










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Science
On-line version ISSN 1996-7489
Print version ISSN 0038-2353
S. Afr. j. sci. vol.114 n.9-10 Pretoria Sep./Oct. 2018
http://dx.doi.org/10.17159/sajs.2018/4407
RESEARCH ARTICLE
Food insecurity, HIV status and prior testing at South African primary healthcare clinics
Makandwe NyirendaI; Renee StreetI, II; Tarylee ReddyIII; Susie HoffmanIV, V; Suraya DawadI, VI; Kelly BlanchardVII; Theresa M. ExnerV; Elizabeth A. KelvinVIII, IX; Joanne E. MantellV; Gita RamjeeI
IHIV Prevention Research Unit, South African Medical Research Council, Durban, South Africa
IIEnvironment and Health Research Unit, South African Medical Research Council, Durban, South Africa
IIIBiostatistics Unit, South African Medical Research Council, Durban, South Africa
IVDepartment of Epidemiology, Columbia University, New York, New York, USA
VHIV Center for Clinical and Behavioural Studies, New York State Psychiatric Institute and Columbia University, New York, New York, USA
VINational Department of Health, Pretoria, South Africa
VIIIbis Reproductive Health, Cambridge, Massachusetts, USA
VIIIDepartment of Epidemiology and Biostatistics, City University of New York, New York, New York, USA
IXCUNY Institute for Implementation Science in Population Health, City University of New York, New York, New York, USA
ABSTRACT
HIV and food insecurity are two prominent causes of morbidity and mortality in sub-Saharan Africa. Food insecurity has been associated with risky sexual practices and poor access to healthcare services. We describe the association between household food insecurity and previous HIV testing and HIV status. We used logistic regression to analyse the association between food insecurity and prior HIV counselling and testing (HCT) and testing HIV positive. A total of 2742 adults who presented for HCT at three primary healthcare clinics in KwaZulu-Natal, South Africa, participated in the study. The prevalence of household food insecurity was 35%. The prevalence of food insecurity was highest in adults who had incomplete high schooling (43%), were unemployed (39%), and whose primary source of income was government grants (50%). Individuals who were food insecure had significantly higher odds of testing HIV positive (adjusted odds ratio 1.41, 95% CI 1.16-1.71), adjusted for demographic and socio-economic variables. There was no association between food insecurity and prior HCT. The findings of this study highlight the important role food insecurity may play in HIV risk. Interventions to turn food-insecure into food-secure households are needed to reduce their household members' vulnerability to HIV acquisition. The absence of such interventions is likely to severely impact ambitious global targets of ending AIDS by 2030 through the 90-90-90 targets and test-and-treat-all initiatives.
Significance:
• One in three adults presenting for HIV counselling and testing came from households with some degree of food insufficiency.
• Experience of food insecurity was very high in young people who did not complete high school and were currently not studying.
• Findings support the need for socio-economic and structural interventions to transform food-insecure into food-secure households.
• Failure or lack of such interventions will contribute to the failure to achieve global targets like the UNAIDS 90-90-90 programme.
Keywords: household food insecurity; HIV counselling; HIV testing; primary health care; South Africa
Introduction
To end AIDS as a global pandemic by 2030, UNAIDS has set the world ambitious targets of 90-90-90.1 That is, by 2020, 90% of all persons living with HIV will be tested and know their status; of those tested positive, 90% will be on antiretroviral treatment; and finally, 90% of those on antiretroviral treatment will achieve viral suppression. HIV counselling and testing (HCT) is thus the initial step in the cascade of HIV prevention, care and treatment towards ending HIV as a public health pandemic.1,2 A number of factors have been identified as contributory to the low uptake of HIV testing services including hunger, poor nutrition and food insecurity.3 In South Africa, the recent National Health and Nutrition Examination Survey revealed that 28% of the population are at risk of hunger and 26% are household food insecure (ever experienced hunger).4
Much of the empirical research focus has been on the relationship between food insecurity and the health and well-being of HIV-infected persons.5-9 Food insecurity has been shown to be associated with poor health and poor adherence to medication, including antiretroviral drugs.10-12 In South Africa, one of the main reasons cited for not accepting free antiretroviral drugs was fear of taking medication on an empty stomach as a consequence of food insufficiency.13,14 In Tanzania, supplementary food cost was cited as an access challenge in sustaining long-term antiretroviral treatment.15
Food insecurity also has been suggested to be a major contributor to risky sexual behaviour and HIV spread in neighbouring Botswana and Swaziland16 and elsewhere. Those who report food insecurity have been found to be less likely to use condoms than those who report food security.17,18
Much less research has focused on the effect of food insecurity on health-seeking behaviour including HIV testing. To date, there is no information on the role of household food insecurity in HIV testing history and/or testing HIV positive among South Africans.
