










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Science
On-line version ISSN 1996-7489
Print version ISSN 0038-2353
S. Afr. j. sci. vol.115 n.3-4 Pretoria Mar./Apr. 2019
http://dx.doi.org/10.17159/sajs.2019/5290
RESEARCH ARTICLES
Leveraging media informatics for the surveillance and understanding of disease outbreaks
Bankole Falade
South African Research Chair in Science Communication, Centre for Research on Evaluation, Science and Technology (CREST), Stellenbosch University, Stellenbosch, South Africa
ABSTRACT
Syndromic disease surveillance mechanisms can be enhanced by incorporating mass media informatics for disease discourse and aberration detection and social psychology for understanding risk perceptions and the drivers of uptake and resistance. Using computerised text analysis, the coverage of the outbreak of Zika virus in Brazil in 2017/2018 in four newspapers - O Estado, O Globo, the Times of London and the New York Times - was examined and patterns were compared with Google Trends. Quantitative indicators showed waves of attention to Zika peaked in the same period but local newspapers, O Estado and O Globo, indicated lower levels of anxiety in the run up to the Olympics when compared with foreign media. The unusual surge in attention to dengue in early 2015 was an early indication to sound the alarm for extensive clinical investigations. This, together with the flagging of Zika by O Globo almost a year before the global alarm, indicates the suitability of this method for surveillance and detection of aberrations. Media attention waves are also significantly associated with Google Trends, indicating empirical equivalence. Qualitative indicators show the extra motivation over Google, World Wide Web or Twitter searches by highlighting public perceptions. Findings show the absence of a stable body of scientific knowledge at the outbreak and an ensuing crisis of understanding. Local concerns were about the economic crisis, religious beliefs, poverty and crime - all inhibitors to containment - while the global alarm was amplified by risk to tourists and athletes, and political disputes mixed with religious beliefs.
Significance:
•This study contributes to research on the use of longitudinal media data as surrogate sources for syndromic disease surveillance.
•Mass media informatics provide empirical equivalence to Google Trends. •Clinical and non-clinical factors contributed to public anxiety over disease epidemics.
•Lack of clinical knowledge at the onset of the crisis contributed to anxiety among scientists and the public
Keywords: Zika; syndromic surveillance; knowledge crisis; risk perception; public understanding of science
Mass media and public health informatics
The news is a form of knowledge1 and a feature article answers to the '5W's and H' principle of journalism: who, what, when, where, why and how. This principle is also true of social psychological approaches to knowledge2 as the 'who', 'how', 'why', 'what' and 'what for' constitute the contexts of knowing and are central to communication, attribution, etc. The diagnosis of epidemiological3 events also follows the same 5W's: what (diagnosis or health event), who (person), where (place), when (time) and why/how (causes, risk factors and modes of transmission). Thus, the conceptual approaches to mediated knowledge transfer by the media, the social psychological studies of knowledge in context and epidemiological studies of the distribution and determinants of health-related states or events are similar, in that they all address the '5W's and H'.
The threat of global pandemics posed by outbreaks of influenza H5N1, H1N1 and Severe Acute Respiratory Syndrome provoked interest in improving early warning systems and reinforced the need for combining data from different sources and experimentation with new types of media.4,5 Rapid outbreak detection and the examination of a wide range of methods have also shown that no single detection approach is likely to be optimal.6 Electronic information sources are proving to be valuable inputs and the Global Public Health Intelligence Network has shown that extensive monitoring and analysis of news media around the world can aid in early detection of disease threats.7
The news media tell the public what to think about by directing attention to problems and solutions and prioritising issues of importance.8-10 Thus, they have become tools for understanding health problems in different contexts11,12 and for understanding the psychosocial factors that propel epidemics13. Newspapers flagged opposition by religious authorities to vaccination in Nigeria in 2001, well ahead of the vaccine revolt of 2003-2004.14
Health informatics remains central to modern epidemiological practice and its advanced surveillance systems facilitate access to new data streams and the automation of processes for case and aberration detection.6,7 Syndromic surveillance focuses on the early signals and an optimal system might be one that integrates data from multiple sources, clinical or surrogate, thereby potentially increasing investigators' confidence in the relevance of an alert from any single data source.15
News media informatics and the knowledge-in-context approach can form part of a complex of syndromic surveillance mechanisms for the early detection of related non-clinical discourses about health. Data mining of both current and archival media data can detect deviations from recognised patterns that may signal amplification of concern or the emergence of certain keywords that signify new entrants. It has been shown that changes in public anxiety about the HIN1 virus were detectable in people's online searches through analysing trends.16
The challenges of a novel and complementary data source and data analysis methodology notwithstanding17, the method is being increasingly employed for passive monitoring. Twitter has been used to track levels of disease activity and public concern and to improve surveillance18,19. Google has been used to monitor Ebola-related web search behaviour and dengue outbreaks.20-22 Some authors have used a travel health website23 to monitor anxiety over the Zika virus, others have examined the framing of the Zika crisis24 in two Brazilian newspapers (O Globo and Folha de Sao Paulo) and the coverage of mosquito-borne diseases in Italian newspapers25 and compared Zika with other diseases.
Newspaper coverage and Google Trends for the Zika virus in Brazilian, UK and US media were examined with the aim of contributing to a growing body of knowledge on the use of non-clinical sources for passive monitoring. Computer-assisted keyword analysis was used for disease discourse and aberration detection and to analyse trends indicative of waves of public concern. Knowledge crisis among scientists, perception crisis in the public and the psychosocial and economic inhibitors to containment were also examined.
