










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Science
versión On-line ISSN 1996-7489
versión impresa ISSN 0038-2353
S. Afr. j. sci. vol.109 no.7-8 Pretoria ene. 2013
RESEARCH ARTICLE
Exposure to CCA-treated wood amongst food caterers and residents in informal areas of Cape Town
Sivapregasen NaidooI, II; Algernon AfricaI; Mohamed Aqiel DalvieI
ICentre for Occupational and Environmental Health Research, School of Public Health and Family Medicine, University of Cape Town, Cape Town, South Africa
IIEnvironmental Processes and Systems Engineering, Chemical Engineering Department, Faculty of Engineering and Built Environment, University of Cape Town, Cape Town, South Africa
ABSTRACT
We investigated the absorption of chromium, copper and arsenic released from treated wood used by street food caterers and household residents in an informal urban area and a peri-urban area in Cape Town, South Africa. Participants (n=78) selected included an equal number of caterers and residents in each area. All participants answered an exposure questionnaire and were tested for urinary chromium, copper and arsenic, while the urine of 29 participants was also tested for toxic arsenic. Urinary chromium and arsenic exceeded the environmental exposure limit in 12% and 30% of participants, respectively. Toxic arsenic was detected in 30% of samples of which 24% exceeded the environmental exposure limit of 6.4 µg/g creatinine. Urinary chromium, copper, arsenic and toxic arsenic levels were not significantly different between participants from the two areas or between caterers and household residents, controlling for confounding effects. The study provides evidence of chromium and arsenic exposure amongst both informal caterers and household residents, which requires further investigation.
Keywords: arsenic; chromium; informal food caterers; treated wood; wood fuel
Introduction
Chromated copper arsenate (CCA) is a wood preservative used worldwide since the 1930s, although its use has been restricted in developed countries. In South Africa, it is still commonly used.
A previous investigation indicated that CCA-treated wood used as fuel for open fires in street catering could be a significant potential public health problem in Cape Town.1 In the latter study, CCA-treated wood samples were found in wood used for informal catering activities with the occurrence of treated wood being more prevalent in urban townships than in peri-urban areas of Cape Town. The wood was sourced from commercial and industrial sources.
Exposure to arsenic (As), chromium (Cr) and copper (Cu) from CCA-treated wood can occur through inhalation of fumes and dust released on combustion of the wood, through contact with the wood ash, or contaminated water and soil, or through ingestion of contaminated water, food or soil.2 The toxic species of Cr is Cr(IV), of As include As(III) and As(V) and of Cu is Cu(II). Intake of high doses of the toxic species of As and Cr are acutely toxic and could be fatal. The toxic species of As and Cr are known carcinogens at lower doses and are associated with a number of non-cancerous long-term health effects (Table 1). Long-term exposure to Cu(II) is associated with respiratory effects.

Urinary measurement of Cr, Cu and As is a reliable method used for the biomonitoring of persons exposed to CCA.3 In the human body, most inorganic As is converted to methylarsonic acid (MMA) and dimethylarsinic acid (DMA) with a small percentage remaining in its original form.4,5 Measurement of total urinary As includes measurement of the toxic inorganic forms as well as low-toxicity organic forms (arsenobetaine, arsenosugars, arsenolipids) sourced generally from seafood.6 Measurement of urinary As species is a more advanced method for As biomonitoring. Absorbed Cr(IV) is reduced in the body to Cr(III) and primarily excreted in the urine. Urinary Cr is a marker of recent exposure to Cr(IV). Cu occurs in two oxidative states - Cu(I) and Cu(II) -and urinary Cu is a marker of recent exposure to total Cu.
