










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Science
versión On-line ISSN 1996-7489
versión impresa ISSN 0038-2353
S. Afr. j. sci. vol.117 no.5-6 Pretoria may./jun. 2021
http://dx.doi.org/10.17159/sajs.2021/8288
RESEARCH ARTICLE
A 5-year overview of fatal thermal and electrical burns in Johannesburg, South Africa
Craig A. Keyes; Khumo L. Liphoko
Department of Forensic Medicine and Pathology, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
Thermal and electrical burn injuries affect millions of people globally each year. South Africa is a developing country where fatal fires are common. Despite the pervasiveness of fatal thermal and electrical burns in South Africa, there is a paucity of information regarding the frequency of such fatal burns in the City of Johannesburg. We aimed to describe the demographics and frequency of fatal thermal and electrical burn cases received at the Johannesburg Forensic Pathology Services Medico-Legal Mortuary for medico-legal death investigations, and compare the burn mortality rates between Johannesburg and those reported in Cape Town, Pretoria, and Mpumalanga. This study was a 5-year (2010-2014) retrospective review of 185 forensic medico-legal case files of fatal burns (156 thermal burn cases and 29 electrical burn cases) received at the Johannesburg Forensic Pathology Services Medico-Legal Laboratory. The demographics at the greatest risk of fatal burns in Johannesburg, South Africa are black (2.11 per 100 000) and male (1.03 per 100 000) individuals, and those in the 30-39-year age group (3.6 per 100 000). Children aged 0-9 years had a high mortality rate due to thermal burns (3.44 per 100 000). The most common type of fatal burns is thermal in nature, as a result of flames (1.62 per 100 000). Electrical burns are relatively rare (0.3 per 100 000). Burns are prevalent in the winter months, most notably in August. Burn wounds are common on the head, chest, back, and abdomen. Johannesburg has an overall lower burn mortality rate and incidence frequency than Cape Town, Pretoria, and Mpumalanga. This study is the first to report on fatal burns in Johannesburg, South Africa.
SIGNIFICANCE:
• A description is provided of fatal thermal and electrical burns of individuals whose deaths were investigated at the Johannesburg Forensic Pathology Services Medico-Legal Mortuary.
• The results highlight the demographic groups at risk of fatal burns in Johannesburg, South Africa.
• Johannesburg has a lower fatal burn incidence and mortality rate than Cape Town, Pretoria, and Mpumalanga; however, young people, particularly male individuals, are at greatest risk.
Keywords: forensic science, unnatural death, mortality rates, fatal burn incidence
Introduction
In South Africa, it is the legal mandate of the Forensic Pathology Services (FPS) to perform post-mortem examinations in all cases of unnatural death.1 Approximately 60 000-80 000 unnatural deaths occur annually in South Africa.2 South African legislation, such as the Inquest Act (Act 58 of 1959), requires that all unnatural deaths have a medico-legal autopsy examination performed.3 An unnatural death is defined by South African law as:
a. Any death due to physical or chemical influence, direct or indirect, and/or related complications.
b. Any death, including those deaths which would normally be considered to be a death due to natural causes, which in the opinion of the medical practitioner, has been the result of an act of commission or omission which may be criminal in nature.
c. Any death as contemplated in the Health Professions Act 56 of 1974: Section 56 (as amended). The death of a person undergoing, or as a result of, a procedure of a therapeutic, diagnostic or palliative nature, or of which any aspect of such a procedure has been a contributory cause, shall not be deemed to be a death from natural causes.
d. A sudden and unexpected, or unexplained, death or where the cause of death is not apparent.1,3,4
In the Gauteng Province, there are 11 FPS medico-legal mortuaries which are divided into two clusters: the Northern Cluster (consisting of three medico-legal mortuaries: Pretoria, Ga-Rankuwa, and Bronkhorstspruit) and the Southern Cluster (consisting of eight medico-legal mortuaries: Johannesburg, Germiston, Diepkloof, Roodepoort, Sebokeng, Carletonville, Springs, and Heidelberg). Approximately 17.5% of all unnatural deaths in South Africa are received by the Gauteng Southern Cluster.2 Over the 2006-2018 period, the Gauteng Southern Cluster received 155 338 cases, averaging 11 949 cases per annum.
The City of Johannesburg municipality has a population of 4.9 million people, making it South Africa's most populous city.5 As a result, the Johannesburg FPS mortuary, which services a large portion of the City of Johannesburg municipality, is one of the busiest FPS mortuaries in South Africa. The Johannesburg FPS performed a total of 36 043 post-mortem examinations between the years 2006 and 2018, averaging 2773 cases per annum.
