










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Science
On-line version ISSN 1996-7489
Print version ISSN 0038-2353
S. Afr. j. sci. vol.112 n.11-12 Pretoria Nov./Dec. 2016
http://dx.doi.org/10.17159/sajs.2016/20160056
REVIEW ARTICLE
The phenomenon of skin lightening: Is it right to be light?
Lester M. DavidsI; Jennifer van WykII; Nonhlanhla P. KhumaloII; Nina G. JablonskiIII
IDepartment of Human Biology, University of Cape Town, Cape Town, South Africa
IIDivision of Dermatology, Groote Schuur Hospital, Cape Town, South Africa
IIIDepartment of Anthropology, Pennsylvania State University, State College, Pennsylvania, USA
ABSTRACT
Chemicals capable of lightening the skin - variously known as skin-bleaching, skin-lightening, depigmenting, skin-evening and skin-brightening agents - are among the most commonly used skin preparations in the world. Globally, Africa reportedly exhibits a high prevalence of skin lightener use. In this review, we provide both clinical and social perspectives on skin lightener use in Africa, with particular emphasis on South Africa. We narratively explore the timeline associated with skin lightener use in South Africa and attempt to interweave the social rhetoric of this specific paradigm. Despite the risks associated with exposing the skin to known constituents of these formulations, such as hydroquinone and mercury, chronic use continues. In spite of legislation banning hydroquinone and mercury in cosmetics in South Africa, these ingredients are present in widely available products. We recommend better implementation of policies and greater ethical responsibility of multinational cosmetic companies in addition to the initiation of a system of random product testing and penalties that could improve industry compliance.
SIGNIFICANCE:
• There is a high prevalence of skin lightener use in Africa.
• Despite legislation banning harmful compounds, these compounds are still used in skin lightening formulations.
• There is an urgent need to implement policies and recommendations for preventing the influx and illicit sale and use of untested skin lighteners.
Keywords: skin lighteners; Africa; colourism; exogenous ochronosis; hydroquinone
Introduction
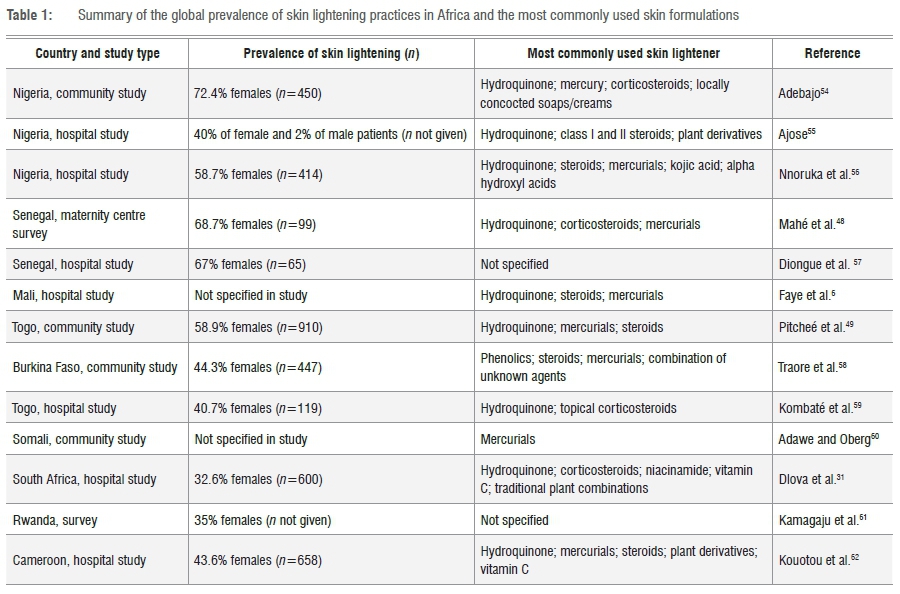
The global use of skin lighteners is not new. Although skin lighteners have been used for centuries, only in the last century has the production of these materials become commercialised and global.1 Currently, Africa has the highest number of studies reporting on the global prevalence of skin lightener use (see Table 1). Despite toxic systemic effects, application of topical skin lighteners remains popular throughout the African continent. The market for commercial skin lighteners has grown in the Caribbean, Asia and the Far East. The chief reasons for this growth remain varied, but, undoubtedly, are strongly linked to historical racism, the perceived social benefits of lighter skin and the marketing expertise of the multinational cosmetics companies now involved in their production.2-4 More recently, incentives for skin lightening use by pigmented people arise in part, and mostly subconsciously, from colourism - that is, the preference for lighter skin tone because of its association with positive social outcomes.1
Sub-Saharan Africa
The prevalence of skin lightener use across the African continent (Table 1) has become a common part of life in African communities. In the late 1960s, 60% of urban African women reported using skin lightener formulations, making these formulations the fourth most commonly used household product (after soap, tea and tinned milk).5 Further evidence of these practices is derived from local vernaculars - in Mali and Senegal, the terms 'caco' and 'xeesal' are used to describe the practice6, and in Ghana, the term 'nensoebenis' describes ochronosis (the hyperpigmentation and damage to the skin as a result of chronic skin lightener use)7. In South Africa, in various ethnic languages related to indigenous tribes, the practice is described as 'ukutsheyisa' (isiXhosa for 'to chase beauty') and 'ukucreamer' (isiZulu for 'applying creams on the skin'). Around Johannesburg, the word 'mashubaba' is