The aim of this study was to compare the exposure to CCA-treated wood and the urinary levels of Cr, Cu and As amongst informal food caterers and household residents in an urban area and a peri-urban area in the Western Cape Province in South Africa, following on from a previous study.1 The relationship between the usage of CCA-treated wood and urinary levels of Cr and Cu will be examined in another paper
Subjects and methods
Study area, design, population and sampling
A cross-sectional study of adult street food caterers and household residents from informal settlement areas was conducted in the Western Cape in 2011. Forty participants each from Langa, an urban area, and Stellenbosch, a peri-urban area, were selected. The urban and periurban areas represented low- and high-exposure groups, respectively, as the results in the previous study1 indicated that wood used for fuel collected from urban areas contained lower levels of CCA than wood samples collected from peri-urban areas. The informal settlements are composed of poor communities of mostly unemployed people who live in galvanised iron shacks and use outdoor sanitation facilities.
In each area, 20 food caterers and 20 household residents, with an equal number of men and women in each group, participated in the study. Fifty community members in each area, identified by community leaders, attended a meeting in the area prior to the commencement of data collection. At these meetings, the community members of both areas agreed to participate after being informed about the study. On the day of data collection, the first 20 food caterers and 20 household residents in each area who could be contacted were selected to participate.
Exposure to CCA-treated wood was assessed based on a short questionnaire that the participants completed as well as urinary concentrations of As, Cr and Cu.
Questionnaire
A piloted and back-translated questionnaire containing sections on demographics and lifestyle information (name, age, schooling, place of residence, sex, household income, alcohol consumption and smoking), doctor diagnosed chronic health diseases, usage of wood during catering and home cooking (number of hours per day, days per week, quantity and size of container drums and number of years), health problems (As poisoning, skin problems, respiratory problems) and recent fish consumption were administered by trained interviewers to participants in either English or their home language (Xhosa). The questionnaire comprised both closed- and open-ended questions. The interviews (about 20 min in duration) were conducted at the catering sites and residences of participants.
Urinary measurements
An experienced and trained research assistant collected spot urine samples from participants after requesting them to provide samples in plastic containers with plastic caps. The research assistant previously underwent training from a nurse and had experience in specimen collection in a number of previous research projects in similar communities. Participants were given an individual detailed briefing by a trained field worker during which they were informed of the purpose and methodology of the study and of the requirements (such as the washing of hands prior to providing a urine sample) to prevent external contamination of the sample.
Urine specimens were provided between 08:00 and 14:30 in a private room at the catering site or home of the participant. Samples were then stored at sub-ambient temperatures in a cooler box. Care was taken to ensure the samples remained intact and free from contamination by storing them in sealed unit packaging. Urine samples were delivered to the Ampath N1 City Hospital Laboratory in Cape Town within 24 h of collection, from where they were transferred to their main laboratory in Gauteng, which is accredited for analysis of As, Cr and Cu (by the South African National Accreditation System).
Total Cr, Cu and As (As(tot)) were measured in all samples using inductively coupled plasma (ICP).7 Additionally, all samples with total As≥20 µg/L were analysed for speciated As including arsenobetaine, arsenite, DMA, MMA and arsenate using high-performance liquid chromatography ICP with mass spectrophotometry analysis.7 As(tox) was calculated as the sum of arsenobetaine, A (arsenite + arsenate), MMA and DMA. Urinary Cr, Cu, As and As(tox) concentrations were adjusted for urinary creatinine concentrations. A zero value was allocated when there was no metal detected.
Urine samples with creatinine concentrations within and outside the World Health Organization's8 recommended creatinine concentration range of 0.3-3.0 g/L were distinguished and taken into account in the analysis.
Statistical analysis
Urinary concentrations of Cr, Cu, As(tot) and As(tox) adjusted for urinary creatinine were the primary outcome variables analysed both as continuous variables and as dichotomous variables. The two cut-off values used for the dichotomous variables were the respective detection and environmental exposure limits for the metals (coding: 1 ≥ limit; 0 < limit). Area and caterer/household resident were the primary exposure variables. Descriptive comparisons were conducted across area and caterer/household resident using univariate and bivariate analyses. Non-parametric tests were used when neither the raw nor the log-transformed data were distributed normally. Tests used in bivariate analysis for two continuous variables were the Pearson correlation coefficient (for normally distributed data) or the rank sum correlation (for data not normally distributed) and simple linear regression analysis. A t-test (for normally distributed data) or Wilcoxon rank sum test (for data not normally distributed) was used for one dichotomous and one continuous variable, and the Chi-squared test was used for two dichotomous variables.