Deaths precipitated by thermal and electrical burns are classified as unnatural deaths and a post-mortem examination must be performed by the FPS. Thermal and electrical burn injuries affect millions of people globally each year.6 Severe burns rank as the fourth highest incidence of injuries requiring medical attention.7 It is estimated that 300 000 people die annually due to flame- or fire-related burns globally.6 Lower-middle- to low-income countries in the Middle East, Asia and Africa6,8, such as Pakistan9, Iraq10, Ethiopia11, and Kenya12, make up 90% of global burn fatalities.
Thermal burns include burns due to flames, scalding, and contact with a hot surface. In developing countries, such as South Africa, fatal and severe thermal injuries caused by flames frequently occur in cities that are densely populated by people of lower income and are residing in informal residential areas.9 The causes of the fires have been due to the usage of affordable domestic appliances and methods such as kerosene stoves and open fires, which are used for cooking and heating water.8,13,14 Informal settlement fires are a common occurrence in South Africa specifically and Africa generally. Ombati et al.12 found that informal settlement fires are the second highest contributors to burn injuries, compared to the small percentage of burn injuries that occur in formal residential areas.
Scalding burns result from contact of the skin and other tissues with hot liquids.15 The American Burn Association reported that scalding burns were common in young children below the age of 5 years.15 Most scalding burns are a result of hot foods and spilled liquids and they tend to cause minor burns that are typically not fatal.15 However, the effect of scalding burns in the elderly is greater, and even small scalding burns can have fatal consequences.16
Severe injuries due to electrical burns are also common in developing nations. The theft of electrical cables is a common problem in South Africa and may result in fatal electrocution.2 Additionally, illegal electrical connections are common in informal settlements and can have deadly consiquences.17 Most electrical fatalities are unintentional, and result from poor maintenance of electrical equipment and carelessness.2
The epidemiology and prevalence of surviving victims of thermal and electrical burns, treated in South African clinics, burns units, and hospitals, are well documented.18-26 However, there is a scarcity of published data on fatal burns in South Africa. A few regional studies have been conducted in the Western Cape, Mpumalanga, and Gauteng13,17,27, with one published study in Durban on suicide by self-immolation28.
The studies for Cape Town13 and Mpumalanga27 used the National Injury Mortality Surveillance System (NIMSS) as their primary source of data and not specific case files or post-mortem reports. There are limitations in using the NIMSS data, especially the limited detail provided. For example, NIMSS combines burn deaths caused by flames, scalding, and contact to a hot object under a single category, which makes comparisons between the three causes of burns difficult. Ideally, data should be collected from FPS case file documents which provide greater detail on each fatal case. The study by Morobadi et al.17 is the only published South African study, so far, to have reported on fatal thermal burns from data collected directly from FPS case files and postmortem reports.
The mortality rate of deaths caused by electrical burns has largely been under-researched in South Africa. Only one study, by Blumenthal2, has reported the incidence of fatal electrical deaths in Gauteng (using NIMSS data).
Despite the pervasiveness of fatal thermal and electrical burns in South Africa, there is a paucity of information regarding the frequency of such fatal burns in Johannesburg. Johannesburg is the largest city in South Africa and the capital of Gauteng - the most densely populated province in South Africa. The Johannesburg FPS is also one of the busiest forensic mortuaries in South Africa. Therefore, in this study, we aimed to describe the incidence and mortality rate of fatal thermal and electrical burns received at the Johannesburg Forensic Pathology Services Medico-Legal Laboratory for medico-legal death investigations. A comparison of the thermal and electrical burn mortality rates for Johannesburg, Cape Town, Pretoria, and Mpumalanga is also provided.
Methods
Data were collected retrospectively from the case files of the Johannesburg Forensic Pathology Services Medico-Legal Mortuary. The inclusion criterion was any case for which the autopsy report stated that thermal or electrical burn injuries were the primary cause of death or contributory to the cause of death. Data were collected for the 5-year period 2010-2014. This amounted to 185 cases of individuals who died as a result of flames, scalding, explosions, electrocution, or lightning strikes. The information that was collected included demographic details, temporal information, geographical location, and the anatomical regions which exhibited burn injuries. The anatomical regions were divided into: head and neck, thorax, back, abdomen (including the lower back), pelvis, upper limbs, and lower limbs.29
A descriptive analysis of the cases was performed. The incidence and mortality rates were stratified by age, sex, and population group (as outlined in the FPS and police documentation). This was reported for the thermal burn cases, electrical burn cases, and all burn cases (thermal and electrical combined). The mortality rates (expressed per 100 000 per year) were calculated using the 2θ11 Census30 data for the Johannesburg FPS catchment area (estimated population size of 1 922 249) which includes the following areas: Johannesburg, Randburg, Sandton, Midrand, Alexandra, and Diepsloot. The population estimates (total population for the mortuary's catchment area, and relative population size for each age group, sex, and population group) provided by the 2011 Census30 were used as denominators when calculating the burn mortality rates.
