










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Science
On-line version ISSN 1996-7489
Print version ISSN 0038-2353
S. Afr. j. sci. vol.109 n.9-10 Pretoria Jan. 2013
RESEARCH ARTICLE
Morphometric analysis of the patella and patellar ligament of South Africans of European ancestry
Oladiran I. OlatejuI; Illke PhilanderI; Mubarak A. BidmosI, II
ISchool of Anatomical Sciences, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIDepartment of Anatomy, Canadian Memorial Chiropractic College, Toronto, Canada
ABSTRACT
Morphometric analyses of the patella and patellar ligament have been reported to be important in human identification, in knee implant design and in certain surgical procedures of the knee. It has also been shown that success in the functionality of a knee arthroplasty (knee replacement) is dependent on the implant being of an appropriate dimension. We undertook this study because of the lack of available data on these dimensions in South Africans. Careful dissection was carried out on both knees of 46 South African cadavers (25 females and 21 males) of European ancestry. The quadriceps femoris tendon and patellar ligament were carefully freed from the underlying structures. Eight measurements of the patella and patellar ligament were taken using a Vernier caliper. Patellae were also classified based on the dimensions of the articular facets. No significant difference was found when the measurements taken from both knees were compared except for the dimensions of patella thickness and widths. Dimensions of the patella, patellar ligament and articular facets are sexually dimorphic. In addition, measurements of the patella and patellar ligament showed significant positive correlations, with Type B patellae being the most prevalent in South Africans of European ancestry. The data from the present study will be beneficial in clinical and pathological practices and for local anthropological records.
Keywords: patella; patellar ligament; articular facets; South African; European ancestry
Introduction
The patella is the largest sesamoid bone in the body which develops within the tendon of the quadriceps femoris muscle. It is a flat bone 'poised like a shield' on the anterior surface of the femoral condyles. It has two surfaces (anterior and posterior), three borders (superior, medial and lateral) and an apex pointing inferiorly. The anterior surface is covered superficially by the continuation of the fibres of the tendon of rectus femoris. The muscles of the quadriceps femoris converge to form a single tendon. In addition, the vastus medialis muscle attaches medially to this tendon before it blends distally with the patellar ligament.1,2
The posterior surface of the patella can be divided into two parts: superior (articulating) and inferior (non-articulating). The inferior part forms the apex of the patella which serves as a site of attachment for the patellar ligament. The superior part, however, is sub-divided into lateral and medial facets which are separated by a vertical ridge.
The usefulness of the patella in human identification as well as its role in the normal mechanical design of the knee have been widely studied.3,4 In addition, morphometric data obtained from the patella and patellar ligament are crucial in the diagnoses and surgical corrections of knee-related injuries or disorders.3,4 Other studies have provided informative prognostic factors for patellofemoral joint disorders.5,6 Consequently, dimensions of the patella and patellar ligament are often utilised in implant design and certain surgical procedures such as patella resurfacing for total knee arthroplasty and the harvesting technique of patellar ligament grafts during the reconstruction of the anterior cruciate ligament.4,7,8
An appropriate size and thickness of a patellar implant is important in ensuring success in the functionality of arthroplasty.4,9 A disproportional implant of the patellofemoral joint would result in an ineffective lever support, limitation of motion, excessive wear and instability of the patella with associated knee pain.4,9 Patella instability is often associated with an abnormal patella position, variable patella shapes, a narrowed medial articular facet or abnormal stress on the patella.10,11 In addition, disproportional patella-patellar ligament lengths could result in a significantly high positioned patella (patella alta) or a low positioned patella (patella baja) in the patellofemoral joint.12 Dimensions and classification of patellae, as well as determining the relationship between the patella and patellar ligament in different population groups, are important anthropologically as well as clinically for the determination of the size of a patellar implant.5,7,8,13-15
Wiberg13 reported that patellae can be categorised into three types based on the dimensions of the widths of medial (MAF) and lateral articular facets (LAF) as well as the curvature of the facets. According to Wiberg's classification, a Type I patella is defined as a patella whose MAF and LAF widths are concave and equal. A Type II patella is one in which the width of the MAF is flat or slightly convex and smaller than the width of the LAF. In Type III patellae, however, the width of the MAF is convex and considerably smaller than the width of the LAF.13,14 Wiberg13 also reported that Type II patellae were the most prevalent, which is in accordance with the report by Fucentese et al.14 in which they compared patella morphology in trochlear dysplastic knees with that in normal knees using a magnetic resonance imaging technique.