used in urban township slang to describe ochronosis. The motivation driving the practice is often the desire to lighten one's skin because of a perceived notion of increased privileges, higher social standing, better employment and increased marital prospects associated with lighter skin. This perception, coupled with influential marketing strategies from transnational cosmetic houses using iconic celebrities, increases the allure for women primarily, but also increasingly, men.8,9 Unfortunately, the main fear is that the presence of these legally available products could potentially cloud the distinction of the consumer between products that are tested and those that are damaging and illegal. This distinction needs to be pertinently highlighted.9
Use of skin lightening agents and their biological consequences
A diverse range of compounds is currently used in skin lightener preparations. However, the 'big four' - mercury-containing compounds (known as mercurials), hydroquinone and its derivatives (monobenzyl ether and monomethyl ether), potent corticosteroids and retinoids - are still considered the primary sources of damage. The biological consequence of each of these is considered below.
Mercurials
Mercurials (mercury and its derivatives) are the oldest known skin lighteners.10 They act to lighten the skin by replacing the copper required for tyrosinase activity and antagonistically inhibiting melanin in melanocytes.11 Although banned by the US Food and Drug Administration in 1973 and by the European Union (EU) in 1976, mercurials continue to be produced and exported to countries in Africa and the Caribbean.1 Moreover, mercury poisoning through the use of skin lightener preparations continues to be reported from Africa12; Europe13,14; USA15,16; Australia17 and Hong Kong18.
Hydroquinone
Hydroquinone, chemically known as 1,4 dihydroxybenzene, is an effective skin lightener which acts by preventing the synthesis of melanin through competing with its natural substrate, the enzyme tyrosinase, in a reversible reaction.19-22 In addition, it inhibits both DNA and RNA synthesis in epidermal melanocytes22 and becomes toxic to melanosomes11. Banned by South Africa in 1980, followed by the EU and Japan in 2001, hydroquinone continues to be available in the USA in dermatologically based preparations1 and its use for treating conditions such as melasma, pregnancy-induced hyperpigmentation, lentigines and other skin depigmentary disorders such as vitiligo23 continues to raise opposition by dermatologists.
Chronic, unsupervised use of hydroquinone could result in a hyper-pigmented, skin-altering condition called exogenous ochronosis (Figure 1). Characterised by progressive asymptomatic hyperpig-mentation, the lower layers of the skin show signs of collagen and elastic fibre degeneration.
Corticosteroids
Most often used in combination with hydroquinone and/or mercurials in skin lightener preparations, corticosteroids are categorised according to their potencies from class I (most potent) to class VII (least potent).24 Clobetasol propionate, licensed in 1973, is a class I fluorinated corticosteroid (generally prescribed at a concentration of 0.05%) which causes vasoconstriction and immunosuppression and results in hypo-pigmentation or skin lightening.10,24 As clobetasol propionate is very stable and able to penetrate the epidermal and dermal skin layers, its inclusion in skin lightening preparations was immediate and its use was manifested in numerous African and Afro-Caribbean communities.25,26
Unfortunately, chronic use of this highly potent corticosteroid leads to severe consequences such as cutaneous atrophy, with clinical manifestations of skin thinning and fragility, telangiectasia and striae.24
Retinoids
Today, the vast majority of skin lightening agents include a form of retinoid. Topical retinoids include all trans-retinoic acid, 13-cis-retinoic acid (isotretinoin), retinol, retinaldehyde, tazarotene and adapalene.27 Well known for their anti-ageing effects28, retinoids function to lighten hyperpigmented skin by decreasing melanosome transfer from epidermal melanocytes, inhibiting both tyrosinase transcription and melanin synthesis29,30.