Ethical clearance for this study was provided by the Human Research Ethics Committee (Medical) (reference: M150315) of the University of the Witwatersrand and the principles of the Declaration of Helsinki were adhered to. The data set is available on request from authors.
Results
Prevalence of fatal burns
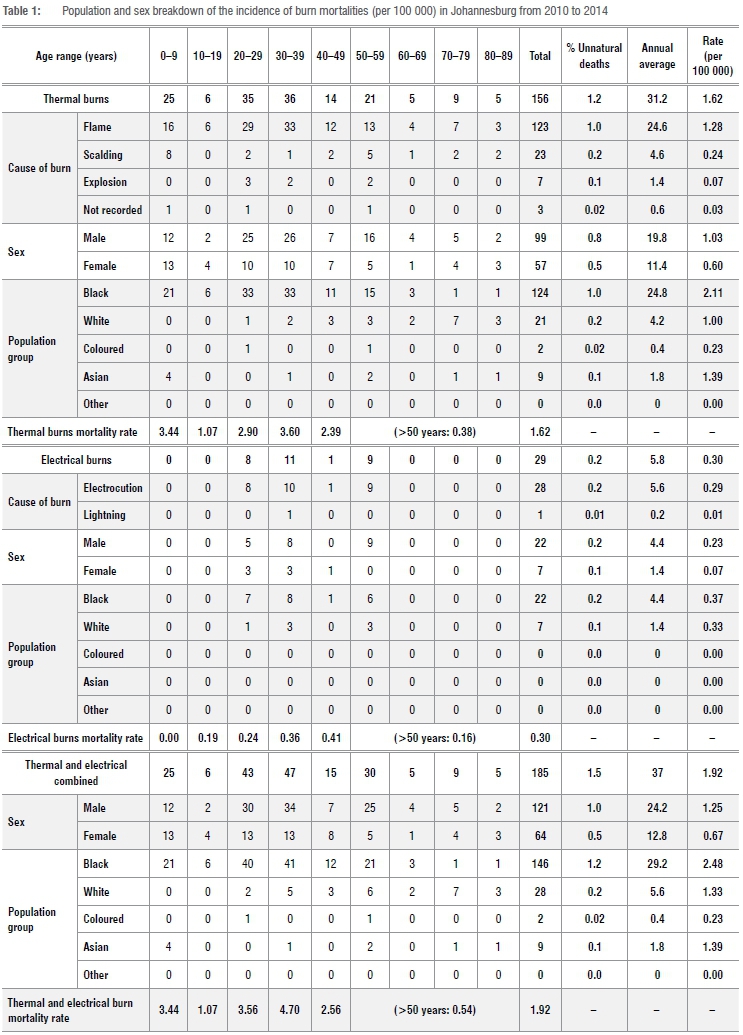
The Johannesburg FPS received a total of 185 thermal and electrical burn fatalities between the years 2010 and 2014, with an annual average of 37 cases. This constituted 1.5% of all unnatural deaths (N=12 591) and a mortality rate of 1.92 (all mortality rates reported are per 100 000). Thermal burns constituted 1.2% of all unnatural deaths (n =156) with a mortality rate of 1.62. Flame-related incidents were the most prevalent cause of thermal burns (n=123; mortality rate = 1.62) followed by scalding (n=23; mortality rate=0.24), and explosions (n=7; mortality rate = 0.07) (Table 1).
Electrical burns were infrequent and only constituted 0.2% of all unnatural deaths, with a mortality rate of 0.30. Electrical burns were predominantly electrocutions (n=28, mortality rate = 0.29); with one case of a fatal lightning strike (mortality rate = 0.01) (Table 1).
Demographics
For all burn types (thermal, electrical, and combined), the mortality rates were highest in black individuals (thermal = 2.11; electrical = 0.37; combined = 2.48) and in male individuals (thermal = 1.03; electrical = 0.23; combined = 1.25). The 30-39-year age group had the highest mortality rate for all burn types (thermal = 3.60; electrical = 0.36; combined = 4.70) (Table 1). The age group with the second highest mortality rate was 20-29 years for both electrical burns (0.24) and the combined thermal and electrical burn cases (3.56); and 0-9 years for thermal burns (3.44) (Table 1).