To address this gap, the aim of this study was to determine the association of household food insecurity with prior HIV testing and HIV serostatus among individuals presenting for HCT at public primary healthcare clinics in KwaZulu-Natal, South Africa. We hypothesised that household food insecurity would be associated with lower likelihood to have previously tested for HIV and higher likelihood to be HIV positive when tested.
Methods
Study population
Data for these cross-sectional analyses were drawn from interviews conducted between November 2010 and May 2012 as part of the Pathways to Care study, a prospective cohort study of newly diagnosed HIV-positive women and men, described elsewhere.19 Women and men presenting for HCT at three public-sector primary healthcare clinics in the Durban region (KwaZulu-Natal, South Africa) were invited to be interviewed prior to HCT. Eligibility for the interview included being 18 years or older, anticipating residing in the community for at least 1 year, being not pregnant, able to speak and understand English or isiZulu, and willing to have HIV test results shared with the study interviewer. Of the population presenting for HCT at the three primary healthcare clinics, 2996 individuals were approached to participate in the study. Of those approached, 29 were not interested and 76 were ineligible based on: age (n=30), pregnancy (n=31), would not be residing in the study community for longer than a year (n=8), and cognitive impairment (n=7). A further 106 individuals who had previously tested HIV positive, 41 individuals with incomplete pre-screening or screening assessments, and 2 individuals with missing data on key study variables were excluded, leaving a final sample size of 2742 individuals for this analysis. For the analysis of HIV status, there were 2693 individuals, as 5 were not tested and it was not possible to determine results for 44 individuals. Written informed consent was obtained prior to the screening interview, and the principles of the Declaration of Helsinki were adhered to throughout the study. Participants were reimbursed ZAR40 (the approximate equivalent of USD5 at the time) for the interview. All study procedures were approved prior to study initiation by the University of KwaZulu-Natal Biomedical Research Ethics Committee and the NYS Psychiatric Institute of the Columbia University Institutional Review Boards.
Data sources
A structured questionnaire of approximately 20-min duration was administered by trained interviewers. Items included socio-demographic factors, history of prior HIV testing, reasons for testing, and who recommended testing. HCT was conducted by clinic staff according to standard rapid testing procedures, after which participants returned to the study interviewer with a card that indicated their HIV test result using a code to blind the information. If participants did not return to the study interviewer after HCT, the interviewer obtained test results directly from the clinic testing counsellor.
Measures
Outcome variables
Positive HIV test: This was a dichotomous variable indicating whether the person tested positive or negative on the day of their visit to the primary healthcare clinic.
Previous HIV testing: This variable was categorised as 'never' if the individual had no history of previous testing for HIV or 'ever' if the individual had ever taken an HIV test before presenting for HCT at the health facility.
Predictor
Food insecurity: The dichotomous household food insecurity variable (ever/never) was created from responses to the question 'Do the people in your household go without food?' The 'ever' category consisted of response options 'often', 'sometimes' or 'seldom', and 'never' was for those who never went without food in their household.
