










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Science
versión On-line ISSN 1996-7489
versión impresa ISSN 0038-2353
S. Afr. j. sci. vol.115 no.9-10 Pretoria sep./oct. 2019
http://dx.doi.org/10.17159/sajs.2019/6452
COMMENTARY
Private sector contribution to SDG 3: Health and Well-being – a South African case study
Lorren K. HaywoodI; Caradee Y. WrightII, III
ISmart Places, Council for Scientific and Industrial Research, Pretoria, South Africa
IIDepartment of Geography, Geoinformatics and Meteorology, University of Pretoria, Pretoria, South Africa
IIIEnvironment and Health Research Unit, South African Medical Research Council, Pretoria, South Africa
Keywords: sustainable development, global health, public health, environmental health, business
Since the Sustainable Development Goals (SDGs) were globally adopted by world leaders in 20151, worldwide the private sector has openly embraced them and committed to address the SDG targets2-4. The United Nations Global Compact5 lists 10 principles that enable businesses to adopt socially responsible practices into their strategies. Similarly, the Global Reporting Initiative is an internationally recognised set of guidelines to enable businesses to report on how they address sustainability.6
While it is primarily governments' responsibility to provide the enabling environment for SDG implementation, they will not be achieved without private sector involvement.2 Businesses have a significant role to play as engines of economic growth, employment, finance, technology and innovation. They report their social contributions in annual sustainability and integrated reports. Because a healthy population contributes to a healthy workforce, it is in the interest of business to address human health.7-9
SDG 3 - Good Health and Well-being - seeks to ensure health and well-being at every life stage.10 This goal is broader than the Millennium Development Goals on child/maternal mortality and communicable diseases.11 SDG 3 includes 13 targets and 26 high-level indicators which address all major health priorities, including reproductive, maternal and child health; communicable, non-communicable and environmental diseases; universal health coverage; and access for all people to safe, effective, quality and affordable medicines and vaccines. Aspects of health are also captured in targets of several other SDGs.11 Interconnectedness of SDG 3 goals with other SDG goals highlights that population health is a major beneficiary of sustainable growth and central to the achievement of SDGs.12
Universal health coverage (SDG Target 3.8) is a unifying platform for making progress on SDG 313 and it emphasises the importance of universal access to health-care services. The private sector has provided financial mechanisms and has also provided expertise in enlarging human capacity and conducting research for health care.14 The contribution that the private sector can make to achieving SDG 3 is being recognised7,14 and should be reported by businesses. Through their corporate social investment (CSI) programmes, business can leverage capabilities that contribute to universal health coverage28, including innovative data collection technologies, enhanced disease surveillance, improved supply chain management practices for storage and delivery of essential health supplies.
SDGs provide an opportunity for businesses to support public health through their value chains, communication activities, occupational health and safety practices, and employee benefits. By ensuring that employees have safe working conditions and access to health services, businesses build better relationships with their employees. The purpose of the current study was to understand the extent to which South African businesses explicitly report contributions to SDG global health objectives. This analysis is important because the country faces significant public health issues that cannot be overcome without private sector contribution.
South Africa and its public health related challenges
South Africa faces a quadruple burden of disease15 and the mortality rate attributed to cardiovascular disease, cancer, diabetes and/or chronic respiratory disease is ranked third worst in sub-Saharan Africa. Mean probability of dying from one or more of these four diseases in 2015 in South Africa (ages 30-70 years) was 26% compared with 21% for all of sub-Saharan Africa.16 There is concern about the increase in the prevalence of non-communicable diseases.17 The Global Burden of Disease 2015 SDG Collaborators created an overall health-related SDG index for which South Africa was ranked 134 (out of 188).18
Business case for social involvement in public health
Today, it is not enough for a business to only make a profit for shareholders; their licence to operate must include a contribution to social capital.19 The unprecedented pace of global change presents businesses with new risks, such as effects on ecosystems and population health, and affects their modi operandi. These interconnected relations are pressuring the private sector to appreciate that it is not isolated from the communities and the physical environment in which it operates.5,20