In another study on the classification of the patellae of foetal cadavers, Koyuncu et al.15 reported that 20% of patellae was Class A (the widths of MAF and LAF are equal). In addition, Class B (the width of the MAF is smaller than the width of the LAF) was reported as the most prevalent (50%) while 30% of patellae was Class C (the width of MAF was greater than the width of the LAF). In the same study, there was no significant difference in the measurements of the patella and patellar ligament between the sexes.15 The difference between the classification of patella as suggested by Wiberg13 and the classifications reported by Fucentese et al.14 and Koyuncu et al.15 is that the convexity of the patella was not considered in the latter studies. Despite the differences in the measuring parameters, the findings of the studies were similar.
More recently, Philips et al.7 used a radiographic technique to calculate the Insall-Salvati index which is defined as the ratio of the length of the patellar ligament to the greatest length of the patella.5,7,8 The mean (range) of the normal ratio of the Insall-Salvati index is 1.0 (0.8-1.2). The drawbacks of using the Insall-Salvati index include a lack of sensitivity to patella morphology and abnormalities, and an approximation only of tibial tuberosity as the measurements are derived from lateral radiographs of the knee.7,16,17 Attempts have been made to reduce the errors from the measurement on radiographs but the approximation and assumptions which are used affect the accuracy of this radiographic technique.7,16 However, measurements performed in situ, that is a cadaveric approach, are likely to be more accurate because they do not involve approximation and assumptions.
As there has been no previous morphometric study on the patellae of any population group of South Africa, it therefore became necessary to establish such data on the dimensions of patella and patellar ligaments, as well as to classify the patella based on the widths of its articular facets. The measurements were taken in situ on a sample of cadavers of South Africans of European ancestry.
Materials and methods
The sample consisted of 46 (25 female and 21 male) South African cadavers of European ancestry, housed for teaching purposes in the School of Anatomical Sciences, University of the Witwatersrand, Johannesburg, South Africa (Human Ethics number W-CJ-101109-1). Cadavers with osteoarthritic changes to the knee, visible surgical scars in the knee region, physical signs of deformity of the patella or signs of patellofemoral disease were excluded from the study. The mean age of the male cadavers was 72.6 years (range 40-92) and of the female cadavers was 77.3 years (range 47-98).
A 15-cm incision was made on the medial sides of both knees of the cadaver after which the skin and facia lata covering both knees were carefully removed in order to expose the quadriceps tendon, the patella and the patellar ligament. The tendon of quadriceps femoris and the patellar ligament were carefully freed from the underlying structures without causing any damage or alteration to the desired structures. With the knee flexed as much as possible but not in excess of 45 degrees,15 the maximum patellar ligament height (PLH) and the maximum patellar ligament width at the proximal attachment (PLW) were measured using a Vernier caliper (Table 1).
Measurements of the patella, namely maximum patella height (PH), maximum patella width (PW) and maximum patella thickness (PT), were also taken with a Vernier caliper (Table 1). The patella was subsequently released by freeing the tendon of the quadriceps femoris from the superior border of the patella. The maximum widths of the medial (WMAF) and the lateral articular facets (WLAF) were also measured (Table 1). Based on the dimension of WMAF in relation to WLAF, each patella was classified into one of three categories15: Type A (WMAF=WLAF), Type B (WMAF WLAF).