Temporal frequency
There was an overall decrease in the total number of fatal burns from 2010 (n=58) to 2014 (n=16); however, there was a spike in the number of fatalities in 2013 (n=46) (Figure 1). Most fatal burn cases occurred in the cooler months (July-October), especially in July and August. Unusually, a relatively large number of deaths repeatedly occurred in the warmer month of February (with a particularly high number in the year 2013) (Figure 2). This pattern was common to both thermal and electrical burns (Figure 2).
Location
The settlement typology and death scene were unknown in many cases because this information was not adequately recorded (in 39.4% and 30.8% of cases, respectively). The incidence of fatal burns was most common in residential settings (52% for both thermal burns and electrical burns). Fatal thermal burns typically occurred in suburbs and informal settlements (54% accumulative), particularly in houses and informal dwellings (56.6% accumulative) (Table 2). Fatal electrical burns were higher in the city and suburbs, in houses and places of employment (Table 2).
Description of burn severity
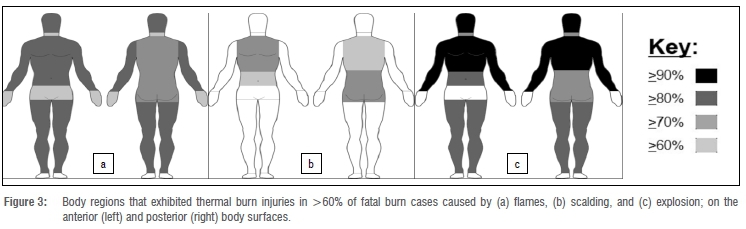
Overall, burn injuries due to flames were common (>60%) on all body regions, except for the feet (Figure 3). Scalding burns were common on the thorax, back, and abdomen (Figure 3). Burns that resulted due to explosions were commonly observed on the head, neck, thorax, back, abdomen, arms, and legs (Figure 3).
There was no clear pattern to the anatomical location of burns caused by electrocution; however, the electrical burns were observed on the chest in 57.1% of cases and on the right arm in 50% of cases. The single lightning case showed burn injuries noted on the head, neck, thorax, lower back, and left foot.
Overall, the feet were the least commonly burned body region (flames = 54.5%, scalding = 39.1%, explosion = 14.3%, electrocution = 7.1%) (Figure 3). In only 27% of all burn cases was the body thermally altered severely enough for a pugilistic posture to be adopted.
Discussion
Mortality rate and cause of burns
Fatal burns constituted only 1.5% of unnatural deaths received by the Johannesburg FPS. Thermal burns were more common and resulted in a higher mortality rate (1.2 per 100 000 per year) than did electrical burns (0.3 per 100 000 per year). Flames were the most common cause of fatal burns and the scene was often in a residential dwelling (formal and informal settlements). This scenario is common in South Africa as it has been observed in studies performed in other South African locations.13,17,25 The high number of fatal thermal and flame-related burns in informal residential areas is due, in part, to unsafe cooking appliances such as petroleum-based stoves.14 These stoves are cheap and portable. Furthermore, candles are often used as a light source. These unsafe appliances, combined with the flammability of the materials used to construct informal residences, non-compliance with fire safety standards31, and the close proximity and density of the dwelling structures allow for fires to spread quickly.
Fatal electrocutions are relatively rare. In the USA, fatal electrocutions occur at a rate of 0.43 per 100 000 per year.32 Comparatively, Johannesburg experienced a similarly low mortality rate of 0.3 per 100 000 per year (only 28 cases in 5 years). Fatal electrocutions were observed only in individuals within the 20-59-year age bracket and occurred most often in city centres and suburban areas. A likely cause of these electrocutions is cable theft. There has been an ongoing escalation in cable theft in urban centres in South Africa as individuals attempt to retrieve the copper wires to sell. These thefts have led to the accidental electrocution and deaths of the culprits and the engineers who attempt to repair or maintain vandalised substations.33 This reason, however, is speculative as little information is provided in such cases and the claims of cable theft are often pronounced only by the media.2
Demographics
Overall, the Johannesburg burns mortality rate (thermal and electrical) was substantially higher in black men aged 20-39 years, than in any other racial, sex, and age group. Although the catchment area of the Johannesburg FPS is 61.2% black, 50.2% male, and 23% falls into the 20-39-year age group (the largest age group by number of individuals), the mortality rate for each group was disproportionally higher than their relative cohorts.