With respect to management of skin lightener use, it is - undoubtedly - the current undivided global opinion of most clinicians and scientists that the inclusion of inorganic and other forms of compounds within cosmetic formulations should be strictly prohibited.18 However, difficulties ensue with compliance and relate to each country's policies and the enforcement thereof. This situation reinforces the pertinent need for a global standardisation of cosmetic policies and recommendations.
South Africa and depigmenting agents
South Africa, in the context of its political overtones, has a distinctive history within the globalisation of skin lighteners.31 The period 19601970 saw a tremendous increase in the popularity of skin lightener use in South Africa with the market peaking in the 1970s.5 Whether this peak was because of aggressive marketing and intelligent advertisement strategies by emerging cosmetic companies or politically motivated cannot be quantified, but the broad appeal of these products continued to rely on the popular ideologies that linked lighter skin to power and beauty.32 An early dermatological study reported on a 6-year trial consisting of 840 volunteers who were drawn from various race groups with skins varying from very fair to very dark. The volunteers were subjected to open skin tests, 'normal usage' tests and standard 48-h closed-patch tests. In all, over 7000 skin test areas were examined. The results showed that concentrations of hydroquinone of 3% or less produced negligible adverse effects, irrespective of the base or the colour of the user's skin. This study stressed that any confusion of hydroquinone with the hazardous monobenzyl ether of hydroquinone (monobenzone) should be avoided.33 Another study34 conducted on 347 patients seen over a 6-month period at the Chris Hani Baragwanath Hospital in Johannesburg further reported on patients presenting with depigmented patches over their skins. The authors found that this effect was a result of the repeated use of an overnight 'depigmenting' cream containing hydroquinone at a concentration greater than 3%.34 By 1975, the South African government banned the inclusion of all forms of mercury in any skin formulations.
Also in 1975, the South African skin lightener cosmetic industry was estimated at ZAR12.8 million per annum (about USD1.6 million at the current exchange rate). Despite warnings from renowned dermatologists, skin lightening creams continued to be illicitly sold and used for 'facial improvement and the elevation of social standing'33. It was claimed at the time that hydroquinone (at a 3% concentration) remained the only substance to reasonably depigment darker skin.33,34 Findlay et al.35 quoted patients as saying that if, on application, a product 'stings or burns the skin' that it is 'working well'. This perception of patients has led to the continued, unregulated use of even stronger formulations with consequential skin damage - a condition called exogenous ochronosis (Figure 1).35 By 1979, there was a growing concern regarding the high occurrence of ochronosis cases and a study by Dogliotti and Leibowitz36 showed that 6% of 5463 patients seen over a 2-year period presented with skin damage related to the use of marketed cosmetic preparations. These products included greasy paraffin derivatives, bleaching creams, lanoline mixtures and surface moisturising agents.36 Individual or multiple products were applied in the hope of 'clearing undesirable patchy hyperpigmentation, curing pimples and changing a dark complexion to one which was bright, lovely and seductive'36. This statement may have implied the perception that black skin was the antithesis of these descriptions, highlighting to young, impressionable black South Africans the 'need' for ongoing use.
By 1980, the South African cosmetic market industry had swelled to an annual turnover of about ZAR25 million (~USD3.1 million), with the market described as 'phenomenal' and 'ripe for the picking'37. Findlay et al.35 further reported that evidence of ochronosis related to the chronic use of a skin lightener containing 8-15% hydroquinone. This cream was subsequently withdrawn from the market and replaced with the monobenzyl ether of hydroquinone known as monobenzone.38 These polyphenolics, traditionally used in the rubber and photographic trades39, work effectively as skin lighteners as they inhibit the enzyme (tyrosinase) primarily involved in producing melanin in the epidermis of human skin40. Unfortunately, chronic use leads to ochronosis35 (Figure 1).
