










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Science
On-line version ISSN 1996-7489
Print version ISSN 0038-2353
S. Afr. j. sci. vol.117 n.3-4 Pretoria Mar./Apr. 2021
http://dx.doi.org/10.17159/sajs.2021/7428
RESEARCH ARTICLE
Clinical supervision in South Africa: Perceptions of supervision training, practices, and professional competencies
Shariefa HendricksI; Duncan J. CartwrightII; Richard G. CowdenIII
ICollege of Law and Management Studies, University of KwaZulu-Natal, Durban, South Africa
IISchool of Applied Human Sciences, University of KwaZulu-Natal, Durban, South Africa
IIIDepartment of Psychology, University of the Free State, Bloemfontein, South Africa
ABSTRACT
We investigated South African clinical and counselling psychology supervisors' (n=44) perceptions of supervision training, their supervision experiences, and their perceived competence, confidence and effectiveness in providing supervision. Results indicated that many supervisors prematurely engage in supervision responsibilities and initiate supervision prior to receiving formal training in supervision. With limited regulatory guidelines available on supervision training and practices in South Africa, the findings indicate a need for the South African psychology profession to establish a formal regulatory framework on supervision training and practices. This includes identifying supervision training needs, developing training programmes, and instituting formal training requirements for practitioners who participate in clinical supervision.
SIGNIFICANCE:
• The sample of South African clinical and counselling psychologists involved in the supervision of trainee psychologists tended to engage in clinical supervision in advance of obtaining three years of independent clinical practice and prior to receiving appropriate training in providing supervision.
• There is a need for the Professional Board for Psychology of the Health Professions Council of South Africa (PBP-HPCSA) to appropriately monitor and enforce ethical obligations of psychologists who engage in supervision of trainee psychologists.
• Psychologists who provide clinical supervision to trainee psychologists ought to take personal responsibility for ensuring that they are appropriately trained and have acquired the necessary competencies to provide supervision before deciding to engage in supervision activities.
• Formal guidelines and policies regulating clinical supervision are necessary for ensuring psychology supervisors obtain appropriate training in supervision and fulfil mandatory HPCSA-accredited supervision training requirements.
Keywords: competency, intern, professional development, counselling supervision, accredited training
Introduction
In recent years, considerable effort has been dedicated to frameworks, guidelines and regulations on competency-related requirements (e.g. training) of psychologists who engage in clinical supervision.1 In comparison to more developed countries (e.g. the UK, USA), South Africa has lingered behind global initiatives to improve standards of supervision practices.2 In South Africa, the directed master's degree in clinical, counselling, education or industrial psychology comprises two years. All trainee psychologists must complete a one-year coursework master's degree at an accredited university. In the second year of their studies, as psychology interns, trainee psychologists are required to undertake a 12-month supervised internship at a Health Professions Council of South Africa (HPCSA)-accredited institution.3
At present, the single competency prerequisite for psychologists prescribed by the regulatory body of health professions in South Africa (i.e. the Professional Board for Psychology of the Health Professions Council of South Africa (PBP-HPCSA)) is completion of at least three years of independent practice prior to supervising interns. The PBP-HPCSA4 considers a psychology supervisor or supervising psychologist as 'a senior psychologist who has been registered as a psychologist with the Board for more than three years'4(p.1). As such, supervision training represents a desirable qualification rather than an essential one. Presently, there appears to be an implicit expectation that supervisors draw on past supervision experiences and their skills as clinicians. This raises ethical concerns about competency and commencing supervisory responsibilities without relevant training.5
As per the PBP-HPCSA's clinical guidelines for internship, supervisors are required to work with psychology interns as they commence their clinical work during their 12-month internship by providing structured clinical supervision for at least two hours per week. The PBP-HPCSA offers clear ethical guidelines on the role of supervisors in (1) the professional development of the trainee and (2) ensuring the welfare of their trainees' clients. Psychologists undertaking supervisory responsibilities are obligated to provide supervision within the boundaries of their competence, training, education and supervised experience.3,6 Supervisors also serve as gatekeepers to the profession by ensuring that trainee psychologists are deemed competent to practice.
Supervision is a critical teaching method and a core component of training mental health professionals.7 Clinical supervision has emerged as a distinct field comprising unique theoretical perspectives, processes and skills, out of which recognised international standards of practice have developed.1, 8,9 However, very little research on clinical supervision has been conducted globally, and much of the existing body of work has focused on developed nations. Since the publication of the Standards for Counselling Supervisors10, the transformation and evolution from traditional supervision practice to competency-based supervision has spotlighted both the recognition and importance of supervision training2,11. The heightened interest in competency-based clinical supervision has also been stimulated by the formal development and implementation of regulatory guidelines and best practices in a number of developed nations, including the British Psychological Society, New Zealand Psychologists Board, Psychology Board of Australia, and the American Psychological Association.1,11
Salience of supervision training
The importance of training and competence in clinical supervision has gained considerable interest12, with specific attention devoted to the effects of training on supervisor and supervisee development13. Supervisor development is regarded as a developmental process that emphasises the acquisition of skills with structured training.14 Despite the importance of supervision in the professional training and development of psychology interns, formal training in supervision has generally been neglected as a core competency area in psychology.12 Several concerns involving competency to supervise have been raised, particularly supervisors' clinical competence and clinical supervision practices.15,16 In fact, a growing body of research has highlighted the negative implications of ineffective supervision experiences and the challenges faced by supervisors in the professional development of trainees17,18, which underscores the need for training in supervision. A number of studies have reported an increase in the incidence of inadequate, ineffective, and harmful supervision experienced during psychology training placements.19 In one recent study involving a sample of South African trainee psychologists, Hendricks and Cartwright20 found evidence of inadequate and potentially harmful supervision among psychology interns in South Africa. Research on supervision training continues to grow, yet research output on clinical supervision has been disproportionately lower in less developed nations, including South Africa.21 While numerous studies have focused on challenges facing clinical psychology training and mental health service provision in the country22,23, insufficient effort has been directed to understanding the extent and quality of training for supervisors24.