A business contributes to community health by ensuring that it safeguards the environment that ensures commercial viability.20 Moreover, public-private partnerships for public health can, for example, increase access to pharmaceuticals in developing countries as new technologies come to market.21 Increase in diseases poses one of the greatest threats to the global economy.22,23 Recent outbreaks such as Ebola demonstrated extraordinary health, economic and security risks associated with infectious disease epidemics.24 Ebola alone affected 28 639 people and caused 11 316 deaths, leading to USD2.2 billion in lost GDP combined in Guinea, Liberia and Sierra Leone.24 Such outbreaks threaten not only macroeconomic stability but also food security, human capital development and private sector growth.8 Investing in global health security and emergency preparedness is a priority in an increasingly globalised world.7,8 Such investment is critical to health equity, as vulnerable, marginalised people are primary victims. Improving health contributes to economic development and stability.25 The private sector has resources and expertise to contribute to strengthening health security by protecting their employees and communities in which they operate.25
Gathering the evidence
Businesses were drawn from those listed on the Johannesburg Stock Exchange (JSE). The top 100 (out of ~400 listed) were extracted from the JSE website (www.jse.co.za), and of these, 88 were included in the study that was based upon available annual reports over three consecutive financial years (2016-2018). The list of 88 businesses and their JSE-defined sector type (https://www.sharenet.co.za) was exported into Microsoft Excel (Microsoft Office 265 ProPlus) for analysis. In 2019, two researchers searched the Internet for top 100 businesses' annual integrated and/or sustainability reports for 2016, 2017 and 2018. Once these reports were located, they were downloaded and analysed to identify: (1) mentions of SDGs; (2) specific mentions of SDG 3; and, if SDG 3 was mentioned (3) whether it was being applied to communities and society beyond their workforce/immediate customers.
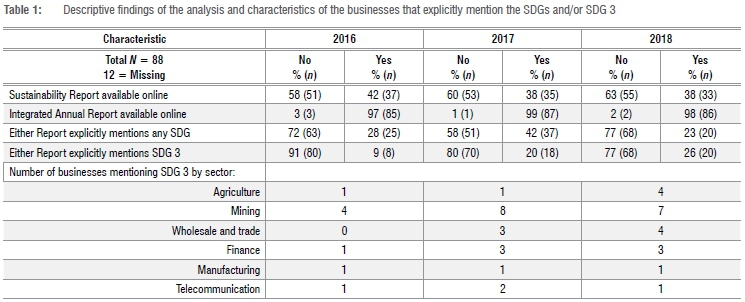
In 2016, 25 businesses specifically mentioned SDGs in either report (Table 1), while only eight reports specifically mentioned SDG 3. The number that reported SDGs and SDG 3 explicitly in 2017 more than doubled (to 18) from that in 2016 and increased again in 2018 (to 20). Businesses stated their contribution to SDG 3 through their health and safety strategies and plans or through CSI initiatives. Where companies discussed their contributions to SDGs and/or SDG 3, this input was mainly through sustainability reports (not a mandatory report as is the case for integrated reports).
Discussion
Even though it is still 'early days' in terms of SDG implementation, we expected more companies to have explicitly linked their contributions to SDG targets and SDG 3 given the UNDC guidance. More of them itemised their SDG contribution in 2017 and 2018 than in 2016 and we expect that this trend will continue.
Of the 88 companies investigated, it was those from the mining sector that currently have the greatest number highlighting their contributions to SDG 3. Companies in the mining sector have to comply with health and safety regulations as a requirement of the Mine Health and Safety Act (Act No. 29 of 1996). Mining health risks include cardiovascular and respiratory diseases, substance abuse and domestic violence. Health and safety programmes are initiated not only for employees but also as a CSI to invest in community health programmes. As health hazards relevant to mining are discussed in SDG 3 Targets 3.3, 3.4 and 3.5, mining companies can align their programmes and reporting. One mining company quantified its data to demonstrate contribution to HIV/Aids and non-communicable disease targets. In this sustainability report, the company detailed relevant SDG 3 targets and also provided dedicated commitment and activities to each target. Another stated exactly how the company contributed to SDG 3 by referring to a memorandum of understanding with the Provincial Department of Health to provide primary health-care services to the communities surrounding their operations.
A beverage business provided insight into its 'healthier world programme' in which it invests in programmes to shift social behaviour around alcohol abuse (SDG 3 Target 3.5). Another company in the same sector noted that although it produced alcoholic drinks, it also had embarked on programmes to educate pregnant women on the impact of alcohol on their unborn children (SDG 3 Target 3.2). There were also programmes to reduce road deaths and injuries from drinking and driving (SDG 3 Target 3.6). But surprisingly, none of the JSE health-related businesses, for example hospital management, long-term care, pharmaceuticals and biotechnology, mentioned SDG 3, despite their potentially critical role.26
Generally, businesses that mentioned SDG 3 did so in relation to either their CSI among their own employees, their customers or, more rarely, society by making employee health care available. There were programmes that extended beyond the commercial responsibilities that aimed to improve livelihoods or their employees' families to access health care. For example, a mining business offered free testing for HIV/Aids, counselling and treatment to their employees as well as education awareness programmes among nearby communities. There is a need for businesses to be made aware of the SDGs through the Global Reporting Initiative to encourage them to align their CSI activities to specific SDGs. This would not only benefit the company but would help government track progress towards meeting SDG targets.