Confounders
Informed by available empirical literature,17,20,21 potential confounders controlled for in the analysis of HIV status included age categorised into age ranges (<24, 25-28, 29-31, 32-36, ≥37 years), gender, clinic site, educational attainment (completed high school or not), relationship status (not married or in a relationship; married or in a relationship, not living together; married or in a relationship, and living together), employment status (employed part-time/full-time/self-employed or unemployed), primary source of income (none, family, employment, spouse/partner, government grant, or other), caring for dependent adults and/or children (none, children only, adults only, both), ability to borrow money (up to ZAR100) if needed for medical expenses (yes/no), and time taken to travel to the clinic (<30 min, 30-60 min, >60 min).
Statistical analysis
Chi-square tests were used to evaluate the association between each demographic and socio-economic factor and household food insecurity. The relationship between household food insecurity and previous HIV testing and HIV status was examined using univariable and multivariable logistic regression models. A variable was deemed a potential confounder if its inclusion in the model containing food security resulted in a 10% or higher change in the model coefficient for food security.
Results
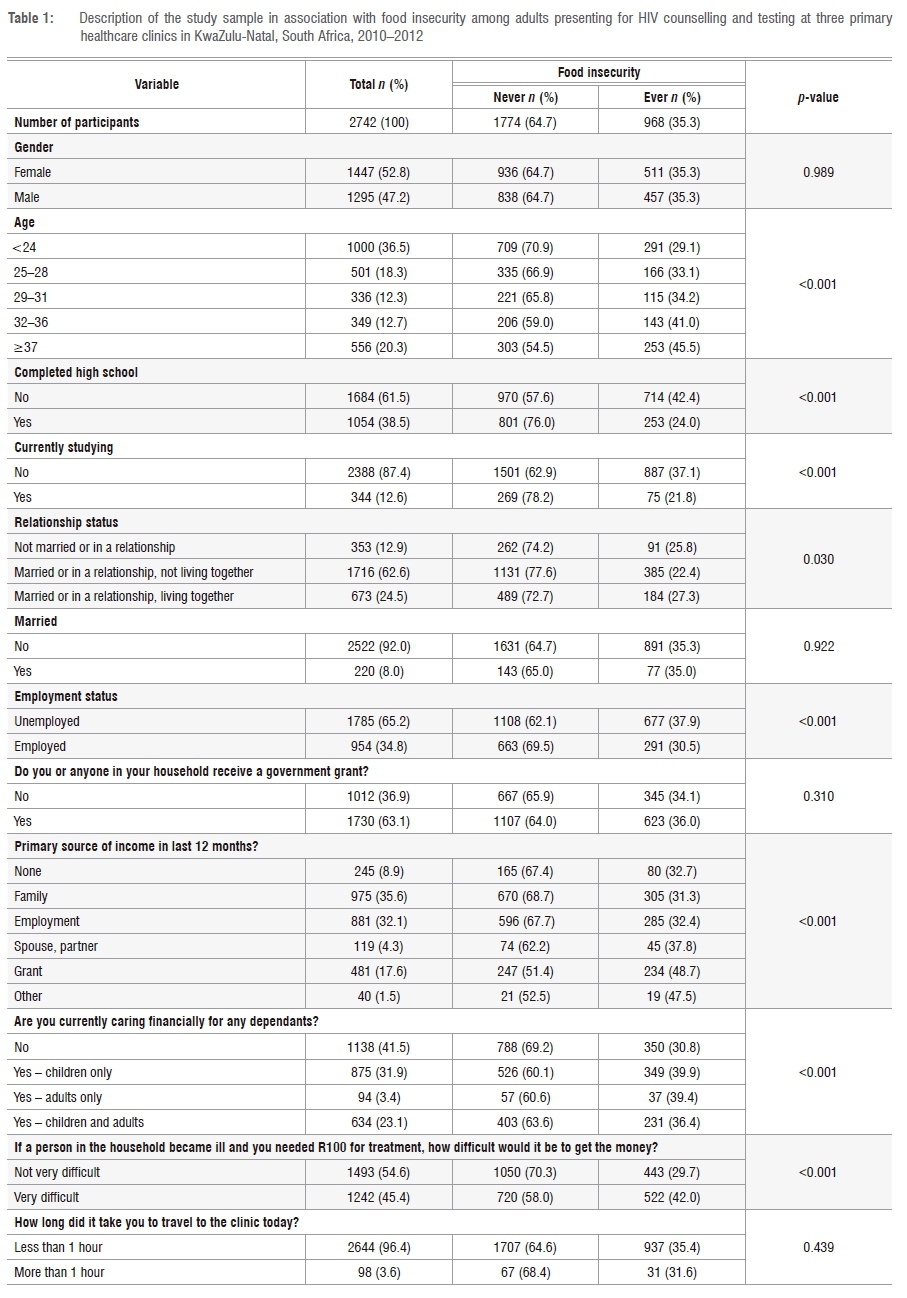
The majority of the participants in this analysis were women (52.8%), were aged less than 24 years (36.5%), had not completed high school (61.5%), were not currently studying (87.4%) and were married or in a relationship but not living together (62.6%) (Table 1). Further characteristics of the sample were that most were unemployed (65.1%) but were currently caring for a dependent adult or child (58.5%). Nearly two-thirds of participants came from households with at least one government grant recipient (63.1%). Nearly all participants (96.4%) travelled less than 1 hour to get to the primary healthcare clinic.