Multiple linear regression analysis and logistic regression analysis were performed to determine the relationships between the dependent (outcome) variable (continuous or dichotomous variable generated from urinary metal levels) and the dependent variables that included one exposure variable (area or caterer/household resident) and the potential confounders (age, gender, education, smoking, eating fish, and eating and drinking while cooking).
Data were entered and analysed using the Stata 8 statistical package.9 A 5% level of significance was used.
Ethics
The study was conducted in accordance with the recommendations outlined in the Declaration of Helsinki10 and the proposal was approved by the University of Cape Town's Research Ethics Committee (Reference 286/2011). Informed consent was obtained from participants who signed a consent form. In the case of illiterate participants, the consent form was read out to them and they signed by making a cross on the form. Arrangements were made for those participants whose urinary As and/or Cr concentrations were above occupational limits to undergo repeat testing.
Results
Participants
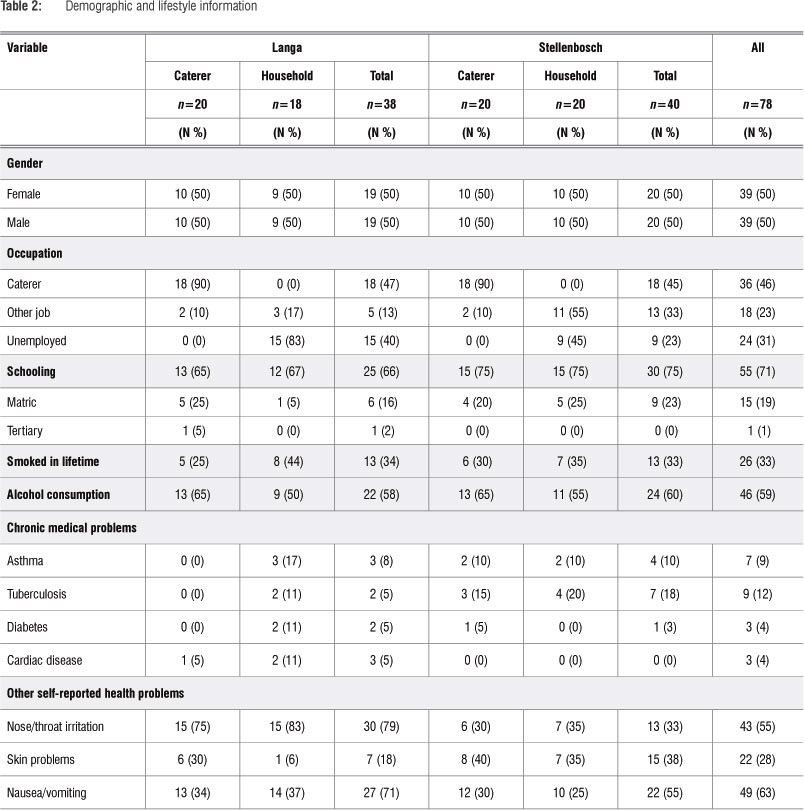
Two participants from households in Langa were excluded because they did not produce urine samples, resulting in a total of 78 participants. There was an equal distribution of participants according to study area, gender and caterer/resident categories (Table 2). Almost all caterers (92%) reported that catering was their only job. About one-third of the participants, mainly from Langa, were unemployed while the remainder, especially those in Stellenbosch, reported that they were employed as cleaners, general workers, artisans and farmworkers. More than two-thirds (71%) of the participants had attended school but only 20% had matriculated. The percentages of participants who engaged in smoking and consumed alcohol were similar between the two areas. IsiXhosa was the predominant home language. The Stellenbosch participants were significantly (p<0.05) younger (median age = 33, range: 19-55 years) than the Langa participants (median age = 41, range: 18-61 years).
