










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Science
versión On-line ISSN 1996-7489
versión impresa ISSN 0038-2353
S. Afr. j. sci. vol.110 no.11-12 Pretoria nov./dic. 2014
http://dx.doi.org/10.1590/sajs.2014/a0089
COMMENTARY
http://dx.doi.org/10.1590/sajs.2014/a0089
A symbiotic glance at the complexities of signature microbiomic interventions: infusing balance
Pradeep Kumar; Yahya E. Choonara; Viness Pillay
Wits Advanced Drug Delivery Platform Research Unit, Department of Pharmacy and Pharmacology, School of Therapeutic Sciences, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
Keywords: microbiome; colorectal cancer; inflammatory bowel disease; obesity; skin microbiome; vaginal microbiome
We're not individuals, we're colonies of creatures.
Bruce Birren1, Co-director: Genome Sequencing and Analysis Program
The Common Fund's National Institutes of Health Human Microbiome Project launched in 2007 is the first major genomics-based effort to reveal the influence of human microbiota, or resident microorganisms, on the health and disease status of humans. The first phase of the Human Microbiome Project (FY2007-2012) focused on characterisation of the composition and diversity and evaluation of the metabolic potential of microbiota that inhabit five major mucosal surfaces of humans: the oral cavity, gastrointestinal tract, nasal passage, skin and urogenital tract. The second and current phase of the Human Microbiome Project (FY2013-2015) is dedicated to data integration of the microbe-host biological properties extracted from cohort studies of microbiome-associated diseases.2
The Human Microbiome Project has provided a few major breakthroughs in understanding the complexity and diversity of human microbiota and their role in human health and disease. At present it is estimated that humans encompass approximately 20 million genes that encode the entire microbiota. In addition, the microbiota in humans contributes immensely toward the micro-xenobiotic and non-xenobiotic interventions inherent to microbiome-associated diseases. However, there are several issues that require thorough consideration before the scientific community can decide on the therapeutic potential of targeting microbiota. This commentary provides a detailed incursion into the complicated inter-microbiome associations and interventions that are related to the five most researched microbiota in humans: (1) the role of the butyrate-producing microbiome in colorectal cancer therapeutics, (2) the protective/defensive microbiome related to inflammatory bowel disease, (3) the risk associated with probiotic delivery in obesity, (4) the antimicrobial-based microbiome disproportion leading to/arising from skin diseases and (5) the maintenance of microbiome loads and confinement to the vaginal mucosa.
Microbiomic intervention in colorectal cancer therapy
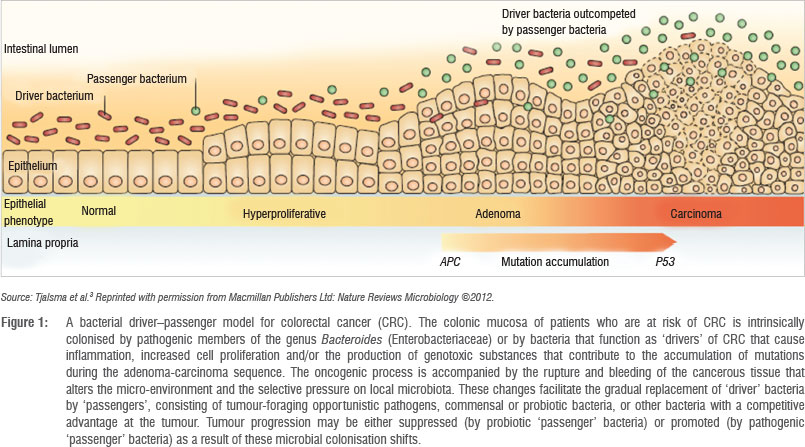
Muco-adherent pro-inflammatory microbes have been associated with the prevalence of colorectal cancer (CRC).3 These microbes are carcinogenic and influence the host's metabolism and function via signalling pathways and genotoxicity and by inciting immune responses.3 The colonic microbiome in CRC functions via two specific mechanisms - muco-adhesion and muco-inflammation. The muco-adhesion mechanism can be disrupted by surgical procedures and the prophylactic administration of antibiotics while the muco-inflammatory mechanism