Statistical analyses
An assessment of the reliability of the measuring technique was performed using an intra-observer reliability test known as Lin's concordance correlation coefficient (Pc). This test was selected because it is a measure of both precision and accuracy between the test and retest measurement.18 With an assumption that the data are analysed with an error low enough to be acceptable, a Student's t-test was used to ascertain whether a significant difference existed between the measurements taken from opposite sides of the body. In addition, a Pearson's correlation coefficient was calculated for a selected measurement in an attempt to determine the strength of the relationship between them. For the classification of the patella articular surfaces, a 95% confidence interval of the measurement error was calculated. All statistical analyses were performed at a significance level of 5%.
Results
Reliability test
The Lin's concordance correlation coefficient (Pc) for all measurements ranged between 0.94 (for WLAF) and 0.99 (for PH) (Table 2). This result shows that there was no significant difference between the test and the retest measurement, which therefore shows that the measuring technique and the data were analysed with an error low enough to be acceptable.

Side differences
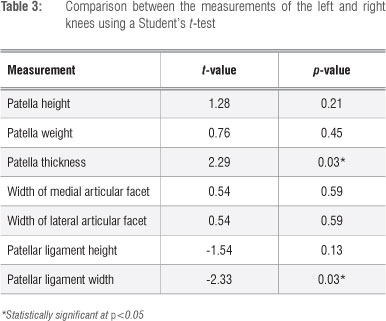
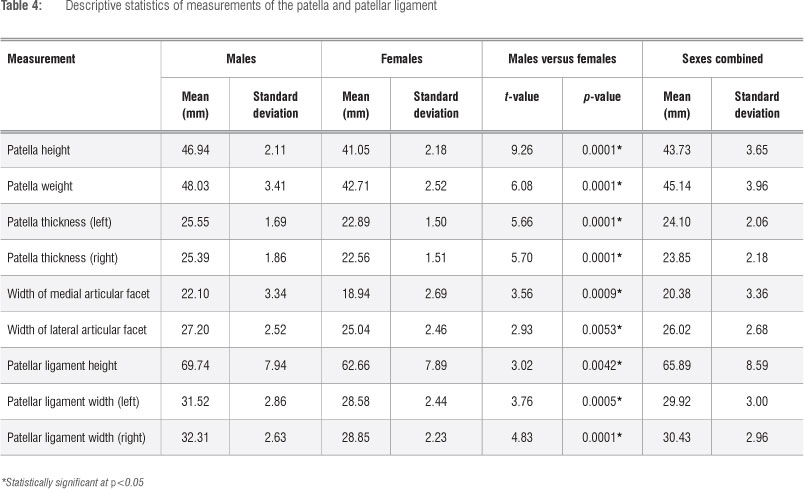
A Student's t-test revealed that there was no statistically significant difference in the measurements of the patella between the sides of the body, except for PT (p=0.03) and PLW (p=0.03) (Table 3).Consequently, the dimensions of PT and PLW were presented and analysed separately for each side (Table 4).
Descriptive analyses
The mean and standard deviation for measurements of the patella and the patellar ligament are presented in Table 4. The means of PH, PW, WMAF, WLAF and PLH were significantly higher in the male cadavers than in the female cadavers. In addition, the mean PT and PLW on both left and right knees were higher in the male cadavers than in the female cadavers (Table 4). The PLH presented with the highest amount of variation (σ2: M = 63.04, F=62.25) while the least amount of variation in both sexes was observed for the PT (σ2: M = 2.86, F=2.25).
