










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Science
versão On-line ISSN 1996-7489
versão impressa ISSN 0038-2353
S. Afr. j. sci. vol.106 no.5-6 Pretoria Mai./Jun. 2010
RESEARCH ARTICLE
A tool for modernisation? The Boer concentration camps of the South African War, 1900-1902
Elizabeth van Heyningen
Department of Historical Studies, University of Cape Town, South Africa
ABSTRACT
While not denying the tragedy of the high mortality of people in the concentration camps in the South African War of 1899-1902, this article suggests that, for Lord Milner and the British Colonial Office, the camps became a means of introducing the rural society of the Boers to the facilities of modern life. To some extent they became, in effect, part of Milner's project for 'civilising' and assimilating the Boers into British colonial society. The high mortality rate was finally contained through the introduction of a modern public health system, including the use of statistics and the employment of qualified doctors and nurses. Young Boer women working in the camp hospitals as nurse aids were trained as 'probationers' and classes in infant and child care were offered to the Boer mothers. In addition, the need for adequate water supplies and effective sanitation meant that an infrastructure was established in the camps that familiarised the Boers with modern sanitary routines and left a legacy of more substantial services for the Transvaal and Orange Free State villages.
Keywords: Anglo-Boer War; concentration camps; historical statistics; Lord Milner; measles mortality; South African War
INTRODUCTION
Most written material on the concentration camps of the South African War is confined to the suffering and mortality of the Boer women and children. This article, while not discounting the incompetence that contributed to the deaths, suggests that the camps can be seen in a broader context; that they might be considered, perhaps, as a vehicle for the modernisation of rural Boer society. In this sense, the camps became linked to Lord Milner's project for the establishment of a strong British presence in South Africa.1,2
One reason for this argument is that the formation of the camps led, in some respects, to the temporary urbanisation of the Boer peasantry. The process bore similarities to the early industrial cities of Europe, in which rapid immigration gave rise to massive mortality. As a result, the British found it necessary to implement in the camps many of the elements of preventive health care available at the end of the 19th century, including the introduction of vital statistics, clean water supplies and effective sanitation. Ration scales were adjusted to provide adequate nutrition and the Boer women were introduced to contemporary nursing and infant care practices. The long-term legacy of the camps, in these respects, is difficult to measure, but it gave the Boers a taste of the modern urban life they were to experience more fully in the years after the war. However, far less is known about the impact of the camps on Black people, who suffered as severely as the Boers but received relatively little consideration.
The suffering experienced within the concentration camps of the South African War has been endlessly mythologised,3 but these camps rarely have been considered as an experiment in emergency public health, or as a vindication of modern Western medicine.4 Yet, while they were initially conceived as a form of poor relief by the Colonial Office (but not by Lord Kitchener, for whom the clearances were military strategy), as the months passed, Lord Milner, the South African High Commissioner, and the civilian administration began to see the camps as a means of demonstrating the virtues of British rule to their new Boer subjects.5 This article explores the notion of the camps as a tool of modernisation in early 20th-century South Africa.
The origins of the camps are well established. They came into being towards the end of 1900, primarily as a result of the burning of Boer farms by the British troops, first initiated by Lord Roberts. The clearances were expanded by Lord Kitchener after he became commander-in-chief of the British forces and instituted a 'scorched earth' policy to bring to an end the guerrilla campaign of the Boers. It is estimated that as many Black people as White people were swept up into camps as a result of an ill-considered policy for which there was little planning. A combination of short-sighted thrift and lack of supplies meant that the early camps were deficient in tents and other basic necessities. Although the ration scales were similar to institutional ration scales of the day, they were inadequate for women and children.