Some scholars have suggested that while training in supervision is far more readily and widely recognised, it remains an anomaly.9 In South Africa, supervision training is not considered a mandatory requirement for South African psychologists who supervise psychology trainees, and explicit regulations on supervision practices have not been promulgated by the PBP-HPCSA. This is surprising, given the compelling evidence in support of the potential efficacy of supervision training. First, it enhances supervisors' theoretical and conceptual knowledge, psychological readiness (e.g. self-confidence, self-awareness), and development of complex supervisory skills and techniques.25 This is purported to improve supervisors' understanding of their own supervision experiences and the supervision services offered to future psychologists.2 Second, there has been some support for the notion that supervision training increases motivation to supervise.26 Third, supervision training increases supervisory self-efficacy and lowers anxiety about the supervisory role.27-30 Conversely, a lack of education and training in supervision theory and practice may lead to insufficient supervisory preparation, which can compromise the supervisory relationship and inhibit trainee growth and clinical competence.31 Without training, novice supervisors may be disadvantaged by their limited experience, may be more inclined to perpetuate mistakes made by their own supervisors32, may not be aware of the need to develop proper supervision contracts, or may fail to participate in the requisite monitoring and evaluation of trainees.33
Developments in supervision training
Training and competence in supervision augment the supervisory process by ensuring supervisors are equipped with the necessary theoretical, organisational and management skills.34 However, the importance of supervision training has historically been underemphasised.2,35 Recently, Counselling and Psychology Boards (e.g. American Psychological Association's Division of Psychotherapy) have advanced the notion of competent practice1,25 and begun to mandate training and acquisition of skills germane to providing supervision. For example, the Council for Accreditation of Counseling and Related Educational Programs in the USA has made supervision training a mandatory requirement for counsellors at the doctoral level. Some international psychology boards (e.g. Psychology Board of Australia) also require psychologists to complete an approved training programme in the provision of supervision before being permitted to obtain board-level approval to offer supervision. Some scholars have stipulated mandatory peer supervision, professional accreditation, and licensure as prerequisites to supervise.12,36
More recent emphasis on competency-based practices of supervision represent a 'culture change' that as developed from reflections on the present status of professional psychology education and training.37 The competencies framework proposed by Falender et al.38 offers an intentional, systematic approach to supervision practice. The competency-based model is strengths-based and adopts a reflective, mindful approach to supervision. The model specifies a number of elements that should be addressed to ensure adequate training and development of the trainee and the role of the supervisor in that process.1 Competence also includes preventing and managing supervisee vicarious traumatisation, engaging in self-care, providing corrective and positive feedback, and managing and evaluating impaired or incompetent supervisees.1 Of the six core competencies outlined by Falender et al.38 - knowledge, skills, values, social context, overarching issues, and assessment of supervision competencies - five assert that providing competent supervision is an ongoing, complex process. Although this framework represents an important point of reference, more discourse is needed to determine the factors that contribute to competent clinical supervision.39 Training in supervision is markedly different from training in the provision of psychotherapy; it requires a substantive shift in vision and perspective.9 However, much like other areas of clinical training, training in supervision also requires designated curricula that guide supervision training and practices. In South Africa, training in the provision of supervision has not been prioritised. Presumably, work demands, teaching and lecturing commitments, high caseloads, limited staff capacity, resources, and budgetary or time constraints in public institutions limit opportunities for and availability of supervision training. Offering evidence in support of this, a qualitative study involving eight South African psychology internship supervisors found that none of the participants had received any formal training in supervision.40 These findings warrant further examination, as perceptions of psychologists' ability to provide supervision in South Africa have historically relied on the assumption that skills and knowledge gained from the clinical domain will automatically transfer to the supervisory domain.41 Although emergent research has speculated that inadequate training in supervision is tied to reduced confidence and self-perceived competence in providing supervision40, a comprehensive examination of South African internship supervisors' confidence, competence and effectiveness in the practice of supervision is necessary.