Clinical reports35,37,41 increased in frequency and their description of the severity of the adverse effects of skin lighteners motivated the government to regulate the amount of hydroquinone in over-the-counter formulations to less than 2% by 198032. Despite this regulation, during the early 1980s no fewer than 58 brands of skin lighteners were still found to be available in pharmacies and supermarkets in the Johannesburg area, and patients in the area were presenting with severe ochronosis.42

In comparison with the late 1970s and testament to the need for a 'fairer skin', by 1986 in South Africa, the total revenue of skin lighteners was estimated at GBP30 million (about ZAR390 million).41 The consequence of this market was becoming more evident. A study reported the prevalence of ochronosis in black individuals attending two South African hospitals at 15% in male patients and 42% in female patients; the prevalence was 69% amongst users of skin lighteners.41 The authors also found an inverse relationship between ochronosis and level of education of the individual. It was noteworthy that even products containing 2% hydroquinone used with a sunscreen were reported to cause ochronosis.41,42
Owing in part to the Black Consciousness movement, laws emanating from the Us Federal Drug Administration and EU's Drug Administration RAPEX (Rapid Alert System for Non-Food Products ), as well as a significant change in the country's political profile, by 1990, South African products containing hydroquinone were completely banned.32 Moreover, South Africa became one of the first countries in the world to restrict cosmetic advertisements from claiming the ability to bleach, 'lighten' or 'whiten' skin.5 Despite this restriction, the skin lightener market did not experience the huge downturn expected. In contrast, there was an increase in use which could be explained by a massive rise in local, informal settlements and their own associated markets possibly further influenced by the opening of South African borders to neighbouring countries after 1994.
As the late 1990s approached, consumerism - the ability of advertisements and media to affect the purchasing of goods - became a major influential factor in the sale of skin lightening formulations. Coupled to consumerism, the influence of social media, mobile telephones with roaming applications (apps) and influential celebrity icons emanating from the West (Hollywood in the USA), the Far East (China and Japan) and Asia (Bollywood in India), accelerated skin lightener use beyond what could be globally imagined.43 In addition, market expansion of large, multinational cosmetic houses as well as the rapid expansion of start-up, entrepreneurial companies, fuelled the global expansion.9
Today, skin lightening cosmetics are widespread and new marketing campaigns describing the 'success' of those with fairer skin, have included products attractive to both young men and young women across Africa.31 However, not all people who use these products do so to lighten their complexion. In a recent South African study of 600 women of African and Indian ancestry, it was reported that 32.7% used skin lightening products, but the main reason cited was treatment of skin problems (66.7%), with skin lightening accounting for only 33.3% of use.44 This point emphasises the need to inform populations that early and prompt treatment of conditions such as acne vulgaris reduces the risk of scarring.
Policies and recommendations