Case study: The Zika virus disease
Alarm over the effect of the Zika virus on pregnancy in several parts of the Americas became a global phenomenon in the latter months of 2015 and early days of 2016. The virus had, however, been of concern in the Americas since 2014.26,27 The first report of autochthonous transmission of Zika virus was reported in Chile in March 2014. In March 2015, the authorities in Brazil notified the World Health Organization (WHO) of an illness characterised by skin rash, but Zika was not suspected at that stage. In the same month, the Brazilian newspaper O Globo alerted to the circulation of Zika in some states and, in May, the Pan American Health Organisation (PAHO) issued an epidemiological alert on the circulation of Zika virus.26,27
In July 2015, Brazil reported neurological disorders associated with a history of infection including 49 confirmed cases of Guillain-Barré syndrome.26 In October that year, the country again alerted WHO to an unusual increase in the number of children born with microcephaly - a neurological disease which manifests as unusually small heads in newborns. The following month, Brazil declared a national public health emergency over microcephaly and, shortly after, authorities in neighbouring countries including El Salvador, Guatemala and Mexico also reported the circulation of Zika virus. A continental transmission had begun with a corresponding global alarm. At this time, however, there was no confirmation of any link between Zika and microcephaly.26
The first report in the Western (UK and US) media sample for this study was in the London Daily Telegraph of 19 November 2015 titled 'The Zika virus: Answers about a growing menace'. The report said Brazil had declared a public health emergency on the confirmation of about 400 cases of newborns with small heads and the detection of the Zika virus in the amniotic fluid of two pregnant women whose foetuses were diagnosed with microcephaly. In January 2016, the US Centers for Disease Control (CDC) issued an alert for pregnant American women to avoid travel to the Americas, and on 1 February 2016, the WHO declared the disease a 'global health emergency'26.
A mild virus of African origin turns invasive
Zika was discovered in monkeys in Uganda in 1947 and was later isolated in the Aedes africanus mosquito. The virus had no known severe effects in Africa and it is thought that the population has pre-existing immunity.28 The disease moved from Africa to Asia and the first large outbreak in humans was in 2007 in the Pacific Island of Yap. Another outbreak followed in 2013 in French Polynesia, and, by 2015, Zika virus was spreading in Brazil. The Aedes species transmitting Zika in the Americas are the Aedes aegypti and Aedes albopictus, which also transmit yellow fever, dengue fever and chikungunya.28-30
Knowledge production by scientists about emerging and highly infectious diseases is often problematic at the onset of major outbreaks. This was the case with the Severe Acute Respiratory Syndrome31, swine-origin Influenza A (H1N1) virus in humans32 and other viral epidemics. In such situations of a crisis of knowledge, 'what' types of perceptions are expressed by the public, 'what' are the non-clinical discourses that may contribute to these public perceptions and 'why' and 'how' may these inhibit containment?
Researchers have examined science and society issues from two perspectives: the public understanding of science and risk perception33; however, both are functionally equivalent. The risk perception research, or the engineering approach, focuses on how scientists and the public perceive risk. While scientists focus on risk assessment using algorithms and normative rules, the public rely on intuitive risk judgements which are informed by images and associations, linked by experience to emotion and affect - thus when a decision is complex, they rely on readily available affective impressions.34,35
The public understanding of science perspective was initially focused on scientific literacy. This was criticised as a 'deficit model' which contrasts knowledgeable scientists against an ignorant public, but the field has transformed over the decades into a science and society paradigm which examines trust and expert deficit, the notion of 'public' and crisis of confidence. The new paradigm also acknowledges that the public can at times be inattentive, unmotivated and ignorant and public education becomes a priority.36-39
The Zika virus disease in Brazil was approached from the science and society38 perspective of knowledge encounters and public sphere40,41 and how the public perceive risk35 from a virus described as the 'doença misteriosa' or mystery disease. Scientific knowledge was problematic at the onset of the crisis, sometimes symptoms were confused with known diseases plausibly leading to a misdiagnosis or delayed diagnosis, and the public had to internalise the disease and its implications for health in a society with strong religious ties and ongoing political and economic crises.
Research objectives
The objective was to examine how disease surveillance and monitoring operations can leverage media reports and contribute to the growing body of evidence on the use of syndromic surveillance mechanisms.18-22 The specific research questions were:
1.What are the quantitative indicators of public anxiety over the Zika virus? The focus here was on computerised text analysis for disease discourse and aberration detection, longitudinal media studies for public attention and patterns of public concern over time. Specifically:
1.1 How early did the Zika virus discourse appear in the Brazilian media? How does the trend compare with those for similar diseases such as dengue and chikungunya? What are the levels of attention that indicate rise in public anxiety and an alarm for further clinical analysis? How do these indicators compare with Google Trends Brazil?
1.2 What are the levels of attention in the media in the United Kingdom and USA? How do these indicators compare with Google Trends worldwide, and in the UK and USA?
2.What are the qualitative indicators42 of the discourse about the Zika virus disease in the British and US press? The focus here being on psychosocial and economic drivers of perception, uptake or resistance.
Data and research methods
The analysis of public health surveillance data is typically performed to detect the presence of unusual patterns in comparison with historical data.6 Mass media archives are also responsive to pattern recognition. Media is the common place through which communities cultivate shared and public notions about facts, values and the contingencies of human existence42 over time, and thus there is stability in what is discussed and what is not. Unusual patterns and discourses then signal the appearance of a new phenomenon or the amplification of concerns over existing ones. However, being shared and collective does not denote consensus, rather it recognises the subcultural, class, generational, ideological, and even conflicts, among groups. Thus, studies of different newspapers within a country will reveal overarching community anxieties while also retaining subcultural differences. However, local interests often cross national boundaries, and the focus of this study is on a disease epidemic ravaging a country but with the potential to globalise in our increasingly interconnected world.
Data for this study were obtained from O Estado de São Paulo (O Estado) and O Globo, two leading Brazilian newspapers; The Times of London and The Telegraph published in the UK and the US-based USA Today and New York Times. Coverage data were downloaded from the NEXIS database at various times between March 2017 and February 2018. Google Trends was used for online searches in Brazil, UK, USA and worldwide to compare with newspaper trends.
The US newspaper was chosen because of the presence of the mosquito carrier in some parts of the USA and the high risk of spread compared with the UK where the carriers are absent. The UK and US newspapers also provide indicators of when the media detected the events to report and the attention on two important events in Brazil (the Rio Carnival and the Olympics) that may have affected foreign visitors from these countries. The Brazilian newspapers were chosen to identify trends and aberrations to media attention in the local press within the review period.