The present study
There have been several recommendations to methodologically examine and apply evidence-based practices to psychotherapy supervisor training.17,42 To date, there have been few attempts to examine the state of supervision training and practices in South Africa. Research suggests that the importance of training in supervision is gaining recognition, with many international credentialing and licensing boards monitoring the practice of supervision.1,43 Given that formal training in supervision is not currently implemented in South Africa and there are no formal requirements for training in supervision for clinicians mandated by the PBP-HPCSA in order to supervise psychology trainees, an improved understanding of the current state of supervision training and practices in South Africa is needed. Thus, the purpose of this study was to examine South African internship supervisors' perceptions of (1) supervision training and practices in South Africa and (2) their own supervision training, supervision experiences, and perceived abilities (e.g. competence, confidence, and effectiveness) in providing supervision.
Method
Participants
The sample consisted of 44 clinical and counselling psychology supervisors who were licensed to practise in South Africa. Participants were stratified into the following age groups: 25 to 34 (15.91%), 35 to 45 (45.45%), and 46 to 65 (38.64%) years of age. The majority of the sample consisted of female participants (68.18%). Participants self-identified as black (11.36%), coloured (15.91%), Indian (25.00%), white (40.91%), or 'other' (2.27%, unspecified race = 4.55%). Supervisors were employed at local universities (54.55%) or hospitals (36.36%), or were in private practice (9.09%) and had been practising for between 1 and 36 years (mean=14.28 years, s.d. = 7.97). Participants were required to have engaged in intern supervision for a minimum of a year (mean=10.33 years, s.d. = 7.23) in order to participate in the study.
Materials
The instrument used in this study contained a range of items that formed part of a broader project on intern training experiences and supervisors' experiences of supervision in South Africa. The items included in the current study were developed to measure different aspects of supervision training based on content areas (detailed below) explored in prior research.44 Participants were asked to respond to the items with reference to their supervision experience as psychologists and their experience as internship supervisors. After developing the initial set of items, a pilot study was performed to assess for content validity. The pilot sample (/7=5, female=60%) consisted of private (40%) and public sector clinical (60%) and counselling psychologists (meanage=40.40, s.d.age=3.56) with a mean of 10.60 years (s.d. = 5.94) of intern supervision experience. They provided qualitative feedback to several open-ended questions that was used to make appropriate revisions to the survey items.
The final set of items included in this study assessed a range of domains, including supervision training and experience (14 items; e.g. 'Had you had any formal training in supervision prior to assuming supervisory responsibilities?'), perceptions of the supervisory relationship and intern training (3 items; e.g. 'Which of the following form part of your training techniques in supervision?'),_supervisor self-ratings on various supervision skills (4 items; e.g. 'How would you rate the priority of supervision in comparison to your other professional tasks?'), Supervisor perceived suitability of interns (1 item; e.g. 'How confident are you in supervising interns perceived as incompetent?'), and intern evaluation and feedback (2 items; e.g., 'Rate your competence in evaluating interns'). Participants rated the items using the rating scales that were specific to each item (see Tables 1 to 4 for details on response options for each item).
Procedure
Ethical clearance to conduct the study was obtained from the University of KwaZulu-Natal's Human Social Sciences Research Ethics Committee (ethical clearance number HSS/1350/013D). We contacted and obtained permission from professional bodies and organisations, including the South African Association for Counselling and Development in Higher Education, HPCSA-accredited higher education institutions, public hospitals, and the Psychological Society of South Africa, to recruit participants from their respective databases of psychologists who met criteria for inclusion in this study. To be eligible, participants needed to (1) have professional registration within the clinical or counselling psychology scope of practise, (2) have at least one year's experience as a clinical supervisor, (3) have actively engaged in the supervision of psychology interns, and (4) be employed in either the private or public sector. A combination of purposive and snowball sampling techniques was used to recruit participants. Using this approach, 152 eligible supervisors working in the public and private sector were initially contacted to participate in this study. Although 75 supervisors agreed to participate, a total of 44 complete responses were received. Based on those who participated, the final response rate was 29%. Prospective participants were provided with a weblink that directed them to a secure data collection website, which ensured that participation was entirely anonymous. After providing online consent to participate in the study, participants completed the survey items. The items included in this study were a subset of items that formed part of a larger project. Participation was voluntary and participants were informed that they could withdraw from the study at any time without any penalties. All data were stored in password-protected electronic format.
Data analyses
Missing data diagnostics revealed 3.66% of missing values across 29.55% of cases. Analyses were computed using a pairwise deletion approach. Descriptive statistics were produced for all study variables. Bivariate associations were estimated using Spearman correlations, and group differences were detected using Wilcoxon rank-sum tests. Estimates of effect size are reported alongside bivariate inferential analyses. Values of 0.20, 0.50 and 0.80 for rs, and values of 0.04, 0.25 and 0.64 for epsilon squared (ε2), represent small, medium and large effects, respectively.45 All statistical analyses were performed in R46, with alpha set to 0.05.
