










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Science
versión On-line ISSN 1996-7489
versión impresa ISSN 0038-2353
S. Afr. j. sci. vol.116 no.1-2 Pretoria ene./feb. 2020
http://dx.doi.org/10.17159/sajs.2020/6095
RESEARCH ARTICLE
Psycho-hormonal effects of aerobic fatigue on collegiate female soccer players
Adele BroodrykI; Cindy PienaarI; David EdwardsII; Martinique SparksI
IPhysical Activity, Sport and Recreation Research Focus Area, Faculty of Health Sciences, North-West University, Potchefstroom, South Africa
IIPsychology Department, University of Zululand, KwaDlangezwa, South Africa
ABSTRACT
Up to 95% of a soccer match entails aerobic actions that may cause fatigue. Little is known about the effects of fatigue on the hormonal and psychological states of female players. Cortisol values (saliva sample), state anxiety (Spielberger State-trait Anxiety Inventory) and mood scores (Incredibly Short Profile of Mood States [ISP], comprising six subscales and total mood disturbances [TMD]) of 43 female players (aged 22.0±2.7 years) were taken immediately prior to and 15 min after an aerobic fatiguing test (AFT: Yo-Yo Intermittent Recovery [YYIR] test). Cortisol increased (d=0.7, p=0.007) and ISP-confusion and ISP-vigour decreased (d=0.5, p=0.01-0.02). At pre-AFT, a slight positive relationship between cortisol and anxiety-absence (r=0.3, p=0.05) was seen. TMD consistently demonstrated a strong relationship with all ISP and anxiety scores (r>0.4, p<0.01). Post-AFT results demonstrated a positive relationship between cortisol and blood lactate (r=0.3, p=0.04), between ISP-anger with maximal heart rate (r=0.3, p=0.03), ISP-anger and YYIR level as well as ISP-fatigue (r=0.4, p=0.04), and between perceived exertion rate and ISP-vigour (r=-0.4, p=0.008) as well as ISP-fatigue (r=0.3, p=0.05). Fatigue caused by prolonged activity may be a greater physiological than psychological stressor, although both may affect soccer performance. We recommend training players to increase their aerobic capacity to ensure maximal quality match-time before fatigue and its subsequent adverse physiological and psychological effects set in.
SIGNIFICANCE:
•The YYIR-1 test is effective in producing significant changes in both the hormonal and psychological states of female soccer players.
•Conditioning staff can effectively implement a mood state questionnaire to predict possible psychological stress (increase in state or trait anxiety) prior to and after a stressor.
•A relationship exists between cortisol and the absenteeism of anxiety prior to this fatiguing test, as well as with blood lactate thereafter. Therefore, the State-trait Anxiety Inventory questionnaire can be administered and blood lactate samples can be collected as they may display sensitive information regarding hormonal state.
•A positive relationship exists between the maximal heart rate achieved following an aerobic fatiguing test and various mood subscales experienced. Thus, with an increase in heart rate (as frequently observed due to fatigue), it can be assumed that an increase in perceived negative mood state might take place
Keywords: cortisol, mood, anxiety, football, exhaustion
Introduction
Soccer is characterised by players performing submaximally for a prolonged period, with fatigue commonly observed due to the inability to endure the required work rate for the entire match.1,2 Most actions are executed at a submaximal exertion level, dominating up to 95% of the work-rate profiles during a match.2-4 Thus, a large aerobic capacity is needed to maintain high performance throughout a 90-min match; in the absence of large aerobic capacity, fatigue may set in either at the peripheral (outside the central nervous system) or central (within the central nervous system) sites of the body, with debilitating physiological and psychological consequences.1,3,5 Physiologically, fatigue (perceived as the 'sense of effort') reflects the dominance of the motor drive from the cerebral cortex to the motor neurons, whereas psychologically it reflects the exercise capacity.5
It is important when planning training sessions to determine when and why fatigue occurs during a match.6 Fatigue usually arises during the second half of a game and is manifested by a decline in specific playing ability (less distance covered, sprints completed and ball contact) and, ultimately, physical performance.1 There may be several physiological reasons for fatigue (such as depleted glycogen stores, hyperthermia, changes in muscle pH and muscle creatine phosphate concentrations, and increased muscle lactate concentrations),6 although owing to the large load placed on the aerobic system during a match, it is argued that fatigue arises from effects on the aerobic system. During prolonged activities (when aerobic glycolysis is the primary energy source), a depletion in glycogen stores and an increase in glucose consumption by the muscle tissues take place.5,6 Although the aerobic system is extremely taxed during a match, limited research is available regarding the fatigue experienced during training on the physiological and psychological domains. Hence, examining the effects of fatigue during exercise is an area of concern in studies of the physiology and psychology of sport.5