The overall prevalence of food insecurity in this sample was 35.3% (Table 1). There were no statistically significant gender differences in reported household food insecurity (p=0.989). Prevalence of food insecurity increased with age and was highest among adults older than 37 years (45.5%, p<0.001). Household food insecurity was also more prevalent in adults who did not complete high school (42.4%); were currently not in school (37.1%) compared with those who had completed high school (24.0%); and individuals who were married or in a co-habiting relationship (27.3%) compared with those who were married or in a relationship but not co-habiting (22.4%). Regarding socio-economic factors, experience of food insecurity was highest among unemployed participants (37.9%) and adults currently financially caring for children (39.9%). Table 1 further shows that 48.7% of individuals whose primary source of income was from government grants reported experiencing some household food insecurity compared to 32.7% among individuals with no income, or family (31.3%) or employment (32.4%) as their primary income source. Experiencing household food insecurity was similarly high (42.0%) in adults who found it very difficult to borrow ZAR100 if needed in situations of ill health.
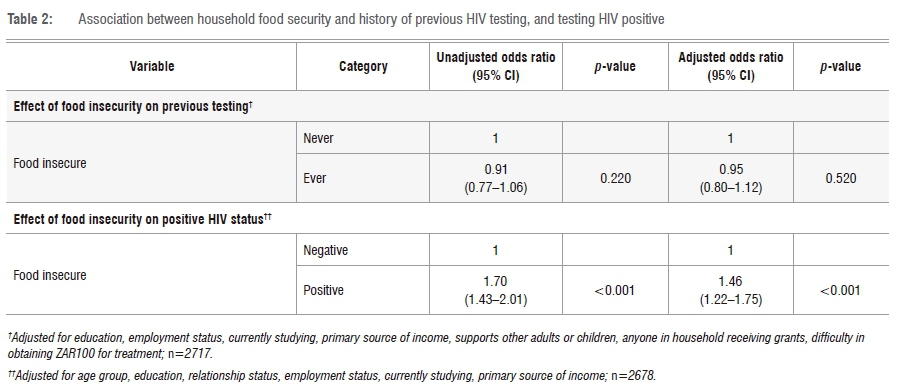
Table 2 shows the unadjusted odds ratio (OR) of ever having been tested associated with food insecurity and the OR adjusting for confounding variables (gender, age, relationship status, employment status, primary source of income, financially supporting other adults or children, and travel time to clinic). We found that household food insecurity was not significantly associated with history of previous HIV testing (OR=0.95, 95% confidence interval (CI)=0.80-1.12, p=0.520).