Results
Univariate analyses
Supervision training
The results on supervision training are reported in Table 1. Only a small portion of participants (16.28%) indicated that they had received formal training in supervision prior to assuming supervision responsibilities, whereas a larger proportion (46.51%) reported receiving some form of training in supervision after assuming supervisory responsibilities. Among those who had received training in supervision, the most frequently cited mode of training was via a workshop (90.48%). The highest proportion (38.10%) reported being mostly satisfied with the training in supervision they had received. As an indicator of self-initiated continued professional development in supervision, a large proportion of the participants (44.19%) reported reading one scholarly article or book on supervision each month. However, 34.88% noted they did not engage in any scholarly reading on supervision. The highest proportion of participants (41.86%) also reported being somewhat prepared for supervision based on their master's-level training. Supervisors tended to rate the importance of receiving training in supervision as extremely important (53.85%), and the majority (88.64%) indicated that training in supervision should be mandatory.
To further examine areas of supervision training considered important to participants, those who reported that supervision training should be mandatory completed additional training component items they considered important to include in a supervision training programme (see Table 2). The training components that received the highest ratings of importance included ethics in supervision, managing supervisee resistance, conflict and power issues in supervision, dealing with boundary violations, and assessing and evaluating competencies. Comparably, components of supervisor training that were given lower ratings of importance were models of supervision, supervisory styles, and contracting in supervision.
Supervision experience
The average number of years of independent practice experience reported by the participants prior to engaging in supervisory responsibilities was 2.14 years (s.d. = 0.94). Most participants (79.07%) had less than the HPCSA's designated three-year minimum independent practice experience requirement before initiating supervision responsibilities. On average, participants reported supervising more than 30 (s.d.=34.87) trainee psychologists during their careers and currently supervised 2 trainee psychologists (s.d. = 1.50) for an average of 2.35 (s.d.=1.24) hours a week.
Supervision abilities and practices
The majority of supervisors (65.12%) indicated that their own positive experiences as supervisees often influence the manner in which they supervise, and the highest proportion of participants (38.64%) also reported negative experiences often influencing their supervision practices (see Table 3). All participants felt they had become more competent (100%) and confident (95.35%) in supervision over time, and the majority of supervisors (55.81%) perceived themselves to be somewhat effective in providing supervision. Most participants (63.41%) indicated that they did not make use of a formal model of supervision, although most (81.82%) noted that they sought supervision relating to their own supervisory performance.
The highest proportion of supervisors (48.84%) indicated that supervision was a high priority responsibility relative to other professional tasks. Almost half of the participants (46.51%) considered supervision to be moderately challenging.
With regard to the types of formal training techniques that participants used while providing supervision (see Table 4), the most commonly utilised supervision training technique was in-session observation (72.73%). The majority of supervisors also used audio taping (63.64%), role playing (56.82%), and supervision contracts (56.82%) as part of their training protocols. A minority of supervisors reported using video recordings (45.45%) and a two-way mirror (40.91%) to facilitate training of supervisees.
Bivariate analyses
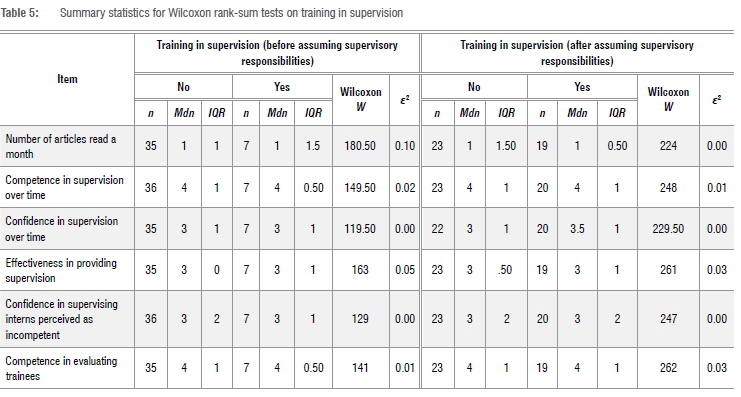
There were no significant differences in the quantity of scholarly articles and books on supervision read among participants who had received formal training in supervision, as compared to those who had not (see Table 5). There were no differences in perceived competence, confidence, or effectiveness in supervision between participants who had received formal training in supervision and those who had not. Supervisors who reported becoming more competent (rs=0.52, 95% CI [0.26, 0.71], p<0.05) and confident (rs=0.35, 95% CI [0.05, 0.59], p<0.05) in providing supervision over time tended to rate themselves as more effective in providing supervision. Participants who reported higher levels of prioritisation of supervision reported higher levels of self-perceived effectiveness in providing supervision (rs=0.40, 95% CI [0.11, 0.63], p<0.05). There was no evidence to suggest that confidence in supervising interns perceived as incompetent (rs= 0.08, 95% CI [-0.22, 0.37], p>0.05), or self-perceived competence in evaluating interns (rs= 0.02, 95% CI [-0.28, 0.31], p>0.05), are associated with years of supervisory experience. The extent to which participants perceived supervision as more challenging was unrelated to perceived effectiveness in providing supervision (rs= -0.16, 95% CI [-0.44, 0.15], p>0.05).
Discussion
In this study, we investigated supervisors' perceptions of supervision training, their supervision experiences, and their perceived abilities in providing supervision to obtain an understanding of the current state of supervision training and practice in South Africa. Overall, findings suggest that South African clinical supervisors perceive themselves to be at least somewhat effective in their supervisory engagements and appear to have developed confidence and competence over time. While internship supervisors considered supervision important and a high-priority professional responsibility, a negligible number of participants undertook formal training in supervision prior to assuming their supervisory responsibilities.