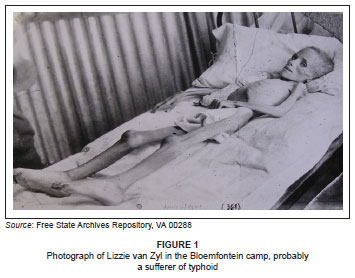
A poorly managed typhoid epidemic killed some 8020 British soldiers and infected many of the main water sources of the country, including the Modder River, which passes through Bloemfontein, and the Vaal River.6,7,8 The troops carried the disease with them as they advanced, polluting the local water supplies. Although the typhoid bacillus was identified in about 1890 and an effective vaccine developed by Dr Almroth Wright in 1897, the vaccine was seldom used during the South African War.8 The camp administrators did their best to combat the epidemic, more or less successfully, but it was a constant worry. By ill-luck, measles, an epidemic rather than an endemic disease in rural South Africa, was already present in the country at the start of the war. In the chaotic conditions of wartime, and in the overcrowded and traumatised camps, the disease spread like wildfire, especially between about February and November 1901. A substantial number of the children who died did so from the sequelae of measles, particularly pneumonia and bronchitis, but also intestinal problems and, occasionally, meningitis or the complaint known at the time as cancrum oris (noma). A common feature of the camps was the 'faded flowers', children who failed to thrive and gradually died. These terrifying and unfamiliar ailments sometimes convinced the distressed parents that the British had deliberately killed their children, either through poison or neglect. These beliefs passed into camp mythology, contributing to the creation of a 'paradigm of suffering' which underlay the fostering of Afrikaner nationalism in the 20th century and they were epitomised by the photograph of Lizzie van Zyl (Figure 1).9,10,11 But 'wasting' was a fairly common occurrence in Britain and Australia as well.12,13
Less is known about morbidity and mortality in the Black camps. Since their accommodation and nutrition were far worse than in the White camps, it is conceivable that mortality was at least as high amongst Black children as White children. It is known that some 14 154 Black people died and the figure may have been at least 20 000.14,15 However, most of the Black camp records have been destroyed and the memory of suffering in the Black camps largely has been erased by the experiences of the 20th century. The limited attempt to acknowledge their share of the tragedy has been unable to penetrate very far into the Black experience.
STATISTICS
Statistics were fundamental to the 19th-century public health movement. With the exception of the Cape Colony, the country was almost statistically barren at the outbreak of the South African War. Both the Orange Free State and the South African Republic conducted censuses in 1890, but the latter, particularly, was flawed; there was no registration of births and deaths and no other vital statistics were collected. Almost as soon as the British civilian administration was formed, legislation was set in place for the registration of births and deaths (the first full censuses were conducted in 1904). But it was in the camps that registration could be implemented most easily and for another practical purpose. The most expensive item of camp expenditure was the rations, with a differentiation between the amount provided for adults and children, and so it was important to keep a close check on the number and ages of the inmates to ensure efficient ration distribution.
In the Orange River Colony (ORC), (the Orange Free State had been annexed by the British in 1900 and renamed) the newly appointed colonial medical officer of health, Dr George Pratt Yule, collected and analysed the camp data in great detail.16 In the Transvaal, Lord Milner and his 'kindergarten' team did the same.17,18,19,20,21,22,23,24,25,26 The result was a remarkably complete record of White camp populations and their mortality. Major G.F. de Lotbinière, who managed the Black camps from about August 1901, supplied similar data.14 The correspondence between camp superintendents and the two head offices, querying and rechecking the figures, testifies to the level of importance the administration placed upon this data. However, these statistics should not be confused with the various death lists, including those published in the government gazettes. For a variety of reasons these lists are inaccurate, as is the official total of White deaths, 27 927, recorded by P.L.A. Goldman.3 The discussion below is therefore based on the statistics found in the Transvaal camp reports and in Pratt Yule's reports.
The statistics demonstrated distinct patterns of mortality (Figure 2).6 In the White camps, deaths peaked in October 1901, while deaths in the Black camps peaked in December, perhaps because the Black camp system was only set up later. ORC mortality was slightly higher than that of the Transvaal, although the data are slightly skewed since, from the end of 1901, large numbers of Boer families from the Transvaal were sent to Natal and these figures were not included. The ORC data include the families sent to the Cape. Once the data are disaggregated, however, a much more complex pattern emerges.
