










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Science
versión On-line ISSN 1996-7489
versión impresa ISSN 0038-2353
S. Afr. j. sci. vol.108 no.11-12 Pretoria ene. 2012
REVIEW ARTICLE
The impact of solar ultraviolet radiation on human health in sub-Saharan Africa
Caradee Y. WrightI; Mary NorvalII; Beverley SummersIII; Lester DavidsIV; Gerrie CoetzeeV; Matthew O. OriowoVI
IModelling and Environmental Health Research Group, Council for Scientific and Industrial Research, Natural Resources and the Environment, Pretoria, South Africa
IIBiomedical Sciences, University of Edinburgh Medical School, Edinburgh, Scotland
IIIDepartment of Pharmacy / Photobiology Laboratory, University of Limpopo, Polokwane, South Africa
IVDepartment of Human Biology, University of Cape Town Medical School, Cape Town, South Africa
VSouth African Weather Services, Pretoria, South Africa
VIDepartment of Optometry, Faculty of Health Sciences, University of Limpopo, Polokwane, South Africa
ABSTRACT
Photoprotection messages and 'SunSmart' programmes exist mainly to prevent skin cancers and, more recently, to encourage adequate personal sun exposure to elicit a vitamin D response for healthy bone and immune systems. Several developed countries maintain intensive research networks and monitor solar UV radiation to support awareness campaigns and intervention development. The situation is different in sub-Saharan Africa. Adequate empirical evidence of the impact of solar UV radiation on human health, even for melanomas and cataracts, is lacking, and is overshadowed by other factors such as communicable diseases, especially HIV, AIDS and tuberculosis. In addition, the established photoprotection messages used in developed countries have been adopted and implemented in a limited number of sub-Saharan countries but with minimal understanding of local conditions and behaviours. In this review, we consider the current evidence for sun-related effects on human health in sub-Saharan Africa, summarise published research and identify key issues. Data on the prevalence of human diseases affected by solar UV radiation in all subpopulations are not generally available, financial support is insufficient and the infrastructure to address these and other related topics is inadequate. Despite these limitations, considerable progress may be made regarding the management of solar UV radiation related health outcomes in sub-Saharan Africa, provided researchers collaborate and resources are allocated appropriately.
Introduction
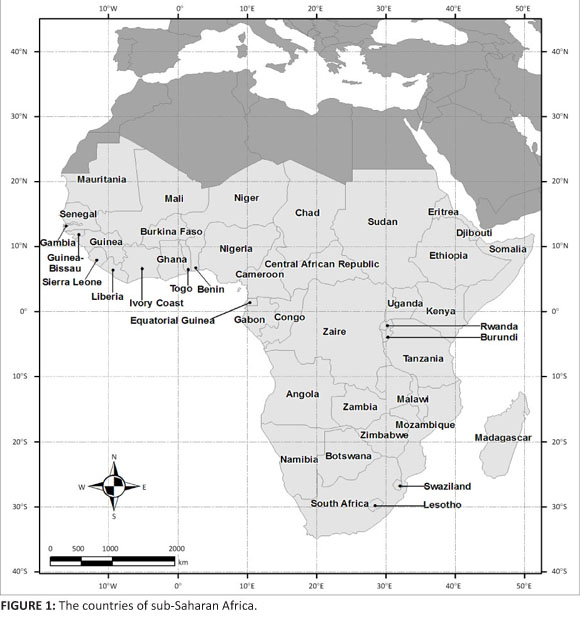
Sub-Saharan Africa consists of 43 countries south of the Sahara (Figure 1). This area spans latitudes 13°N to 33°S with an average annual daytime temperature of 21 °C. The UV Index is often higher than 10 (extreme) and rarely drops below 7, except at high altitudes and towards the tip of South Africa in the winter months (June, July and August). The land varies from equatorial rainforest to dry woodland, savannah, grassland and mountain grassland.