The effects of exercise on mood are influenced by various factors, among others neurobiological features, player characteristics, features of the exercise and psychological state.7,8 Studies have reported increased positive and reduced negative mood (such as tension, anger, fatigue and confusion) and anxiety states following various aerobic exercises9-11, partially due to the release of endorphins whilst training8. Furthermore, for every 30 min of training (≥60% VO2max), there is a progressive improvement in mood for various psychological states - including state anxiety, depression, confusion, fatigue and extent of mood disturbances overall.7,10 However, when prolonged physical exertion becomes distressing, cortisol (the main stress hormone) is secreted.12
The secretion of cortisol is modulated by the hypothalamic-pituitary-adrenocortical axis12, which is important for normal physiological functioning and cognitive and affective processes12. Physiologically, cortisol is involved in providing energy for muscle tissue by increasing blood glucose levels12 and promoting/inhibiting inflammatory processes13. Psychologically, it is associated with various behaviours such as expression of mood and anxiety.14 Because of the bidirectional relationship between hormones and behaviour15, it is speculated that improvements in mood might modify the perception of stressors, which subsequently can alter the release of cortisol, and vice versa16,17. This has been reported previously with increased positive mood states reducing cortisol responses (F(1,901)=5.86, p<0.05), compared to negative mood states raising them (F(1,901)=6.91, p<0.01).17 Furthermore, training has been shown to increase (p<0.05) cortisol secretion by up to 36%18, although a larger increase (250%) was described after a soccer match14. This indicates the necessity to maximise the match components, and more specifically the aerobic basis, to minimise the incidence of increased negative psychological states and cortisol due to fatigue.
The influence of aerobic fatigue on the hormonal and psychological states of female soccer players is of practical interest in view of its large role during match play, and the importance of these components for maximal performance on the field. Based on an extensive literature review and searches, we found no published research on the effect of an aerobic fatiguing test (AFT) on the psycho-hormonal state of female soccer players in South Africa and, more broadly, in Africa. The aim of our study was, therefore, first to evaluate the effect of an AFT on the anxiety, mood and cortisol levels of these players; and second, to determine what associated relationships prevail between anxiety, mood and cortisol levels and/or the AFT. Such knowledge will aid coaches, sport scientists and sport psychologists in determining whether fatigue due to prolonged physical exertion may lead to physiological and/or psychological stress in players and whether it adversely influences their performance.
Materials and methods
Subjects
A total of 43 female university students who were soccer players at the time of the study volunteered to partake (age: 22.0±2.7 years; stature: 158.5±5.9 cm; mass: 54.1±6.2 kg, competitive playing experience: 8.2±4.8 years). They all reported being healthy at the start of testing and were excluded if they became injured or ill, or did not complete all the tests. They experienced normal day-to-day stressors as registered students committed to their academic tasks. The specific testing regime was compiled in accordance with their soccer training schedule (training 3-5 times/week) to prevent overtraining. Their internal training load was monitored during the testing period by means of their maximal heart rate (HRmax) and perceived exertion rate (RPE).
During the testing period they were in their competitive training phase, with average VO2max values of 41.0±1.5 mL/min/kg. An average total sleep duration of 7.7±2.3 h the night before the tests was reported. The majority of participants was in the luteal phase of their menstrual cycle, and none was on oral contraceptives or prescribed medication, as testified in the information questionnaire.