may be reduced by the regular use of non-steroidal anti-inflammatory drugs (NSAIDs).4 The prophylactic administration of antibiotics also has a negative effect on the beneficial commensal microbiota of the gut. Although controversial, the involvement of short-chain fatty acids such as butyrates has been proposed because they act via cell-cycle arrest that results in increased apoptosis of carcinogenic cells. Therefore, the introduction and preservation of the butyrate-producing microbiome can intervene in CRC therapy.5 Furthermore, it has been suggested that carcinogenic (specific to CRC) microbiota have inflammatory niches and hence are further influenced by introducing an anti-inflammatory commensal bacterium that is capable of blocking NF-kB expression and IL-8 secretion.6 Certain probiotics produce antibacterial peptides that are capable of protecting the host from pathogenic commensals and can significantly reduce the occurrence and recurrence of CRC in conjugation with a probiotic that is an adhesion competitor (Figure 1). In conclusion, CRC therapy can be effectively intervened by administering (1) antibiotics that are selective toward Enterococcus, Streptococcus and Fusobacterium species, (2) NSAIDs and (3) anti-inflammatory and butyrate-producing probiotics.
Inflammatory bowel disease and the microbial imbalance
Inflammatory bowel disease (IBD) is associated with an imbalance (preferentially known as dysbiosis) between the aggressive and protective microbiome in the gut. This imbalance is mainly an increase in Bacteroides and a decrease in Bifidobacterium and Lactobacillus species.7-11 The latter species are prescribed as probiotics in the treatment of IBD and their administration may help in correcting the imbalance. However, the efficacy of these probiotics in an already compromised inflammatory environment is doubtful and an immediate reduction of the aggressive species is required to reverse the imbalance. An interventional strategy involving the administration of a purified form of polysaccharide A (a molecule from Bacteroides fragilis) was reported by Mazmanian and co-workers8, wherein it was proposed that polysaccharide A can suppress the pro-inflammatory responses in IBD.8 However, in a recent study, Hueber and co-workers9 stated that suppression of such pro-inflammatory responses attained no benefit in severe inflammatory Crohn's disease even after administering highly potent therapeutic agents such as secukinumab. Therefore, broad-spectrum antibiotics such as a combination of ciprofloxacin and metronidazole are still the drugs of choice as they are capable of treating IBD complications such as abscesses, inflammatory phlegmon, fistulae, fissures, bacterial overgrowth secondary to strictures, prophylactic postoperative infections and secondary infections. Furthermore, antimicrobial peptides such as α-defensin 1-4, α-defensin 5, β-defensin 1-3, lysozyme, sPLA2, Reg3A/HIP/PAP and lipocalin 2 are significantly effective against Gram-positive and Gram-negative pathogenic microbes. They have also shown significant activity against lectins and selective bacteria. These antimicrobial peptides can further enhance the composition of the colonising defensive microbiota in the gut.10,11
Microbiota associated with obesity -The probiotic risk
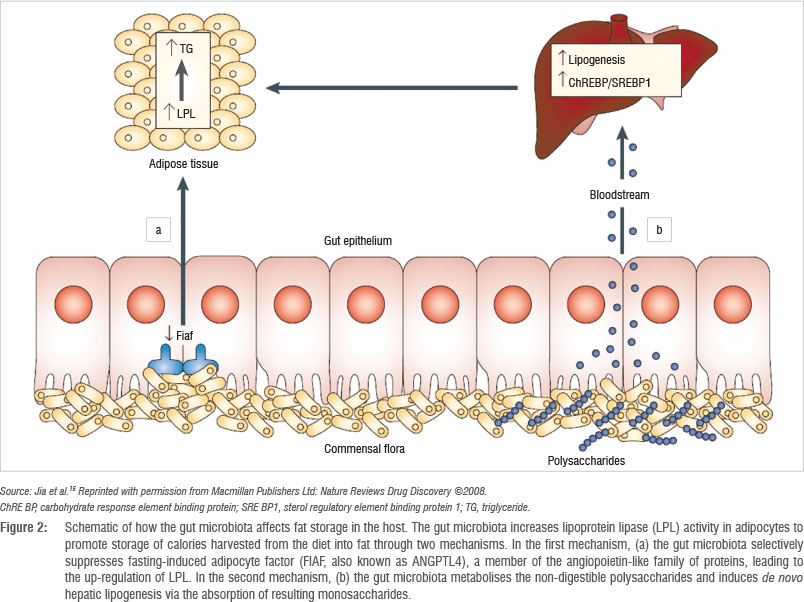