The major beneficial outcome of solar ultraviolet radiation (UVR) exposure on human health lies in the endogenous production of vitamin D, while adverse outcomes of excess exposure include skin cancers and eye diseases.1 Extensive research and public health interventions relating to the consequences of solar UVR on human health have been carried out in many developed countries; however, the same is not true for sub-Saharan Africa. Limited information suggests health and exposure risks do exist in this area of the world, although accessing published and verified data is a challenge, because most sub-Saharan countries do not have operational health information systems or ground-based networks to monitor solar UVR. The aim of this review is to broaden the understanding of the effects of solar UVR on human health in sub-Saharan Africa by considering an update of relevant health outcomes and by documenting public perceptions and interventions.
Search strategy
A systematic approach was used to identify key published resources of substance and appropriate scientific merit. Databases searched were African Journals Online, SABINET, Academic Search Premier, Pubmed, SciELO, Medline, JSTOR, Web of Science and Scopus. Keywords entered were "solar UV radiation" AND health AND [country]; "sun exposure" AND health AND [country]; sunburn AND [country]; "skin cancer" AND [country]; albinism AND "sun exposure" AND [country]; [range of sun-related eye diseases] AND "sun exposure" AND [country]; "sun protection" AND [country]; "sun behaviour" AND [country]; and "sunsmart awareness programme" AND [country]. Reference lists of collected articles including reports of the World Health Organization (WHO) were examined. Using the same keywords, Google was searched for grey literature, a particularly important source in the African context. The websites of national departments of health and cancer associations were investigated for information on 'SunSmart' programmes and sun-related health statistics.
Results
Skin cancers
Sun exposure is the major environmental risk factor for melanoma and for the non-melanoma skin cancers (NMSCs), basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). The lifetime risk of these tumours is low in those with black skin and highest in those with fair skin, estimated at a difference of up to 60-fold. There are other major differences depending on skin colour.2 While BCCs represent about 80% of cutaneous tumours in fair-skinned people, they are the least common of the skin tumours in deeply pigmented people, in whom SCCs are the most frequent. In dark-skinned individuals, SCCs occur most often on the lower limbs (developing from antecedent lesions such as ulcerations, burns and scars), followed by the head and neck. In fair-skinned people, SCCs are found almost entirely on the most sun-exposed areas of the body, such as the face and ears. Unlike the situation in individuals with fair skin, the majority of melanomas in black skin occur on a lower extremity, particularly on the sole of the foot, a body site with little pigmentation.
The occurrence of NMSCs in sub-Saharan Africa is rarely monitored. However, the UVR-attributable disease burden caused by SCCs and BCCs for some of the countries in this region was calculated for the year 2000 using three levels of skin pigmentation, models for global assessment and country-specific population-weighted average daily ambient UVR.3,4 Using actual results, the annual incidence of SCC in Black individuals was estimated as 1 in 100 000 in a township near Soweto, Johannesburg in 1966-1975,5 whereas the age-standardised annual incidence of BCC in the Netherlands is currently more than 140 in 100 000. A study in Kano, Nigeria revealed that 6.3% of all cancers in female individuals and 9.9% in male individuals were NMSCs in 1995-2004.6 One recent report based on rural hospitals in Kenya found that 44% of all cutaneous malignancies were SCCs and 7% were BCCs.7
For melanoma, which accounts for more than 80% of skin cancer deaths, there are also few figures available regarding incidence and prevalence for sub-Saharan Africa, although, as for the NMSCs, the UV-attributable disease burden from this tumour was calculated as approximately 5100 deaths for the year 2000 in this area of the world.4 For South Africa, in 2001 - one of the last years for which statistics are currently available - the National Cancer Registry recorded an age-standardised incidence rate per 100 000 for melanoma of 1.1 for Black males, 1.5 for Black females, 22.5 for White males and 17.4 for White females.8 The incidence has risen since then and the South African Cape region was estimated in 2009 to have the highest incidence of melanoma in the world at 69 new cases per 100 000 White individuals9 (Australia has 65 per 100 000).
Accurate figures on the prevalence of skin cancers in all subpopulations in sub-Saharan Africa are required, especially to record any changes in incidence. Such data are needed to inform the public regarding photoprotection and to improve clinical awareness.