Table 2 also presents the unadjusted and adjusted ORs for the association between household food insecurity and testing HIV positive. In both the unadjusted (OR=1.70, 95%CI=1.43-2.01) and adjusted models (OR=1.46, 95%CI=1.22-1.75), individuals who had ever experienced household food insecurity had higher odds of testing HIV positive when they presented for HCT at primary healthcare facilities.
Discussion
As UNAIDS has set ambitious global targets of 90-90-90 to be reached by 2020 in order to end AIDS as a global pandemic by 2030, achieving or exceeding the first 90% (that is, 90% of all adults knowing their HIV status) is key to ending the epidemic given the expected fallout along the cascade steps from testing to treatment and viral suppression.22,23 We examined the links between household food insecurity and previous HIV testing and testing HIV positive to ascertain if food insecurity is a barrier to HIV testing or a risk factor for HIV infection. We found that 35.3% of study participants came from households with some degree of food insufficiency. Although there was no association between household food insecurity and previous HIV testing, individuals who were food insecure had significantly higher odds of testing HIV positive [OR 1.47 (1.22-1.77)].
Our study revealed that 29.1% of those reporting household food insecurity were young adults (<24 years old). The incidence of HIV in South Africa is highest among young women below age 25.24-26 The majority (61.9%) of participants in our study had not completed high school. Experience of food insecurity was higher among participants who had not completed high school compared to those who had completed high school (42.4% versus 24.0%, respectively). Weiser et al.16 found that educational level did not significantly influence the association between food insecurity and risky sexual behaviour. However, De Swardt et al.27 found a positive relationship between educational level and strategies to survive food crises among South African households. Higher educational level was shown to be associated with greater ability to survive a food crisis.27 Elsewhere it has further been shown that completing secondary education helps to protect against HIV acquisition, more so among young girls.18,28
HIV and food insecurity are leading causes of morbidity and mortality in sub-Saharan Africa. Eradication of both HIV and food insecurity is central to the Sustainable Development Goals.29 The first three of these goals are to: (1) end poverty of every form; (2) end hunger, ensure food security and better nutrition through sustainable farming; and (3) ensure health and well-being for all. Despite South Africa willingly consenting to the SDGs, the proportions of at-risk and food-insecure households have remained largely unchanged over the years.4,30 Considering the association between food insecurity and high-risk sexual behaviour that has been demonstrated by others among women in southern Africa16, it is a likely contributory factor to the continued high HIV risk among young women and may explain the association we found in this study17,20,21.
There are some limitations to this study that should be mentioned. This analysis relied on self-reports of food sufficiency in the household by an individual member of the household. In addition, study participants were interviewed about food security cross-sectionally. Thus, we were unable to determine whether food insecurity 'caused' someone to become HIV positive or whether being HIV positive created a condition of food insecurity. A more robust design would have been to conduct a longitudinal cohort study using food diaries. This approach was, however, not feasible and beyond the scope of the Pathways to Care study. The study was also limited by the use of a single question to assess food insecurity. Finally, we did not have data that would have enabled us to explore sexual risk behaviour as a possible mediator of the association that we found between HIV positive status and food insecurity.
Despite these limitations, this analysis makes an important contribution to the literature. A strength of the analysis is that study participants were newly diagnosed HIV-positive individuals; therefore, we could show the likely role of food insecurity in seeking HIV counselling and testing. Findings of this study, together with other available literature, support the need for socio-economic and structural interventions that will transform households experiencing food insecurity into food-secure households so as to reduce household members' vulnerability to HIV acquisition. This recommendation is consistent with the Sustainable Development Goals. Failure or lack of such prudent interventions is likely to contribute to the failure to achieve the UNAIDS 90-90-90 goals.