Chronic and other health problems
The most common chronic health problems reported were tuberculosis and asthma. No one reported bronchitis or As poisoning. More than half of the participants reported nose or throat irritation, nearly one-third reported skin problems, including irritation (70%), pimples (23%), lesions (5%) and ringworm (2%), and nearly two-thirds reported nausea and vomiting. There was a higher number of reports of nose or throat irritation (p=0.001) and nausea and vomiting (p=0.143) in participants from Langa while more participants from Stellenbosch reported skin problems (p=0.06)(Table 2). Skin problems were more prevalent in caterers than in household residents.
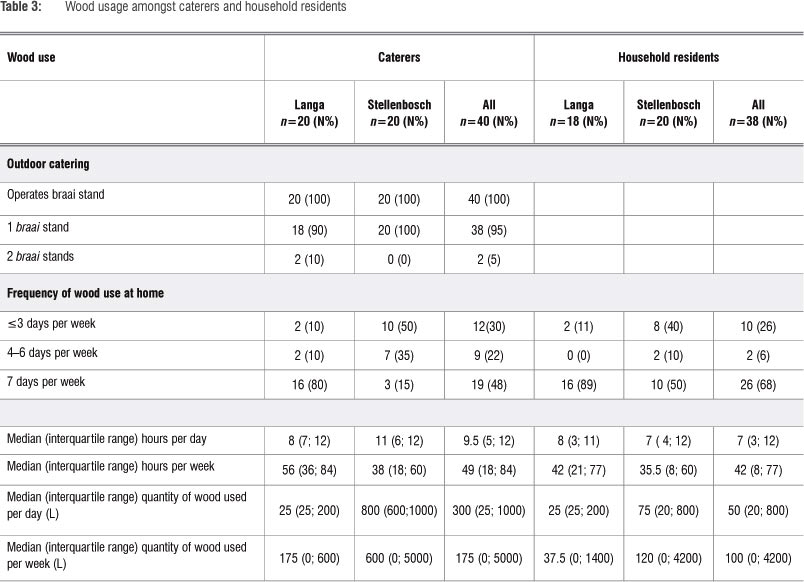
Wood usage amongst caterers and household residents
All caterers in the two areas indicated that they used various colours of wood and did not specifically identify the green tint of CCA-treated timber. They also reported using all kinds of wood for catering (Table 3). Almost all caterers (95%) operated with only one braai(grill) stand. About 80% of caterers in Langa operated 7 days per week and 50% in
Stellenbosch operated 3 days per week. All residents used wood and to the same extent as caterers. The quantity of wood used by household residents in Stellenbosch was more than that used by residents in Langa. Two (5%) residents reported that they used wood for outdoor cooking and 7 (18%) caterers reported that they also cooked indoors.
Urinary levels of Cr, Cu and As Descriptive results
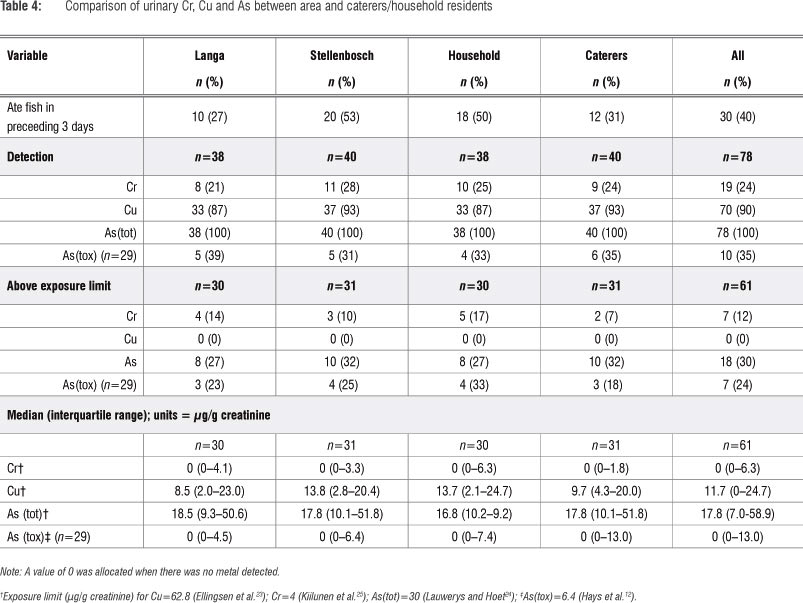
Urinary As(tot) was detected in all participants and the median As(tot) was nearly 20 µg/g creatinine (Table 4). Urinary Cr exceeded the environmental exposure limit in 12% of participants and As(tot) in 30% of participants. Amongst those reporting that they had not consumed fish in the last 3 days (n=45), and whose As(tot) levels were therefore not elevated by such intake, the median As(tot) level was 15.9 µg/g (interquartile range: 10.5-24.8 µg/g) while 25% of them (n=11) exceeded the As(tot) environmental exposure limit. As(tox) was detected in one-third of 29 urine samples analysed for speciated As, predominantly as MMA, while Asi was detected in two samples and DMA in one sample. Nearly one-quarter (24%) of participants had As(tox) levels in excess of the environmental exposure limit of 6.4 µg/g creatinine.11