Design
It was postulated that the AFT would result in a statistically significant increase (p<0.05, d≥0.8) in salivary cortisol and total mood disturbances (TMD). A linear relationship between anxiety, cortisol and/or TMD was expected. A repeated measure, quantitative research design was adopted to test the hypothesis. Information was collected using various questionnaires and a test battery. Ethical approval was provided by the Health Research Ethics Committee of the North-West University, South Africa (NWU-00055-15-A1) and all principles of the Declaration of Helsinki were adhered to.
Methodology
The study was completed over two consecutive days, two weeks prior to the main tournament. On the first day, written consent was obtained and the testing procedures were explained to the participants. During this period, participants were granted the opportunity to ask questions. They were advised to obtain a good night's rest (at least 8 h sleep), to wake up between 6:00 and 7:00 and to have their last meal at least an hour before the start of testing.
Upon arrival on the second day, each student's body mass (BFW platform scale, Adam Equipment Co. Ltd., UK) and stature (Harpenden portable stadiometer, Holtain Ltd., UK) were recorded. Following a 15-min warm-up session comprising aerobic, stretching and sport-specific activities, the participants rinsed their mouths with lukewarm water to remove any food substances, and after a period of 10 min their saliva was sampled. In this period, they were fitted with a Fix Polar Heart Rate Transmitter Belt (Polar Electro, Kempele, Finland) to monitor the HRmax obtained post-AFT, and completed the psychological questionnaires. After 10 min, they provided a saliva sample (pre-AFT) and completed the AFT with the Yo-Yo Intermittent Recovery (YYIR)-1 test. Immediately thereafter, the players' RPE, HRmax and blood lactate (BLa-) were recorded, with the last saliva sample and questionnaires completed 15 min post-AFT.
Saliva sampling
Saliva samples were collected using the passive drool test for the assessment of cortisol.19 If needed, the participants could chew on a piece of Parafilm™ to stimulate saliva flow. Saliva was then collected through a plastic straw into a 20-mL collection vial, after which the sample was stored in a fridge (at 4±1 ºC) and transported to a qualified laboratory for analysis.19 The cortisol concentrations were determined from 20-µL saliva samples by using a luminescence immunoassay. The samples were transferred into a Berthold luminometer to determine the average relative luminescence units, after which they were converted to exact values by plotting against the cortisol concentrations. This method has a non-linear (r=1.0) and linear correlation coefficient (r=0.8) with serum cortisol values, with an intra-CV (correlation of variation) range of 0.4-1.7% and inter-CV range of 0.8-1.8%.20 The first sample was collected following warm-up (immediately prior to the AFT), and the last sample 15 min post-AFT, as previous studies have demonstrated that mean cortisol values peak at 10-30 min following a stressor.16
Sport-psychology questionnaires
Mood states
Mood states were evaluated pre- and post-AFT by using the Incredibly Short Profile of Mood States (ISP) questionnaire derived from the original Profile of Mood States questionnaire21 by Dean and colleagues22. The ISP consists of six questions targeting the same subscales (involving anger, depression, tension, confusion, fatigue and vigour). Correlations between the two questionnaires (r=0.67-0.82)22, as well as between the six subscales (r=0.72-0.83), have been reported previously23. The participants rated the questions on a five-point Likert scale from 1 ('not at all') to 5 ('extremely'). Individual scores for each subscale were the rating indicated per question and the TMD score was calculated by adding the negative and subtracting the positive scales.