Analyses of correlation
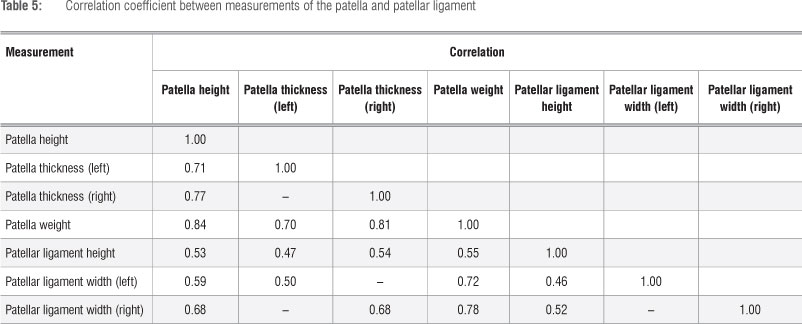
There was a positive correlation between all the paired dimensions of the patella (Table 5). The strongest relationship was observed between the PH and PW (R=0.84). The weakest relationship was found between the PLH and PLW (left) with a correlation coefficient of 0.46. Overall, most of the measurements showed moderate correlation (range 0.4-0.7) with each other (e.g. PLH/PH: 0.53; PLH/PW: 0.55). A strong correlation (range 0.7-0.9) was between PH and PW (0.84), PT (right) (0.77) and PT (left) (0.71).
Classification of the articular surface of patella
Most (87%) of the patellae in the studied sample were classified as Type B. Of the 46, 5 (11%) were Type A, and one (2%) was classified as Type C.
Discussion
Previous studies have used different measuring techniques, including measurements taken during total knee arthroplasty9,19 and the use of radiographs14,20, in an attempt to obtain the dimensions of the patella, the articular facets of the patella and the patellar ligaments. An advantage of a radiographic collection is the availability of a larger sample size compared to a limited number of (embalmed) cadavers. However, the disadvantage of the radiographic method is that the number of measurements of the patella, its articular facets and the patellar ligament that can be measured at any given time is limited. It is also difficult to establish a possible integration of the dimensions of the patella with the patellar ligament. In addition, with radiographic methods there is a need for assumptions, such as approximating the extent of the tibial tuberosity while measuring the length of the patellar ligament.
The cadaveric approach, which was used in this study, allowed several measurements to be taken on each cadaver in situ. The integration of measurements could be beneficial for surgeries of the knee and for the anthropological records in South Africa. It could be argued that shrinkage of soft tissue in embalmed samples could be a disadvantage of this method; however, studies have shown that the extent of shrinkage in a formalin-fixed soft tissue is considerably minimal,21,22 although prolonged tissue fixation in formalin could produce more tissue shrinkage and hardening.21 Because the embalming process requires formalin perfusion of specimens and there is no report in the literature that states the extent of shrinkage during such a process, we considered that shrinkage in the embalmed samples used in this study had negligible effects on the data and the final analysis. In order to negate any possible effects of such shrinkage, we suggest that samples of fresh cadavers (before embalming) be used or that measurements be taken on living humans during knee surgery.
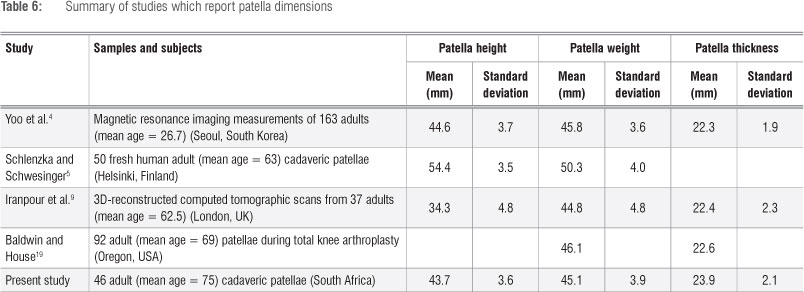
In the present study, the mean height, width and thickness of the patella of both sexes were 43.73 mm, 45.14 mm and 24.10 mm, respectively. In addition, the mean height and width of the patellar ligament in both sexes were 65.89 mm and 30.17 mm, respectively (Table 4). The data obtained from this study were compared with those from previous studies as summarised in Table 6. It is well documented that morphometric variations are often observed in measurements taken within any population group and that the variation could be more significant between different groups. Although the reasons for these variations have not been validated, it has been suggested that differences in measuring methods, sexes, age and stature could be contributing factors.