Broadly, the earlier a camp was founded, the earlier mortality peaked (Figure 3). The camps at Kimberley, Bloemfontein and Kroonstad were all on the route of the primary northward march of the British troops and disease followed in their wake; the Bloemfontein camp was formed in about September 1900 and mortality peaked very early. Bethulie, on the other hand, was formed at the end of April 1901, as an overflow of the Springfontein camp and, consequently, had a later mortality peak.
More significant than the timing of the mortality peaks were the patterns of mortality (Figure 4). Brandfort and Mafeking had the highest mortality peaks of any camps, in Brandfort reaching 1166 per 1000 per annum in October 1901; at this rate, every camp inmate would have died within a year had the population remained static. Appalling though this was, the pattern was worse in Bethulie camp, which had a higher total number of deaths and a prolonged period of elevated mortality. All three camps were about the same size, with an average monthly population of 3000, but Bethulie had a total of 1370 deaths, compared with a total of 1081 at Brandfort and a total of 1029 at Mafeking.
Bethulie's mortality pattern was remarkable in another respect as well, for the ratio of adult deaths to child deaths within this camp was far higher than almost any other camp (Figure 5).
In their analysis of the Transvaal camps, Low-Beer et al.6 noted that measles was the largest single cause of death, accounting for 42% - 43% of deaths, three times more than any other illness. Pneumonia was the second most prevalent, with these two causes accounting jointly for 61% of all deaths. Dysentery and diarrhoea, typhoid and whooping cough were also major causes of death.6 Reasons for deaths in the ORC were very similar. In Bethulie, measles and respiratory complaints formed, by far, the most significant causes of death (Figure 6) and this is true of all the other camps as well. Typhoid was usually regarded as a summer disease in South Africa and the second mortality peak in the Bethulie camp (Figures 3 and 4) probably reflects the increase in this malady in the summer months, especially because this was an illness to which adults were particularly vulnerable.
Although measles occurred as an epidemic disease, it was not unknown in the Boer republics prior to the outbreak of war. The ages of mortality suggest that most adults had some immunity and a proportion of children under a year shared their mothers' resistance (Figure 7), especially as the Boers tended to wean their children late. Infants, who inherited an immunity from their mothers, were also protected from typhoid, which struck their older siblings and their parents.
The statistics do not reflect the range of other diseases which struck the camps. Observers, for instance, remarked on the prevalence of flies and so trachoma was also probably widespread. Occasional references to bleeding gums suggest that many people suffered from scurvy, but other teething complaints are rarely mentioned. Even more striking is the absence of any discussion of women's ailments. Puerperal fever after childbirth only occurred in a few instances but, in these camps of women, there must have been other problems which were not openly talked about in late Victorian culture. For most of 1901 it is likely that the camp inhabitants were never completely healthy. However, the position was very different in 1902.
DOCTORS, NURSES AND HOSPITALS
Camp mortality occurred in an era in which the prevention of infectious disease was well understood. The 19th-century public health movement had greatly reduced deaths in the industrial cities and the development of the 'germ theory of disease' made it possible to identify pathogens such as the Salmonella typhi bacillus, which caused typhoid. There were still few effective therapies, but, by 1900, there was an anti-toxin for diphtheria, which was used successfully in the camps. Nevertheless, two crucial obstacles remained. Firstly, Britain's child mortality rate was still very high - the infant mortality rate in England in 1899 was 146 per 1000 per annum - having increased since 1876 - and the medical profession was only just beginning to grasp the need for more informed maternal care and the careful monitoring of young babies.27 Infant mortality rates in the camps were also high but, in the light of the British experience of the day, should not be judged by modern standards. Secondly, the origins of viral diseases remained unidentified and there was no means of combating measles, except through the age-old technique of quarantine, which was impossible under South Africa's wartime conditions. By 1902, when the flow of people into the camps had been reduced, isolation camps and contact camps were established, as subsidiaries to the main camps, but this was very much a case of closing the gate after the horse had escaped. Nevertheless, modern medical practice played a major role in improving camp health.