Anxiety
The participants' perceived anxiety levels pre- and post-AFT were estimated from the results obtained from the state-subscale (SAI) of the original State-Trait Anxiety Inventory.24 The state-anxiety scale consists of 20 statements that evaluate how respondents feel 'right now, at this moment' on a four-point Likert scale, ranging from 1 ('not at all') to 4 ('very much so'). Trait anxiety was not measured, as it evaluates how a person feels 'in general' and was therefore not within the scope of this study. Total anxiety scores were determined by calculating the sum of the different scores; thereafter the two state-subscales (anxiety - present and absent) were calculated. The scores range from 20 to 80; the higher the score, the greater the anxiety perceived.24 Internal consistency has been demonstrated for state anxiety (r=0.91) over a wide range of studies and participants.25
Aerobic fatiguing test
A YYIR-1 test was performed to tax the participants' aerobic system maximally to induce aerobic fatigue.26 The test was executed as described by Bangsbo and colleagues6 to measure the participants' HRmax and VO2max values while performing intervals over a prolonged period of time. The test was conducted on a flat, clearly marked 20-m stretch of a grass soccer field with the players wearing their soccer boots. The following measurements were made: total distance covered (m), YYIR-1 level completed, HRmax, BLa- and RPE. There is a high correlation for female soccer players between BLa- and the YYIR-1 test (r=0.73, p=0.003), the total distance covered (r=0.64, p=0.014) and the amount of high-intensity running (r=0.83, p<0.001) covered during a match.4
Immediately post-AFT, BLa- (mmol/L) was measured by collecting a blood sample from a finger prick of the left hand and transferring this to a portable analyser (Lactate Pro, Arkray, Japan). Prior to collection, the portable analyser was calibrated according to the manufacturer's guidelines. This reading was measured as BLa- and can be an indication of the degree to which the aerobic and anaerobic glycolysis systems are taxed during the test, and can confirm that the onset of fatigue occurred, as values above 8 mmol/L have been reported for soccer players.27 The participants then indicated their RPE on a 10-point Borg scale, with 1 being the lowest and 10 the highest perceived exertion level.28
Statistical analyses
IBM SPSS (v. 24.0.0.0) was used to analyse the data. Descriptive statistics (means, maxima, minima and standard deviation values) were calculated at every time point for each variable. Linear mixed model analyses were then conducted to investigate time-point differences with an autoregressive 1 covariance structure.
Next, the variables were categorised into three rankings (low, average/neutral and high) as derived from the results for each time point. Prior to their ranking, the cortisol values were adjusted according to the awakening and sample collection times.29 The score for each ranking at each time point was then expressed as a percentage of the total score for the specific variable as calculated by chi-squared analysis, with practical significance indicated by Cramer's V values.
Finally, Pearson's rank correlation, rho, determined the relationship between the variables (cortisol, TMD and anxiety) and AFT. A Fisher's r to z transformation was calculated to determine the 90% confidence interval (CI) from the correlation coefficient. The level of significance was set at p≤0.05. The strength of the correlation was categorised from ≤0.01 to ≥1 (perfect). In each case, magnitudes of standardised effects ± 95% confidence interval (d±95% CI) were calculated and interpreted as: d≥0.8 (large), d≥0.5 (moderate) and d≥0.2 (slight). Effect sizes with wide confidence intervals that overlap categorical classifications of effect were downgraded as 'unclear'.
Results
The average results for the AFT were: level: 14.1±0.9; total distance: 560.9±212.8 m; HRmax: 190.1±8 bpm; BLa-: 10.9±3.6 mmol/L; RPE: 7.1±1.9. Only 36 complete sets (cortisol and full questionnaires at pre- and post-AFT) were used for analysis, with incomplete sets excluded.
Cortisol results
Cortisol increased significantly (52.2%) (F(2,216) =5.2; p=0.007, d=0.7 CI: 0.3-1.2). The total number of cortisol values rated as 'high' increased significantly from pre- to post-AFT (pre-AFT: 28.2% to post-AFT: 59%, p<0.01, V=0.4).
Psychological results
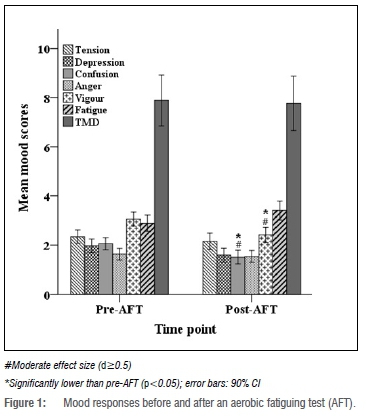
Only the ISP subscales confusion (pre-AFT=2.1, post-AFT=1.5, p=0.01, d =0.6 CI: 0.2-1.1) and vigour (pre-AFT=3.1, post-AFT=2.4, p=0.02, d=0.6 CI: 0.2-1.1) showed moderate decreases from pre- to post-AFT (Figure 1). The subscale anxiety-absence was larger than anxiety-present (pre-present = 16.5±5.0, pre-absent = 21.6±6.0, post-present = 16.2±5.1, post-absent = 22.5±6.6), although a moderate effect was seen in the anxiety-present scores from pre- to post-AFT (d=0.5 CI: 0.07-1.0).