Melasma
Melasma is an uneven hyperpigmentation which appears as dark, macular, pigmented patches on the face.10 The cause of melasma is complex - genetic, hormonal, therapy and lifestyle-related contributions are implicated, as is sun exposure. For example, 51% of patients reported sun exposure as a triggering factor and 84% reported sun exposure as an aggravating factor in a study based in Tunisia, with a high lifetime sun exposure increasing the risk of severe melasma threefold.11 Melasma represents a significant problem in sub-Saharan Africa, primarily because of its impact on quality of life. It is suggested to have a significant psycho-emotional effect on women.12 While different scales, including the Melasma Quality of Life scale, have been devised, these have not been tailored effectively for the cultural needs of multiethnic subpopulations.
Few statistics are available for sub-Saharan Africa regarding the prevalence of other skin disorders induced by either acute sun exposure, such as sunburn, or by chronic sun exposure, such as photoageing and actinic keratoses, the latter recognised as premalignant lesions.
Oculocutaneous albinism
Oculocutaneous albinism (OCA) is a genetically inherited, autosomal recessive condition characterised by hypopigmentation of the skin, hair and eyes as a result of a lack of, or reduced, melanin. There are many people living with OCA in sub-Saharan Africa; estimates indicate a prevalence of 1 in 4728 in Zimbabwe, 1 in 3900 in South Africa and as high as 1 in 1000 in the Tonga tribe in Zimbabwe.13,14 Individuals with OCA are at increased risk from the adverse effects of sun exposure, such as extreme sun sensitivity and photophobia. SCCs of the neck and head are the most common cutaneous tumours seen in African patients with OCA,15 with melanomas occurring rarely.14
Ophthalmohelioses
There is a range of eye diseases associated with sunlight exposure - ophthalmohelioses. These diseases include photoconjunctivitis, photokeratitis and activation of ocular herpes simplex virus following acute exposure to solar UVR, and NMSCs of the lid and conjunctiva, ocular melanoma, pinguecula (local degeneration of conjunctiva), pterygium (inflammation, proliferation and invasive growth on conjunctiva and cornea), climatic droplet keratopathy (epithelial degeneration), age-related cataracts and possibly age-related macular degeneration following chronic exposure to solar UVR.
Few data are available for sub-Saharan Africa that estimate the scale of health problems caused by these ophthalmohelioses, although it is recognised that this area has the highest regional burden of blindness at 20% of the world's blindness and only 11% of the world's population.16 Indeed, 1% of Africans are blind.17 Cataracts account for approximately 50% of the cases of blindness worldwide. The evidence to link cataract development with sun exposure is strongest for cortical cataracts, the form found in about 33% of subjects with cataracts in one survey based in rural Tanzania.18 In the first population-based study in an African setting (Nigeria), it was reported that there were 5000 per million population with functional low vision and 340 per million blind.19 One-quarter of the functional low vision cases were as a result of corneal opacity and about 3% were as a result of pterygium. The prevalence of functional low vision was highest in the northern part of Nigeria, which is drier and sunnier than the south. Earlier studies in South Africa showed an annual incidence of cataract blindness of 0.14% with a prevalence of 0.6% in a rural population in KwaZulu-Natal,20 and a prevalence of 0.3% in rural northern Transvaal.21
Figures for the incidence and prevalence of corneal and other external eye diseases in sub-Saharan Africa are not generally available for recent years, although such disorders are recognised to be very common. For example, corneal diseases, the majority being pterygium and climatic droplet keratopathy, were found in more than 20% of a mixed race community in the north-western Cape (South Africa),22 and pterygium represented 9% of all new cases at an eye clinic in Ibadan (Nigeria)23 and 8% of ocular problems in adults aged 18-49 in rural Nigeria, most of which occurred in outdoor workers.24
Concern has been expressed recently that sub-Saharan Africa is not on track to achieve the main goal of 'VISION 2020: The Right to Sight' - to eliminate avoidable blindness by 2020.25 This imminent failure has been attributed to the lack of eye care teams, staff development, infrastructure and community programmes.25 In this context, it is disappointing to note that the national target for cataract surgery in South Africa was downgraded in 2010 from 2000 to 1500 per million population, when at least 2000 per million per year is required to eliminate cataract blindness.26 Guidance for the general public about protecting the eye by wearing hats with wide brims or sunglasses that meet an appropriate standard for solar UVR protection would be very helpful in reducing the risk of ophthalmohelioses.
