-2 [ Links ]
30. Hoy D, Brooks P, Woolf A, Blyth F, March L, Bain C, et al. Assessing risk of bias in prevalence studies: Modification of an existing tool and evidence of interrater agreement. J Clin Epidemiol. 2012;65(9):934-939. https://doi.org/10.1016/j.jclinepi.2011.11.014 [ Links ]
31. Wang KS, Liu X. Statistical methods in the meta-analysis of prevalence of human diseases. J Biostat Epidemiol. 2016;2(1):20-24. [ Links ]
32. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539-1558. https://doi.org/10.1002/sim.1186 [ Links ]
33. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al., editors. Cochrane handbook for systematic reviews of interventions version 6.2 [document on the Internet]. c2021 [cited 2021 Feb 22]. Available from: https://training.cochrane.org/handbook/current [ Links ]
34. Wang Y Liu M, Lu Q, Farrell M, Lappin JM, Shi J, et al. Global prevalence and burden of HIV-associated neurocognitive disorder: A meta-analysis. Neurology. 2020;95:e2610-e2621. https://doi.org/10.1212/WNL.0000000000010752 [ Links ]
35. UNAIDS. Global HIV AIDS statistics: 2019 fact sheet [webpage on the Internet]. No date [cited 2020 May 08]. Available from: www.unaids.org/en/resources/fact-sheet [ Links ]
36. Joska JA, Dreyer AJ, Nightingale S, Combrinck MI, De Jager CA. Prevalence of HIV-1 infection in an elderly rural population and association with impairment. AIDS. 2019;33(11):1765-1771. https://doi.org/10.1097/QAD.0000000000002257 [ Links ]
37. Milanini B, Allen I, Paul R, Bahemana E, Kiweewa F, Nambuya A, et al. Frequency and predictors of HIV-related cognitive impairment in East Africa: The Africa Cohort Study (AFRICOS). J Acquir Immune Defic Syndr. 2020;83(2):157-164. https://doi.org/10.1097/QAI.0000000000002242 [ Links ]
38. Mogambery JC, Dawood H, Wilson D, Moodley A. HIV-associated neurocognitive disorder in a KwaZulu-Natal HIV clinic: A prospective study. South Afr J HIV Med. 2017;18(1):732. https://doi.org/10.4102/sajhivmed.v18i1.732 [ Links ]
39. Sacktor N, Nakassyja N, Okonkwo O, Skolasky RL, Robertson K, Musisi S, et al. Longitudinal neuropsychological test performance among HIV seropositive individuals in Uganda. J Neurovirol. 2013;19(1):48-56. https://doi.org/10.1007/s13365-012-0139-5 [ Links ]
40. Patel SM, Thames AD, Arbid N, Panos SE, Castellon S, Hinkin CH. The aggregate effects of multiple comorbid risk factors on cognition among HIV-infected individuals. J Clin Exp Neuropsychol. 2013;35(4):421-434. https://doi.org/10.1080/13803395.2013.783000 [ Links ]
41. Nightingale S, Joska JA, Winston A, Gisslén M, Barber T. Reader response: Global prevalence and burden of HIV-associated neurocognitive disorder: A meta-analysis. Neurology. 2020. Available from: https://n.neurology.org/content/reader-response-global-prevalence-and-burden-hiv-associated-neurocognitive-disorder-meta [ Links ]
42. Gisslen M, Price RW, Nilsson S. The definition of HIV-associated neurocognitive disorders: Are we overestimating the real prevalence? BMC Infect Dis. 2011;11, Art. #356. https://doi.org/10.1186/1471-2334-11-356 [ Links ]
43. Habib AG, Yakasai AM, Owolabi LF, Ibrahim A, Habib ZG, Gudaji M. Neurocognitive impairment in HIV-1-infected adults in sub-Saharan Africa: A systematic review and meta-analysis. Int J Infect Dis. 2013;17(10):e820-e831. https://doi.org/10.1016/j.ijid.2013.06.011 [ Links ]
44. Debalkie Animut AM, Sorrie MB, Birhanu YW, Teshale MY High prevalence of neurocognitive disorders observed among HIV/AIDS in Southern Ethiopia: A cross-sectional study. PLoS ONE. 2019;14(3), e0204636. https://doi.org/10.1371/journal.pone.0204636 [ Links ]
45. Mugendi AG, Kubo MN, Nyamu DG, Mwaniki LM, Wahome SK, Haberer JE. Prevalence and correlates of neurocognitive disorders among HIV patients on antiretroviral therapy at a Kenyan Hospital. Neurol Res Int. 2019;2019, Art. #5173289. https://doi.org/10.1155/2019/5173289 [ Links ]