Regions with a low socio-economic status often present with larger numbers of burn cases than regions with higher socio-economic status. Each of these regions is often predominately composed of particular population or ethnic groups, due to historical inequalities. Differences in burn mortality rates among racial and ethnic groups is a phenomenon that is observed globally and is related to socio-economic challenges. Socio-economic status has a greater impact on a group's susceptibility to burns than do cultural or educational factors.15 It is therefore unsurprising that the black population in the Johannesburg region had a higher mortality rate, due to the catchment area's predominantly low socio-economic status and the effects thereof on the population in the region.
Generally, the mortality rate of male individuals tends to be higher than that of female individuals.34 There are numerous theories that have been proposed for why male individuals are more likely to be injured than female individuals, such as that they are socialised differently35,36 and tend to engage in activities that involve riskier behaviours and act more impulsively than female individuals37,38. These behavioural observations are general but have been observed in both young and adult individuals.15
The higher mortality rate of male individuals, particularly in the 20-39-year age range, is also not unexpected as the fire mortality rate has also been found to be predominant in men in this age group in other studies in the USA and Australia.15,39,40 This is likely attributable to the employment and domestic activities of individuals in this age group.
In Johannesburg, young children aged 0-9 years had a particularly high mortality rate due to thermal burns. This is a trend that corresponds to global trends. Globally, fire-related death rates occur most commonly in children under the age of 4 years.15 The death rate begins to increase again from the age of 15 years, which is related to the age-related changes in behaviours associated with risk-taking, exposure to hazards, and employment.7 Children in Africa are at a particularly higher risk for burns compared to the rest of the world. African infants have a three-times higher incidence rate of fire-related burns than the world average.41 A large number of factors influence the higher likelihood of young children being burned in Africa. Some of these factors may include the lower literacy, age, and education level of mothers, the limited availability and means to access healthcare services, combined cooking and living areas in a dwelling, the lack of smoke alarms and access to water in a residential space, and poor emergency response services.42 The increased mortality rate in young children can also be attributed to their stage of development which results in an increase in their motor skills and activity rates. This increases the chance of their coming into contact with harmful objects that could result in their being burned.15
Temporal variations
The global incidence of burns presented at emergency departments and hospitals has been declining since 1982, as has the number of fatal burns.15,43 The linear decline in the mortality rate due to burns is a general, global trend; however, annual and national variations are to be expected. This was highlighted in the overall decrease in the number of fatal burn cases in Johannesburg between the years 2010 and 2014, with a spike in 2013. Such variations to the general trend could be due to individual factors that impacted that year. Unfortunately, we cannot provide any reasonable explanations for the spikes in the year 2013 or the general increase in cases seen in the month of February. No probable causes related to climatic changes, population dynamics, or mortuary intake variances could account for the spikes in the respective mortality rates. It is possible that factors related to social, political, and environmental variations could be the cause15; however, the exact causes are currently not apparent. Ultimately, the decreasing burn mortality rate seen globally and in Johannesburg is a promising trend that is likely the result of increasing urbanisation and development.
Most fatal burn cases occurred in the winter months of July and August. The cooler temperatures result in people using unsafe heating appliances and open flames to warm themselves, which can be dangerous, especially to the very young and elderly. The winter season in Johannesburg is characterised as very dry with no precipitation. Large open fields of long dry grass, called veld, are common in urban areas.
The dry grass and low moisture content often result in veld fires which are a safety hazard in urban areas.
Anatomical regions
The anatomical locations of burns can vary greatly because their causes are contextual. Thermal burns in general were common to the thorax, back, and abdomen. These were also the only body regions to be injured by scalding burns. Burn injuries due to flames exhibited the greatest spread over all body regions (excluding the feet). All thermal burns due to explosions displayed burns to the head, neck, back, and both arms. Fatal electrical burns exhibited very few wounds; however, burns were observed on the right arm in 50% of cases and the chest in 57.1% of cases.