Notwithstanding the potential benefit that the business sector can contribute to the achievement of SDG 3, it must be noted that there have been challenging situations and tensions between some CSI programmes and public health.27 Some CSI activities conducted by the tobacco and alcohol industries were beset with conflicts of interest and systematic biases. Careful evaluation and monitoring, and even possible policy and regulation by independent bodies, may be required to ensure sound, ethical public health and health promotion initiatives by businesses.27
In our review of the reports that mentioned being involved in activities relevant to SDG 3, we also considered missed opportunities. We believe there is potential for private health-care providers to work more closely with public providers to expand the reach of health-care services and to close gaps in quality care. Some companies could upgrade hospital and clinic infrastructure and even prioritise access to new services and products via CSI. There were also opportunities where private resources and expertise might be extended to state institutions by introducing innovation or training for health-care workers. And large international businesses could use their transborder reach to tackle global health challenges on the scale required to achieve SDG targets.
Conclusions
Many of South Africa's top JSE-listed companies do not publicly report on their contribution to the SDGs. This is not to say they do not contribute to SDGs or SDG-related public health targets but they are failing to align their activities and/or to report on them in the public domain. Given that the SDGs are guiding principles for humanity's future, it is important that businesses not only report on their activities but also make greater contributions towards achieving the SDGs by working in partnership with government and other organisations.
Acknowledgements
C.Y.W. receives research funding support from the South African Medical Research Council and the National Research Foundation (South Africa). L.K.H. receives research funding from a parliamentary grant.
References
1.United Nations. Transforming our world: The 2030 agenda for sustainable development. In: World public sector report 2015: Responsive and accountable governance. New York: United Nations; 2015. p. 73-87. https://doi.org/10.18356/e5a72957-en [ Links ]
2.Global Reporting Initiative/United Nations Global Compact/World Business Council for Sustainable Development SDG Compass. The guide for business action on the SDGs [document on the Internet]. c2015 [cited 2017 Aug 21]. Available from: http://sdgcompass.org/wpcontent/uploads/2016/05/019104_SDG_Compass_Guide_2015_v29.pdf [ Links ]
3.Pricewaterhouse Coopers. Navigating the SDGs: A business guide to engaging with the global goals [document on the Internet]. c2016 [cited 2017 Aug 23]. Available from: https://www.pwc.com/gx/en/sustainability/ [ Links ]
4.Business and Sustainable Development Commission. Better business, better world [document on the Internet] c2017 [cited 2017 Aug 17]. Available from: http://report.businesscommission.org/uploads/BetterBiz-BetterWorld_170215_012417.pdf (last accessed17 August 2017) [ Links ]
5.United Nations Global Compact. United Nations Global Compact progress report: Business solutions to sustainable development [document on the Internet] c2017 [cited 2018 Feb 12]. Available from: https://doi.org/10.18356/bb7953d3-en [ Links ]
6.Maubane P, Prinsloo A, Van Rooyen N. Sustainability reporting patterns of companies listed on the Johannesburg Securities Exchange. Public Relat Rev. 2014;40:153-160. https://doi.org/10.1016/j.pubrev.2014.02.014 [ Links ]
7.World Economic Forum. How can business improve global health? [webpage on the Internet]. c2015 [cited 2018 Jan 26]. Available from: https://www.weforum.org/agenda/2015/09/how-can-business-improve-global-health/ [ Links ]
8.World Economic Forum. The global risks report 2016 [document on the Internet]. c2016 [cited 2018 Jan 26]. Available from: http://www3.weforum.org/docs/GRR/WEF_GRR16.pdf [ Links ]
9.World Economic Forum. Global healthcare: The $300 billion question [webpage on the Internet]. c2017 [cited 2018 Feb 27]. Available from: https://www.weforum.org/agenda/2017/11/the-300-billion-global-health-question [ Links ]
