Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Science
versión On-line ISSN 1996-7489
versión impresa ISSN 0038-2353
S. Afr. j. sci. vol.109 no.5-6 Pretoria ene. 2013
COMMENTARIES
What is the ideal ratio of categories of nurses for the South African public health system?
Leana R. UysI; Hester C. KlopperII, III
IProfessor Emeritus, School of Nursing and Public Health, University of KwaZulu-Natal, Durban, South Africa
IIExtraordinary Professor, School of Nursing Science, North-West University, Potchefstroom, South Africa
IIIFUNDISA, Pretoria, South Africa
Keywords: nurses; workforce; categories; ratio; specialists
Context and importance of the problem
In South Africa we have four categories of nurses according to the qualifications framework currently in use: (1) enrolled nursing auxiliaries (ENA) who train for 1 year, (2) enrolled nurses (EN) who train for 2 years, (3) registered nurses/midwives (RN/M) who train for 4 years and (4) specialist registered nurses/midwives (SRN/M) who have 1 or 2 years post-RN/M training. According to 2010 statistics of the South African Nursing Council, in 2006 South Africa had a ratio of 3:2:1:4 for ENA:EN:RN/M:SRN/M. Each of these categories has a circumscribed role and a mandated scope of practice in the service, which are not interchangeable. Because South Africa has a nurse-based health system,1 workforce planners should have a clear idea of the ratio of each category of nurse needed to serve each level of the health service. Without agreed upon evidence-based ratios, it would be impossible to plan the nursing workforce for the country.
At the Nursing Summit of April 2011, the Minister of Health repeatedly challenged the nurses of South Africa to present a ratio of registered nurses to other categories to enable the planning of the human resources for health for the country. In March 2011, a draft document was produced by the Department of Health entitled 'Planning for Key Health Professional Categories' in which the same issue was highlighted as a problem that needs to be addressed before the workforce can be reliably planned.
Assumptions
We have based this commentary on the current nursing qualification framework, and not on the new proposed framework, which will take at least 5 years to produce its first group of nurses. We refer to the nursing qualification and not to the National Qualifications Framework which was developed according to the National Qualifications Framework Act 67 of 2008 as amended. Although much may not change, some norms will change when the new framework is implemented. We also assume that the ratio of categories will have to be reviewed in 5 years and treat registered nurses and midwives as a single group of registered professionals (RN/Ms).
The policy issues
Without evidence-based ratios, ENs and ENAs may be overproduced and overutilised. The training of ENs and ENAs is significantly better distributed over the country and is easier and less costly to offer than the training of RN/Ms and SRN/Ms. ENs and ENAs are also less expensive to employ. Another scenario is that RNMs may be underproduced and their employment restricted. Internationally, the duration of training of RN/Ms is 3 or 4 years after 12 years of school. Training for RNMs is usually situated in the higher education system and centralised in urban areas, which makes it less accessible and more expensive than that for the ENs and ENAs. It is also more expensive to employ RN/Ms than ENs and ENAs. Finally, SRN/Ms may be underproduced and incorrectly utilised because many policy documents dealing with the nursing workforce do not address the issue of specialist nurses, but see all RN/Ms as equal. Such a lack of differentiation does not reflect the reality of any of the levels of service. For instance, in the primary health care service nurses with specialist training in diagnosis, treatment and care are seen as essential, while in Critical Care Units, nurses prepared in this specialty are essential.
The three-dimensional model for workforce planning2 includes: planning (designing patterns of staff mixes and utilisation in line with strategic policy goals), production (all aspects of basic and post-basic education and training) and management (employment and utilisation). The most important point made by this model's first dimension is that the planning of the workforce cannot be based on international norms, but should be based on the policy goals. Because these goals are different for each country, they should be developed by each country based on their own policies.
Summary of analysis and research
With regard to RN/Ms vs ENs or ENAs (Table 1), most of the research internationally is about nurse:patient ratios and many states in the USA have legislated a nurse:patient (RN:patient) ratio for hospitals. The US Joint Commission on Accreditation of Healthcare Organizations stated that 'Current mandated ratios do not address other critical issues, such as nurse competency, skill mix in relation to patient acuity and ancillary staff support'3. It is the issue of skills mix and ancillary support that this policy brief is trying to address. Studies have also shown that patients in hospitals with better educated nurses (20% more with a Bachelor of Nursing degree) have an 8% lower risk of dying in hospital.4 Both medical and surgical patients in hospitals had better outcomes if the proportion of RNs caring for them was higher.5 An additional RN hour per patient day was associated with a 3% lower fall rate in ICUs, and an additional licensed practical nurse or nursing auxiliary hour was associated with a 2-4% higher fall rate in non-ICU settings.6 Higher rates of RN staffing were associated with a 3-12% reduction in adverse outcomes, depending on the outcome.7 Not all countries have a range of nurse categories. In Kenya there are only three categories of nurses: EN, RN and RSN. ENs are being phased out. Kenya's staffing norms are therefore for RNs only. They have calculated nurse staffing norms for different levels of care, but have not made provision for specialist nurse norms.8 In South Africa, the norms of a specific service authority play a role. For instance, the Department of Minerals and Energy Affairs requires that every nurse working in a primary health care clinic of the mining companies be qualified in diagnosis, treatment and care, as well as have a dispensing licence.