Although controversial, obesity in humans has been microbiotically related to the changes in the ratio of Gram-positive Firmicutes and Gram-negative Bacteroidetes. However, these studies were performed in subjects on restricted diets and hence their findings can be debated.12,13 In studies with no dietary restrictions, it has been reported that Bacteroidetes significantly differed in obese patients, confirming the role of diet in the prevalence of microbiota and obesity.14 It should be noted that Firmicutes such as Lactobacillus spp., Bifidobacterium spp. and Enterococcus spp. form the majority of functional food and therapeutic adjuvants added to farm products as probiotics or prebiotics (Figure 2).15 Furthermore, the concentration of live Lactobacillus spp. and Bifidobacterium spp. in these functional foods is in the range of that used in animals as growth promotors. Surprisingly, the level of these adjuvants - especially Lactobacillus acidophilus - in probiotic-containing dairy foods was enough to cause weight gain in experimental piglets. The same is applicable to the weight gain in children on prebiotic supplements which contain Lactobacillus rhamnosus - independent of disease intervention.16 These findings lead to the conclusion that controlling and maintaining the relative abundance of these two bacterial species - along with the less researched but dominant archaeon Methanobrevibacter smithii - may provide future researchers with drug targets for the treatment and prevention of obesity and related disorders.17
Therapeutic intervention of the skin microbiome
The skin microbiome, constituting mainly Actinobacteria and Proteo-bacteria, is distributed throughout the human body and differs considerably with respect to external factors such as type of occupation, hygiene and climate as well as intrinsic factors such as skin temperature, humidity and degree of glandular secretions. For example, sebaceous glands are inhabited by Propionbacterineae species, moist areas of the skin are colonised by Staphylococcus and Corynebacterium spp., while the drier regions are inhabited with Proteobacteria.18 Unique to the skin microbiome is the relative inverse abundance correlation among various microbial species such as (1) the bacterial deficiency of Propionibacterium acnes in the presence of staphylococcal species and (2) the relative scarcity of Staphylococcus aureus as a result of the abundance of Staphylococcus epidermidis. The staphylococcal species and S. epidermidis can be useful probiotics against P acnes and S. aureus, respectively, while also providing prognostic information related to these slow dwelling infections.19 However, this entirely symbiotic interaction has been adversely affected by the overuse of antibiotics, leading to the generation of the highly pathogenic strain of methicillin-resistant S. aureus that has acquired genes which are further resistant to the antimicrobial peptide released from S. epidermidis.20 21 The skin microbiome is responsible for various dermatological disorders such as atopic dermatitis (S. aureus) and psoriasis (S. pyogenes) caused by bacterial infection and seborrheic dermatitis and tinea versicolor caused by fungal infection.22 Although antimicrobial interventions have shown to be an effective approach for the treatment and prevention of these skin disorders, the recovery of the symbiotic microbiome may take several weeks and some populations of the microbial community, such as S. epidermidis, may never recover to their original concentration.