For O Globo and O Estado, the NEXIS search was conducted using the keywords dengue or Zika or chikungunya between 1 January 2015 and 31 December 2016. Using these keywords, 503 articles for O Globo and 813 for O Estado were downloaded. For the UK and US newspapers, the keyword used was 'Zika'. There were no search results returned for 'Zika' between 1 January 2015 and 31 October 2015. Blogs, duplicates and articles with high levels of similarity were discarded. In total, 246 articles from The Times of London and 414 from the New York Times were used for the trend analysis. Google Trends21 was used for online searches. For Google Brazil, the keywords used for the search were 'Zika', 'Dengue' and 'Chikungunya' to map the co-occurrence of searches about the three diseases from 1 January 2015 to 31 December 2016. The same dates were used for 'Zika' on Google worldwide, Google UK and Google USA. The NEXIS output is in the daily format of newspapers and downloads both headlines and text. The daily format was re-coded to weekly to match Google weekly outputs.
The QDA/Miner WordStat program, which runs in both English and Portuguese, was used to analyse the data.
Limitations of research
Secondary data were used and are limited in time to 2 years and to selected newspapers in Brazil, UK and USA. The study of the Brazilian media was limited to detecting aberrations and trends and comparing with Google searches. Other authors24 have examined the framing of the debate in the Brazilian media. It would be interesting to see how a wider longitudinal study of newspapers worldwide could be used to trace the movement of the disease in the Americas and when the debates about its presence emerged in other Latin American newspapers. This would provide more data to support growing research on mass media as surrogate data for epidemiological studies.
Findings
Research question 1.1
This question addressed how early the Zika virus discourse appeared in the Brazilian media. How did the trend compare with similar diseases such as dengue and chikungunya? What were the levels of attention that indicate a rise in public anxiety and an alarm for further clinical analysis? How did these indicators compare with Google Trends Brazil?
Figure 1 shows the co-occurrence of Zika and dengue, both with similar symptoms, in May 2015 in O Globo. May 2015 is the earliest appearance of the word Zika in the two Brazilian newspapers; the articles indicate the level of unfamiliarity with the disease at that time. The first report, on 14 May 2015, titled 'O novo vírus do 'aedes' ('The new 'aedes' virus') said (translated) 'It [Zika] seems less serious, but it is possible to acquire the three viruses at the same time, and we do not know the clinical course of this co-infection with the Zika virus, for which we do not have immunity'. A 3 June 2015 follow-up article titled 'Rio tem o primeiro caso confirmado de Zika' ('Rio has the first confirmed case of Zika') shows health officials still regarded Zika as benign and advised clinicians to treat as dengue when in doubt. Reference to both diseases did not occur again until November 2015 with Zika later reaching its peak in the second week of February 2016 when WHO declared a global emergency. The Kendall's tau_b correlation coefficient from 13 December 2015 to 31 December 2016 shows a significant association between Zika and dengue (r=0.70; p<0.001) but not between Zika and chikungunya (r=0.54; p<0.08).
Figure 1b shows that dengue and chikungunya had been in the media discourse in Brazil, in O Estado, from 1 January 2015 when the sampling commenced, with coverage of dengue rising rapidly thereafter with a major peak in the first week of May 2015. This peak shows an unusual pattern - an indication of rising public anxiety - which should raise an alarm for further clinical investigation. May 2015 was also the month Zika appeared in O Globo (Figure 1a), indicating it was flagged by one local newspaper and not the other, also showing the need for multiple media sources. The experience of doctors was with dengue and Zika was thought, at this time, to be benign. This may explain the comment by a Brazilian official reported in the New York Times of 31 December 2015 that 'Zika virus doesn't worry us' because it is a 'benign disease'. The appearance of Zika peaked at about the same time in the second week of February 2016 in both Brazilian newspapers. There is a significant association between Zika and dengue (r=0.69; p<0.001) and between Zika and chikungunya (r=0.68; p<0.001) between 13 December 2015 and 31 December 2016.
Figure 1c compares Google searches for dengue, Zika and chikungunya. The Google search number represents an index of popularity. It is used here as a variable indicating an index of appearances. The graph shows that those seeking online information had a much higher and sustained interest in dengue in the review period, except in early December 2015 when it was surpassed by Zika. The December surge coincides with similar surges in O Estado and O Globo. Searches for Zika were noticeable from the beginning of the review period in very low numbers, mostly one, with the highest peak recorded in the second week of February 2016, as with the newspapers. For Google and newspaper searches between 13 December 2015 and 31 December 2016, the correlation was significant for Zika in Google Brazil and O Estado (r=0.65; p<0.001) and O Globo (r=0.59; p<0.001). The correlation was also significant for dengue in Google Brazil and O Estado (r=0.69; p<0.001) and O Globo (r=0.53; p=0.001).
Coverage by both newspapers was compared over the period. The correlation for Zika in O Globo and O Estado was significant (r=0.54; p<0.001) as was the correlation for dengue (r=0.61; p<0.001).