10.United Nations. The Sustainable Development Goals report. New York: United Nations; 2017. [ Links ]
11.Kumar S, Kumar N, Vivekadhish S. Millennium Development Goals (MDGS) to Sustainable Development Goals (SDGS): Addressing unfinished agenda and strengthening sustainable development and partnership. Indian J Community Med. 2016;41:1. https://doi.org/10.4103/0970-0218.170955 [ Links ]
12.World Health Organization (WHO). Health in 2015: From MDGs, Millennium Development Goals to SDGs, Sustainable Development Goals. Geneva: WHO; 2015. https://doi.org/10.4324/9781315228068-4 [ Links ]
13.Chapman AR. Assessing the universal health coverage target in the Sustainable Development Goals from a human rights perspective. BMC Int Health Hum Rights. 2016;16, Art.#33, 9 pages. https://doi.org/10.1186/s12914-016-0106-y [ Links ]
14.De Wolf AH, Toebes B. Assessing private sector involvement in health care and universal health coverage in light of the right to health. Health Human Rights. 2016;18:79. [ Links ]
15.Pillay-van Wyk V, Msemburi W, Laubscher R, Dorrington RE, Groenewald P, Glass T, et al. Mortality trends and differentials in South Africa from 1997 to 2012: Second National Burden of Disease Study. Lancet Glob Health. 2016;4(9):642-653. https://doi.org/10.1016/s2214-109x(16)30113-9 [ Links ]
16.World Health Organization. World health statistics 2017 [webpage on the Internet]. c2017 [cited 2017 Dec 14]. Available from: http://www.who.int/gho/publications/world_health_statistics/2017/en/ [ Links ]
17.Day C, Gray A. Health and related indicators. In: Padarath A, Barron P, editors. South African health review 2017. Durban: Health Systems Trust; 2017. [ Links ]
18.Lim SS, Allen K, Bhutta ZA, Dandona L, Forouzanfar MH, Fullman N, et al. Measuring the health-related Sustainable Development Goals in 188 countries: A baseline analysis from the Global Burden of Disease Study 2015. Lancet. 2016;388:1813-1850. https://doi.org/10.1016/S0140-6736(16)31467-2 [ Links ]
19.Buhmann K. Public regulators and CSR: The 'social licence to operate' in recent United Nations instruments on business and human rights and the juridification of CSR. J Bus Ethics. 2016;136(4):699-714. https://doi.org/10.1007/s10551-015-2869-9 [ Links ]
20.World Economic Forum. Managing the risk and impact of future epidemics: Options for public-private co-operation [document on the Internet]. c2015 [cited 2018 Jan 16]. Available from: http://www3.weforum.org/docs/WEF_Managing_Risk_Epidemics_report_2015.pdf [ Links ]
21.Reich MR. Public-private partnerships for public health. Nat Med. 2002;6:617-620. [ Links ]
22.Reubi D, Herrick C, Brown T. The politics of non-communicable diseases in the Global South. Health Place. 2016;39:179-187. https://doi.org/10.1016/j.healthplace.2015.09.001 [ Links ]
23.Islam SMS, Purnat TD, Phuong NTA, Mwingira U, Schacht K, Fröschl G. Non‐communicable diseases (NCDs) in developing countries: A symposium report. Global Health. 2014;10:81. https://doi.org/10.1186/s12992-014-0081-9 [ Links ]
24.World Bank. Update on the economic impact of the 2014-2015 Ebola epidemic on Liberia, Sierra Leone and Guinea [document on the Internet]. c2015 [cited 2017 Dec 12]. Available from: https://openknowledge.worldbank.org/bitstream/handle/10986/21965/95804.pdf [ Links ]
25.Sturchio JL, Goel A. The private-sector role in public health: Reflections on the new global architecture in health [webpage on the Internet]. c2012 [cited 2018 Nov 20]. Available from: https://csis-prod.s3.amazonaws.com/s3fs-public/legacy_files/files/publication/120131_Sturchio_PrivateSectorRole_Web.pdf [ Links ]
26.Thorsteinsdóttir H, Ovtcharenko N, Kohler JC. Corporate social responsibility to improve access to medicines: The case of Brazil. Global Health. 2017;13:10. https://doi.org/10.1186/s12992-017-0235-7 [ Links ]
27.De Vries H. Invited Commentary: Corporate social responsibility and public health: An unwanted marriage. Prev Med. 2016;89:345. https://doi.org/10.1016/j.ypmed.2016.07.003 [ Links ]
 Correspondence:
Correspondence:
Caradee Wright
cwright@mrc.ac.za
Published: 26 September 2019


{kind=link}