The medical staff in the camps were vital. In the early months, trained doctors and certified nurses were in short supply and many camps had to manage with the occasional attendance of a local military doctor or district surgeon and untrained nurses. While some camps, like Norvals Pont, coped successfully with this limited care, the importance of competent medical staff is illustrated by the cases of Mafeking and Bethulie.
Mafeking's extreme mortality was the product of a sudden, rather late, measles epidemic in August 1901 and the doctors present were unable to cope when the disease struck. Dr Kaufmann, a Viennese man, was both conscientious and hard-working but had no administrative skills. His assistant, who was German, spoke little English and no Dutch. The result was severe staff shortages, a lack of medical supplies and poorly kept records. Some children had not seen a doctor for a week or more before they died. When he resigned, Kauffman wrote aggrievedly:
I am sorry that I am so overworked and exhausted that I must stop my work except giving all over to Dr. Morrow [his replacement]... I should have asked assistance, but as you replied to my first request (20th of August) that other larger camps have only one doctor, I resented it as a reproach and restrained from asking more. The fact is, that here is work enough for five hardworking doctors.28
Bethulie, too, had an inept superintendent who failed to recruit suitable medical staff. The town doctor, who attended the camp in the beginning, was so aggressive that a charge of assault was laid against him. His replacement, Dr Madden, was so incompetent that he would have been dismissed within a week if he had not been needed so badly. However, Dr Madden was never well and died a couple of months later, while still at Bethulie. As mortality mounted, an investigation brought to light the fact that later doctors were often drunk. Moreover, the medical staff quarrelled with one another and the superintendent. Thus it was hardly surprising that Bethulie was probably the most demoralised camp in the entire system.29
Once he finally grasped the dire nature of the health situation in the camps, Lord Milner swiftly recruited properly qualified staff from Britain. Perhaps 50 doctors and over 100 nurses came out to South Africa to work in the camps. The majority of the doctors appear to have been young and newly qualified. With limited prospects in the overcrowded medical market of Britain, many hoped to make careers abroad and a number of these camp doctors stayed on as district surgeons in the ORC and Transvaal towns after the war (e.g. Dr John Graham, whose later career has been recorded).30 The nurses, on the other hand, were older, usually in their thirties, perhaps with little prospect of marriage. A few may have come for the adventure, sometimes as friends. It was reported that Edinburgh Infirmary lost a number of nurses to the camps. But the greatest inducement seems to have been the salaries which, at £10 a month, were far more than they had been earning before. They were given a free return passage to South Africa and few appear to have remained in the country after the war. These nurses may have found adventure but camp conditions were difficult. They lived in the same threadbare tents as the Boers and shared their rations, supplemented by a few 'medical comforts' like rice and jam.
Inevitably, there were some 'bad eggs' amongst the recruits, as in the case of the Bethulie doctors. These were men, like John Hunter in the Kimberley camp, who were described as ambitious and arrogant and clashed with the superintendents over authority.31 Owing to the fact that, at £500 a year, the doctors were paid more than the superintendents, this was hardly surprising. Nevertheless, the majority of medical staff gave good service. Men and women, such as these, brought professional standards to the hospitals, often the first medical institutions in the upcountry towns.