Research question 1.2
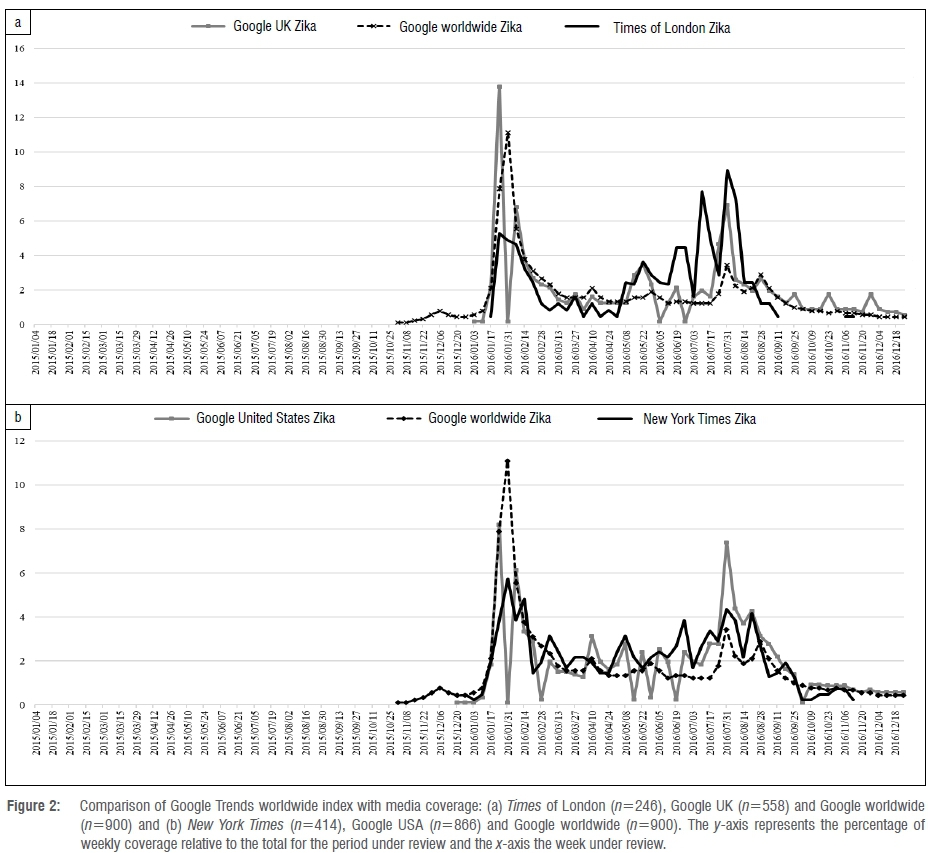
This question addressed the levels of attention in the UK and US media. How did attention levels compare with Google Trends UK, USA and worldwide? For the UK, a comparison was made between Google UK, Google worldwide and The Times of London. Figure 2a shows that coverage in Google UK and The Times of London peaked at the same time, the third week of January 2016, a week before Google worldwide, and remained high until March 2016. The Rio Carnival was held in February 2016 and there is a noticeable peak in coverage in Google UK at this time. Coverage in the Times of London peaked again in the last week of July, just before the commencement of the Rio Olympics held from 5 August to 21 August 2016. The July to August surge in coverage in The Times of London, higher than the February peak, was not replicated in Brazilian newspapers42, indicating differences in the perception of risk and anxiety. There was a significant association for the keyword Zika between The Times of London and Google UK (r=0.37; p<0.001) and between The Times of London and Google worldwide (r=0.30; p<0.008).
The New York Times data show a similar trend with those of The Times of London. The first peak in coverage in the New York Times was in late January 2016, coinciding with that in Google worldwide but a week after coverage in Google USA peaked. Coverage in the New York Times reached another height 2 weeks later, followed by several highs and lows mimicking the UK data in the run up to the Olympics with a noticeable July to August surge. There was a significant association in coverage of Zika between the New York Times and Google USA (r=0.44; p<0.001) and between the New York Times and Google worldwide (r=0.52; p<0.001). The Kendall's tau_b correlation coefficient also shows significant correlations for the weekly appearance of Zika in The Times and the New York Times (r=0.55; p<0.001).
Debates about the Zika virus began in the foreign media - in the Daily Telegraph of 19 November 2015 - about 8 weeks before the first travel alert by the CDC on 15 January 2016. Reports later appeared in the Sunday Times of 13 December 2015, USA Today of 18 December 2015 and the New York Times of 29 December 2015. This is an indication of global anxiety ahead of the confirmation of a major outbreak. The disease had, however, been flagged in Brazil much earlier - in the second week of May 2015 - and public anxiety had risen much earlier, from February through April, over dengue, which presents similar symptoms to those of Zika.
Altogether, a collection of world newspapers on an ongoing basis produces a very similar trend chart to that for Google online searches and can thus form part of a routine surveillance system of non-clinical data. The process can also be automated for case and aberration detection3,6,7 mapping the movement of invasive foreign species across continents. In addition to similarities with Google searches, the February peak is similar to Twitter data43 in the same period. The February and August peaks are also similar, coinciding with visits to a UK travel health website.23
In addition, as will be shown in the next section, newspapers provide information on the scientific and non-scientific discourses about disease, public perceptions and how these may have influenced the uptake of containment information.
Research question 2
What are the qualitative indicators42 of the discourse about the Zika virus disease in the UK and US press?
Crisis of knowledge, the known and unknowns
The first part of this section examines a crisis of knowledge among scientists during the early days of the outbreak while the second part reviews public perceptions of risk from the virus and psychosocial and economic inhibitors to containment - representations34,35,40,41 and the crisis of mind. This section is limited to the US and UK media - from 'the outside looking in' (see Ribeiro et al.24 for the framing of the debate in the Brazilian media).
Diagnosis
The inexperience with Zika disease meant existing facilities were inadequate, leading to several false positives and fears Zika may have been misclassified. Scientists were also not certain at the early stages of the outbreak about the causative agent. One doctor said44:
We don't know if it's only Zika or if it's a combination of Zika, dengue and chikungunya…Maybe a woman was infected by dengue a year before, and now is pregnant and gets Zika.
How the virus crosses the placenta to the foetal brain to cause damage - a condition referred to as microcephaly - was also unknown.45 The extent of the dengue problem was captured by a news report which stated that Brazil registered more than 1.6 million cases of dengue, with 863 people dying of the disease the previous year.46 There were also fears expressed in the media that the infection could lead to other serious diseases such as Guillain-Barré syndrome, which attacks the nervous system and can lead to fatal paralysis.
The government was also unsure about what instructions to issue for diagnosis. Health professionals were originally told to report suspected microcephaly cases when a baby's head at birth was 330 mm, or 13 inches, or less. The government then changed the threshold to 320 mm after concluding that there were many babies with small heads but without problems. Later, discussions began on lowering the circumference to 319 mm for boys and 315 mm for girls.47
Transmission
There were a lot of unknowns about the mode of transmission of the virus, whether it was a single route through mosquito bites, or whether there were multiple routes of transmission. Reports later emerged that the disease could be transmitted through sexual intercourse, blood and other body fluids such as saliva and could remain in semen for more than 2 months after infection. The uncertainty led to some taking extreme precautions:
We've also made the decision to have Greg's sperm frozen. We'd love to have more children and with research in its infancy, I wouldn't want to put myself in a situation which could have been prevented…48
Causative consensus
In April 2016, more than a year after the disease epidemic became a public concern in the Americas and over 4 months after the crisis became a global concern, the WHO agreed that there was a strong link between Zika and microcephaly in newborns. The announcement was not without debate though, as the CDC researchers, who also confirmed the link, sidestepped the more stringent Koch's Postulates, which require that scientists must re-isolate the suspected pathogen after infecting healthy people or animals with the suspected pathogen, and the Bradford Hill Criteria, a model for studying infectious diseases. Instead, a framework called Shepard's Criteria for Teratogenecity, which has a lower threshold, was adopted.49
Despite agreement on the cause, much remained unknown about the effects of Zika, including effects on other organs, the risk for pregnant women of having brain-damaged babies, and to what extent the risk varies according to when in pregnancy the infection occurs and other types of brain defects possible.