Bivariate results
Urinary Cr was detected in more participants from Stellenbosch than from Langa, but the number of samples with concentrations of Cu above the environmental exposure limit was higher in Langa. Median urinary levels of Cu were slightly higher in participants from Stellenbosch, but levels of Cu and As were not different between participants in the two areas (Table 4). More participants from Stellenbosch than from Langa ate fish in the 3 days preceding sampling, which likely raised the As(tot) level in participants from Stellenbosch. The percentage of samples in which As(tox) was detected, the median As(tox) level and the percentage of samples in which the environmental exposure limit was exceeded were similar in the two areas (Table 4).
The number of samples in which urinary Cr was above the environmental exposure limit was higher for household residents than for caterers. The median urinary Cu level was also slightly higher in household residents, but median Cu and As(tot) levels were not different between the two groups (Table 4). However, a greater percentage of household residents than caterers ate fish in the 3 days preceding sampling. The speciated As sub-analysis showed that the percentage of participants in which As(tox) was detected, the median As(tox) level and the percentage of samples in which the exposure limit was exceeded were similar amongst household residents and caterers (Table 4).
Multivariate analyses results
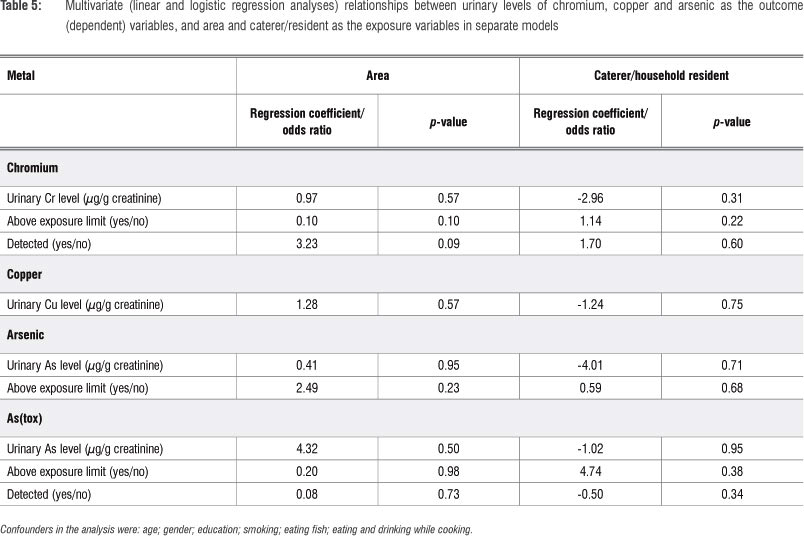
Multivariate analysis of the associations between urinary Cr, Cu, As(tot) and As(tox) modelled as the outcome variables and area as the exposure variable controlling for confounding (Table 5) showed that urinary levels, levels exceeding exposure limits and the number of samples with detectable levels were consistently higher in participants from Stellenbosch compared with participants from Langa, but not significantly so (Table 5).
Multivariate analysis of the associations between urinary Cr, Cu, As(tot) and As(tox) as outcome variables and caterer/resident as the exposure variable controlling for confounding (Table 5) showed that urinary levels, levels exceeding exposure limits and the number of samples with detectable levels were consistently higher in household residents than caterers, although not significantly so (Table 5).