Immunosuppression and effects on diseases
UV-induced downregulation of immunity to a variety of antigens has been demonstrated in humans. The pathways involved are complex,27 and may involve vitamin D which has many immunoregulatory properties.28 The majority of vitamin D in most people is produced as a result of sun exposure. The vitamin D status of almost all populations in sub-Saharan Africa is unknown but, from the incomplete data available, is lower in South Africa compared with the tropical African countries.29 However, even near the equator, there can be a high rate of vitamin D deficiency, as demonstrated in adults in Ethiopia (10°N)30 and Guinea-Bissau (12°N).31 Nutritional rickets remains prevalent in some tropical countries despite good sunshine exposure, although this may be as a result of a low calcium intake rather than a deficiency in vitamin D.32
From many studies covering a variety of approaches, it can be concluded that UVR and/or vitamin D have the potential to protect against some inflammatory diseases and autoimmune diseases, such as multiple sclerosis, while decreasing the immune surveillance against skin tumours and infectious diseases. Each of these categories is discussed briefly below.
In the context of diseases in sub-Saharan Africa, the lightsensitive dermatoses (e.g. polymorphic light eruption where there is a lack of immunosuppression following sun exposure with development of an allergic response) do not constitute a major health problem as they are much less common in people with pigmented skin and occur rarely in regions near the equator.33 Similarly, multiple sclerosis is uncommon in the indigenous Black, Coloured or Indian people of Africa. In southern Africa, there is a relatively high prevalence of multiple sclerosis in White migrants from Europe with a lower prevalence in White African-born people, possibly as a result of the protective effect of early exposure to high levels of solar UVR.34
UVR not only causes mutations but also downregulates immunity, an effect which is recognised to be critical in the development of skin tumours. For the same dose of UVR, fair-skinned people exhibit more DNA damage,35 a higher production of immune mediators and a higher degree of immunosuppression36 than those with darker skins. This difference is likely to contribute to the increased susceptibility of individuals with fair skin to develop skin cancers compared with individuals with more pigmented skin.
It is unclear whether UV-induced immunosuppression can affect the course of human infectious diseases, apart from triggering the reactivation from latency of herpes simplex virus. Some human infections exhibit a strong seasonal incidence. For example, influenza is highly seasonal in southern Africa with the peak incidence occurring in the drier cooler winter months: the seasonality becomes less pronounced with closeness to the equator.37 This pattern is also seen in other parts of the world, and has been attributed to lower vitamin D levels (and thus less effective innate immunity) in the winter compared with the summer in countries outside the tropics. Tuberculosis presents a major public health issue in sub-Saharan Africa with Nigeria having the fourth largest tuberculosis burden in the world and South Africa the fifth largest. Many of the new cases of tuberculosis are co-infections with HIV; currently sub-Saharan Africa accounts for 79% of the worldwide HIV-tuberculosis burden. From a survey of studies conducted in 11 countries or regions around the world (including South Africa), a seasonal pattern of tuberculosis is indicated with a peak in the spring and summer months.38 This pattern has been explained by low vitamin D levels in the winter leading to less effective control of microbial growth. Hypovitaminosis D is highly prevalent in tuberculosis patients and is associated with an increased risk of disease progression, although it is not known if the low level is a symptom or is causal.31 Recent research has considered whether vitamin D prevents reactivation of tuberculosis.39 With regard to HIV, while some observations support a role for UVR in altering the interaction of the virus with the host, clinical and epidemiological reports have not demonstrated that exposure to sunlight changes the course of the disease.40 Many HIV-infected people are vitamin D deficient but the impact of this deficiency on disease progression is unknown and should be investigated.
Vaccination represents a major public health strategy in sub-Saharan Africa in attempts to control common infections, particularly in childhood. The potential of UVR to decrease the efficacy of vaccination by downregulating immunity has not been rigorously assessed for human vaccines although there are reports indicating that a less effective immune response is induced if the vaccine is administered in the summer compared with the winter, and in tropical compared with temperate regions.41 Perhaps of most relevance in the context of sub-Saharan Africa is finding that the protection against tuberculosis following vaccination correlates positively with distance from the equator.42 More severe UV-induced immunosuppression nearer to the equator as a result of the higher sun intensity could account for this result.