Despite numerous countries in Africa making a concerted effort to stop the chronic use of skin lightening products through national bans of constituent compounds such as hydroquinone and mercury, there still remains an inconsistent level of regulation within the sector. With many people still engaging in this practice, discovering new means to curb the use of skin-bleaching products and prevent dangerous health consequences remains a pressing area of inquiry. The sustained use of these products is suggested to be primarily a consequence of classification of these products as cosmetic rather than pharmaceutical and a lack of regulation means there is no consistent requirement for ingredient labelling. Williams45 suggests that had skin lighteners been classified as drugs and not cosmetics, the product licence would have probably long been withdrawn. Moreover, many product labels do not list all the ingredients, and in some developing countries there is evidence of misbranding.45 Most African countries have regulatory organisations. In South Africa, the watchdog organisation is the Cosmetic, Toiletries and Fragrance Association (CTFA). This association, as in other African countries, controls the policies relating to labelling and regulation and should work closely with governmental sectors relating to importation and availability of products. Unfortunately, the current status quo seems to be a lack of enforcement of existing regulation - a topic that needs to be addressed at the governmental level. However change is evident, and examples include the governments of Nigeria, South Africa, Kenya, Zimbabwe and, more recently, the Ivory Coast, banning the import and sale of skin-bleaching products that contain mercury and hydroquinone.46 Unfortunately governments cannot address the issue through policy changes alone.46-49 Hall50 suggested that in order to initiate real change, destigmatisation of dark skin needs to be advocated, and subsequent studies acknowledging the realities of these motivations are needed. Others suggest that more pressure on corporations to change their concept of beauty may be influential in discouraging skin bleaching.51,52 The concept of beauty is a tentative and sensitive issue. For example, Eagle et al.53 posed the question of ethical responsibility of multinational cosmetic companies. They suggest that these multinational companies may be inadvertently (or indeed consciously) sustaining prejudices and stereotypes. Of particular concern is that these companies have the financial resources to reinforce the desirability of these products by using marketing techniques glamorising the use of their products.53
Conclusions
The use of illegal ingredients in skin lightener products continues to prevail throughout many African countries. A strong argument for safety exists to justify an interim ban (in all countries) on over-the-counter creams containing hydroquinone, pending long-term trials on the safety of these products. Moreover, the onus should be on manufacturers rather than consumers to establish such safety. Many countries in Africa and the African Diaspora, including Uganda, Kenya, South Africa and Gambia, have banned skin lightener products, while others - such as Ghana, Zambia, Jamaica and, most recently, Ivory Coast, have promoted public health education to dissuade people from using bleaching creams.9 Overall, Africa, and particularly South Africa, needs to continue research into the motivation for skin lightening. Given the inability of government bans to effectively prevent skin lightening, current studies should investigate other strategies aimed at improving industry compliance,8,49,52 such as random testing and penalties.
Acknowledgements
We thank Mrs Theresa M. Wilson for her assistance, proofreading and general comments on this manuscript.
Authors' contributions
L.M.D. and N.G.J. conceptualised the paper and researched the topic. All authors contributed towards the writing and editing of the manuscript.
References
1. Jablonski NG. Living color: The biological and social meaning of skin color. Berkeley, CA: University of California Press; 2012. [ Links ]
2. Glenn EN. Yearning for lightness: Transnational circuits in the marketing and consumption of skin lighteners. Gender Soc. 2008;22(3):281-302. http://dx.doi.org/10.1177/0891243208316089 [ Links ]