Hormonal and psychological relationship results
At pre-AFT, a slight positive relationship between cortisol and anxiety-absence (r=0.3, p=0.05) was seen. TMD demonstrated a strong relationship with all ISP and anxiety scores (r>0.4, p<0.01). Post-AFT results demonstrated a positive relationship between cortisol and BLa- (r=0.3, p=0.04), between ISP-anger and HRmax (r=0.3, p=0.03), ISP-anger and YYIR-level as well as ISP-fatigue (r=0.4, p=0.04), and between RPE and ISP-vigour (r=-0.4, p=0.008) as well as ISP-fatigue (r=0.3, p=0.05).
Discussion
The most significant observation from the current study was the increase in cortisol with only two mood subscales (vigour and confusion) decreasing following an aerobic fatiguing test. This suggests that aerobic fatigue, as frequently observed during a match, primarily influences the individual's physiology and its underpinnings rather than the psychological state. In addition, a positive relationship between cortisol and anxiety-absence and between cortisol and BLa- was observed. The mood and anxiety scores correlated strongly at all times, whereas some mood subscale scores correlated with the AFT measurements. We therefore propose that a connection exists between physiological and psychological states when dealing with a physical stressor.
The sensation of fatigue during training is common due to the increased training load and decreased energy stores of the athletes involved.5 These sensations can be related to both psychological and physiological states, as exercise affects both a person's physiology and neuromuscular condition.5
Hormonal responses
The significant cortisol increase is similar to that reported previously18,30, following either a 30-min treadmill run18 or after a high-intensity resistance training session30. As evident in the results, a linear relationship exists between cortisol and physical exertion.30 In this regard, training below 60% VO2max decreases cortisol31, whereas training above 60% VO2max generally increases cortisol either to aid in the metabolism and mobilisation of energy sources in providing sufficient fuel, or as a consequence of its secretion exceeding its removal.12,32 In addition, the high BLa- and HR values recorded following the test might indicate a quicker onset of fatigue owing to the participants' training status (average rated VO2max values), which has the ability to influence hormonal response patterns,30 as seen from the correlation between cortisol and BLa-.
Psychological responses
As seen from the negative correlation between ISP-vigour and RPE, fatigue caused vigour to decrease during the test. The significant reduction in the players' state of confusion might be attributed to them becoming familiar with the specific test, as it was completed regularly during the tournament season. Previous research reported a significant decrease in tension, anger, fatigue and confusion following a treadmill session at 61% HRmax.9 During aerobic training the body releases endorphins (the natural mood-enhancing hormones), with a particular release threshold reached at higher training loads.8 Although no significant changes in anxiety were reported, previous research demonstrated reduced anxiety levels following aerobic training.10,33 This might be due to studies proposing training sessions of at least 30 min to stimulate the release of endorphins and provoke well-being improvements.7,8,10 Finally, negative mood states did not increase as postulated, possibly due to the maintenance of a coherent mood state, as the training session offered a diversion from the tensions of normal life; alternatively, the positive feelings followed the accomplishment of a specific task, the AFT.8
The positive relationship found between the TMD and anxiety at all times is similar to that reported by Guszkowska and Sionek34. They reported a correlation between trait anxiety and various mood subscales (tension and vigour) following a training programme. Although not the sole measurement, an anxiety subscale was examined in the ISP questionnaire, which might explain this relationship. This noteworthy observation makes it possible to use this questionnaire to indicate a participant's state of anxiety.
Hormonal and psychological relationships
Not only is cortisol physiologically involved during exercise, but also psychologically.15 Research indicates a link between the higher central nervous system's functioning and the neuroendocrine system, together with the psychological sense of training.5 Whereas our findings demonstrated only a slight positive relationship between cortisol and the absence of anxiety pre-AFT, Haneishi and colleauges14 described a higher positive correlation between cortisol and cognitive anxiety prior to training (r=0.7). However, they did not report the specific training regime, making it possible that more intense training was expected.17 Our subjects, on the other hand, were familiar with the specific fatigue test, thus reducing their perceived anxiety.