Vaginal microbiome and related lactobacilli abundance and transport
The lactic acid producing microbiome in healthy women consists of one of the four species of Lactobacillus, namely L. crispatus, L. iners, L. gasseri or L. jensenii.23 The lactic acid produced provides various benefits such as acidification of the vaginal milieu (hence preventing growth of pathogenic microbes) and modulation of the host vaginal membrane and biochemical environment.23 A change in this protecting mechanism may lead to the prevalence of pathogenic anaerobic and facultative bacteria such as Gardnerella vaginalis, leading to the well-known condition bacterial vaginosis (BV).24,25 Another important opportunistic infection is vaginal candidiasis in which the vaginal epithelium is asymptomatically colonised with Candida. These bacterial species are also responsible for preterm birth as a result of the passage of bacteria to the upper genital tract, for the infrequent problem known as vulvovaginal pain, and for increased susceptibility to HIV and other sexually acquired infections. Therefore, therapeutic opportunities related to the vaginal microbiome should be focused on maintaining the Lactobacillus load in the vagina as well as preventing its passage to the upper regions of the reproductive tract.26 Antimicrobials can be an effective intervention for containing the aggressive vaginal microbiome. However, they should be avoided in pregnant women. Although the administration of metronidazole for BV results in the back shift of microbial profiles, this back shift results in replenishment of L. iners in abundance but fails to recover the L. crispatus levels.27,28 The use of oestrogen replacement therapy has also shown potential for treating urogenital infections caused by the increased colonisation of the upper genital tract by Lactobacillus species.29 Readers are encouraged to refer to a recent review by MacPhee and co-workers30 in which they discuss the possibility and efficacy of using topically applied vaginal probiotics under regulations characterising their use as drugs or intravaginal devices.
Impact of the Human Microbiome Project in South Africa
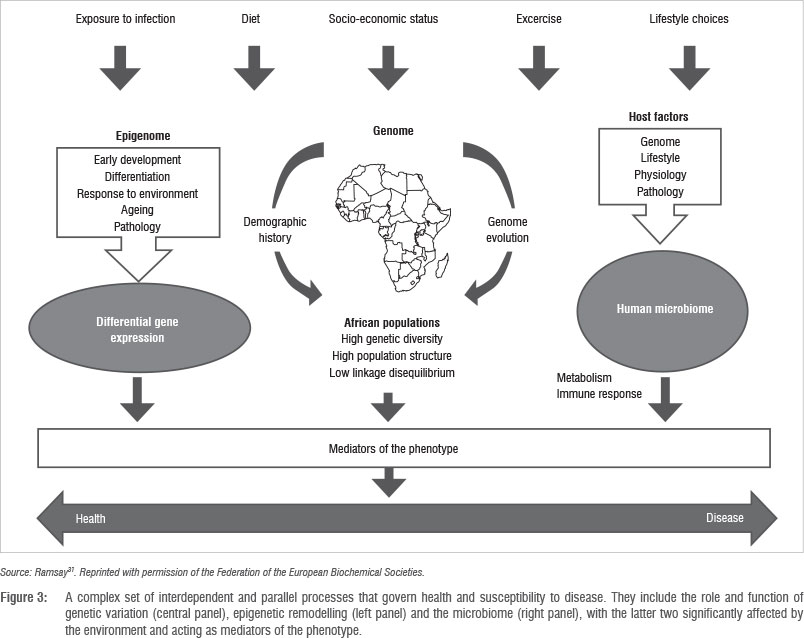
The human microbiome forms one of four pillars that has a health impact in Africa; the other three being genetics, socio-economics and environmental factors.31 Figure 3 effectively displays the role and importance of the human microbiome in delineating the health-and-disease model in African populations. However, South Africa (and in fact the African continent) has been neglected and hugely under-represented in the Human Genome Project and its status in the Human Microbiome Project is not any different.