3. Glenn EN. Consuming lightness: Segmented markets and global capital in the skin-whitening trade. In: Glenn EN, editor. Shades of difference: Why skin color matters. Stanford, CA: Stanford University Press; 2009. p. 166-187. [ Links ]
4. Rondilla JL, Spickard P Is lighter better? Skin-tone discrimination among Asian Americans. Lanham, mD: Rowman and Littlefield Publishers Inc.; 2007. [ Links ]
5. Thomas LM. Skin lighteners, black consumers and Jewish entrepreneurs in South Africa. Hist Workshop J. 2012;73(1):259-283. http://dx.doi.org/10.1093/hwj/dbr017 [ Links ]
6. Faye O, Keita S, Diakité FS, Konaré HD, Ndiaye HT. Side effects of depigmenting products in Bamako, Mali. Int J Dermatol. 2005;44(S1):35-36. http://dx.doi.org/10.1111/j.1365-4632.2005.02809.x [ Links ]
7. Dadzie O, Petit A. Skin bleaching: Highlighting the misuse of cutaneous depigmenting agents. J Eur Acad Dermatol. 2009;23(7):741-750. http://dx.doi.org/10.1111/j.1468-3083.2009.03150.x [ Links ]
8. Hunter ML. Buying racial capital: Skin-bleaching and cosmetic surgery in a globalized world. J Pan Afr Stud. 2011;4(4):142-164. [ Links ]
9. Bird D, Caldwell H, DeFanti M. The quest for beauty: Asia's fascination with pale skin. In: Oglesby RA, LeBlanc HP III, Adams MG, editors. Global business perspectives. Beltsville, MD: International Academy of Business Disciplines; 2010. p. 26-32. [ Links ]
10. Olumide YM, Akinkugbe AO, Altraide D, Mohammed T, Ahamefule N, Ayanlowo S, et al. Complications of chronic use of skin lightening cosmetics. Int J Dermatol. 2008;47(4):344-353. http://dx.doi.org/10.1111/j.1365-4632.2008.02719.x [ Links ]
11. Denton CR, Lerner AB, Fitzpatrick TB. Inhibition of melanin formation by chemical agents. J Invest Dermatol. 1952;18(2):119-135. http://dx.doi.org/10.1038/jid.1952.16 [ Links ]
12. Saffer D, Tayob H, Bill PL, Baily P. Continued marketing of skin-lightening preparations containing mercury. S Afr Med J. 1976;50(39):1499. [ Links ]
13. Summa JD. Chronic mercury poisoning from cosmetic creams. Munch Med Wochenschr. 1975;117(26):1121-1124. [ Links ]
14. Otto M, Ahlemeyer C, Tasche H, Von Mühlendahl KE. Endemic mercury burden caused by a bleaching ointment in Balken refugees. Gesundheitswesen. 1994;56(12):686-689. [ Links ]
15. McRill C, Boyer LV, Flood TJ, Ortega L. Mercury toxicity due to use of a cosmetic cream. J Occup Environ Med. 2000;42(1):4. http://dx.doi.org/10.1097/00043764-200001000-00004 [ Links ]
16. Weldon MM, Smolinski MS, Maroufi A, et al. Mercury poisoning associated with a Mexican beauty cream. Western J Med. 2000;173(1):15-18. http://dx.doi.org/10.1136/ewjm.173.1.15 [ Links ]
17. Dyall-Smith DJ, Scurry JP. Mercury pigmentation and high mercury levels from the use of a cosmetic cream. Med J Aust. 1990;153(7):409-410, 414-415. [ Links ]
18. Tang HL, Chu HK, Mak YF, Lee W, Cheuk A, Yim KF, et al. Minimal change disease following exposure to mercury-containing skin lightening cream. Hong Kong Med J. 2006;12(4):316-318. [ Links ]
19. Chan TYK. Inorganic mercury poisoning associated with skin-lightening cosmetic products. Clin Toxicol. 2011;49(10):886-891. http://dx.doi.org/10.3109/15563650.2011.626425 [ Links ]
20. Gupta AK, Gover MD, Nouri K, Taylor S. The treatment of melasma: A review of clinical trials. J Am Acad Dermatol. 2006;55(6):1048-1065. http://dx.doi.org/10.1016/j.jaad.2006.02.009 [ Links ]
21. Parvez S, Kang M, Chung H-S, Cho C, Hong M-C, Shin M-K, et al. Survey and mechanism of skin depigmenting and lightening agents. Phytother Res. 2006;20(11):921-934. http://dx.doi.org/10.1002/ptr.1954 [ Links ]
22. Parvez S, Kang M, Chung H-S, Bae H. Naturally occurring tyrosinase inhibitors: Mechanism and applications in skin health, cosmetics and agriculture industries. Phytothery Res. 2007;21(9):805-816. http://dx.doi.org/10.1002/ptr.2184 [ Links ]
23. Jimbow K. Vitiligo: Therapeutic advances. Dermatol Clin. 1998;16(2):399- 407. http://dx.doi.org/10.1016/S0733-8635(05)70021-8 [ Links ]