Although anxiety questionnaires are primarily developed to detect anxiety changes, it is plausible that other variables, such as cortisol fluctuations, might be detected, as researchers believe that our emotions are influenced by physiological processes and vice versa.35 A possible explanation for this relationship is the bottom-up approach - a stressful situation can result in various negative emotions, leading to erratic heart rates, taxing the nervous system, activating the hypothalamic-pituitary-adrenocortical axis (thereby resulting in the secretion of cortisol) and, subsequently, impeding the psychophysiological system.35 Therefore, implementing a psychological questionnaire could be functional to detect not only underlying psychological states, but also physiological states needed to enhance performance.
Practical application
Aerobic fatigue elicits a greater physiological than psychological stress response (which might be due to the depletion of energy stores). Players and their coaches could therefore focus on maximising the aerobic component, as it may contribute to longer quality match-time for players before fatigue sets in.
Seven data sets were excluded - either due to saliva samples not being thoroughly analysed or because questionnaires were incomplete. Subjects acknowledged that the SAI is lengthy and that they did not complete all the questions. Therefore, future studies could instead implement the ISP questionnaire as it correlated strongly with the SAI. Furthermore, a thorough analysis of participants' sleep could be obtained for plausible explanations on the hormonal and/or psychological states.
Due to the circadian rhythm of cortisol, the saliva collection times should have been limited to a specific time period to exclude potential outliers. Additionally, the fitness levels of the subjects could have been a confounding factor, as fitness affects onset of fatigue. Future studies could take into account the current readiness level by making use of physical and/or psychological inclination questionnaires.
Conclusion
To our knowledge, this study is the first to evaluate the effect of an AFT on the hormonal and psychological states of female soccer players in South Africa and, more generally, in Africa. The investigation demonstrated that an AFT, such as the YYIR test, led to an increase in cortisol and a decrease in vigour. The easy administration of the YYIR-1 test, together with its soccer-specific nature, makes it a useful tool for future evaluations to monitor soccer-specific fitness and hormonal changes. The positive relationship observed between cortisol and anxiety-absence can enable coaches to use the questionnaire to anticipate cortisol responses as a reaction to aerobic fatigue. Our study affirms the negative effects of fatigue due to prolonged activity on the players' psychophysiological state.
Acknowledgements
We thank the players and coaches of the respective soccer teams. We also thank all the field personnel actively involved during the data capturing process. The project was funded by the National Research Foundation of South Africa (grant no 105506:27) and the Physical Activity, Sport and Recreation Research Entity of the North-West University (2015:01). We also thank the anonymous reviewers for their time and effort in reviewing this manuscript.
Authors' contributions
A.B. was responsible for conceptualising the research goals and aims, developing the methodology, data collection, applying statistical techniques to analyse the data and preparing and creating the published work as well as reviewing and revising the work. M.S. was responsible for conceptualising the research goals and aims, developing the methodology, data collection, validating the experimental process and results, overall project leadership and management, student supervision and reviewing and revising the writing. C.P. was responsible for conceptualising the research goals and aims, developing the methodology, data collection, student supervision and reviewing and revising the writing. D.E. was responsible for student supervision and reviewing and revising the writing.