The role of human microbiota discussed earlier in this commentary covers all three major physiological areas of microbiome research - the surface of the skin, the gastrointestinal tract and the urogenital tract. In addition, one lifestyle disorder (obesity) and an infectious factor (the vaginal microbiome) affecting metabolism and immunity, respectively, are also discussed. This commentary explains the importance of microbiome research to understand specific physiological phenomena and disease susceptibility. A better understanding of (1) the lifetime stability of human microbiota, (2) the similarity and diversity of microbiota among individuals, their families, the community and the entire population, (3) the possibility of founding a universal microbiota database and, finally, (4) the microbiomal adaptation and mutation with changing lifestyles and environmental factors, can provide important insights into novel therapeutic targets and diagnostic biomarkers for various illnesses.31
According to a recent study, covering 188 countries over a period of 33 years (1980-2013), published in the Lancet (29 May 20l4), South Africa has the highest overweight and obesity rate in sub-Saharan Africa with 40% of men and 69% of women overweight or obese.32 The major reasons for obesity in South Africa are (1) easy access to a low-cost calorie-rich diet, (2) sedentary lifestyles because of fast-growing urbanisation and (3) the social stigma associating 'being-fat' with health and wealth and 'being-thin' with HlV infection. However, the role of the gut microbiome in obesity cannot be overruled as the obesity-associated gut microbiome, e.g. Firmicutes, is significantly more capable of extracting energy from food than the microbiota of lean individuals and hence may indirectly increase the risk of concomitant cardiometabolic diseases such as diabetes and hypertension. Therefore, a complete array of experimental and analytical tools need to be generated nationally and regionally via a thorough gut microbiome investigation.33
Another microbiomic factor impacting the South African health system is the vaginal microbiome imbalance. In a recent study published in PLOS Medicine, it was reported that BV, due to the prevalence of pathogenic anaerobic and facultative bacteria such as Gardnerella vaginalis, is associated with a threefold increased risk of female-to-male HIV-1 transmission. High BV prevalence in women has been associated with lower socio-economic status (hygiene) and in South Africa may further be associated with race (black women have a higher incidence of BV because of lower dominance of lactobacilli), sexual practices (women with multiple sex partners have a higher incidence), trichomoniasis, HIV-1 infection (leading to BV and vice versa), recent antibiotic use, and the absence of lactic acid and peroxide producing lactobacilli. The introduction of antibiotics against G. vaginalis and Atopobium vaginae and/or the use of lactobacilli probiotics as an adjuvant/alternative to antibiotic intervention may subdue the impact of BV on HIV-1 transmission. However, maintaining a lactobacilli-predominant flora in the vagina appears longer lasting and more effective because of the ability of G. vaginalis and A. vaginae to form biofilms recalcitrant to antibiotic treatment.3435 As stated by Cohen and co-workers34:
A lactobacillus-predominant vaginal flora might not only reduce the risk of HIV-1 acquisition in women, but also HIV-1 transmission to male partners, and points to the potential benefits of using the human microbiota to prevent disease.
South Africa is struggling with a food allergy epidemic among black children. This expression or suppression of food allergy is attributed to the differences in intestinal microbial populations between allergic and non-allergic infants caused by an alarming increase in the rate of caesarean sections, socio-economic status and changing diet, as well as the frequent use of antimicrobials. The mutation and modification of the maternal intestinal microbial milieu may also affect the child's microflora. In addition, environmental factors such as exposure to soil/dust in close vicinity to migrant populations may lead to hand-to-mouth transmission of harmful microbiota in children. Although this theory requires further experimentation and explanation, the role of the microbiome in food allergy in black South African children cannot be ignored.36
Various factors such as genetic polymorphism, pathogenic infection, poor nutrition and hygiene can also significantly affect the efficiency and efficacy of oral vaccines against pathogenic gut microbiota. In a typical example, the altered gut microbial composition in the case of IBD leads to the disruption of mucosal integrity and function, which in turn compromises mucosal immunity. This significantly altered gut physiology may directly or indirectly affect vaccine efficacy and obstruct the development of effective and durable mucosal immune responses.37
The human microbiome will continue to alter with age, health status, sickness frequency and type, and hormonal variations, as well as under changing physico-chemical, environmental and social factors.38 The above-mentioned specialised conditions represent merely the tip of the 'microbiomic iceberg' impacting health in South Africa. Since inception of the USD100 million Human Microbiome Project in 2007, only a handful of studies have covered the South African microbiome paradigm, with the majority of studies conducted overseas. We urge the South African biomedical research community to join hands to unfold the African microbiome landscape which, given the disease prevalence in Africa, might prove to be the most diverse, challenging and disease predisposing microbiome known to humankind.