It was, however, not surprising to find that the measurements of the patella, patellar ligament and articular facets were higher in the male cadavers than in the female cadavers. This finding is an indication that the patella, the patellar ligament and the width of articular facets are sexually dimorphic. Previously, Bidmos et al.23, in a study on 120 dried normal and undamaged patellae of South Africans of European ancestry which were obtained from an osteological collection, reported that the maximum height and maximum width of the patella can be used in correct sex classification with an average accuracy of 85% and 79%, respectively. Their results are similar to those of a study conducted in Iran24 in which a higher average accuracy was obtained for the maximum height (89%) and maximum width (91%).
In the present study, there was no significant difference in the dimensions of all the measurements of the patella, the patellar ligament and the articular facets when the measurements taken on both the right and left knees were compared, except in the case of patella thickness and patella width. Even though we do not have an explanation for the variation in the measurements taken on both knees for the patella thickness and patella width, we hypothesise that the predominant use of one limb could produce better muscle tone on one side, which could possibly have a direct effect on the shape of the sesamoid bone (patella) within its tendon (quadriceps femoris). Posture and physique could also be contributing factors, but the exact contributions of these factors could not be ascertained in this study.
There is a moderate to strong correlation between paired measurements of the patella in the current study. In addition, the correlation observed in the right knee was stronger than that in the left knee when the thickness and the width of the patellae were compared. This observation is in agreement with the results of Iranpour et al.9 in which a strong correlation was reported between the thickness and width of the patella (R=0.89). The width of the patella has been suggested to be a dependable factor for predicting the normal size of patella thickness, as well as for helping surgeons to decide on the thickness of the patella prosthesis during arthroplasty.9 Although certain factors such as height, weight and ancestry4,15,25 could also be used to predict the normal size of patella thickness.
The patella thickness to width ratio is also a reliable predictive factor as long as there is no damage to the median ridge on the articular surface.9 The observed strong positive correlation between the patella height and the patella width in this study supports the findings of Koyuncu et al.15, in which a linear relationship was demonstrated between the length and width of the patella throughout gestational age. However, the correlation between the height of the patellar ligament and the height of the patella, in the present study, was moderate.
While several studies have used the Insall-Salvati ratio (which ranges between 1 and 1.3) to determine the resting position of the patella,5,7,15 an attempt was made in this study to also calculate the ratio. The Insall- Salvati ratio obtained for female specimens was 1.53 and that for male specimens was 1.49 - both greater than 1.3, which indicates that the patellae of South Africans of European ancestry are positioned high (patella alta) in the patellofemoral joint. While it is well documented that a significant variation exists in the positions of patella among different population groups (including Europeans, Arabs, Africans and Chinese), patella alta has been found to be more common amongst non-European population groups.7 The Insall-Salvati ratios obtained from the sample used in the present study are relatively high and are not in agreement with findings from other studies.5,7,15 However, the higher value obtained for female individuals compared with male individuals is in agreement with the findings of Norman et al.26 and Koyuncu et al.15
Apart from the classification of the patella based on its relative position, patellae can also be classified based on the dimensions of the articular facets. In the present study, it was found that the Type B patella was the most prevalent, which is in support of previous observations by Reider et al.2, Fucentese et al.14 and Koyuncu et al.15 Fucentese et al.14 found Type B to be the most prevalent while Type C was the least prevalent.