Comparison with other South African studies
Previous studies have reported on fatal burns in Cape Town, Pretoria, and Mpumalanga, and a comparison with the Johannesburg data warrants further investigation. In Johannesburg, fatal burns constituted 1.5% (n=185) of the total number of unnatural deaths (N=1259), which included thermal burns (n=156; 1.2%) and electrical burns (n=29; 0.2%). We collected data from one mortuary, for a 5-year period (20102014). In Cape Town, fatal thermal burns constituted 4.6% (n=256) of the total number of unnatural deaths (N=5534). Fatal electrical burns were not reported on.13 The Cape town data were collected from two mortuaries, over 4 years (2010-2013).13 In Pretoria, fatal thermal burns constituted 3% (n=291) of the total number of unnatural deaths (N =9558). Fatal electrical burns were not reported on.17 The Pretoria data were collected from one mortuary, over 5 years (2011-2015).17 In Mpumalanga, a combined total of 304 cases of thermal and electrical burn mortalities occurred over a 2-year period (2007-2008) at 18 mortuaries.27 The number of fatal thermal burns and electrical burns were not reported individually and the total number of unnatural deaths was not reported.27
Generally, Johannesburg had a lower mortality rate and lower incidence of fatal burns (overall, overall males, and overall females) than did Cape Town13, Pretoria17, and Mpumalanga27 (Tables 3-5). However, Johannesburg had a higher mortality rate in female individuals than did Cape Town13 (Table 3). Johannesburg had a generally higher mortality rate in the younger age groups than did Cape Town13 and Mpumalanga27; particularly the 0-24-year age group (Tables 3 and 5). Johannesburg also had a higher mortality rate in female individuals in the 0-38-year age range than did Cape Town13 and Mpumalanga27 (Tables 3 and 5). Johannesburg, Cape Town13, and Mpumalanga27 all had higher mortality rates in the later months of the year, compared to the earlier months (Tables 3 and 5). In particular, Johannesburg had higher mortality rates in June to August, compared to June to November in Cape Town13 (Table 3). Johannesburg and Mpumalanga27 both had higher mortality rates in August to October (Table 5).
Overall, Johannesburg had a lower mortality rate due to thermal and electrical burns compared to those reported in Cape Town13, Pretoria17, and Mpumalanga27. Although this finding is surprising, given the high population density in the region, it is a promising result. This is likely because the catchment area of the Johannesburg FPS covers a largely urbanised and developed region made up of formal dwellings with access to electricity. However, there were certain groups that had higher burn mortality rates in comparison to that in other areas in South Africa. This included young individuals (0-24 years) and female individuals aged 0-38 years. These groups typically experience a disproportionally higher burn incidence rate (as has been previously discussed). The reasons for their higher mortality rates in Johannesburg compared to the rest of South Africa is unknown and should be further investigated.
Limitations and recommendations
Limitations to the study included case file documents that were incomplete or lacking detail. In this study, we did not investigate the pathology of the burns and the causes of death, which can be further explored in future studies. Due to a large national backlog in toxicology testing in South Africa (an up to 7-10-year delay in test results), toxicology, blood alcohol concentration and blood carboxyhaemoglobin level were not explored in the present study.
A comparison of the burn mortality rate between different manners of death (accident, homicide, suicide) was not included in this study because the manner of death is decided by the courts and not the Forensic Pathology Services. This information is not explicitly present in the medico-legal case file documents. The classification of burn levels (such as first-, second- and third- degree burns) was not presented as this is not typically reported in the autopsy reports.
Conclusion
A 5-year retrospective review of forensic medico-legal case files indicates that the following demographic groups are at greatest risk of fatal burns in Johannesburg, South Africa: black individuals, male individuals, and individuals in the 30-39-year age group. Thermal burns, as a result of flames, are the most common type of burn and are prevalent in the winter months, most notably in August. Electrical burns are relatively rare. Burn wounds are most common to the head, chest, back, and abdomen. Johannesburg has a lower burn mortality rate than other regions in South Africa. This study is the first to report on fatal burns in Johannesburg, South Africa.
Acknowledgements
We acknowledge the Johannesburg Forensic Pathology Services Medico-Legal Laboratory for providing access to the case files and Mr Jaco Louw for providing the data on the case load of the Gauteng Forensic Pathology Service.
Competing interests
We declare that there are no competing interests.
Authors' contributions
C.A.K.: Conceptualisation; methodology; data analysis; validation; writing - the initial draft; student supervision. K.L.L.: Conceptualisation; methodology; data collection; writing - the initial draft.