Concluding comments
The microbiome-associated diseases discussed in this commentary can act (in future) as a guidance point for other related or unrelated conditions with emphasis on the fact that the microbial supplements (probiotics), facilitators (prebiotics), terminators (antibiotics) and bacteriocins should be linked to form an effective synergistic therapeutic paradigm. The microbiomic interconnection between various continuous systems such as the gastrointestinal and respiratory systems should be considered and studied for their co-therapeutic potential. Furthermore, the very confusing and complicated scenarios arising from probiosis and dysbiosis as well as from probiotics and synbiotics need thorough laboratory and clinical investigation in order to complete the phenotypic profiling of related microbiome-associated diseases. From a South African, sub-Saharan and African perspective, the role of xenobiotic interventions via prebiotics, probiotics and synbiotics in special cases such as immunocompromised patients, neonates and children must also be carefully studied by taking their safety considerations into account.
Acknowledgements
We thank the National Research Foundation of South Africa for support.
References
1. The Broad Institute. Human Microbiome Project [homepage on the Internet]. [ Links ] No date [cited 2014 Nov 10]. Available from: http://www.broadinstitute.org/scientific-community/science/projects/microbiome-projects/hmp/human-microbiome-project
2. National Institutes of Health. Human Microbiome Project: Overview [homepage on the Internet]. [ Links ] No date [updated 2014 Sep 24; cited 2014 Nov 10]. Available from: http://commonfund.nih.gov/hmp/overview
3. Tjalsma H, Boleij A, Marchesi JR, Dutilh BE. A bacterial driver-passenger model for colorectal cancer: Beyond the usual suspects. Nat Rev Microbiol. 2012;10:575-582. http://dx.doi.org/10.1038/nrmicro2819 [ Links ]
4. Makivuokko H, Tiihonen K, Tynkkynen S, Paulin L, Rautonen N. The effect of age and non-steroidal anti-inflammatory drugs on human intestinal microbiota composition. Br J Nutr. 2009;103:227-234. http://dx.doi.org/10.1017/S0007114509991553 [ Links ]
5. Zackular JP Baxter NT, Iverson KD, Sadler WD, Petrosino JF, Chen GY et al. The gut microbiome modulates colon tumorigenesis. mBio. 2013;4(6):e00692-13. [ Links ]
6. Sokol H, Pigneur B, Watterlot L, Lakhdari O, Bermudez-Humaran LG, Gratadoux JJ, et al. Faecalibacterium prausnitzii is an anti-inflammatory commensal bacterium identified by gut microbiota analysis of Crohn disease patients. Proc Natl Acad Sci USA. 2008;105:16731-16736. http://dx.doi.org/10.1073/pnas.0804812105 [ Links ]
7. Tamboli CP Neut C, Desreumaux P Colombel JF. Dysbiosis in inflammatory bowel disease. Gut. 2004;53:1-4. http://dx.doi.org/10.1136/gut.53.1.1 [ Links ]
8. Mazmanian SK, Round JL, Kasper DL. A microbial symbiosis factor prevents intestinal inflammatory disease. Nature. 2008;453:620-625. http://dx.doi.org/10.1038/nature07008 [ Links ]