Risk perception, psychosocial and economic inhibitors
We perceive new issues and objects through our existing images of the world. Thus, how we initially react to a new phenomenon is determined largely by our shared experiences of similar objects, our culture and aspirations.50 Invasive microbes have been in the news worldwide with their devastating consequences resulting in global panic. Previously unknown Severe Acute Respiratory Syndrome (SARS) spread from Guangdong Province in China to 37 countries including Canada, Singapore and Taiwan, with 774 reported deaths.51 The Ebola virus13 caused global panic when it resulted in the death of thousands in West Africa, where it was previously unknown. It is these shared images of fatalities with which the public perceive new viruses with the potential to globalise in new areas.
The arrival of Zika in a previously uninfected Latin America, its capacity to spread and the debilitating effect on the foetus caused a global panic. Brazil, a major tourist destination, was to host the annual Rio carnival and the 2016 summer Olympics, both of which would attract thousands of foreign visitors, which served to amplify anxiety over capacity of the disease to spread to new countries.
Local and international perceptions of risk
On the international scene, there was a high level of anxiety over the possible exposure to Zika of athletes and their family members during the Olympic Games. Some athletes withdrew from the Olympic Games, others followed safety measures. Over 100 leading scientists called for the Games to be postponed:
An unnecessary risk is posed when 500,000 foreign tourists from all countries attend the Games, potentially acquire that strain, and return home to places where it can become endemic…The Games should be moved or postponed.52
Despite one expert warning that the Olympics could become the 'the Olympics of brain damage', the International Olympic Committee rejected calls for its postponement. The Committee's response followed a statement from the WHO that there was 'no public health justification for postponing or cancelling the Games'53.
Some athletes were not worried. One told a newspaper that the Games were more important than 'the bugs': 'It's the Olympics, it's the Olympics! … Mosquitoes? Like, whatever, I'm going. This is my shot.'54 Others expressed concerns about safety.
The reaction of holidaymakers was of fear leading to several cancellations and anxiety among tourism firms and hotels over the financial implications. A travel consultant said she had 10 cancellations in a week, mostly for babymoons (vacations that some parents take before the impending arrival of their baby). Another travel consultant said she had 48 cancellations for trips to the Caribbean and Mexico:
I have a lot of clients who are pregnant or trying to get pregnant, so they're scared and are halting their travel plans altogether or rebooking to travel within the US instead.55
In Brazil, public apathy to the disease was evident during the annual Rio carnival where scantily dressed women danced on the streets in open defiance of the mosquitoes and warnings. In Salvador, a city hit hard by Zika, a lady said: 'Do I look worried? Ask me next week, after Carnival is over.' 'Carnival', the report added, 'is like anaesthesia' as it stops people from thinking about the problems we have…'
No crisis has ever diminished the magic and excitement of Carnival. During pessimistic and depressing times, it becomes more important ... It's escapism on steroids.56
An hotelier, however, pointed out that Brazilians have problems much bigger than Zika. He said: 'Most of my friends are more worried about finding jobs', and added: 'If you're not a pregnant woman, you don't need to worry.' He also noted that dengue fever, which killed more than 800 people in Brazil the previous year, was far more dangerous.56
The Church, politics and abortion
The Catholic Church is opposed to abortion and all forms of contraception, but these are options for women against the disease, reigniting the debate over church, state and choice in Brazil. Both are also bitterly contested in the United States Congress between Democrats and Republicans.
A Cardinal in Brazil said mothers must accept babies born with microcephaly 'as a mission', and that abortion was not an option, but Pope Francis was more open to contraception, arguing that avoiding pregnancy is 'not an absolute evil like abortion which is a crime and an absolute evil'57.
Some Brazilians sought solace in God. A woman, when confronted with a diagnosis of possible microcephaly for her foetus said: 'It's God's will: he wanted us to have a baby like this.'58
There was, however, anxiety over the future of the infected babies. A woman with an infected 3-month-old son wondered about his future and his integration into society:
What kind of life would he have? It gets me angry when someone on the bus looks at Arthur and asks, What's wrong with his head? … I tell them, Nothing's wrong, he's just different. But then I think to myself, Yes, something's wrong. My son will never be like the other boys.59
In the USA, a report noted that while the feud on Capitol Hill over responding to the virus appeared to be over how much money was needed, beneath the surface were issues that have long stirred partisan mistrust, including Republicans' fears about the use of taxpayers' money for abortion and possible increased use of contraception, and Democratic worries about protecting the environment from potentially dangerous pesticides.60
Political, economic and social crisis
It was also a period of severe political and economic crisis in Brazil, leading to cuts in public spending with implications for funding prevention strategies and health care. The epidemic also exposed the wide gap between the rich and the poor in Brazil.
The epidemic mirrors the social inequality of Brazilian society as it is concentrated among young, poor, black and brown women, a vast majority of them living in the country's least-developed regions. The women at greatest risk of contracting Zika live in places where the mosquito is part of their everyday lives, where mosquito-borne diseases like dengue and chikungunya were already endemic.61
The same article indicated that the rich did not feel too concerned:
I am a Brazilian woman. My friends who are planning to have children soon are worried about Zika. But they don't need to be too concerned. In our well-to-do neighbourhood in Brasília, the capital, there has not been a single case of a baby with the birth defects associated with the Zika epidemic.61
Violence among the gangs in the favelas (slums) also posed limitations to containment efforts as even the army, brought in to help clear mosquito breeding sites, were limited to safe areas.
The army has been told not to go into areas controlled by gangs, which could provoke clashes. Health workers negotiate with residents' committees often linked to crime bosses, for safe entry.62
The blame game
Pharmaceutical companies were targets of blame, on the one hand for neglecting diseases which were not deemed profitable, and on the other hand for spreading diseases for profit. Some commentators also blamed urbanisation and air travel - offshoots of social and economic progress.