Discussion
Health implications of urinary Cr, Cu and As levels
To our knowledge, this is the first study investigating Cu, Cr and As absorption through exposure to CCA-treated wood amongst informal food caterers. The median As(tot) level amongst all participants (20 µg/g creatinine) and the percentage of participants whose levels exceeded the As(tot) environmental exposure limit (30%) are higher than those of non-exposed persons.11 The elevated As(tot) levels could not be only because of intake of non-toxic forms of As as the median As(tot) level (15.9 µg/g creatinine) and the percentage of those participants whose levels exceeded the As(tot) environmental exposure limit (25%) among those that had not consumed fish in the preceeding 3 days, were also higher than those of non-exposed persons,11 indicating Asi exposure amongst the participants. Additionally, As(tox) was detected in one-third of urine samples analysed for speciated As (n=29), predominantly as MMA, which is not affected by fish consumption. A total of 24% of these 29 participants (n=7) had levels exceeding the environmental exposure limit of 6.4 µg/g creatinine.12 Median As(tox) levels and the percentage of samples in which As(tox) was detected were, however, substantially lower than those measured in CCA-treatment plant workers,3 other As-exposed industrial workers,13,14 and persons exposed to As-contaminated drinking water15,16. In areas with higher than normal As levels in the water and soil, Asi levels in foods such as flour and rice are usually also elevated.17.
In addition to the As(tox) results, a high percentage (12%) of participants also had levels that exceeded the environmental exposure limit for Cr, which could indicate that participants were exposed to CCA. Other possible sources of Cr, including occupational and environmental exposure from industry, amongst these participants are unlikely, but Cr exposure from landfills and from tobacco smoke is possible.
It is difficult to comment on the long-term health effects resulting from exposure to As and Cr at the levels measured in this study, as few epidemiological studies could be found that have investigated health effects at these levels of exposure.18 The few studies done amongst CCA-exposed workers in a wood-preserving plant reported no adverse health effects amongst workers, but the number of participants was small. 2 As mentioned before, As and Cr are associated with a number of cancer-related and non-cancer-related health effects (Table 4). Health effects resulting from combined exposure to As and Cr may be additive, but there is no evidence of any interaction between these metals.2 Interestingly, there was a high prevalence of respiratory, diarrhoeal and skin problems reported amongst participants, which requires more detailed epidemiological investigation; these symptoms might be a result of other environmental exposures in the communities and the self-reports are too crude a measure of these health problems. The self-reports were included in this study merely to provide preliminary evidence of health effects as the aim of the study was to determine the level of exposure of the participants to CCA.
Comparisons between areas and caterers/residents
The higher levels of metals measured in the urine of participants from Stellenbosch is consistent with the higher wood usage reported in the area and also with the higher level of treated wood used in the area, as found in the previous study.1 However, the differences in urinary levels of the metals were not as substantial as the differences in wood usage. It is unlikely that other exposure to Cr and As not measured in the study, such as exposure to leather products, paints, cement, mortar, anti-corrosives, electroplating, tanning and chromium production, confounded these results.19 The self-reports of wood usage may not have been accurate, which may have impacted the results.
The consistently higher levels of metals in the urine of household residents was consistent with the higher wood usage reported by these participants. Although the percentage of residents that ate fish in the preceeding 3 days was higher than that of caterers, which probably raised As(tot) levels amongst residents, this effect was accounted for in the analysis.
Limitations
Apart from the limitations already mentioned, additional limitations were the lack of a control group of participants that did not use wood, a low sample size with As(tox) measured in only 37% of participants and the cross-sectional design of the study. An appropriately higher sample size would have produced statistically significant associations in the study and a longitudinal design would have enabled more accurate monitoring of levels of metals in participants when they were using and not using treated wood.