Conclusion
Household food insecurity is related to similar risk factors for HIV, such as low education, not attending school, not being married and low socio-economic status.25,31,32 Although we did not find an association between food insecurity and prior HCT, we found that testing HIV positive was associated with household food insecurity among adults attending HCT at public primary healthcare facilities. These findings highlight the important role that food insecurity plays in HIV risk, and are supported by findings from other sub-Saharan African countries.16,17 Thus, interventions such as targeted food support in poor and food-insecure populations are key to mitigating vulnerability to HIV infection. In South Africa, such an intervention could be implemented with similar means testing, as the child support or old age grants.33,34 If left unaddressed, household food insecurity is likely to adversely affect the global targets of ending AIDS by 2030 through the 90-90-90 and test-and-treat initiatives.
Acknowledgements
The contributions of individuals who participated in this research are greatly acknowledged. This research was supported by the US National Institute of Mental Health (R01 MH83561 and R01 MH083561-03S1; Principal Investigator: Susie Hoffman, DrPH), and by a grant from the National Institute of Mental Health to the HIV Center for Clinical and Behavioral Studies at NY State Psychiatric Institute and Columbia University [P30-MH43520; Principal Investigators: Anke A. Ehrhardt (1987-2013)/Robert H. Remien, PhD (2013-2018)]. Additional support was provided by the South African Medical Research Council to M.N. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Mental Health or the South African Medical Research Council. We thank the anonymous peer reviewers of this manuscript.
Authors' contributions
M.N.: Conceptualisation, data analysis, writing the initial draft, writing revisions. R.S.: Conceptualisation, writing the initial draft, critically reviewing the writing. T.R.: Methodology, sample analysis, critically reviewing the writing. S.H. Conceptualisation, methodology, data collection, data analysis, data curation, critically reviewing the writing, writing revisions, project leadership, funding acquisition. S.D.: Data collection, critically reviewing the writing, writing revisions, funding acquisition. K.B.: Data collection, validation, critically reviewing the writing, writing revisions. T.M.E.: Conceptualisation, critically reviewing the writing, writing revisions. E.A.K.: Data collection, critically reviewing the writing, writing revisions, project leadership. J.E.M.: Conceptualisation, critically reviewing the writing, writing revisions, project leadership. G.R.: Conceptualisation, methodology, data collection, critically reviewing the writing, writing revisions, project leadership, funding acquisition.
References
1. UNAIDS. 90-90-90: An ambitious treatment target to help end the AIDS epidemic. Geneva: Joint United Nations Programme on HIV/AIDS (UNAIDS); 2014. [ Links ]
2. World Health Organization (WHO). Towards universal access: Scaling up priority HIV/AIDS interventions in the health sector: Progress report April 2007. Geneva: WHO; 2007. [ Links ]
3. UNAIDS. UNAIDS guidance for partnerships with civil society, including people living with HIV and key populations. Geneva: UNAIDS; 2011. [ Links ]
4. Hongoro C, Hoosain E, Maluleke T, Reddy P, Jacobs L, Shisana O, et al. The South African National Health and Nutrition Examination Survey: SANHANES-1. Cape Town: HSRC Press; 2014. [ Links ]
5. Weiser SD, Young SL, Cohen CR, Kushel MB, Tsai AC, Tien PC, et al. Conceptual framework for understanding the bidirectional links between food insecurity and HIV/AIDS. Am J Clin Nutr. 2011;94(6):1729S-1739S. https://doi.org/10.3945/ajcn.111.012070 [ Links ]