Formal training in supervision
A major finding of this study is the relative lack of supervision training reported by internship supervisors. Falender et al.12 consider training in supervision beneficial to perceived competence and effectiveness in providing supervision. Evidence suggests that supervisors are prone to perceiving themselves as underprepared for the supervisory role.47 The findings of this study are concerning, given research suggesting that practitioners with more training in supervision have a stronger understanding of the supervision process and the supervisory relationship, are more psychologically prepared (e.g. confident and motivated) and effective in providing supervision, and engage supervisees with less criticism and dogmatism.48,49 Therefore, training or preparation for supervision may enhance trainees' clinical training experiences, thereby increasing the likelihood that emerging practitioners acquire necessary professional skills and competencies via supervisors who have relevant knowledge and skills in the provision of supervision.20
Supervision training opportunities
Although the majority of supervisors included in this study rated training in supervision as highly important and indicated that supervision training should be mandated by the HPCSA, many had not completed formal training prior to assuming supervision responsibilities. This finding is consistent with supervision training patterns evidenced in prior studies involving non-South African samples48,50, but likely stems from the paucity of formal training opportunities available to supervisors in South Africa. Of those supervisors who had received some form of supervision training prior to initiating supervision practices, many reported attending professional workshops.
Even though supervision training choices may be directed by financial and time constraints, brief trainings (e.g. workshops) are often held intermittently and have restricted periods of knowledge transfer and acquisition34, ultimately affecting the quality of learning outcomes. Selected evidence supports the efficacy of short-term training initiatives (e.g. workshops) in promoting supervisor competence2,51, but there have been few studies examining the effectiveness of such in the South African context. The findings of this study highlight a need for the PBP-HPCSA to formulate formal supervision training guidelines and engage higher education institutions to develop training curricula for practitioners to complete prior to initiating supervision responsibilities.
Competence and confidence in supervision
The majority of supervisors included in this study felt confident and competent in their ability to supervise, which associated positively with perceived effectiveness in supervision. However, formal training in supervision was unrelated to perceptions of competence, confidence and effectiveness in supervising trainees. As many of the supervisors who completed training in supervision had attended short-term training programmes (e.g. workshops), it is plausible that South African supervisors develop their supervision skills and competencies through informal experiences, non-training avenues and clinical practice experience. However, clinical experience is not a sufficient prerequisite for ensuring competence in supervision49,52, and evidence suggests that formal didactic training in supervision is essential for appropriate supervisor development53,54. More importantly, self-perceived competency does not mean that a clinician has demonstrated competency as a supervisor.
Compliance with ethical guidelines
The finding that the majority of internship supervisors in this study prematurely commenced supervision of psychology interns in advance of obtaining three years of independent practice experience raises ethical concerns about the current practice of supervision in accredited training hospitals and higher education institutions in South Africa. It is speculated that this may sometimes arise out of limited supervision training opportunities, employment expectations imposed by employers or limited staff capacity and the absence of mandated supervision training by regulatory bodies (e.g. HPCSA). For example, Singh-Pillay found that South African supervisors employed in the public sector perceived supervision as an 'imposition and an unavoidable obligation'40(p.117). Further, supervisors often felt pressured into providing supervision without being adequately prepared - a process that necessitates an automatic transition from being a novice therapist to supervising trainees.40 Hence, there appears to be a false assumption that clinicians who supervise are competent to do so.55 This practice also inadvertently supports the assumption that clinical skills are a sufficient prerequisite for providing competent supervision36,56 and fails to recognise supervision as a distinct professional competence57.
Thus, South African internship supervisors may be conflicted between adhering to necessary employment requirements in the public sector and the ethical guidelines that govern the profession. For this reason, some internship supervisors may be unable to fully comply with the HPCSA's regulatory and professional practice guidelines and may compromise unwittingly to accommodate a system that has yet to completely appreciate and value the importance of training as a prerequisite to effective supervision practice.
Implications for supervision training and practice
Drawing on the findings of this study, there are a number of relevant practical implications for the training and practice of intern supervision in South Africa. First, the PBP-HPCSA may be providing inadequate monitoring and oversight to internship supervision practices in the country. Currently, there are no policies regulating psychologists to (1) obtain supervision training and accreditation and (2) fulfil mandatory, HPCSA-approved supervision training. This is inconsistent with international trends and regulations enforced by regulatory bodies in other countries (e.g. Psychology Board of Australia). Because the HPCSA has a critical role in ensuring mental health professionals provide services in accordance with ethical regulations, and that supervisors are charged with gatekeeping the profession and protecting those who seek mental health support, it is imperative that the HPCSA is at the forefront of developing, monitoring and enforcing supervision training and supervision practice guidelines.