Conclusions
Household residents and food caterers in the informal sector in the Cape Town region were subjected to exposures resulting in the absorption of Cr and inorganic As at levels higher than persons regarded as unexposed, although their levels were substantially lower than those of highly exposed persons. These exposures could be a significant contributing factor to the health problems in these communities, which represent a major public health problem in developing countries. Household residents use as much or more wood than food caterers and wood usage appears to be higher in peri-urban areas. It is unclear if the absorption of Cr and inorganic As is as a result of exposure to CCA-treated wood. Further analysis of the relationship between wood usage and urinary levels of Cr, Cu and As will be conducted and presented in another paper. A larger study with a longitudinal design will more accurately investigate this question. Environmental monitoring of Cr, Cu and As in these areas is important. Interventions such as awareness and educational programmes in these communities are required by industry and government to prevent the use of treated wood in these informal settlements. A study investigating the impact of such interventions on urinary levels of Cr, Cu and As amongst these informal communities would also provide important insight on the extent that these toxic metals are absorbed through exposure to CCA-treated wood.
Acknowledgements
We thank the UCT Vice-Chancellor's Strategic Funding, UCT Research Committee and the National Research Foundation for their financial support of this study. We also thank the participants and community development workers from Langa and Kayamandi (Stellenbosch) for arranging access to the study areas.
Authors' contributions
M.A.D. was the principal investigator and senior author, S.N. assisted with all aspects of the study and is the first author of the manuscript and A.A. was the project coordinator and assisted with the analysis and write-up.
References
1. Niyobuhungiro R, Naidoo S, Dalvie MA, Von Blottnitz H. Occurrence of CCA-treated timber in caterers' fuelwood stocks in the Cape Town region. S Afr J Sci. 2013;109(1/2), Art. #1015, 5 pages. http://dx.doi.org/10.1590/sajs.2013/1015 [ Links ]
2. Chou AS, Colman BJ, Tylendaa C, De Rosa C. Chemical-specific health consultation for chromated copper arsenate chemical mixture: Port of Djibouti. Toxicol Ind Health. 2007;23:183-208. http://dx.doi.org/10.1177/0748233707076810
3. Cocker J, Morton J, Warren N, Wheeler JP Garrod ANI. Biomonitoring for chromium and arsenic in timber treatment plant workers exposed to CCA wood preservatives. Ann Occup Hyg. 2006;50:517-525. http://dx.doi.org/10.1093/annhyg/mel009
4. Aposhian HV, Aposhian MM. Arsenic toxicology: Five questions. Chem Res Toxicol. 2006;19:1-15. http://dx.doi.org/10.1021/tx050106d
5. Cullen WR, Reimer KJ. Arsenic speciation in the environment. Chem Rev. 1989;89:713-764. http://dx.doi.org/10.1021/cr00094a002
6. Francesconi KA, Kuehnelt D. Determination of arsenic species: A critical review of methods and applications. Analyst. 2004;129:373-395. http://dx.doi.org/10.1039/b401321m
7. Lintschinger J, Schramel P Hatalak-Rauscher A, Wendler I, Michalke B. A new method for the analysis of arsenic species in urine by HPLC-ICP-MS. Fresenius J Anal Chem. 1998;362:313-318. http://dx.doi.org/10.1007/s002160051080
8. World Health Organization. Biological monitoring of chemical exposure in the workplace [document on the Internet]. c1996 [cited 2012 June 05]. Available from: http://whqlibdoc.who.int/hq/1996/WHO_HPR_OCH_96.1.pdf. [ Links ]
9. Stata statistical software. Release 8.0. College Station, TX: Stata Corporation; 2003. [ Links ]