Sun-related exposure, protection, perceptions and awareness
The people of sub-Saharan Africa are genetically diverse: migrants from other countries have settled here since the Greeks, Romans and Arabs 3000 years ago, Europeans since the 1600s and Asians since the 1800s. If this heterogeneity is added to the range of environments and social conditions in sub-Saharan Africa, it can be anticipated that solar UVR will not have straightforward health outcomes. In addition, the only country to possess solar UV monitoring instruments in this region is South Africa, where a four-station network has been in operation since the early 1990s. The network aims to provide measured data to the media daily to inform the public regarding times of intense solar irradiation.
Personal sun exposure studies in sub-Saharan Africa are nonexistent, inaccessible or sparsely documented. One of the few studies, based in Durban (South Africa), emphasised the risk of sunburn and NMSC for children and outdoor workers.43 Schoolchildren in this city experienced a mean total daily solar exposure of two Standard Erythemal Doses, with boys experiencing greater sun exposure than girls and outdoor physical activity being the most important determinant of sun exposure.
Knowledge about sun protection is not widespread in sub-Saharan Africa. Sunscreen use and environmental awareness were investigated in White Cape Town beachgoers; the results showed that only 50% wore sunscreen, although 90% of respondents cited skin cancer as a potential adverse effect of excess sun exposure and a few acknowledged other health effects.44 A survey of students attending four large tertiary institutions in South Africa showed that 82.3% knew that excessive sunlight may have harmful ocular effects, but only a quarter reported that they often wore sunglasses outdoors and 38.5% recognised that not all spectacles and contact lenses were protective.45
Sun protection is of special importance for individuals with OCA to prevent skin damage and thus lessen the risk of skin cancer. Most OCA cases present late in the tumour process and patients do not complete treatment because of a lack of funds or for cultural reasons. Education regarding protective clothing, sunscreens, indoor occupations and early treatment of skin lesions would be beneficial. An investigation in Tanzania of albinos' understanding of skin cancer risk and attitudes toward sun protection showed that 78% of respondents believed skin cancer was preventable, 63% knew that skin cancer was related to the sun and 77% thought sunscreens afforded sun protection.46 Reasons for not wearing a hat included fashion, culture and heat. Hat-wearing among children with OCA and visual impairment in northern South Africa was high (although the brim width was not always sufficient) and one-third used sunscreens.47
Few sub-Saharan countries have active, sun-related awareness and disease prevention campaigns although some work has been carried out to improve primary health care for the management of cataracts and skin cancer. The non-governmental African Organisation for Research and Training in Cancer promotes cancer control and palliative care, and several sub-Saharan countries have cancer societies. The Cancer Association of South Africa is one of the few with a SunSmart programme. As outlined above, there are currently insufficient data to assess the extent of sun-related health effects and the relevance of any interventions in sub-Saharan Africa.
Challenges and opportunities
Several challenges will need to be overcome and opportunities created to improve the understanding of the health impacts of solar UVR and to implement interventions locally for a sustained improvement in public health. The WHO INTERSUN programme is one possible mechanism. For this programme to be effective in sub-Saharan Africa, fundamental research is needed on local disease prevalence and incidence, exposure patterns (occupational, early life and recreational) and sun awareness, especially the lack thereof but also how awareness is affected by cultural beliefs and practices. The capacity to initiate and manage public health information to support such research is required. For example, a National Cancer Registry has only recently been re-instated in South Africa. There are additional unknowns such as any consequence of climate change in sub-Saharan Africa. Ground-based monitoring of ambient solar UVR is limited, mainly because of financial and personnel restrictions. Little research has been done on potential interactions of solar UVR with local diseases, such as HIV, AIDS, malaria and tuberculosis, and with vaccine responses. Research is also needed on personal solar UVR exposure and sun protection studies on at-risk subpopulations should be conducted. The potential of solar UVR to decrease the efficacy of vaccination by immunosuppression also merits investigation.