In conclusion, we suggest that measurements of fresh cadavers or of living subjects during knee surgery be used to eliminate the uncertainty of tissue shrinkage associated with embalmed cadavers. However, the ability to integrate measurements from the cadaveric method and the availability of embalmed specimens are advantages over fresh cadavers or living subjects. A significant difference in the measurements of the PT and the PLW between the left and right knees is an indication that one side of the body is not a direct mirror image of the other side. Further investigations should be done to determine if the dominant use of a limb could be a contributing factor to these variations. Furthermore, the findings of this study indicate that the dimensions of the patella, the patellar ligament and the widths of the articular facets are sexually dimorphic. The prevalence of the Type B patella in South Africans of European ancestry is similar to that of other population groups reported in the literature. The morphometric data presented in this study is beneficial for local anthropological records as well as clinically to assist local orthopedic surgeons in procedures involving the knee, such as in the design of patella implants. It is thus recommended that similar studies should be performed on other population groups in South Africa.
Acknowledgements
We are grateful to the School of Anatomical Sciences of the University of the Witwatersrand for giving us access to the Human Collections and to Jason Hemingway for his assistance with the statistical analysis.
Authors' contributions
O.I.O. was the project leader; he was responsible for the experimental and project design, assisted in the collection of data and wrote the manuscript. I.P. was responsible for the collection of data, made conceptual contributions and performed the calculations. M.A.B. made conceptual contributions, verified the calculations and assisted in writing the manuscript.
References
1. Drake RL, Vogl AW, Mitchell AWM. Lower limb. In: Gray's anatomy for students. 2nd ed. Philadelphia, PA: Churchill Livingstone; 2010. p. 558-564. http://dx.doi.org/10.1016/B978-0-443-06952-9.00011-4 [ Links ]
2. Reider B, Marshall JL, Koslin B, Ring B, Girgis FG. The anterior aspect of the knee joint. J Bone Joint Surg Am. 1981;63:351-356.
3. Miller TT, Staron RB, Feldman F. Patellar height on sagittal MR imaging of the knee. AJR Am J Roentgenol. 1996;167:339-341. http://dx.doi.org/10.2214/ajr.167.2.8686598
4. Yoo JH, Yi SR, Kim JH. The geometry of patella and patellar tendon measured on knee MRI. Surg Radiol Anat. 2007;29:623-266. http://dx.doi.org/10.1007/s00276-007-0261-x
5. Schlenzka D, Schwesinger G. The height of the patella: An anatomical study. E J Radiol. 1990;11:19-21. http://dx.doi.org/10.1016/0720-048X(90)90097-U
6. Andrikoula S, Tokis A, Vasiliadis HS, Georgoulis A. The extensor mechanism of the knee joint: An anatomical study. Knee Surg Sports Traumatol Arthrosc. 2006;14:214-220. http://dx.doi.org/10.1007/s00167-005-0680-3
7. Philips CL, Silver DAT, Schranz PJ Mandalia V. The measurement of patellar height: A review of the methods of imaging. J Bone Joint Surg Br. 2010;92B:1045-1053. http://dx.doi.org/10.1302/0301-620X.92B8.23794
8. Portner O, Pakzad H. The evaluation of patellar height: A simple method. J Bone Joint Surg Am. 2011;93:73-80. http://dx.doi.org/10.2106/JBJS.L01689
9. Iranpour F, Merican AM, Cobb JP, Amis AA. The width:thickness ratio of the patella: An aid in knee arthroplasty. Clin Orthop Relat Res. 2008;466:1198-1203. http://dx.doi.org/10.1007/s11999-008-0130-x