6. Pellowski JA, Kalichman SC, Cherry S, Conway-Washington C, Cherry C, Grebler T, et al. The daily relationship between aspects of food insecurity and medication adherence among people living with HIV with recent experiences of hunger. Ann Behav Med. 2016;50(6):844-853. https://doi.org/10.1007/s12160-016-9812-x [ Links ]
7. Boyer S, Iwuji C, Gosset A, Protopopescu C, Okesola N, Plazy M, et al. Factors associated with antiretroviral treatment initiation amongst HIV-positive individuals linked to care within a universal test and treat programme: Early findings of the ANRS 12249 TasP trial in rural South Africa. AIDS Care. 2016;28(suppl3):39-51. https://doi.org/10.1080/09540121.2016.1164808 [ Links ]
8. Aibibula W, Cox J, Hamelin AM, Mamiya H, Klein MB, Brassard P. Food insecurity and low CD4 count among HIV-infected people: A systematic review and meta-analysis. AIDS Care. 2016;28(12):1577-1585. https://doi.org/10.1080/09540121.2016.1191613 [ Links ]
9. Singer AW, Weiser SD, McCoy SI. Does food insecurity undermine adherence to antiretroviral therapy? A systematic review. AIDS Behav. 2015;19(8):1510-1526. https://doi.org/10.1007/s10461-014-0873-1 [ Links ]
10. Young S, Wheeler AC, McCoy SI, Weiser SD. A review of the role of food insecurity in adherence to care and treatment among adult and pediatric populations living with HIV and AIDS. AIDS Behav. 2014;18(5):505-515. https://doi.org/10.1007/s10461-013-0547-4 [ Links ]
11. Ivers LC, Chang Y, Gregory Jerome J, Freedberg KA. Food assistance is associated with improved body mass index, food security and attendance at clinic in an HIV program in central Haiti: A prospective observational cohort study. AIDS Res Ther. 2010;7(33):1-8. https://doi.org/10.1186/1742-6405-7-33 [ Links ]
12. Nelson K, Cunningham W, Andersen R, Harrison G, Gelberg L. Is food insufficiency associated with health status and health care utilization among adults with diabetes? J Gen Int Med. 2001;16(6):404-411. https://doi.org/10.1046/j.1525-1497.2001.016006404.x [ Links ]
13. Mshana GH, Wamoyi J, Busza J, Zaba B, Changalucha J, Kaluvya S, et al. Barriers to accessing antiretroviral therapy in Kisesa, Tanzania: A qualitative study of early rural referrals to the national program. AIDS Patient Care STDs. 2006;20(9):649-657. https://doi.org/10.1089/apc.2006.20.649 [ Links ]
14. Katz IT, Dietrich J, Tshabalala G, Essien T, Rough K, Wright AA, et al. Understanding treatment refusal among adults presenting for HIV-testing in Soweto, South Africa: A qualitative study. AIDS Behav. 2015;19(4):704-714. https://doi.org/10.1007/s10461-014-0920-y [ Links ]
15. Unge C, Johansson A, Zachariah R, Some D, Van Engelgem I, Ekstrom AM. Reasons for unsatisfactory acceptance of antiretroviral treatment in the urban Kibera slum, Kenya. AIDS Care. 2008;20(2):146-149. https://doi.org/10.1080/09540120701513677 [ Links ]
16. Weiser SD, Leiter K, Bangsberg DR, Butler LM, Percy-de Korte F, Hlanze Z, et al. Food insufficiency is associated with high-risk sexual behavior among women in Botswana and Swaziland. PLoS Med. 2007;4(10), e260, 10 pages. https://doi.org/10.1371/journal.pmed.0040260 [ Links ]
17. Tsai AC, Hung KJ, Weiser SD. Is food insecurity associated with HIV risk? Cross-sectional evidence from sexually active women in Brazil. PLoS Med. 2012;9(4), e1001203, 10 pages. https://doi.org/10.1371/journal.pmed.1001203 [ Links ]
18. Ramjee G, Daniels B. Women and HIV in sub-Saharan Africa. AIDS Res Ther. 2013;10(1), Art. #30, 9 pages. https://doi.org/10.1186/1742-6405-10-30 [ Links ]