24. Pels R, Sterry W, Lademann J. Clobetasol propionate - Where, when, why? Drugs Today. 2008;44(7):547-557. http://dx.doi.org/10.1358/dot.2008.44.7.1122221 [ Links ]
25. Olumide YM, Elesha SO. Hydroquinone induced exogenous ochronosis. Niger Med Pract. 1986;11:103-106. [ Links ]
26. Keane FM, Munn SE, Taylor NF, Du Vivier AWP. Unregulated use of clobetasol propionate. Brit J Dermatol. 2001;144(5):1095-1096. http://dx.doi.org/10.1046/j.1365-2133.2001.04213.x [ Links ]
27. Sorg O, Kasraee B, Salomon D, et al. The potential depigmenting activity of retinaldehyde. Dermatology. 2013;227(3):231-237. http://dx.doi.org/10.1159/000354294 [ Links ]
28. Ortonne J-P Marks R. Photodamaged skin: Clinical signs, causes and management. London: Martin Dunitz Ltd.; 1999. [ Links ]
29. Ortonne J-P Retinoid therapy of pigmentary disorders. Dermatol Ther. 2006;19(5):280-288. http://dx.doi.org/10.1111/j.1529-8019.2006.00085.x [ Links ]
30. Roméro C, Aberdam E, Larnier C, Ortonne JP. Retinoic acid as modulator of UVB-induced melanocyte differentiation. Involvement of the melanogenic enzymes expression. J Cell Sci. 1994;107(4):1095-1103. [ Links ]
31. Dlova N, Hamed SH, Tsoka-Gwegweni J, Grobler A, Hift R. Women's perceptions of the benefits and risks of skin-lightening creams in two South African communities. J Cosmet Dermatol. 2014;13(3):236-241. http://dx.doi.org/10.1111/jocd.12104 [ Links ]
32. Thomas LM. Skin lighteners in South Africa: Transnational entanglements and technologies of the self. In: Glenn EN, editor. Shades of difference: Why skin color matters. Stanford, CA: Stanford University Press; 2009. p. 188-210. [ Links ]
33. Bentley-Phillips B, Bayles MAH. Cutaneous reactions to topical application of hydroquinone. Results of a 6-year investigation. S Afr Med J. 1975;49(34):1391-1395. [ Links ]
34. Dogliotti M. Survey of skin disorders in the urban black population of South Africa. Brit J Dermatol. 1975;93(3):259-270. http://dx.doi.org/10.1111/j.1365-2133.1975.tb06491.x [ Links ]
35. Findlay GH, Morrison J, Simson I. Exogenous ochronosis and pigmented colloid milium from hydroquinone bleaching creams. Brit J Dermatol. 1975;93(6):613-622. http://dx.doi.org/10.1111/j.1365-2133.1975.tb05110.x [ Links ]
36. Dogliotti M, Leibowitz M. Granulomatous ochronosis: A cosmetic-induced skin disorder in blacks. S Afr Med J. 1979;56(19):757-760. [ Links ]
37. Findlay G, De Beer H. Chronic hydroquinone poisoning of the skin from skin-lightening cosmetics. S Afr Med J. 1980;57:187-190. [ Links ]
38. Westerhof W, Kooyers T. Hydroquinone and its analogues in dermatology - A potential health risk. J Cosmet Dermatol. 2005;4(2):55-59. http://dx.doi.org/10.1111/j.1473-2165.2005.40202.x [ Links ]
39. Anderson F, Kessler J. Quinone continuous recycle process for electrolytic conversion of benzene to quinone. US Patent US3758392 A; 1973. [ Links ]
40. Parvez S, Kang M, Chung HS, Bae H. Naturally occurring tyrosinase inhibitors: Mechanism and applications in skin health, cosmetics and agriculture industries. Phytother Res. 2007;21(9):805-816. http://dx.doi.org/10.1002/ptr.2184 [ Links ]
41. Hardwick N, Van Gelder LW, Van der Merwe CA, Van der Merwe MP. Exogenous ochronosis: An epidemiological study. Brit J Dermatol. 1989;120(2):229-238. http://dx.doi.org/10.1111/j.1365-2133.1989.tb07787.x [ Links ]
42. Phillips JI, Isaacson C, Carman H. Ochronosis in black South Africans who used skin lighteners. Am J Dermatopath. 1986;8(1):14-21. http://dx.doi.org/10.1097/00000372-198602000-00003 [ Links ]
43. Hunter ML. "If you're light you're alright": Light skin color as social capital for women of color. Gender Soc. 2002;16(2):175-193. http://dx.doi.org/10.1177/08912430222104895 [ Links ]
44. Dlova NC, Hamed SH, Tsoka-Gwegweni J, Grobler A. Skin lightening practices: An epidemiological study of South African women of African and Indian ancestries. Br J Dermatol. 2015;173(Suppl 2):2-9. http://dx.doi.org/10.1111/bjd.13556 [ Links ]