Sun education needs to be tailored for sub-Saharan Africa and its multi-ethnic subpopulations. Sun protection and health intervention programmes targeted at children with OCA have proved relatively successful48 and similar targeted interventions for groups at particular risk may be an appropriate way forward. A multidisciplinary approach for research and intervention programmes is essential, especially given the limited resources, capacity and infrastructure, and the high burden of communicable diseases in sub-Saharan Africa. Seeking health co-benefits that arise from dovetailing research with society and government priorities could be the best strategy to manage the health consequences of solar UVR in sub-Saharan Africa.
Acknowledgements
The preparation of this manuscript was funded, in part, by a CSIR Parliamentary Grant to C.W. and a South African Medical Research Council Career Award to L.D.
Competing interests
We declare that we have no financial or personal relationships which may have inappropriately influenced us in writing this paper.
Authors' contributions
C.W. was the project leader, conceptualised the article content and compiled the sun protection and albinism sections. M.N. compiled the immune system section, B.S. compiled the melasma section, L.D. compiled the skin cancer section and M.O.O. compiled the ophthalmohelioses section. C.W., M.N., B.S., L.D. and M.O.O. wrote the manuscript. G.C. gave input to the challenges and opportunities section.
References
1. Norval M, Lucas RM, Cullen AP, et al. The human health effects of ozone depletion and interactions with climate change. Photochem Photobiol Sci. 2011;10:199-225. http://dx.doi.org/10.1039/c0pp90044c [ Links ]
2. Gloster HM, Neal K. Skin cancer in skin of colour. J Am Acad Dermatol. 2006;55:741-760. http://dx.doi.org/10.1016/j.jaad.2005.08.063 [ Links ]
3. Lucas RM. Solar ultraviolet radiation. Assessing the environmental burden of disease at national and local levels. Environmental Burden of Disease Series number 13. Geneva: World Health Organization; 2006. [ Links ]
4. Lucas RM. Solar ultraviolet radiation. Assessing the environmental burden of disease at national and local levels. Environmental Burden of Disease Series number 17. Geneva: World Health Organization; 2010. [ Links ]
5. Isaacson C. Cancer of the skin in urban blacks of South Africa. Br J Dermatol. 1979;100:347-350. http://dx.doi.org/10.1111/j.1365-2133.1979.tb06210.x [ Links ]
6. Mohammed AZ, Edino ST, Ochicha O, Gwarzo AK, Samila AA. Cancer in Nigeria: A 10-year analysis of the Kano registry. Niger J Med. 2008;17:280-284. http://dx.doi.org/10.4314/njm.v17i3.37396 [ Links ]
7. Nthumba PM, Cavadas PC, Landin L. Primary cutaneous malignancies in sub-Saharan Africa. Ann Plast Surg. 2011;66:313-320. http://dx.doi.org/10.1097/SAP.0b013e3181e7db9a [ Links ]
8. Mqoqi N, Kellet P, Sitas F, Jula M. Incidence of histologically diagnosed cancer in South Africa, 1998-1999. Johannesburg: National Cancer Registry of South Africa, National Health Laboratory Service; 2004. [ Links ]
9. Davids LM, Kleemann B. Combating melanoma: The use of photodynamic therapy as a novel, adjuvant therapeutic tool. Cancer Treat Rev. 2011;37(6):465-475. [ Links ]
10. Victor FC, Gerlber J, Rao B. Melasma: A review. J Cutan Med Surg. 2004;8:97-102. http://dx.doi.org/10.1007/s10227-004-0158-9 [ Links ]
11. Guinot C, Cheffai S, Latreille J, et al. Aggravating factors for melasma: A prospective study in 197 Tunisian patients. J Eur Acad Dermatol Venereol. 2010;24:1060-1069. [ Links ]