The same conditions that drove cholera, overcrowding, corruption, poor hygiene, expanded transportation, are what drive pandemics today. In the age of cholera, shipping trade helped spread disease, today, it's air travel. If you want to understand the helter-skelter distribution of flu outbreaks, simply consult a map of airline routes.63
Rumours and conspiracy theories
Rumours are known to thrive during major health crises as the public attempts to find socio-political and economic origins of disease. Some people suggested that the plea by the government of El Salvador to delay having children was an effort to stem population growth. A lady said 'This government doesn't want anyone else … We don't fit already!'64
There were other interests opposed to genetic modification of insects and global powers. An article read:
The Zika virus, some Brazilians are convinced, is the inadvertent creation of a biotech company that has been releasing genetically modified mosquitoes to combat dengue fever in Brazil. Others here and elsewhere see it as a plot by global elites to depopulate the earth and install a 'one-world government'.65
Conclusions
The detection of aberrations in patterns, the emergence of discourse about disease and public perceptions bring together three areas of research: epidemiology, media and social psychology. Combining multiple approaches allows epidemiologists to harness the strengths of individual research paradigms for a whole that has the potential to be greater than the sum of its parts.
The news media are fairly stable artefacts in cultural contexts; deviations or aberrations indicating new disease debates or a sudden upsurge in coverage of known diseases or the flagging of potential obstacles to scientific interventions should trigger the need for further clinical investigation and early interventions. As no single approach is optimal and extensive monitoring aids detection6,7, media informatics, as this research has shown, has great potential as part of a web of disease surveillance mechanisms16,18,21.
The high upsurge in media discourse about dengue in Brazil in 2015 was an early indication to sound the alarm for extensive clinical investigations on the causes of the sudden aberration. This shows that a sudden rise in public anxiety about a known disease was the indicator of the emergence of an alien species with similar symptoms. This finding affirms the suitability of longitudinal mass media data as part of a complex of syndromic surveillance mechanisms. The flagging of Zika by one newspaper and not another in the sample also shows the need to use multiple sources for surveillance.
Qualitative indicators show the extra motivation over Google, web or Twitter searches in that they further mirror the perception of the public about the disease and psychosocial factors that may enhance or inhibit uptake. The Zika virus epidemic was not a case of public deficit in knowledge of the disease in contrast to scientists36,37 or of mistrust or expert deficit36. This was an instance of a virus, benign in its natural habitat, which crossed the continent and became virulent in another country. The virus also presents with the same symptoms of locally established diseases such as dengue and chikungunya. Zika was the 'doença misteriosa', or mystery disease, which initially puzzled both scientists and the public.
The knowledge crisis, inadequate infrastructure to detect the presence of the disease and its capacity to globalise led to a global alarm and the declaration of a global health emergency. International concern focused on the risk to travellers for the Rio Carnival, the Olympics and tourism, all of which attract thousands of visitors to Brazil with the risk of being infected and transmitting the disease to their home countries. Local issues were about prevention, obstacles to containing the spread of the disease, the blame game, rumours and living with long-term effects on the children born to infected mothers.
The spread of the Zika virus has shown that in the age of international mobility, classification of a disease as benign is no longer sustainable and surveillance needs to be extended to uninfected areas, particularly where possible vectors of the disease can be found. Also in the age of massive computing power and web crawlers, monitoring public anxiety over diseases around the world in real time using a keyword approach is increasingly possible. Scientists also need to investigate why some diseases appear harmless in some communities, the source of immunity in these populations, the applicability of the immunity to vaccine production and the consequences if the disease appears in new areas - that the disease is not yet there does not preclude it from reaching there.
Acknowledgements
The South African Research Chair in Science Communication is the initiative of the Department of Science and Technology and the National Research Foundation of South Africa (grant no. 93097). Assistance for writing and publication was also received from the MACAS Project (Mapping the Cultural Authority of Science) (www.macas-project.com) Economic and Social Research Council (ESRC), UK grant ES/K005820/1, through the Department of Psychological and Behavioural Sciences, London School of Economics and Political Science. Dr Kikelomo Wright of the Community Health & Primary Health Care Department of the Lagos State University Teaching Hospital, Nigeria, is thanked for her comments which assisted in shaping the article. The data will be provided in txt. form if required and are available from NEXIS with licence and permission.