46. Granich R, Gupta S, Hersh B, Williams B, Montaner J, Young B, et al. Trends in AIDS deaths, new infections and ART coverage in the top 30 countries with the highest AIDS mortality burden; 1990-2013. PLoS ONE. 2015;10(7), e0131353. https://doi.org/10.1371/journal.pone.0131353 [ Links ]
47. Molloy DW, Standish TI. A guide to the standardized Mini-Mental State Examination. Int Psychogeriatr. 1997;9(suppl 1):87-94; discussion 143150. https://doi.org/10.1017/S1041610297004754 [ Links ]
48. Power C, Selnes OA, Grim JA, McArthur JC. HIV dementia scale: A rapid screening test. J Acquir Immune Defic Syndr Hum Retrovirol. 1995;8(3):273-278. https://doi.org/10.1097/00042560-199503010-00008 [ Links ]
49. Sumonu TA, Imarhiagbe F, Owolabi LF, Ogunrin OA, Komolafe MA, Ilesanmi OS. Cognitive functions in newly diagnosed patients with HIV infection in a tertiary health facility: Assessment using community screening interview for dementia. eNeurologicalSci. 2017;24(9):8-13. https://doi.org/10.1016/j.ensci.2017.10.001 [ Links ]
50. Sacktor NC, Wong M, Nakasujja N, Skolasky RL, Selnes OA, Musisi S, et al. The International HIV Dementia Scale: A new rapid screening test for HIV dementia. AIDS. 2005;19(13):1367-1374. [ Links ]
51. De Almeida SM, Kumat R, Cherner M, Umlauf A, Ribeiro CE. Improving detection of HIV-associated cognitive impairment: Comparison of international HIV dementia scale and a brief screening battery. J Acquir Immune Defic Syndr. 2017;74(3):332-338. https://doi.org/10.1097/QAI.0000000000001224 [ Links ]
52. Kakuba N, Menon JA, Franklin DR, Heaton RK, Hestad KA. Use of Western neuropsychological test battery in detecting HIV-associated neurocognitive disorders in Zambia. AIDS Behav. 2017;21(6):1717-1727. https://doi.org/10.1007/s10461-016-1443-5 [ Links ]
53. Gandhi NS, Moxley RT, Creighton J, Roosa HV, Skolasky RL, Selnes OA, et al. Comparison of scales to evaluate the progression of HIV-associated neurocognitive disorder. HIV Ther. 2010;4(3):371-379. https://doi.org/10.2217/hiv.10.23 [ Links ]
54. Tierney SM, Sheppard DP Kordovski VM, Faytell MP Avci G, Woods SP A comparison of the sensitivity, stability, and reliability of three diagnostic schemes for HIV-associated neurocognitive disorders. J Neurovirol. 2017;23(3):404-421. https://doi.org/10.1007/s13365-016-0510-z [ Links ]
55. Akolo C, Royal W III, Cherner M, Okwuasaba K, Eyzaguirre L, Adebiyi R, et al. Neurocognitive impairment associated with predominantly early stage HIV infection in Abuja, Nigeria. J Neurovirol. 2014;20(4):380-387. https://doi.org/10.1007/s13365-014-0254-6 [ Links ]
56. Gandhi NS, Moxley RT, Creighton J, Roosa HV Skolasky RL, Selnes OA, et al. Comparison of scales to evaluate the progression of HIV-associated neurocognitive disorder. HIV Ther. 2010;4(3):371-379. https://doi.org/10.2217/hiv.10.23 [ Links ]
57. Singh D, Joska JA, Goodkin K, Lopez E, Myer L, Paul RH. Normative scores for a brief neuropsychological battery for the detection of HIV-associated neurocognitive disorder (HAND) among South Africans. BMC Res Notes. 2010;3:28. https://doi.org/10.1186/1756-0500-3-28 [ Links ]
58. Chetty V Maharaj SS. Collaboration between health professionals in the era of antiretroviral therapy. J Assoc Nurses AIDS Care. 2013;24(2):166-175. https://doi.org/10.1016/j.jana.2012.04.005 [ Links ]
59. Belete T, Medfu G, Yemiyamrew E. Prevalence of HIV associated neuro-deficit among HIV positive people in Ethiopia: A Cross-sectional study at Ayder Referral Hospital. Ethiop J Health Sci. 2017;27(1):67-76. [ Links ]
60. Hendershot CS, Stoner SA, Pantalone DW, Simoni JM. Alcohol use and antiretroviral adherence: Review and meta-analysis. J Acquir Immune Defic Syndr. 2009;52(2):180. https://doi.org/10.1097/QAI.0b013e3181b18b6e [ Links ]
61. Anderson SG, McCaul M, Khoo S, Wiesner L, Sacktor N, Joska JA, et al. The neurologic phenotype of South African patients with HIV-associated neurocognitive impairment. Neurol Clin Pract. 2020;10(1):15-22. https://doi.org/10.1212/CPJ.0000000000000687 [ Links ]