12. Jobanputra R, Bachmann M. The effect of skin diseases on quality of life in patients from different social and ethnic groups in Cape Town, South Africa. Int J Dermatol. 2000;39:826-831. http://dx.doi.org/10.1046/j.1365-4362.2000.00073.x [ Links ]
13. Hong ES, Zeeb H, Repacholi MH. Albinism in Africa as a public health issue. BMC Public Health. 2006;6:212. http://dx.doi.org/10.1186/1471-2458-6-212 [ Links ]
14. Asuquo ME, Otei OO, Omotoso J, Bassey EE. Letter: Skin cancer in albinos at the University of Calabar teaching Hospital, Calabar, Nigeria. Dermatol Online J. 2010;16:14. [ Links ]
15. Yakabu A, Mabogunje OA. Skin cancer in African albinos. Acta Oncologica. 1993;32:621-622. http://dx.doi.org/10.3109/02841869309092440 [ Links ]
16. Resnikoff S, Pascolini D, Etya'ale D, et al. Global data on visual impairment in the year 2002. Bull World Health Org. 2004;82:844-851. [ Links ]
17. Lewallen S, Courtright P. Blindness in Africa: Present situation and future needs. Br J Ophthalmol. 2001;85:897-903. http://dx.doi.org/10.1136/bjo.85.8.897 [ Links ]
18. Congdon N, West SK, Buhrmann RR, Kouzis A, Munoz B, Mkocha H. Prevalence of the different types of age-related cataract in an African population. Invest Ophthalmol Vis Sci. 2001;42:2478-2482. [ Links ]
19. Entekuma G, Patel J, Sivasubramaniam S, et al. Prevalence, causes, and risk factors for functional low vision in Nigeria: Results from the national survey of blindness and visual impairment. Invest Ophthalmol Vis Sci. 2011;52:6714-6719. http://dx.doi.org/10.1167/iovs.11-7293 [ Links ]
20. Cook CD, Stulting AA. Prevalence and incidence of blindness due to age-related cataract in the rural areas of South Africa. S Afr Med J. 1995;85:26-27. [ Links ]
21. Bucher PJ, Ijsselmuiden CB. Prevalence and causes of blindness in the Northern Transvaal. Br J Ophthalmol. 1988;72:721-726. http://dx.doi.org/10.1136/bjo.72.10.721 [ Links ]
22. Hill JC. The prevalence of corneal disease in the coloured community of a Karoo town. S Afr Med J. 1985;67:723-727. [ Links ]
23. Ashaye AO. Pterygium in Ibadan. West Afr J Med. 1991;10:232-243. [ Links ]
24. NwosuSN. OcularproblemsofyoungadultsinruralNigeria.IntOphthalmol. 1998;22:259-263. http://dx.doi.org/10.1023/A:1006338013075 [ Links ]
25. Lewallen S, Kello AB. The need for management capacity to achieve VISION 2020 in sub-Saharan Africa. PloS Med. 2009;6:e1000184. http://dx.doi.org/10.1371/journal.pmed.1000184 [ Links ]
26. Lecuona K, Cook C. South Africa's cataract surgery rates: Why are we not meeting our targets? S Afr Med J. 2011;101:510-512. [ Links ]
27. Schwarz T, Schwarz A. Molecular mechanisms of ultraviolet radiation-induced immunosuppression. Eur J Cell Biol. 2011;90:560-564. http://dx.doi.org/10.1016/j.ejcb.2010.09.011 [ Links ]
28. Schwalfenberg GK. A review of the critical role of vitamin D in the functioning of the immune system and the clinical implications of vitamin D deficiency. Mol Nutr Food Res. 2011;55:96-108. http://dx.doi.org/10.1002/mnfr.201000174 [ Links ]
29. Prentice A. Vitamin D deficiency: A global perspective. Nutr Rev. 2008;66:s153-164. http://dx.doi.org/10.1111/j.1753-4887.2008.00100.x [ Links ]
30. Feleke Y, Abdulkadir J, Mshana RM, et al. Low levels of serum calcidiol in an African population compared to a North European population. Eur J Endrocrinol. 1999;141:358-360. http://dx.doi.org/10.1530/eje.0.1410358 [ Links ]
31. Wejse C, Olesen R, Rabna P, et al. Serum 25-hydroxyvitamin D in a West African population of tuberculosis patients and unmatched healthy controls. Am J Clin Nutr. 2007;86:1376-1383. [ Links ]