45. Williams H. Skin lightening creams containing hydroquinone: A case for a temporary ban. Brit Med J. 1992;305:903-904. http://dx.doi.org/10.1136/bmj.305.6859.903 [ Links ]
46. Olumide YM. Use of skin lightening creams. Brit Med J. 2010;341:345-346. http://dx.doi.org/10.1136/bmj.c6102 [ Links ]
47. Lewis KM, Robkin N, Gaska K, Njoki LC. Investigating motivations for women's skin bleaching in Tanzania. Psychol Women Quart. 2011;35(1):29-37. http://dx.doi.org/10.1177/0361684310392356 [ Links ]
48. Mahé A, Perret J, Ly F, Fall F, Rault J, Dumont A. The cosmetic use of skin-lightening products during pregnancy in Dakar, Senegal: A common and potentially hazardous practice. T Roy Soc Trop Med H. 2007;101(2):183-187. http://dx.doi.org/10.1016/j.trstmh.2006.06.007 [ Links ]
49. Pitché P, Kombaté K, Tchangai-Walla K. Cosmetic use of skin-bleaching products and associated complications. Int J Dermatol. 2005;44(s1):39-10. http://dx.doi.org/10.1111/j.1365-4632.2005.02811.x [ Links ]
50. Hall RE. The bleaching syndrome in the context of somatic norm image among women of color: A qualitative analysis of skin color. Eur J Soc Sci. 2010;17(2):180-185. [ Links ]
51. Lewis KM, Gaska K, Robkin N, Martin A, Andrews E, Williams J. The need for interventions to prevent skin bleaching: A look at Tanzania. J Black Stud. 2012;43(7):787-805. http://dx.doi.org/10.1177/0021934712446701 [ Links ]
52. Shimo A. The quest for a lighter shade of pale. Maclean's. 2008 November 14;121(46):150-152. [ Links ]
53. Eagle L, Dahl S, Low DR. Ethical issues in the marketing of skin lightening products. In: ANZMAC 2014 Proceedings; 2014 December 01-03; Brisbane, Australia. Brisbane: ANZMAC; 2014. p. 75-81. Available from: http://www.anzmac.org/_files/1423706830anzmac%202014%20proceedings.compressed.pdf [ Links ]
54. Adebajo SB. An epidemiological survey of the use of cosmetic skin lightening cosmetics among traders in Lagos, Nigeria. W Afr J Med. 2002;21(1):51-55. [ Links ]
55. Ajose FOA. Consequences of skin bleaching in Nigerian men and women. Int J Dermatol. 2005;44(S1):41-43. http://dx.doi.org/10.1111/j.1365-4632.2005.02812.x [ Links ]
56. Nnoruka E, Okoye O. Topical steroid abuse: Its use as a depigmenting agent. J Natl Med Assoc. 2006;98(6):934. [ Links ]
57. Diongue M, Ndiaye P, Douzima P-M, Seck M, Seck I, Faye A, et al. Economic impact of skin-lightening products on household income in sub-Saharan Africa: The case of Senegal. Med Sante Trop. 2013;23(3):308-312. [ Links ]
58. Traore A, Kadeba JC, Niamba P, Barro F, Ouedraogo L. Use of cutaneous depigmenting products by women in two towns in Burkina Faso: Epidemiologic data, motivations, products and side effects. Int J Dermatol. 2005;44(s1):30-32. http://dx.doi.org/10.1111/j.1365-4632.2005.02807.x [ Links ]
59. Kombaté K, Mouhari-Toure A, Saka B, Akakpo AS, Maboudou A, Pitché P, et al. Acne and skin bleaching in Lome, Togo. Int J Dermatol. 2012;51(s1):27-29. http://dx.doi.org/10.1111/j.1365-4632.2012.05560.x [ Links ]
60. Adawe A, Oberg C. Skin-lightening practices and mercury exposure in the Somali community. Minn Med. 2013;96(7):48-49. [ Links ]
61. Kamagaju L, Morandini R, Gahongayire F, Stévigny C, Ghanem G, Pirotte G, et al. Survey on skin-lightening practices and cosmetics in Kigali, Rwanda. Int J Dermatol. 2016;55(1):45-51. http://dx.doi.org/10.1111/ijd.12833 [ Links ]
62. Kouotou E, Bissek A, Nouind C, Defo D, Sieleunou I, Ndam E, editors. Dépigmentation volontaire: Pratiques et dermatoses associées chez les commergantes de Yaoundé (Cameroun) [The practice of skin bleaching and associated skin diseases among female traders in Yaounde (Cameroon)]. Ann Dermatol Venereol. 2015;142(6-7):443-l45. French. http://dx.doi.org/10.1016/j.annder.2015.02.023 [ Links ]
 Correspondence:
Correspondence:
Lester Davids
Lester.davids@uct.ac.za
Received: 17 Feb. 2016
Revised: 30 June 2016
Accepted: 01 July 2016
FUNDING: William J. Fulbright Foundation (USA)


{kind=link}
{kind=link}