Practitioners are also obligated to provide professional services in an ethically responsible manner. Engaging in supervision practices without requisite competencies represents a violation of ethical obligations and professional code of conduct. Acquiring supervision training should be a shared responsibility and supervisors should take personal responsibility for ensuring they are appropriately trained to provide supervision before deciding to engage in supervision activities. Considering supervisors' training may affect clinical and non-clinical (e.g. conflict resolution) interactions with trainees, the growth and professional development of interns may be compromised by supervisors' lack of training and inadequate competence in providing supervision. As such, there is an urgent need for the South African psychology profession to develop and implement a competency-based framework of supervisory training.57
Limitations and future research directions
The findings of this study should be considered alongside selected limitations. First, the low sample size may have contributed to truncated statistical power, lowering the likelihood of detecting significant effects in inferential analyses. Second, a combination of non-probability sampling techniques was used to recruit participants, which affects the representativeness of the sample and generalisability of the results to the larger professional population of practitioners engaged in supervision within South Africa. Further research is needed to determine how the pattern of South African internship supervisors' training and practices compare across (1) the different categories of psychology professions governed by the HPCSA in South Africa (e.g. clinical versus educational) and (2) other countries in which psychological services are offered and governed by professional bodies. Third, the cross-sectional design precludes determinations of causality. Research is needed to examine changes in supervisors' perceptions of competence and confidence over time, particularly as a function of access to and participation in training activities. Along similar lines, researchers are encouraged to examine the impact of supervision training on supervisors, their trainees' experiences in supervision, their professional development and clinical training outcomes.
Conclusion
In this study, we explored South African internship supervisors' perspectives on supervision training, their supervision experiences, and their perceived abilities in providing supervision. Overall, findings indicate that a large proportion of intern supervisors prematurely initiate supervision responsibilities and engage in supervision without receiving formal training. However, supervisors tended to become more confident and competent in providing supervision over time, with many perceiving themselves as effective in their supervisory responsibilities. Considering regulatory guidelines on supervision training requirements are not currently provided, coupled with the dearth of available supervision training opportunities in the country, there is a need for further study on intern supervision training and practices in South Africa, including access to training opportunities, evaluating supervision training needs, designing a training framework and curriculum, and instituting formal training requirements for practitioners who participate in clinical supervision.
Acknowledgements
This research was supported by the UKZN University Teaching and Learning Office (TLCRG15).
Competing interests
We declare that there are no competing interests.
Authors' contributions
The data reported here come from a PhD project that was conceptualised and designed by S.H. S.H. developed the online survey and was responsible for managing data collection. Input, critical review and supervision was provided by D.J.C. S.H. and R.G.C. contributed to the data analysis and interpretation of results. S.H. wrote the initial draft of the article. S.H. and R.G.C. provided critical commentary and revisions in preparing the article for publication. Funding acquisition for the study was the responsibility of S.H.
References
1. Falender CA. Clinical supervision in a competency-based era. S Afr J Psychol. 2014;44:6-17. https://doi.org/10.1177/0081246313516260 [ Links ]
2. McMahon M, Simons R. Supervision training for professional counselors: An exploratory study. Couns Educ Superv. 2004;43:301-309. https://doi.org/10.1002/j.1556-6978.2004.tb01854.x [ Links ]
3. Health Professions Council of South Africa. Health Professions Act, 1974 (Act no. 56 of 1974). Ethical rules of conduct for practitioners registered under the Health Professions Act, 1974; 2006. [ Links ]
4. Health Professions Council of South Africa (HPCSA). The professional board for psychology policy regarding intern psychologists: Guidelines for universities, internship training institutions and intern psychologists. Pretoria: HPCSA; 2014. [ Links ]
5. Russell RK, Petrie TA. Issues in training effective supervisors. Appl Prev Psychol. 1994;3:27-42. https://doi.org/10.1016/s0962-1849(05)80106-4 [ Links ]