10. WMA. Declaration of Helsinki - Proposed International Guidelines for Biomedical Research involving Human subjects [document on the Internet]. c2008 [cited 2012 June 05]. Available from: http://www.wma.net/en/30publications/10policies/b3/17c.pdf [ Links ]
11. Shah AQ, Kazi TG, Arain MB. Accumulation of arsenic in different freshwater fish species - Potential contribution to high arsenic intakes. J Food Chem. 2009;112:520-524. http://dx.doi.org/10.1016/j.foodchem.2008.05.095
12. Hays SM, Aylward LL, Gagné M, Nong A, Krishnan K. Biomonitoring equivalents for inorganic arsenic. Regul Toxicol Pharm. 2010;58:1-9. http://dx.doi.org/10.1016/j.yrtph.2010.06.002
13. Hakala E, Pvy L. Assessment of exposure to inorganic arsenic by determining the arsenic species excreted in urine. Toxicol Lett. 1995;77:249-258. http://dx.doi.org/10.1016/0378-4274(95)03304-1
14. Vimercati L, Carrus A, Sciannamblo G. A study of factors influencing urinary arsenic excretion in exposed workers. Int J Environ Heal R. 2009;19(5):369-377. http://dx.doi.org/10.1080/09603120903079349
15. Hsueh Y Hsu M, Chiou H, Yang M, Huang C, Chen C. Urinary arsenic speciation in subjects with or without restriction from seafood dietary intake. Toxicol Lett. 2002;133:83-91. http://dx.doi.org/10.1016/S0378-4274(02)00087-5 [ Links ]
16. Fillol C, Dor F, Labat L. Urinary arsenic concentrations and speciation in residents living in an area with naturally contaminated soils. Sci Total Environ. 2010;408:1190-1194. http://dx.doi.org/10.1016/j.scitotenv.2009.11.046
17. Del Razo LM, Garcia-Vargar GG, Garcia-Salcedo J. Arsenic levels in cooked food and assessment of adult dietary intake of arsenic in the region Lagunera, Mexico. Food Chem Toxicol. 2002;40:1423-1431. http://dx.doi.org/10.1016/S0278-6915(02)00074-1
18. Solo-Gabriele HM, Townsend TG, Messick B, Calitu V. Department of Civil, Architectural, and Environmental Engineering characteristics of chromated copper arsenate-treated wood ash. J Hazard Mater. 2002;B89:213-232. http://dx.doi.org/10.1016/S0304-3894(01)00311-9
19. Basketter D, Horev L, Slodovnik D, Merimes S, Trattner A, Ingber A. Investigation of the threshold for allergic reactivity to chromium. Contact Dermatitis. 2000;44(2):70-74. http://dx.doi.org/10.1034/j.1600-0536.2001.440202.x
20. ATSDR. Toxicological profile for arsenic [document on the Internet]. Atlanta, GA: ATSDR, US Department of Health and Human Services. c2007 [cited 2010 Aug 09]. Available from: http://www.atsdr.cdc.gov/toxprofiles/tp2.pdf [ Links ]
21. ATSDR. Toxicological profile for chromium [document on the Internet]. Atlanta, GA: ATSDR, US Department of Health and Human Services. c2003 [cited 2010 Aug 19]. Available from: http://www.atsdr.cdc.gov/toxprofiles/tp7.pdf. [ Links ]
22. ATSDR. Toxicological profile for copper (update) [document on the Internet]. Atlanta, GA: ATSDR, US Department of Health and Human Services. c2004 [cited 2010 Aug 19]. Available from: http://www.atsdr.cdc.gov/toxprofiles/tp132.pdf [ Links ]
23. Ellingsen DG, Horn N, Aaseth J. Handbook on the toxicology of metals. 3rd ed. Burlington, MA: Academic Press; 2007. p. 529-546. http://dx.doi.org/10.1016/B978-012369413-3/50081-1 [ Links ]
24. Lauwerys RR, Hoet P. Industrial chemical exposure: Guidelines for biological monitoring. 2nd ed. Boca Raton, FL: Lewis Publishers; 1993. [ Links ]
25. Kiilunen M, Jarvisalo J, Makitie O, Aitio A. Analysis, storage stability and reference values for urinary chromium and nickel. Int Arch Occup Environ Health. 1987;59:43-50. http://dx.doi.org/10.1007/BF00377677
 Correspondence:
Correspondence:
Mohamed Aqiel Dalvie
Centre for Occupational and Environmental Health Research
School of Public Health and Family Medicine
University of Cape Town
Faculty of Health Sciences
Anzio Road, Observatory 7925, South Africa
aqiel.dalvie@uct.ac.za
Received: 17 Oct. 2012
Revised: 06 Feb. 2013
Accepted: 08 Feb. 2013


{kind=link}
{kind=link}
{kind=link}
{kind=link}