9. Hueber W, Sands BE, Lewitzky S, Vandemeulebroecke M, Reinisch W, Higgins PDR, et al. Secukinumab, a human anti-IL-17A monoclonal antibody, for moderate to severe Crohn's disease: Unexpected results of a randomised, double-blind placebo-controlled trial. Gut. 2012;61:1693-1700. http://dx.doi.org/10.1136/gutjnl-2011-301668 [ Links ]
10. Bevins CL. Antimicrobial peptides in inflammatory bowel disease. In: Baumgart DC, editor. Crohn's disease and ulcerative colitis. New York: Springer; 2012. p. 119-132. http://dx.doi.org/10.1007/978-1-4614-0998-4_8 [ Links ]
11. Rigottier-Gois L. Dysbiosis in inflammatory bowel diseases: The oxygen hypothesis. ISME J. 2013;7:1256-1261. http://dx.doi.org/10.1038/ismej.2013.80 [ Links ]
12. Ley RE, Turnbaugh PJ, Klein S, Gordon JI. Microbial ecology: Human gut microbes associated with obesity. Nature. 2006;444(7122):1022-1023. http://dx.doi.org/10.1038/4441022a [ Links ]
13. Armougom F, Henry M, Vialettes B, Raccah D, Raoult D. Monitoring bacterial community of human gut microbiota reveals an increase in Lactobacillus in obese patients and Methanogens in anorexic patients. PLoS One. 2009;4(9):e7125. http://dx.doi.org/10.1371/journal.pone.0007125 [ Links ]
14. Zhang H, DiBaise JK, Zuccolo A, Kudrna D, Braidotti M, Yu Y et al. Human gut microbiota in obesity and after gastric bypass. Proc Natl Acad Sci USA. 2009;106(7):2365-2370. http://dx.doi.org/10.1073/pnas.0812600106 [ Links ]
15. Jia W, Li H, Zhao L, Nicholson JK. Gut microbiota: A potential new territory for drug targeting. Nat Rev Drug Disc. 2008;7:123-129. http://dx.doi.org/10.1038/nrd2505 [ Links ]
16. Raoult D. Probiotics and obesity: A link? Nat Rev Microbiol. 2009;7:616. http://dx.doi.org/10.1038/nrmicro2209 [ Links ]
17. Jia W, Li H, Zhao L, Nicholson JK. Gut microbiota: A potential new territory for drug targeting. Nat Rev Drug Discov. 2008;7(2):123-129. http://dx.doi.org/10.1038/nrd2505 [ Links ]
18. Kong HH, Segre JA. Skin microbiome: Looking back to move forward. J Investigat Dermatol. 2012;132:933-939. http://dx.doi.org/10.1038/jid.2011.417 [ Links ]
19. Lai Y Cogen AL, Radek KA, Park HJ, MacLeod DT, Leichtle A, et al. Activation of TLR2 by a small molecule produced by Staphylococcus epidermidis increases antimicrobial defense against bacterial skin infections. J Investigat Dermatol. 2010;130:2211-2221. http://dx.doi.org/10.1038/jid.2010.123 [ Links ]
20. Grice EA, Kong HH, Conlan S, Deming CB, Davis J, Young AC, et al. Topographical and temporal diversity of the human skin microbiome. Science. 2009;324(5931):1190-1192. http://dx.doi.org/10.1126/science.1171700 [ Links ]
21. Grice EA, Segre JA. The skin microbiome. Nat Rev Microbiol. 2009;9:244-253. http://dx.doi.org/10.1038/nrmicro2537 [ Links ]
22. Pflughoeft KJ, Versalovic J. Human microbiome in health and disease. Annu Rev Pathol. 2012;7:99-122. http://dx.doi.org/10.1146/annurev-pathol-011811-132421 [ Links ]
23. Linhares IM, Kanninen TT, Orfanelli T, Jayaram A, Doulaveris G, Witkin SS. The vaginal microbiome: New findings bring new opportunities. Drug Dev Res. 2013;74:360-364. http://dx.doi.org/10.1002/ddr.21090 [ Links ]
24. White BA, Creedon DJ, Nelson KE, Wilson BA. The vaginal microbiome in health and disease. Trends Endocrinol Metab. 2011;22(10):389-393. http://dx.doi.org/10.1016/j.tem.2011.06.001 [ Links ]