Fewer studies are available with regard to RN/M and SRN/M ratios. According to the Australian College of Critical Care Nurses, ICUs must have a minimum of 50% qualified critical care nurses, as well as a nursing manager for each unit and a clinical nurse educator for every 50 nurses in ICU.9 A study by Kendall-Gallagher et al.10 in surgical inpatient units found that certification as a specialist nurse made no difference to outcomes in the absence of a degree in nursing. However, having a degree in nursing significantly decreased mortality and failure to rescue rates. A 10% increase in the proportion of nurses with BN degrees decreased 30-day mortality from 6% to 2%. In the suggested staffing norms for hospital units developed by the South African Department of Health,11 the need for specialist nurses are recognised for ICU units only, despite comprehensive recognition for the need for specialist doctors, and the provision of additional qualifications for nurses in areas such as paediatrics and geriatrics.
Recommendations
Many details are yet to be resolved to develop national ratio norms. However, based on evidence from the literature, we provide some recommendations:
• It is essential that the need for specialist nurses be part of the detailed planning, as is the case for Medicine. An RN/M is prepared as a generalist with a wide range of relatively superficial competence in order to render a generalist level of care. A SRN/M is a professional person who has been prepared beyond the level of a generalist and is authorised to practise as a specialist in a field of nursing or midwifery (adapted from ICN12 ).
• Specialist organisations should be approached to describe the ratio of their specialty to other nurses in different service levels.
• The South African Nursing Council's registers for nurse specialists should be updated and historical qualifications, such as 'fever nurses' and 'gas and anaesthetic nurses', should be abolished so that only practising nurse specialists are included. Up-to-date registers would allow for more accurate planning in the future.
• Although we currently do not have a health policy based workforce plan, evidence supports the importance of high numbers of RN/Ms, trained through a comprehensive 4-year qualification (which includes general, community health, and psychiatric nursing and midwifery), in the system to ensure positive outcomes. There should therefore be a focus on increasing the production of RN/Ms and not increasing the production of ENAs and ENs without evidence that increased numbers are necessary.
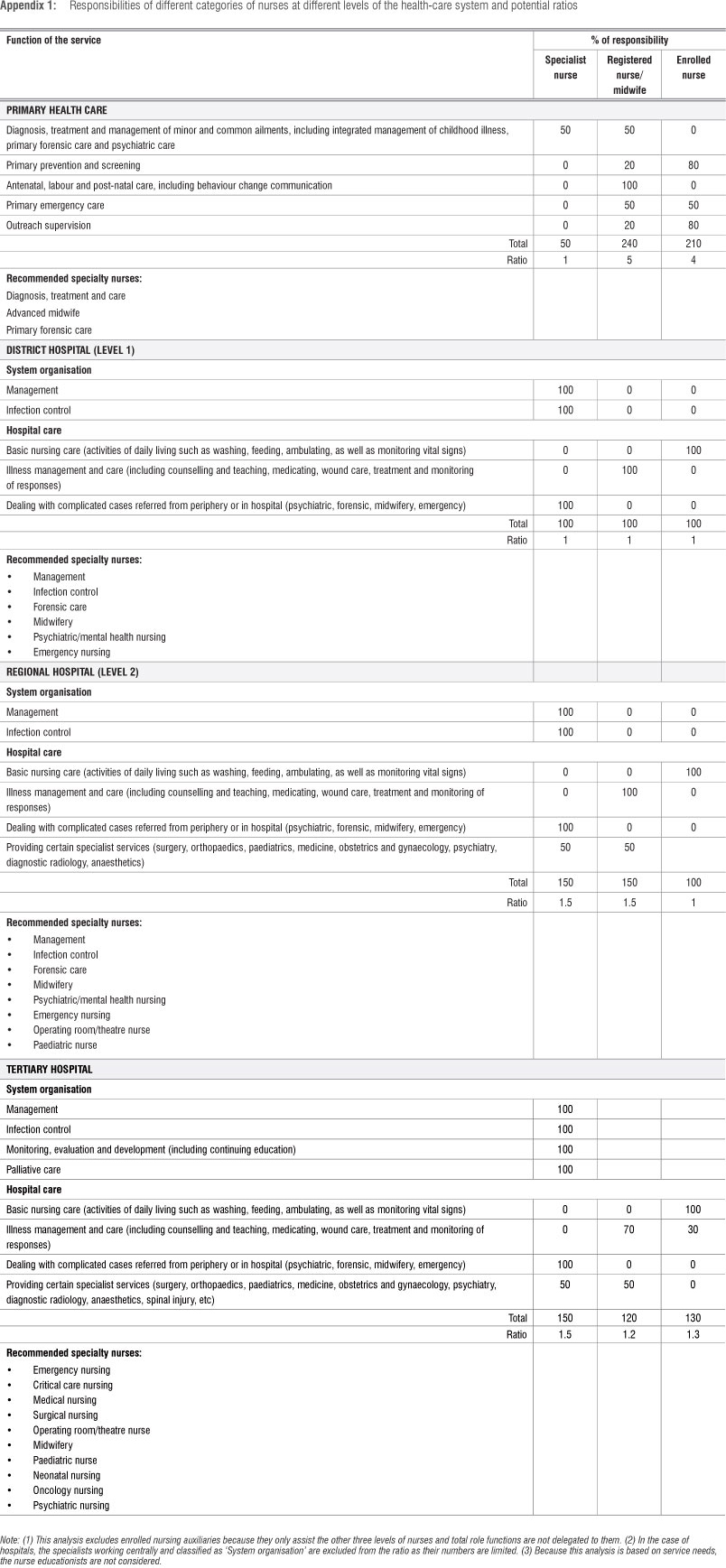