References
1.Park E. News as a form of knowledge. A chapter in the sociology of knowledge. Am J Sociol. 1940;45(5):669-686. https://doi.org/10.1086/218445 [ Links ]
2.Jovchelovitch S. Knowledge in context: Representations, community and culture. New York: Routledge; 2007. [ Links ]
3.Centers for Disease Control and Prevention. Principles of epidemiology in public health practice: An introduction to applied epidemiology and biostatistics [webpage on the Internet]. No date [updated 2012 May 18; cited 2018 Jan 01]. Available from: https://www.cdc.gov/ophss/csels/dsepd/ss1978/lesson1/section1.html [ Links ]
4.Bernardo TM, Rajic A, Young I, Robiadek K, Pham MT, Funk JA. Scoping review on search queries and social media for disease surveillance: A chronology of innovation. J Med Internet Res. 2013;15(7), e147, 13 pages. https://doi.org/10.2196/jmir.2740 [ Links ]
5.Aslam AA, Tsou MH, Spitzberg BH, An L, Gawron JM, Gupta KD, et al. The reliability of tweets as a supplementary method of seasonal influenza surveillance. J Med Internet Res. 2014;16(11), e250, 12 pages. https://doi.org/10.2196/jmir.3532 [ Links ]
6.Groseclose SL, Buckeridge DL. Public health surveillance systems: Recent advances in their use and evaluation. Annu Rev Public Health. 2017;38:57-79. https://doi.org/10.1146/annurev-publhealth-031816-044348 [ Links ]
7.Freifeld CC, Mandl KD, Reis BY, Brownstein JS. HealthMap: Global infectious disease monitoring through automated classification and visualization of Internet media reports. J Am Med Inform Assoc. 2008;15(2):150-157. https://doi.org/10.1197/jamia.M2544 [ Links ]
8.McQuail D. The influence and effects of mass media. Mass Commun Soc. 1977:70-94. [ Links ]
9.McCombs ME, Shaw DL. The agenda-setting function of mass media. Public Opin Q. 1972;36(2):176-187. https://doi.org/10.1086/267990 [ Links ]
10.Cohen BC. The press and foreign policy. Princeton, NJ: Princeton University Press; 1963. [ Links ]
11.Washer P, Joffe H. The "hospital superbug": Social representations of MRSA. Soc Sci Med. 2006;63(8):2141-2152. https://doi.org/10.1016/j.socscimed.2006.05.018 [ Links ]
12.Joffe H, Haarhoff G. Representations of far-flung illnesses: The case of Ebola in Britain. Soc Sci Med. 2002;54(6):955-969. https://doi.org/10.1016/S0277-9536(01)00068-5 [ Links ]
13.Falade BA, Coultas CJ. Scientific and non-scientific information in the uptake of health information: The case of Ebola. S Afr J Sci. 2017;113(7/8), Art. #2016-0359, 8 pages. https://doi.org/10.17159/sajs.2017/20160359 [ Links ]
14.Falade B. Familiarizing science: A Western conspiracy and the vaccination revolt in Northern Nigeria. Pap Soc Represent. 2015;24:3.1-3.24. [ Links ]
15.Henning KJ. Overview of syndromic surveillance. What is syndromic surveillance? Morbidity Mortality Weekly Rep. 2004;53(Suppl):5-11 [article online]. No date [updated 2004 Sep 09; cited 2018 Nov 12]. Available from: https://www.cdc.gov/mmwr/preview/mmwrhtml/su5301a3.htm [ Links ]
16.Tausczik Y, Faasse K, Pennebaker JW, Petrie KJ. Public anxiety and information seeking following the H1N1 outbreak: Blogs, newspaper articles, and Wikipedia visits. J Health Commun. 2012;27(2):179-185. https://doi.org/10.1080/10410236.2011.571759 [ Links ]
17.Müller O, Junglas I, Vom Brocke J, Debortoli S. Utilizing big data analytics for information systems research: Challenges, promises and guidelines. Eur J Inf Syst. 2016;25(4):289-302. https://doi.org/10.1057/ejis.2016.2 [ Links ]
18.Santillana, M, Nguyen AT, Dredze M, Paul MJ, Nsoesie EO, Brownstein, JS. Combining search, social media, and traditional data sources to improve influenza surveillance. PLoS Comput Biol. 2015;11(10), e1004513, 15 pages. https://doi.org/10.1371/journal.pcbi.1004513 [ Links ]
19.Signorini A, Segre AM, Polgreen PM. The use of Twitter to track levels of disease activity and public concern in the US during the influenza A H1N1 pandemic. PLoS One. 2011;6(5), e19467, 10 pages. https://doi.org/10.1371/journal.pone.0019467 [ Links ]
20.Alicino C, Bragazzi NL, Faccio V, Amicizia D, Panatto D, Gasparini R, et al. Assessing Ebola-related web search behaviour: Insights and implications from an analytical study of Google Trends-based query volumes. Infect Dis Poverty. 2015;4(1), Art. #54, 13 pages. https://doi.org/10.1186/s40249-015-0090-9 [ Links ]
21.Nuti SV, Wayda B, Ranasinghe I, Wang S, Dreyer RP, Chen SI, et al. The use of Google Trends in health care research: A systematic review. PLoS One. 2014;9(10), e109583, 49 pages. https://doi.org/10.1371/journal.pone.0109583 [ Links ]
22.Chan EH, Sahai V, Conrad C, Brownstein JS. Using web search query data to monitor dengue epidemics: A new model for neglected tropical disease surveillance. PLoS Negl Trop Dis. 2011;5(5), e1206, 6 pages. https://doi.org/10.1371/journal.pntd.0001206 [ Links ]
23.Petersen J, Simons H, Patel D, Freedman J. Early detection of perceived risk among users of a UK travel health website compared with Internet search activity and media coverage during the 2015-2016 Zika virus outbreak: An observational study. BMJ Open. 2017;7(8), e015831, 6 pages. https://doi.org/10.1136/bmjopen-2017-015831 [ Links ]
24.Ribeiro B, Hartley S, Nerlich B, Jaspal R. Media coverage of the Zika crisis in Brazil: The construction of a 'war' frame that masked social and gender inequalities. Soc Sci Med. 2018;200:137-144. https://doi.org/10.1016/j.socscimed.2018.01.023 [ Links ]
25.Giardullo P. Spreading mosquitoes: A media analysis of Italian national newspaper coverage of mosquito-borne diseases and related interventions. In: Claeys C, editor. Mosquito management: Environmental issues and health concerns. Brussels: PIE Peter Lang; 2018. p. 84-111. [ Links ]
26.Pan American Health Organization/World Health Organization. Timeline of emergence of Zika virus in the Americas [webpage on the Internet]. c2016 [updated 2017 Jan 17; cited 2017 Sep 09]. Available from: http://www.paho.org/hq/index.php?option=com_content&view=article&id=11959%3Atimeline-of-emergence-of-zika-virus-in-the-americas&catid=8424%3Acontents&Itemid=41711&lang=en [ Links ]