References
1.Reilly T, Drust B, Clarke N. Muscle fatigue during football match-play. Sport Med. 2008;38(5):357-367. https://doi.org/10.2165/00007256-200838050-00001 [ Links ]
2.Carling C, Bloomfield J, Nelsen L, Reilly T. The role of motion analysis in elite soccer. Sport Med. 2008;38(10):839-862. https://doi.org/10.2165/00007256-200838100-00004 [ Links ]
3.Robineau J, Jouaux T, Lacroix M, Babault N. Neuromuscular fatigue induced by a 90-minute soccer game modeling. J Strength Cond Res. 2012;26(2):555-562. https://doi.org/10.1519/jsc.0b013e318220dda0 [ Links ]
4.Krustrup P, Mohr M, Ellingsgaard H, Bangsbo J. Physical demands during an elite female soccer game: Importance of training status. Med Sci Sports Exerc. 2005;37(7):1242-1248. https://doi.org/10.1249/01.mss.0000170062.73981.94 [ Links ]
5.Ament W, Verkerke G. Exercise and fatigue. Sport Med. 2009;39(5):389-422. [ Links ]
6.Bangsbo J, Mohr M, Krustrup P. Physical and metabolic demands of training and match-play in the elite football player. J Sports Sci. 2006;24(7):665-674. https://doi.org/10.1080/02640410500482529 [ Links ]
7.McDowell CP, Campbell MJ, Herring MP. Sex-related differences in mood responses to acute aerobic exercise. Med Sci Sports Exerc. 2016;48(9):1798-1802. https://doi.org/10.1249/mss.0000000000000969 [ Links ]
8.Rocheleau CA, Webster GD, Bryan A, Frazier J. Moderators of the relationship between exercise and mood changes: Gender, exertion level, and workout duration. Psychol Health. 2004;19(4):491-506. https://doi.org/10.1080/08870440310001613509 [ Links ]
9.Chase R, Hutchinson J. The effects of acute aerobic exercise versus resistance exercise on mood state. J Multidisciplinary Res. 2015;7(2):15-16. [ Links ]
10.Cox RH, Thomas TR, Hinton PS, Donahue OM. Effects of acute 60 and 80% VO2max bouts of aerobic exercise on state anxiety of women of different age groups across time. Res Q Exerc Sport. 2004;75(2):165-175. https://doi.org/10.1080/02701367.2004.10609148 [ Links ]
11.Byrne A, Byrne DG. The effect of exercise on depression, anxiety and other mood states: A review. J Psychosom Res. 1993;37(6):565-574. https://doi.org/10.1016/0022-3999(93)90050-p [ Links ]
12.Dickerson SS, Kemeny ME. Acute stressors and cortisol responses: A theoretical integration and synthesis of laboratory research. Psychol Bull. 2004;130(3):355-391. https://doi.org/10.1037/0033-2909.130.3.355 [ Links ]
13.Chennaoui M, Bougard C, Drogou C, Langrume C, Miller C, Gomez-Merino D, et al. Stress biomarkers, mood states, and sleep during a major competition: 'Success' and 'failure' athlete's profile of high-level swimmers. Front Physiol. 2016;7(94):1-10. https://doi.org/10.3389/fphys.2016.00094 [ Links ]
14.Haneishi K, Fry AC, Moore CA, Schilling BK, Li Y, Fry MD. Cortisol and stress responses during a game and practice in female collegiate soccer players. J Strength Cond Res. 2007;21(2):583-588. https://doi.org/10.1519/r-20496.1 [ Links ]
15.Nelson RJ. An introduction to behavioral endocrinology. 4th ed. Sunderland, MA: Sinauer Associates Inc.; 2011. [ Links ]
16.Kirschbaum C, Hellhammer DH. Salivary cortisol. In: Fink IG, editor. Encyclopedia of stress. 3rd ed. San Diego, CA: Academic Press; 2000. p. 379-384. [ Links ]
17.Smyth J, Ockenfels MC, Porter L, Kirschbaum C, Hellhammer DH, Stone AA. Stressors and mood measured on a momentary basis are associated with salivary cortisol secretion. Psychoneuroendocrinology. 1998;23(4):353-370. https://doi.org/10.1016/s0306-4530(98)00008-0 [ Links ]
18.Karacabey K, Saygin O, Ozmerdivenli R, Zorba E, Godekmerdan A, Bulut V. The effects of exercise on the immune system and stress hormones in sportswomen. Neuroendocrinol Lett. 2005;26(4):361-366. https://doi.org/10.1080/13102818.2004.10817142 [ Links ]