References
1. National Health Act No. 61 of 2003, South Africa. [ Links ]
2. Blumenthal R. A retrospective descriptive study of electrocution deaths in Gauteng, South Africa: 2001-2004. Burns. 2009;35(6):888-894. https://doi.org/10.1016/j.burns.2009.01.009 [ Links ]
3. The Inquests Act No. 58 of 1959, South Africa. [ Links ]
4. National Health Act No. 61 of 2003, South Africa. Regulations: Rendering of Forensic Pathology Service. [ Links ]
5. Statistics South Africa (StatsSA). Community survey 2016, statistical release P0301. Pretoria: StatsSA; 2016. [ Links ]
6. Peck M, Molnar J, Swart D. A global plan for burn prevention and care. Bull World Health Organ. 2009;87:802-803. https://doi.org/10.2471/BLT.08.059733 [ Links ]
7. World Health Organization (WHO). The global burden of disease: 2004 update. Geneva: World Health Organization; 2008. [ Links ]
8. Lerer LB. Homicide-associated burning in Cape Town, South Africa. Am J Forensic Med Pathol. 1994;15(4):344-347. https://doi.org/10.1097/00000433-199412000-00012 [ Links ]
9. Al Ibran E, Mirza FH, Memon AA, Farooq MZ, Hassan M. Mortality associated with burn injury - a cross sectional study from Karachi, Pakistan. BMC Res Notes. 2013;6(1):1-3. https://doi.org/10.1186/1756-0500-6-545 [ Links ]
10. Qader AR. Burn mortality in Iraq. Burns. 2012;38(5):772-775. https://doi.org/10.1016/j.burns.2011.12.016 [ Links ]
11. Courtright P Haile D, Kohls E. The epidemiology of burns in rural Ethiopia. J Epidemiol Commun Health. 1993;47(1):19-22. https://doi.org/10.1136/jech.47.1.19 [ Links ]
12. Ombati AN, Ndaguatha PL, Wanjeri JK. Risk factors for kerosene stove explosion burns seen at Kenyatta National Hospital in Kenya. Burns. 2013;39(3):501-506. https://doi.org/10.1016/j.burns.2012.07.008 [ Links ]
13. Van Niekerk A, Laubscher R, Laflamme L. Demographic and circumstantial accounts of burn mortality in Cape Town, South Africa, 2001-2004: An observational register based study. BMC Public Health. 2009;9(1), Art. #374. https://doi.org/10.1186/1471-2458-9-374 [ Links ]
14. Ahuja RB, Dash JK, Shrivastava P A comparative analysis of liquefied petroleum gas (LPG) and kerosene related burns. Burns. 2011;37(8):1403-1410. https://doi.org/10.1016/j.burns.2011.03.014 [ Links ]
15. Peck MD. Epidemiology of burns throughout the world. Part I: Distribution and risk factors. Burns. 2011;37(7):1087-1100. https://doi.org/10.1016/j.burns.2011.06.005 [ Links ]
16. Alden N, Bessey P Rabbitts A, Hyden P Yurt R. Tap water scalds among seniors and the elderly: Socioeconomics and implications for prevention. J Burn Care Res. 2006;27:S97. https://doi.org/10.1097/01253092-200603001-00098 [ Links ]
17. Morobadi K, Blumenthal R, Saayman G. Thermal fatalities in Pretoria: A 5-year retrospective review. Burns. 2019;45(7):1707-1714. https://doi.org/10.1016/j.burns.2019.05.007 [ Links ]
18. Steenkamp W, Botha N, Van der Merwe A. The prevalence of alcohol dependence in burned adult patients. Burns. 1994;20(6):522-525. https://doi.org/10.1016/0305-4179(94)90012-4 [ Links ]
19. Van Niekerk A, Rode H, Laflamme L. Incidence and patterns of childhood burn injuries in the Western Cape, South Africa. Burns. 2004;30(4):341-347. https://doi.org/10.1016/j.burns.2003.12.014 [ Links ]
20. Van Niekerk A, Reimers A, Laflamme L. Area characteristics and determinants of hospitalised childhood burn injury: A study in the city of Cape Town. Public Health. 2006;120(2):115-124. https://doi.org/10.1016/j.puhe.2005.08.015 [ Links ]
21. Van Niekerk A, Seedat M, Menckel E, Laflamme L. Caregiver experiences, contextualizations and understandings of the burn injury to their child. Accounts from low-income settings in South Africa. Child Care Health Develop. 2007;33(3):236-245. https://doi.org/10.1111/j.1365-2214.2006.00724.x [ Links ]
22. Eyal A, Kemp M, Luvhengo T. A 10-year audit of burns at Kalafong Hospital. Burns. 2007;33(3):393-395. https://doi.org/10.1016/j.burns.2006.07.011 [ Links ]
23. Allorto N, Oosthuizen G, Clarke D, Muckart D. The spectrum and outcome of burns at a regional hospital in South Africa. Burns. 2009;35(7):1004-1008. https://doi.org/10.1016/j.burns.2009.01.004 [ Links ]