6. American Psychological Association (APA). Ethical principles of psychologists and code of conduct [Revised]. Section 2.01. Washington DC: APA; 2017. [ Links ]
7. Barnett J, Molzon C. Clinical supervision of psychotherapy: Essential ethics issues for supervisors and supervisees. J Clin Psychol. 2014;70:1051-1061. https://doi.org/10.1002/jclp.22126 [ Links ]
8. Ellis MV. Critical incidents in clinical supervision and in supervisor supervision: Assessing supervisory issues. Train Educ Prof Psyc. 2006;S(2):122-132. https://doi.org/10.1037/1931-3918.s.2.122 [ Links ]
9. Watkins CE. Being and becoming a psychotherapy supervisor: The crucial triad of learning difficulties. Am J Psychother. 2013;67:135-151. https://doi.org/10.1176/appi.psychotherapy.2013.67.2.135 [ Links ]
10. Association for Counseling and Education. Standards for counseling supervisors. J Couns Dev. 1990;69:30-32. http://dx.doi.org/10.1002/j.1556-6676.1990.tb01450.x [ Links ]
11. Borders LD, Glosoff HL, Welfare LE, Hays DG, DeKruyf L, Fernando DM, et al. Best practices in clinical supervision: Evolution of a counseling specialty. Clin Superv. 2014;33:26-44. https://doi.org/10.1080/07325223.2014.905225 [ Links ]
12. Falender CA, Cornish JAE, Goodyear R, Hatcher R, Kaslow NJ, Leventhal G, et al. Defining competencies in psychology supervision: A consensus statement. J Clin Psychol. 2004;60:771-785. https://doi.org/10.1002/jclp.20013 [ Links ]
13. Ybrandt H, Armelius K. Changes in self-image in a psychotherapy supervisor training program. Clin Superv. 2009;28:113-123. https://doi.org/10.1080/07325220903343819 [ Links ]
14. Borders LD, Fong ML. Cognitions of supervisors-in-training: An exploratory study. Couns Educ Superv. 1994;33:280-293. https://doi.org/10.1002/j.1556-6978.1994.tb00294.x [ Links ]
15. Barnett JE. Ethical issues in clinical supervision. Clin Psych. 2011;64:14-20. https://doi.org/10.1037/e582572011-006 [ Links ]
16. Barnett J, Johnson W. Ethics desk reference for psychologists. Washington DC: American Psychological Association; 2008. https://doi.org/10.5860/choice.46-1823 [ Links ]
17. Watkins CE. Handbook of psychotherapy supervision. New York: Wiley; 1997. [ Links ]
18. Magnuson S, Wilcoxon SA, Norem K. A profile of lousy supervision: Experienced counselors' perspectives. Couns Educ Superv. 2000;39:189-202. https://doi.org/10.1002/j.1556-6978.2000.tb01231.x [ Links ]
19. Ellis MV Taylor EJ, Corp DA, Hutman H, Kangos KA. Narratives of harmful clinical supervision. Introduction to the special issue. Clin Superv. 2017;36:4-19. https://doi.org/10.1080/07325223.2017.1297753 [ Links ]
20. Hendricks S, Cartwright DJ. A cross-sectional survey of South African psychology interns' perceptions of negative supervision events. S Afr J Psychol. 2018;48:86-98. https://doi.org/10.1177/0081246317698858 [ Links ]
21. Watkins CE Jr. Psychoanalytic developmental psychology and the supervision of psychotherapy supervisor trainees. Psychodyn Prac. 2010;16:393-407. https://doi.org/10.1080/14753634.2010.510345 [ Links ]
22. Pillay AL, Ahmed R, Bawa U. Clinical psychology training in South Africa: A call to action. S Afr J Psychol. 2013;43:46-58. https://doi.org/10.1177/0081246312474411 [ Links ]
23. Pillay AL, Kramers-Olen AL. The changing face of clinical psychology intern training:A 30-year analysisof a programme in KwaZulu-Natal, South Africa. S Afr J Psychol. 2014;44:364-374. https://doi.org/10.1177/0081246314535683 [ Links ]
24. Milne DL, James IA. The observed impact of training on competence in clinical supervision. Br J Clin Psychol. 2002;41:55-72. https://doi.org/10.1348/014466502163796 [ Links ]
25. Falender CA, Shafranske EP. Clinical supervision: The state of the art. J Clin Psychol. 2014;70:1030-1041. https://doi.org/10.1002/jclp.22124 [ Links ]
26. Merlin-Knoblich C, Harris PN, Chung SY Gareis CR. Reported experiences of school counseling site supervisors in a supervision training program. J Sch Couns. 2018;16:1-33. [ Links ]
27. Nelson KW, Oliver M, Capps F. Becoming a supervisor: Doctoral student perceptions of the training experience. Couns Educ Superv. 2006;46:17-31. https://doi.org/10.1002/j.1556-6978.2006.tb00009.x [ Links ]
28. Lorenz D. Counseling self-efficacy in practicum students: Contributions of supervision [doctoral dissertation]. Pennsylvania: Pennsylvania State University; 2009. [ Links ]
29. Motley V Reese MK, Campos P Evaluating corrective feedback self-efficacy changes among counselor educators and site supervisors. Couns Educ Superv. 2014;53:34-46. https://doi.org/10.1002/j.1556-6978.2014.00047.x [ Links ]
30. Wheeler S, Richards K. The impact of clinical supervision on counsellors and therapists, their practice and their clients. A systematic review of the literature. Couns Psychother Res. 2007;7:54-65. https://doi.org/10.1080/14733140601185274 [ Links ]
31. Magnuson S, Wilcoxon SA, Norem K. A profile of lousy supervision: Experienced counselors' perspectives. Couns Educ Superv. 2000;39:189. https://doi.org/10.1002/j.1556-6978.2000.tb01231.x [ Links ]