10. Biedert RM, Albrecht S. The patellotrochlear index: A new index for assessing patellar height. Knee Surg Sports Traumatol Arthrosc. 2006;14:707-712. http://dx.doi.org/10.1007/s00167-005-0015-4
11. Teichtahl AJ, Parkins K, Hanna F, Wluka AE, Urquhart DM, English DR, et al. The relationship between the angle of the trochlear groove and patella cartilage and bone morphology: A cross-sectional study of healthy adults. Osteoarthr Cartil. 2007;15:1158-1162. http://dx.doi.org/10.1016/j.joca.2007.03.010 [ Links ]
12. Shabshin N, Schweitzer ME, Morrison WB, Parker L. MRI criteria for patella alta and baja. Skeletal Radiol. 2004;33:445-450. http://dx.doi.org/10.1007/s00256-004-0794-6
13. Wiberg G. Roentgenographic and anatomic studies on the femoropatellar joint. Acta Orthop Scand. 1941;12:319-410. http://dx.doi.org/10.3109/17453674108988818
14. Fucentese SF, Von Roll A, Koch PP Epari DR, Fuchs B, Schottle PB. The patella morphology in trochlear dysplasia: A comparative MRI study. Knee. 2006;13:145-150. http://dx.doi.org/10.1016/j.knee.2005.12.005
15. Koyuncu E, Cankara N, Sulak O, Ozguner G, Albay S. The morphometry of patella and patellar ligament during the fetal period. Clin Anat. 2011;24:225-231. http://dx.doi.org/10.1002/ca.21075
16. Grelsamer RP Meadows S. The modified Insall-Salvati ratio for assessment of patellar height. Clin Orthop Relat Res. 1992;282:170-176.
17. Basso O, Johnson DP Amis AA. The anatomy of the patellar tendon. Knee Surg Sports Traumatol Arthrosc. 2001;9:2-5. http://dx.doi.org/10.1007/s001670000133
18. Landis JR, Koch GG. The measurement of the observer agreement for categorical data. Biometrics. 1977;33:159-174. http://dx.doi.org/10.2307/2529310
19. Baldwin JL, House K. Anatomical dimensions of the patella measured during total knee arthroplasty. J Arthroplasty. 2005;20:250-257. http://dx.doi.org/10.1016/j.arth.2004.09.027
20. Roberts CS, King DH, Goldsmith LJ. A statistical analysis of the accuracy of sonography of the patellar tendon. Arthroscopy. 1999;15:388-391. http://dx.doi.org/10.1016/S0749-8063(99)70056-3
21. Hopwood D. Fixation and fixatives. In: Bancroft JD, Stevens A, editors. Theory and practice of histological techniques. London: Churchill Livingstone; 1982. p. 20-40. [ Links ]
22. Boonstra H, Oosterhuis JW, Oosterhuis AM, Fleuren GJ. Cervical tissue shrinkage by formaldehyde fixation, paraffin wax embedding, section cutting and mounting. Virchows Arch (Pathol Anat). 1983;402:195-201. http://dx.doi.org/10.1007/BF00695061
23. Bidmos MA, Steinberg N, Kuykendall KL. Patella measurements of South African Whites as sex assessors. Homo. 2005;56:69-74. http://dx.doi.org/10.1016/j.jchb.2004.10.002
24. Akhlaghi M, Sheikhazadi A, Naghsh A. Identification of sex in Iranian population using patella dimensions. J Forensic Legal Med. 2010;17:150- 155. http://dx.doi.org/10.1016/j.jflm.2009.11.005
25. Yoon-Seok Y Woo-Shin C, Jae-Ho W, Byung-Kwan K. The effect of patellar thickness changes on patellar tilt in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2010;18:923-927. http://dx.doi.org/10.1007/s00167-010-1059-7
26. Norman O, Egund N, Ekelund L, Runow A. The vertical position of the patella. Acta Orthop Scand. 1983;54:908-913. http://dx.doi.org/10.3109/17453678308992932
 Correspondence:
Correspondence:
Oladiran Olateju
School of Anatomical Sciences
Faculty of Health Sciences
University of the Witwatersrand, 7 York Road
Parktown 2193, Johannesburg, South Africa
Email: oladiran.olateju@wits.ac.za
Received: 15 Mar. 2013
Revised: 10 May 2013
Accepted: 03 Jun. 2013


{kind=link}
{kind=link}
{kind=link}
{kind=link}