24. Maritz D, Wallis L, Van Der Merwe E, Nel D. The aetiology of adult burns in the Western Cape, South Africa. Burns. 2012;38(1):120-127. https://doi.org/10.1016/j.burns.2010.12.007 [ Links ]
25. Blom L, Klingberg A, Laflamme L, Wallis L, Hasselberg M. Gender differences in burns: A study from emergency centres in the Western Cape, South Africa. Burns. 2016;42(7):1600-1608. https://doi.org/10.1016/j.burns.2016.05.003 [ Links ]
26. Cloake T, Haigh T, Cheshire J, Walker D. The impact of patient demographics and comorbidities upon burns admitted to Tygerberg Hospital Burns Unit, Western Cape, South Africa. Burns. 2017;43(2):411-416. https://doi.org/10.1016/j.burns.2016.08.031 [ Links ]
27. Blom L, Van Niekerk A, Laflamme L. Epidemiology of fatal burns in rural South Africa: A mortuary register-based study from Mpumalanga Province. Burns. 2011;37(8):1394-1402. https://doi.org/10.1016/j.burns.2011.07.014 [ Links ]
28. Sukhai A, Harris C, Moorad R, Dada MA. Suicide by self-immolation in Durban, South Africa: A five-year retrospective review. Am J Forensic Med Pathol. 2002;23(3):295-298. https://doi.org/10.1097/00000433-200209000-00020 [ Links ]
29. Drake R, Vogl A, Mitchell A. Gray's anatomy for students. 2nd ed. Philadelphia, PA: Churchill Livingstone/Elsevier; 2009. [ Links ]
30. Statistics South Africa (StatsSA). Census 2011 statistical release. Pretoria: StatsSA; 2012. [ Links ]
31. Ono R, Da Silva S. An analysis of fire safety in residential buildings through fire statistics. Fire Safety Sci. 2000;6:219-230. https://doi.org/10.3801/IAFSS.FSS.6-219 [ Links ]
32. Taylor AJ, McGwin G, Valent F, Rue L. Fatal occupational electrocutions in the United States. Injury Prevention. 2002;8(4):306-312. https://doi.org/10.1136/ip.8.4.306 [ Links ]
33. Dzansi D, Rambe P Mathe L. Cable theft and vandalism by employees of South Africa's electricity utility companies: A theoretical explanation and research agenda. J Social Sci. 2014;39(2):179-190. https://doi.org/10.1080/09718923.2014.11893281 [ Links ]
34. Peck MD. Epidemiology of burns throughout the world. Part II: Intentional burns in adults. Burns. 2012;38(5):630-637. https://doi.org/10.1016/j.burns.2011.12.028 [ Links ]
35. Fagot BI. The influence of sex of child on parental reactions to toddler children. Child Develop. 1978;49(2):459-465. https://doi.org/10.2307/1128711 [ Links ]
36. Block JH. Differential premises arising from differential socialization of the sexes: Some conjectures. Child Develop. 1983;54(6):1335-1354. https://doi.org/10.2307/1129799 [ Links ]
37. Eaton WO, Yu AP Are sex differences in child motor activity level a function of sex differences in maturational status? Child Develop. 1989;60(4):1005-1011. https://doi.org/10.2307/1131040 [ Links ]
38. Rosen BN, Peterson L. Gender differences in children's outdoor play injuries: A review and an integration. Clin Psychol Rev. 1990;10(2):187-205. https://doi.org/10.1016/0272-7358(90)90057-H [ Links ]
39. Forjuoh SN. The mechanisms, intensity of treatment, and outcomes of hospitalized burns: issues for prevention. J Burn Care Rehab. 1998;19(5):456-460. https://doi.org/10.1097/00004630-199809000-00019 [ Links ]
40. Begg S, Vos T, Barker B, Stevenson C, Stanley L, Lopez AD. The burden of disease and injury in Australia 2003. PHE 82. Canberra: Australian Institute of Health and Welfare; 2007. [ Links ]
41. Hyder AA, Kashyap K, Fishman S, Wali S. Review of childhood burn injuries in sub-Saharan Africa: A forgotten public health challenge: Literature review. Afr Safety Promotion. 2004;2(2):43-58. https://doi.org/10.4314/asp.v2i2.31610 [ Links ]
42. Peden M, Oyegbite K, Ozanne-Smith J, Hyder AA, Branche C, Rahman A, et al. World report on child injury prevention. Geneva: World Health Organization; 2009. [ Links ]
43. Ahuja RB, Bhattacharya S, Rai A. Changing trends of an endemic trauma. Burns. 2009;35(5):650-656. https://doi.org/10.1016/j.burns.2009.01.008 [ Links ]
 Correspondence:
Correspondence:
Craig Keyes
Email: craig.keyes@wits.ac.za
Received: 06 May 2020
Revised: 11 Dec. 2020
Accepted: 13 Dec. 2020
Published: 28 May 2021
Editors: Pascal Bessong; Sandiswa Mbewana
Funding: None


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}