19. Hoffman S, Exner TM, Lince-Deroche N, Leu CS, Phillip JL, Kelvin EA, et al. Immediate blood draw for CD4+ cell count is associated with linkage to care in Durban, South Africa: Findings from Pathways to Engagement in HIV Care. PLoS One. 2016;11(10), e0162085, 16 pages. https://doi.org/10.1371/journal.pone.0162085 [ Links ]
20. Miller CL, Bangsberg DR, Tuller DM, Senkungu J, Kawuma A, Frongillo EA, et al. Food insecurity and sexual risk in an HIV endemic community in Uganda. AIDS Behav. 2011;15(7):1512-1519. https://doi.org/10.1007/s10461-010-9693-0 [ Links ]
21. Pascoe SJ, Langhaug LF, Mavhu W, Hargreaves J, Jaffar S, Hayes R, et al. Poverty, food insufficiency and HIV infection and sexual behaviour among young rural Zimbabwean women. PLoS One. 2015;10(1), e0115290, 21 pages. https://doi.org/10.1371/journal.pone.0115290 [ Links ]
22. MacPherson P, Corbett EL, Makombe SD, Van Oosterhout JJ, Manda E, Choko AT, et al. Determinants and consequences of failure of linkage to antiretroviral therapy at primary care level in Blantyre, Malawi: A prospective cohort study. PLoS One. 2012;7(9), e44794, 9 pages. https://doi.org/10.1371/journal.pone.0044794 [ Links ]
23. Plazy M, Dray-Spira R, Orne-Gliemann J, Dabis F, Newell ML. Continuum in HIV care from entry to ART initiation in rural KwaZulu-Natal, South Africa. Trop Med Int Health. 2014;19(6):680-689. https://doi.org/10.1111/tmi.12301 [ Links ]
24. Shisana O, Rehle T, Simbayi LC, Zuma K, Jooste S, Zungu N, et al. South African National HIV Prevalence, Incidence and Behaviour Survey, 2012. Cape Town: HSRC Press; 2014. [ Links ]
25. UNAIDS. Global AIDS update 2016. Geneva: Joint United Nations Programme on HIV/AIDS (UNAIDS); 2016. [ Links ]
26. Ramjee G, Moonsamy S, Abbai NS, Wand H. Individual and population level impact of key HIV risk factors on HIV incidence rates in Durban, South Africa. PLoS One. 2016;11(4), e0153969,11 pages. https://doi.org/10.1371/journal.pone.0153969 [ Links ]
27. De Swardt C, Puoane T, Chopra M, Du Toit A. Urban poverty in Cape Town. Environ Urban. 2005;17(2):101-111. https://doi.org/10.1177/095624780501700208 [ Links ]
28. SANAC. National Strategic Plan on HIV, STIs and TB 2012-2016. Pretoria: South African National AIDS Council; 2011. [ Links ]
29. United Nations. Sustainable Development Goals: 17 goals to transform our world. New York: United Nations; 2015. Available from: http://www.un.org/sustainabledevelopment/sustainable-development-goals/ [ Links ]
30. Roberts B, wa Kivilu M, Davids YD. South African social attitudes: The 2nd report: Reflections on the Age of Hope. Cape Town: HSRC Press; 2010. [ Links ]
31. Naicker N, Kharsany AB, Werner L, Van Loggerenberg F, Mlisana K, Garrett N, et al. Risk factors for HIV acquisition in high risk women in a generalised epidemic setting. AIDS Behav. 2015;19(7):1305-1316. https://doi.org/10.1007/s10461-015-1002-5 [ Links ]
32. Chimbindi NZ, McGrath N, Herbst K, San Tint K, Newell ML. Socio-demographic determinants of condom use among sexually active young adults in rural KwaZulu-Natal, South Africa. Open AIDS J. 2010;4:88-95. https://doi.org/10.2174/1874613601004010088 [ Links ]
33. Case A, Hosegood V, Lund F. The reach and impact of Child Support Grants: evidence from KwaZulu-Natal. Develop South Afr. 2005;22(4):467-482. https://doi.org/10.1080/03768350500322925 [ Links ]
34. Moitse S, Hosegood V. Accessing grants: The never ending story. Children First. 2003;49:3-5. [ Links ]
 Correspondence:
Correspondence:
Makandwe Nyirenda
Email: makandwe.nyirenda@mrc.ac.za
Received: 14 Nov. 2017
Revised: 07 Feb. 2018
Accepted: 05 May 2018
Published: 11 Sep. 2018
FUNDING: US National Institute of Mental Health; South African Medical Research Council


{kind=link}
{kind=link}