32. Worthington EL. Changes in supervision as counselors and supervisors gain experience: A review. Prof Psychol. 1987;18:189-208. https://doi.org/10.1037/1931-3918.s.2.133 [ Links ]
33. Nielsen JA, Jacobsen CH, Mathiesen BB. Novice supervisors' tasks and training - A descriptive study. Nord Psychol. 2012;64:182-191. https://doi.org/10.1080/19012276.2012.731312 [ Links ]
34. Bernard JM, Goodyear RK. Fundamentals of clinical supervision. 5th ed. Boston, MA: Allyn & Bacon; 2014. [ Links ]
35. Milne DL, James IA. The observed impact of training on competence in clinical supervision. Br J Clin Psychol. 2002;41:55. https://doi.org/10.1348/014466502163796 [ Links ]
36. Milne DL, A.I. S, Pattison S, Wilkinson A. Evidence-based training for clinical supervisors: A systematic review of 11 controlled studies. Clin Superv. 2011;30:53. https://doi.org/10.1080/07325223.2011.564955 [ Links ]
37. Kaslow NJ, Falender CA. Valuing and practicing competency-based supervision: A transformational leadership perspective. Train Educ Prof Psyc. 2012;6:47-54. https://doi.org/10.1037/a0026704 [ Links ]
38. Falender CA, Shafranske EP Ofek A. Competent clinical supervision: Emerging effective practices. Couns Psychol Q. 2014;27:393-408. http://dx.doi.org/10.1080/09515070.2014.934785 [ Links ]
39. Rings JA, Genuchi MC, Hall MD, Angelo M-A, Cornish M, A EJ. Is there consensus among predoctoral internship training directors regarding clinical supervision competencies? A descriptive analysis. Train Educ Prof Psyc. 2009;3:140-147. https://doi.org/10.1037/a0015054 [ Links ]
40. Singh-Pillay ND. The unsaid: An interpretative phenomenological analysis to understanding non-disclosure in clinical supervision from trainee and supervisor perspectives [dissertation]. Durban: University of KwaZulu-Natal; 2016. [ Links ]
41. Hess AK. Psychotherapy supervision: Stages, Buber, and a theory of relationship. Prof Psychol-Res Pr. 1987;18:251-259. https://doi.org/10.1037//0735-7028.18.3.251 [ Links ]
42. Ellis MV Ladany N. Inferences concerning supervisees and clients in clinical supervision: An integrative review. In Watkins CE Jr, editor. Handbook of psychotherapy supervision,. Hoboken, NJ: John Wiley & Sons Inc.; 1997. [ Links ]
43. Desmond KJ, Rapisarda CA, Nelson JR. A qualitative study of doctoral student supervisory development. J Int Couns Educ. 2011;3:39-54. [ Links ]
44. Robiner WN, Saltzman SR, Hoberman HM, Schirvar JA. Psychology supervisors' training, experiences, supervisory evaluation and self-rated competence. Clin Superv. 1997;16:117-144. https://doi.org/10.1300/j001v16n01_07 [ Links ]
45. Ferguson CJ. An effect size primer: A guide for clinicians and researchers. Prof Psychol-Res Pr. 2009;40:532-538. https://doi.org/10.1037/14805-020 [ Links ]
46. R CoreTeam. R: A language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2019. [ Links ]
47. Uellendahl GE, Tenenbaum MN. Supervision training, practices, and interests of California site supervisors. Couns Educ Superv. 2015;54:274-287. https://doi.org/10.1002/ceas.12026 [ Links ]
48. DeKruyf L, Pehrsson DE. School counseling site supervisor training: An exploratory study. Couns Educ Superv. 2011;50:314-327. https://doi.org/10.1002/j.1556-6978.2011.tb01918.x [ Links ]
49. Ladany N, Bradley LJ. Counselor supervision: Principles, process and practice. 4th ed. New York: Routledge; 2011. [ Links ]
50. Studer JR, Oberman A. The use of the ASCA National Model in supervision. Prof Sch Couns. 2006;10:82-87. https://doi.org/10.5330/prsc.10.1.f82t14475451422m [ Links ]
51. Culloty T, Milne D, Sheikh AI. Evaluating the training of clinical supervisors: A pilot study using the fidelity framework. Cog Beh Ther. 2010;3:132-144. https://doi.org/10.1017/s1754470x10000139 [ Links ]
52. Lyon RC, Heppler A, Leavitt L, Fisher L. Supervisory training experiences and overall supervisory development in predoctoral interns. Clin Superv. 2008;27:268-284. https://doi.org/10.1080/07325220802490877 [ Links ]
53. McMahon M, Errity D. From new vistas to life lines: Psychologists' satisfaction with supervision and confidence in supervising. Clin Psychol Psychot. 2014;21:264-275. https://doi.org/10.1002/cpp.1835 [ Links ]
54. Stevens D, Goodyear R, Robertson P. Supervisor development. Clin Superv. 1998;16:73-88. https://doi.org/10.1300/J001v16n02_05 [ Links ]
55. Falender CA. Clinical supervision-the missing ingredient. Am Psychol. 2018;73:1240-1250. http://dx.doi.org/10.1037/amp0000385 [ Links ]
56. Gonsalvez CJ, Milne DL. Clinical supervisor training in Australia: A review of current problems and possible solutions. Aust Psychol. 2010;45:233-242. https://doi.org/10.1080/00050067.2010.512612 [ Links ]
57. Falender CA, Shafranske E. Clinical supervision: A competency-based approach. Washington DC: American Psychological Association; 2004. https://doi.org/10.1037/10806-000 [ Links ]
 Correspondence:
Correspondence:
Shariefa Hendricks
Email: Hendrs@unisa.ac.za
Received: 25 Sep. 2019
Revised: 26 May 2020
Accepted: 20 Sep. 2020
Published: 29 Mar. 2021
Editor: Pascal Bessong
Funding: UKZN University Teaching and Learning Office (TLCRG15)


{kind=link}