27.Zanluca C, Melo VCAD, Mosimann ALP, Santos GIVD, Santos CNDD, Luz K. First report of autochthonous transmission of Zika virus in Brazil. Mem Inst Oswaldo Cruz. 2015;110(4):569-572. https://doi.org/10.1590/0074-02760150192 [ Links ]
28.Hayes EB. Zika virus outside Africa. Emerg Infect Dis. 2009;15(9):1347-1350. https://doi.org/10.3201/eid1509.090442 [ Links ]
29.Chen LH, Hamer DH. Zika virus: Rapid spread in the western hemisphere. Ann Intern Med. 2016;164(9):613-635. [ Links ]
30.World Health Organization. The history of Zika [webpage on the Internet]. No date [updated 2017 Feb 01; cited 2017 Dec 12]. Available from: https://www.who.int/emergencies/zika-virus/timeline/en/ [ Links ]
31.Peiris JSM, Guan Y, Yuen KY. Severe acute respiratory syndrome. Nat Med. 2004;10(12s):S88-S97. https://doi.org/10.1038/nm1143 [ Links ]
32.Goodwin R, Haque S, Neto F, Myers LB. Initial psychological responses to Influenza A, H1N1 ("Swine flu"). BMC Infect Dis. 2009;9(1), Art. #166, 6 pages. https://doi.org/10.1186/1471-2334-9-166 [ Links ]
33.Bauer M. Atoms, bytes and genes - Public resistance and techno-scientific responses. New York: Routledge; 2014. [ Links ]
34.Slovic P. Perception of risk. Science. 1987;236(4799):280-285. https://doi.org/10.1126/science.3563507 [ Links ]
35.Slovic P, Finucane ML, Peters E, MacGregor DG. Risk as analysis and risk as feelings: Some thoughts about affect, reason, risk and rationality. Risk Anal. 2004;24(2):311-322. https://doi.org/10.1111/j.0272-4332.2004.00433.x [ Links ]
36.Wynne B. Rationality and ritual: The Windscale inquiry and nuclear decisions in Britain. Chalfont St. Giles: British Society for the History of Science; 1982. [ Links ]
37.Ziman J. The public understanding of science. Sci Technol Hum Val. 1991;16(1):99-105. https://doi.org/10.1177/016224399101600106 [ Links ]
38.Bauer MW, Allum N, Miller S. What can we learn from 25 years of PUS survey research? Liberating and expanding the agenda. Public Underst Sci. 2007;16:79-95. https://doi.org/10.1177/0963662506071287 [ Links ]
39.Einseidel EF. Understanding publics in the public understanding of science. In: Dierkes M, Grote V, editors. Between understanding and public trust: The public, science and technology. London: Gordon and Breach Publishing Group; 2000. p. 144-149. [ Links ]
40.Jovchelovitch S, Priego-Hernandez J. Cognitive polyphasia, knowledge encounters and public spheres. The Cambridge handbook of social representations. Cambridge: Cambridge University Press; 2015. p. 163-178. https://doi.org/10.1017/CBO9781107323650.014 [ Links ]
41.Moscovici S. La Psychanalyse, son image et son public [Psychoanalysis: Its image and its public. Cambridge: Polity Press; 2008. French. [ Links ]
42.Gerbner G. Toward "cultural indicators": The analysis of mass mediated public message systems. AV Commun Rev. 1969;17(2):137-148. [ Links ]
43.Southwell BG, Dolina S, Jimenez-Magdaleno K, Squiers LB, Kelly BJ. Zika virus-related news coverage and online behavior, United States, Guatemala, and Brazil. Emerg Infect Dis. 2016;22(7):1320-1321. https://doi.org/10.3201/eid2207.160415 [ Links ]
44.McNeil D. Influx of brain damage may be linked to virus. The New York Times. 2015 December 29;6. [ Links ]
45.McNeil D, Romeo S. Pregnant women warned on Latin American trips. The New York Times. 2016 January 16;3. [ Links ]
46.Romero SA. Struggle against mosquito-borne diseases. The New York Times. 2016 January 18;4. [ Links ]
47.Sreeharsha V. Guidelines may lead to over-reporting of defect in Brazil. The New York Times. 2016 February 04;10. [ Links ]
48.Hirst P. Rutherford freezes sperm over Zika fear. The Times of London. 2016 June 08;76. [ Links ]
49.Belluck P, McNeil D. Health officials say Zika damages infant brains. The New York Times. 2016 April 14;16. [ Links ]
50.Moscovici S. The phenomenon of social representations. In: Farr RM, Moscovici S, editors. Social representations. Cambridge: Cambridge University Press; 1984. p. 3-69. [ Links ]
51.Smith RD. Responding to global infectious disease outbreaks: Lessons from SARS on the role of risk perception, communication and management. Soc Sci Med. 2006;63(12):3113-3123. https://doi.org/10.1016/j.socscimed.2006.08.004 [ Links ]
52.Whipple T. Move Rio Olympics over virus; Zika threat too great, say 100 leading scientists. The Times of London. 2016 May 28;1-2. [ Links ]
53.Boswell J, Leake J. Olympic chiefs dismiss Zika fears for Rio. The Sunday Times. 2016 May 29;2. [ Links ]
54.Maccur J. Opting to skip Olympics because of Zika fears. The New York Times. 2016 June 04;7. [ Links ]
55.Vora S. How the Zika virus is affecting travel. The New York Times. 2016 January 29;In Transit. Available from: https://www.nytimes.com/2016/01/29/travel/how-the-zika-virus-is-affecting-travel.html [ Links ]
56.Jacobs A, Perpétua S. Zika? Partying Brazilians offer collective shrug. The New York Times. 2016 February 11;1. [ Links ]
57.Kington T. Pope ready to lift condom ban in fight against Zika. The New York Times. 2016 February 19;5. [ Links ]
58.Bowater D. How the Zika virus is striking at the heart of terrified families in Brazil. The Daily Telegraph, London. 2016 January 30;7. [ Links ]
59.Romeo S, Sreeharsha V. Tears and bewilderment at center of Zika crisis. The New York Times. 2016 January 30;1. [ Links ]
60.Herszenhorn D. Partisan mistrust adds complexity to congressional feuding over Zika. The New York Times. 2016 May 25;15. [ Links ]
61.Doniz D. Zika and a woman's right to choose. The New York Times. 2016 February 08;25. [ Links ]
62.Hider J. Fear and conspiracy theories hinder Brazil's Zika battle. The Times of London. 2016 February 22;2016: 34. [ Links ]
63.Senior J. Hosting the perfect pathogen party. The New York Times. February 25, 2016: 1. [ Links ]
64.Ahmed A. El Salvador's advice on Zika: Don't have babies. The New York Times. 2016 January 26;1. [ Links ]
65.Jacobs A. Conspiracy theories about Zika spread through Brazil with the virus. The New York Times. 2016 February 17;6. [ Links ]
 Correspondence:
Correspondence:
Bankole Falade
bankolefalade@gmail.com
Received: 02 July 2018
Revised: 12 Nov. 2018
Accepted: 29 Nov. 2018
Published: 27 Mar. 2019


{kind=link}