32. Thacher TD, Fischer PR, Pettifor JM, et al. A comparison of calcium, vitamin D, or both for nutritional rickets in Nigerian children. N Engl J Med. 1999;341:563-568. http://dx.doi.org/10.1056/NEJM199908193410803 [ Links ]
33. Honigsmann H. Polymorphous light eruption. Photodermatol Photoimmunol Photomed. 2008;24;155-161. http://dx.doi.org/10.1111/j.1600-0781.2008.00343.x [ Links ]
34. Dean G, Bhigjee AI, Bill PL, et al. Multiple sclerosis in black South Africans and Zimbabweans. J Neurol Neurosurg Psychiatry. 1994;57:1064-1069. http://dx.doi.org/10.1136/jnnp.57.9.1064 [ Links ]
35. Tadokoro T, Kobayashi N, Zmudzka BZ, et al. UV-induced DNA damage and melanin content in human skin differing in racial/ethnic origin. FASEB J. 2003;17:1177-1179. [ Links ]
36. Kelly DA, Young AR, McGregor JM, Seed PT, Potten CS, Walker SL. Sensitivity to sunburn is associated with susceptibility to ultraviolet radiation-induced suppression of cutaneous immunity. J Exp Med. 2000;191:561-566. http://dx.doi.org/10.1084/jem.191.3.561 [ Links ]
37. Gessner BD, Shindo N, Briand S. Seasonal influenza epidemiology in sub-Saharan Africa: A systematic review. Lancet Infect Dis. 2011;11:223-235. http://dx.doi.org/10.1016/S1473-3099(11)70008-1 [ Links ]
38. Fares A. Seasonality of tuberculosis. J Glob Infect Dis. 2011;3:46-55. http://dx.doi.org/10.4103/0974-777X.77296 [ Links ]
39. Martineau AR, Nhamoyebonde S, Oni T, et al. Reciprocal seasonal variation in vitamin D status and tuberculosis notifications in Cape Town, South Africa. Proc Natl Acad Sic USA. 2011;108(47):19013-19017. http://dx.doi.org/10.1073/pnas.1111825108 [ Links ]
40. Akaraphanth R, Lim HW. HIV, UV and immunosuppression. Photodermatol Photoimmunol Photomed. 1999;15:28-31. http://dx.doi.org/10.1111/j.1600-0781.1999.tb00049.x [ Links ]
41. Norval M, Woods GM. UV-induced immunosuppression and the efficacy of vaccination. Photochem Photobiol Sci. 2011;10:1267-1274. http://dx.doi.org/10.1039/c1pp05105a [ Links ]
42. Colditz GA, Brewer TF, Berkey CS, et al. Efficacy of BCG vaccine in the prevention of tuberculosis. JAMA. 1994;271:698-702. http://dx.doi.org/10.1001/jama.1994.03510330076038 [ Links ]
43. Guy CY, Diab RD. A health risk assessment of ultraviolet radiation in Durban. S Afr Geographical J. 2002;84:208-213. http://dx.doi.org/10.1080/03736245.2002.9713772 [ Links ]
44. Von Schirnding Y, Strauss N, Mathee A, Robertson P, Blignaut R. Sunscreen use and environmental awareness among beach-goers in Cape Town, South Africa. Public Health Rev. 1991/92;19:209-217. [ Links ]
45. Oduntan OA, Carlson A, Clarke-Farr P, Hansraj R. South African university student knowledge of eye protection against sunlight. S Afr Optom. 2009;68:25-31. [ Links ]
46. McBride SR, Leppard DM. Attitudes and beliefs of an albino population towards sun avoidance: Advice and services provided by an outreach albino clinic in Tanzania. Arch Dermatol. 2002;138:629-632. http://dx.doi.org/10.1001/archderm.138.5.629 [ Links ]
47. Lund PM, Taylor JS. Lack of adequate sun protection for children with oculocutaneous albinism in South Africa. BMC Public Health. 2008;8:225. http://dx.doi.org/10.1186/1471-2458-8-225 [ Links ]
48. Lund PM, Gaigher R. A health intervention programme for children with albinism at a special school in South Africa. Health Educ Res. 2002;17:365-372. http://dx.doi.org/10.1093/her/17.3.365 [ Links ]
![]() Correspondence to:
Correspondence to:
Caradee Wright
PO Box 395, Pretoria 0001, South Africa
Email: cwright@csir.co.za
Received: 24 Apr. 2012
Accepted: 11 June 2012
Published: 26 Oct. 2012
© 2012. The Authors. Licensee: AOSIS OpenJournals. This work is licensed under the Creative Commons Attribution License.