25. Hickey RJ, Zhou X, Pierson JD, Ravel J, Forney LJ. Understanding vaginal microbiome complexity from an ecological perspective. Transl Res. 2012;160:267-282. http://dx.doi.org/10.1016/j.trsl.2012.02.008 [ Links ]
26. Macklaim JM, Fernandes AD, Di Bella JM, Hammond JA, Reid G, Gloor GB. Comparative meta-RNA-seq of the vaginal microbiota and differential expression by Lactobacillus iners in health and dysbiosis. Microbiome. 2013;1(1):12. http://dx.doi.org/10.1186/2049-2618-1-12 [ Links ]
27. Carey JC, Klebanoff MA, Hauth JC, Hillier SL, Thom EA, Ernest JM. Metronidazole to prevent preterm delivery in pregnant women with asymptomatic bacterial vaginosis. N Engl J Med. 2000;342(8):534-540. http://dx.doi.org/10.1056/NEJM200002243420802 [ Links ]
28. Hummelen R, Fernandes AD, Macklaim JM, Dickson RJ, Changalucha J, Gloor GB. Deep sequencing of the vaginal microbiota of women with HIV PLoS ONE. 2012;5(8):e12078. [ Links ]
29. Heinemann C, Reid G. Vaginal microbial diversity among postmenopausal women with and without hormone replacement therapy. Can J Microbiol. 2005;51(9):777-781. http://dx.doi.org/10.1139/w05-070 [ Links ]
30. MacPhee RA, Hummelen R, Bisanz JE, Miller WL, Reid G. Probiotic strategies for the treatment and prevention of bacterial vaginosis. Expert Opin Pharmacother. 2010;11(18):2985-2995. http://dx.doi.org/10.1517/14656566.2010.512004 [ Links ]
31. Ramsay M. Africa: Continent of genome contrasts with implications for biomedical research and health. FEBS Lett. 2012;586:2813-2819. http://dx.doi.org/10.1016/j.febslet.2012.07.061 [ Links ]
32. Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384(9945):766-781. http://dx.doi.org/10.1016/S0140-6736(14)60460-8 [ Links ]
33. Kuczynski J, Lauber CL, Walters WA, Parfrey LW, Clemente JC, Gevers D, et al. Experimental and analytical tools for studying the human microbiome. Nat Rev Genet. 2012;13(1):47-58. http://dx.doi.org/10.1038/nrg3129 [ Links ]
34. Cohen CR, Lingappa JR, Baeten JM, Ngayo MO, Spiegel CA, Hong T, et al. Bacterial vaginosis associated with increased risk of female-to-male HIV-1 transmission: A prospective cohort analysis among African couples. PLoS Med. 2012;9(6):e1001251. [ Links ]
35. Dols JA, Smit PW, Kort R, Reid G, Schuren FH, Tempelman H, et al. Microarray-based identification of clinically relevant vaginal bacteria in relation to bacterial vaginosis. Am J Obstet Gynecol. 2011;204(4):305.e1-305.e7. [ Links ]
36. Gray C, Chung S-L. Food allergy in South Africa: Joining the food allergy epidemic? Curr Allergy Clin Immunol. 2012;25(1):24-29. [ Links ]
37. Serazin AC, Shackelton LA, Wilson C, Bhan MK. Improving the performance of enteric vaccines in the developing world. Nat Immunol. 2010;11(9):769-773. http://dx.doi.org/10.1038/ni0910-769 [ Links ]
38. Kent A. Modern medical microbiology. Rev Obstet Gynecol. 2011;4(2):92-93. [ Links ]
 Correspondence:
Correspondence:
Viness Pillay
Department of Pharmacy and Pharmacology
University of the Witwatersrand Medical School,
7 York Road
Parktown 2193
South Africa
EMAIL: viness.pillay@wits.ac.za


{kind=link}
{kind=link}
{kind=link}