• Different ratios of nursing categories will be essential for different levels of the health-care system, such as primary health care (clinics and centres), district hospitals, regional hospitals and tertiary or specialist hospitals. The ideology behind a first estimate of these ratios is provided in Appendix 1. According to this calculation, the recommended ratios are summarised in Table 2. To calculate the overall ratio for the country, the size of each of these components would need to be calculated.
•The ratio of all categories of nurses to patients in different health-care settings also needs to be researched, as this too will influence the overall ratios of nurses.

References
1. Health Systems Trust. Human resources for health 2030 [document on the Internet]. c2011 [cited 2013 Jan 15]. Available from: www.hst.org.za/publications/humanresr [ Links ]
2. Scott C. Setting safe nurse staffing levels. London: RCN Institute; 2003. [ Links ]
3. Joint Commission on Accreditation of Healthcare Organizations (JCAHO). Health care at the crossroads: Strategies for addressing the evolving nursing crisis. Washington: JCAHO; 2005. [ Links ]
4. Aiken L, Clarke S, Sloane D, Lake E, Cheney T. Effects of hospital care environment on patient mortality and nurse outcomes. J Nurs Admin. 2008;38(5):223-229. http://dx.doi.org/10.1097/01.NNA.0000312773.42352.d7
5. Needleman J, Bauerhaus P Potter V Mattke S, Stewart M, Zelevinsky K. Nurse-staffing levels and patient outcomes in hospitals. Final report for Health Resources and Services Administration. Contract No. 230-99-0021. Boston, MA: Harvard School of Public Health; 2001. [ Links ]
6. Lake ET, Shang J, Klaus S, Dunton NE. Patient falls: Association with hospital Magnet status and nursing unit staffing. Res Nurs Health. 2010;33(5):413-425. http://dx.doi.org/10.1002/nur.20399
7. Cho SH, Ketefian S, Barkauskas VH, Smith DG. The effects of nurse staffing on adverse outcomes, morbidity, mortality, and medical costs. Nurs Res. 2003;52(2):71-79. http://dx.doi.org/10.1097/00006199-200303000-00003
8. Health Sector Service Delivery Team. Norms and standards for health service delivery. Nairobi: Ministry of Health; 2006. [ Links ]
9. Editor. Position statement on intensive care nursing staffing. Aust Crit Care. 2002;15(1):6-7. http://dx.doi.org/10.1016/S1036-7314(02)80037-6 [ Links ]
10. Kendall-Gallagher D, Aiken LH, Sloane DM, Cimiotti JP. Nurse specialty certification, inpatient mortality and failure to rescue. J Nurs Scholarship. 2011;43(2):188-194. http://dx.doi.org/10.1111/j.1547-5069.2011.01391.x
11. Department of Health. Strategic framework for the modernization of tertiary hospital services. Pretoria: Department of Health; 2003. Available from: http://www,doh.gov.za/mts/docs/framework01.pdf [ Links ]
12. ICN. Nurse practitioner/advanced practice nurse: Definition and characteristics. ICN Factsheet Advanced Practice [document on the Internet]. c2010 [cited 2013 Jan 14]. Available from: www.icn.ch/publications/fact_sheets [ Links ]
 Correspondence:
Correspondence:
Leana Uys
PO Box 577, St Francis Bay 6312, South Africa
Email: UYS@ukzn.ac.za