62. Asiedu N, Kretchy I, Asampong E. Psycho-behavioral factors associated with neurocognitive performance among people living with HIV on antiretroviral therapy in Accra, Ghana. Afr Health Sci. 2020;20(2):487-596. https://doi.org/10.4314/ahs.v20i2.6 [ Links ]
63. Hestad KA, Chinyama J, Anitha MJ, Ngoma MS, McCutchan JA, Franklin DR Jr, et al. Cognitive impairment in Zambians with HIV infection and pulmonary tuberculosis. J Acquir Immune Defic Syndr. 2019;80(1):110-117. https://doi.org/10.1097/QAI.0000000000001880 [ Links ]
64. Joska JA, Westgarth-Taylor J, Myer L, Hoare J, Thomas KG, Combrinck M, et al. Characterization of HIV-associated neurocognitive disorders among individuals starting antiretroviral therapy in South Africa. AIDS Behav. 2011;15:1197-1203. https://doi.org/10.1007/s10461-010-9744-6 [ Links ]
65. Joska JA, Fincham DS, Stein DJ, Paul RH, Seedat S. Clinical correlates of HIV-associated neurocognitive disorders in South Africa. AIDS Behav. 2010;14(2):371-378. [ Links ]
66. Mohamed AA, Oduor C, Kinyanjui D. HIV-associated neurocognitive disorders at Moi teaching and referral hospital, Eldoret, Kenya. BMC Neurol. 2020;20:280. https://doi.org/10.1186/s12883-020-01857-3 [ Links ]
67. Nakasujja N, Skolasky RL, Musisi S, Allebeck P Robertson K, Ronald A, et al. Depression symptoms and cognitive function among individuals with advanced HIV infection initiating HAART in Uganda. BMC Psychiatry. 2010;102, Art. #44. https://doi.org/10.1186/1471-244X-10-44 [ Links ]
68. Nakku J, Kinyanda E, Hoskins S. Prevalence and factors associated with probable HIV dementia in an African population: A cross-sectional study of an HIV/AIDS clinic population. BMC Psychiatry. 2013;13, Art. #126. https://doi.org/10.1186/1471-244X-13-126 [ Links ]
69. Njamnshi AK, Bissek AC, Ongolo-Zogo P Tabah EN, Lekoubou AZ, Yepnjio FN, et al. Risk factors for HIV-associated neurocognitive disorders (HAND) in sub-Saharan Africa: The case of Yaoundé-Cameroon. J Neurol Sci. 2009;285(1-2):149-153. ]https://doi.org/10.1016/j.jns.2009.06.043 [ Links ]
70. Nweke MC, Akinpleu A, Ezema CI. Variation in spatio-temporal gait parameters among patients with HIV-related neurocognitive impairment. Indian J Physiother Occup Ther. 2019;13(4):186-191. [ Links ]
71. Nyamayaro P Gouse H, Hakim J, Robbins RN, Chibanda D. Neurocognitive impairment in treatment-experienced adults living with HIV attending primary care clinics in Zimbabwe. BMC Infect Dis. 2020;20:383. https://doi.org/10.1186/s12879-020-05090-8 [ Links ]
72. Tomita A, Ramlall S, Naidu T, Mthembu SS, Padayatchi N, Burns JK. Neurocognitive impairment risk among individuals with multiple drug-resistant tuberculosis and human immunodeficiency virus coinfection: Implications for systematic linkage to and retention of care in tuberculosis/human immunodeficiency virus treatment. J Nerv Ment Dis. 2019;207(4):307-310. https://doi.org/10.1097/NMD.0000000000000962 [ Links ]
73. Tsegaw M, Andargie G, Alem G, Tareke M. Screening HIV-associated neurocognitive disorders (HAND) among HIV positive patients attending antiretroviral therapy in South Wollo, Ethiopia. J Psychiatr Res. 2017;85:37-41. https://doi.org/10.1016/j.jpsychires.2016.10.016 [ Links ]
74. Yusuf AJ, Hassan A, Mamman AI, Muktar HM, Suleiman AM, Baiyewu O. Prevalence of HIV-associated neurocognitive disorder (HAND) among patients attending a tertiary health facility in northern Nigeria. J Int Assoc Provid AIDS Care. 2017;16(1):48-55. https://doi.org/10.1177/2325957414553839 [ Links ]
 Correspondence:
Correspondence:
Martins Nweke
Email: martins.nweke@gmail.com
Received: 28 June 2020
Revised: 22 Feb. 2021
Accepted: 16 May 2021
Published: 29 Sep. 2021
Editors: Pascal Bessong, Sandiswa Mbewana
Funding: University of Pretoria


{kind=link}
{kind=link}
{kind=link}
{kind=link}