19.Salimetrics LLC, SalivaBio LLC. Saliva collection and handling advice. In: Methods. 3rd ed. State College, PA: Salimetrics LLC, SalivaBio LLC; 2011. p. 1-14. Available from: www.salimetrics.com [ Links ]
20.Westermann J, Demir A, Herbst V. Determination of cortisol in saliva and serum by a luminescence-enhanced enzyme immunoassay. Clin Lab. 2004;50(1-2):11-24. [ Links ]
21.McNair DM, Lorr M, Droppleman LF. Profile of mood states. San Diego, CA: Educational and Industrial Testing Service; 1981. p. 1-29. [ Links ]
22.Dean JE, Whelan JP, Meyers AW. An incredibly quick way to assess mood states: The incredibly short POMS. Paper presented at: Annual Conference of the Association for the Advancement of Applied Sport Psychology; 1990 October; San Antonio, TX, USA. [ Links ]
23.Bourgeois A, Leunes A, Meyers M. Full-scale and short-form of the Profile of Mood States: A factor analytic comparison. J Sport Behav. 2010;33(4):355-376. [ Links ]
24.Spielberger CD. Manual for the State-Trait Anxiety Inventory STAI (Form Y) ('self-evaluation questionnaire'). In: UBIR Repository. 1983. http://hdl.handle.net/10477/1873 [ Links ]
25.Barnes LLB, Harp D, Jung WS. Reliability generalization of scores on the Spielberger State-Trait Anxiety Inventory. Educ Psychol Meas. 2002;62(4):603-618. https://doi.org/10.1177/001316402128775049 [ Links ]
26.Bangsbo J, Iaia FM, Krustrup P. The Yo-Yo Intermittent Recovery Test. Sports Med. 2008;38(1):37-51. http://dx.doi.org/10.2165/00007256-200838010-00004 [ Links ]
27.Svensson M, Drust B. Testing soccer players. J Sports Sci. 2005;23(6):601-618. [ Links ]
28.Borg G. Perceived exertion: A note on history and methods. Med Sci Sports Exerc. 1973;5:90-99. [ Links ]
29.Broodryk A, Pienaar C, Edwards D, Sparks M. The psycho-hormonal influence of anaerobic fatigue on semi-professional female soccer players. Physiol Behav. 2017;180(August):8-14. Available from: http://linkinghub.elsevier.com/retrieve/pii/S0031938417302329 [ Links ]
30.McGuigan MR, Egan AD, Foster C. Salivary cortisol responses and perceived exertion during high intensity and low intensity bouts of resistance exercise. J Sports Sci Med. 2004;3(1):8-15. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3896117&tool=pmcentrez&rendertype=abstract [ Links ]
31.Crewther BT, Hamilton D, Casto K, Kilduff LP, Cook CJ. Effects of oral contraceptive use on the salivary testosterone and cortisol responses to training sessions and competitions in elite women athletes. Physiol Behav. 2015;147:84-90. http://dx.doi.org/10.1016/j.physbeh.2015.04.017 [ Links ]
32.Powers SK, Howley ET. Hormonal responses to exercise. In: Exercise physiology: Theory and application to fitness and performance. 6th ed. New York: The McGraw-Hill Companies, Inc.; 2007. p. 73-105. [ Links ]
33.Broman-Fulks JJ, Berman ME, Rabian BA, Webster MJ. Effects of aerobic exercise on anxiety sensitivity. Behav Res Ther. 2004;42(2):125-136. https://doi.org/10.1016/s0005-7967(03)00103-7 [ Links ]
34.Guszkowska M, Sionek S. Changes in mood states and selected personality traits in women participating in a 12-week exercise program. Hum Mov. 2009;10(2):163-169. Available from: http://www.degruyter.com/view/j/humo.2009.10.issue-2/v10038-009-0014-2/v10038-009-0014-2.xml [ Links ]
35.McCraty R, Atkinson M, Tomasino D, Bradley RT. The coherent heart: Heart-brain interactions, psychophysiological coherence, and the emergence of system-wide order. Integr Rev. 2009;5(2):10-115. [ Links ]
 Correspondence:
Correspondence:
Adele Broodryk
della2001@gmail.com
Received: 03 Mar. 2019
Revised: 18 Aug. 2019
Accepted: 08 Sep. 2019
Published: 29 Jan. 2020
Editor: Pascal Bessong
Funding: National Research Foundation (South Africa), North-West University


{kind=link}