But, in this gendered environment, the nurses had another involuntary role to play, for they were also seen as models of ideal British womanhood, examples of gentility and femininity to the Boer peasantry.5 The Transvaal Director of Burgher Camps wrote to General Maxwell,
[The nurses] have created a very favourable impression, being physically strong and attractive, and presenting by ocular demonstration, to the inmates of the Camps, examples of British womanhood. The moral effect of the association of these earnest noble-minded and cultivated ladies, with the people of the veld ... cannot fail to be productive of much good in many ways, and especially in softening the bitter feelings of enmity which unfortunately are inborn in so many of the Boer women against the British name.32
The camp hospitals received a significant amount of bad press. Boer women were accustomed to doing their own nursing and they hated the separation from their children. To make matters worse, some camp hospitals limited parents' visits; it was even claimed that mothers were only allowed to see their sick children once a week, for five minutes, and, even then, they were not allowed to speak to them.33 Most hospitals, however, allowed mothers to remain with their dying children. Food was another major issue and the Boer mothers found the reduced diets allowed for typhoid patients very difficult to understand, with some mothers attempting to smuggle in unsuitable food, even to the very end, complaining that their children were starving.17,34
The Boers' aversion to entering a hospital was not uncommon in societies where hospitals were alien environments to be feared; the poor of Britain and the United States of America had been as reluctant as any camp inmate to be hospitalised. There had been good reason for this antipathy in the past but late-19th-century hospitals were very different institutions from those of the pre-Nightingale era. By 1902, however, most camps reported that the resistance to entering hospitals was disappearing, as parents could see that their children fared better in hospital than in the tents.35
A critical mediator between parents and hospitals were the so-called 'probationers' - young Boer women who served as nurse-aids in the hospitals. By 1902, every camp employed at least 20 young women in the hospitals and several hundred must have seen such service by the end of the war. In some cases relations were poor, but the ability of the British staff to get along with the Boer girls was often an indicator of the competence of the former. Particularly in the early days, British doctors could be patronising, as in the Middelburg camp, where the medical officer complained that these young women were 'very slow and difficult to train'. But, he believed, the Boers, and especially the girls, would greatly benefit from the education and discipline they acquired.17
In many cases, however, the British medical staff took great pride in the skills they instilled in the Boer women. Superintendent Nowers at the Orange River camp felt that some of his probationers were sufficiently competent to be promoted to nursing assistants at £6 a month, a considerable improvement on the 1 shilling a day they were usually paid. Inspector Tonkin recommended a similar promotion at the Kroonstad camp.36,37 By the end of the war, the camp administrators had introduced training programmes for their probationers, in which the women were given lectures and tests and some were issued with certificates.38 At the very least, these young women took home with them a knowledge of sanitary practice and nutrition, which had been lacking before the war. A handful of them were even able to get nursing jobs outside the camps and it was hoped that some would train further after the war. Few took advantage of the offer, but others may have been amongst the earliest South African recruits to nursing, although it was only in the 1920s that Afrikaner women began to enter the nursing profession in any numbers.39
SANITATION
When war broke out in 1899, the Boer republics were still largely rural. The only town of any substance was Johannesburg and, to some extent, Pretoria. Bloemfontein, with a population of 3379 in 1890, was the only town in the Orange Free State to have more than 1000 inhabitants and there was no substantial urbanisation over the next decade. In contrast, most camps had at least 2000 inmates. The Bloemfontein camp, with an average population of 4825, which rose to nearly 7000 at times, was considerably larger than the town outside which it was situated. This is even more striking in Middelburg, which had a White village population of 563 in 1890, while the camp housed over 7000 at one point (Black people were not counted in these censuses).
The camps existed side-by-side with societies in which urban administration was often extremely rudimentary. Repeatedly, the early district commissioners complained about the insanitary condition of the towns they were administering.40,41 Boer farms often lacked any form of sanitation. Accounts of Boer sanitary practices, though much resented by middle-class Afrikaners then and later, are so graphic and so frequent that there can be no doubt that most Boers in the camps, who were bywoners (landless farmers) rather than middle class, lived in comfortable association with human and animal excrement.
Therefore, a major concern of the camp superintendents was sanitation and every camp report contained some comment on the cleanliness of the camp. Camp inmates had to be prevented from fouling the ground around their tents, from throwing out slops and rubbish and, with more difficulty, they had to be persuaded to use the communal latrines. On dark nights, when the entire family was sometimes struck down with dysentery or diarrhoea, it was impossible to expect them to walk up to half a mile (0.8 kilometres) to the latrines. The latrines themselves ranged from trenches, which the army used and which were entirely unsuitable for small children, to the bucket system. Lack of wood, galvanised iron, pails, transport animals, labourers (for able-bodied Black and White men were recruited to serve in the military wherever possible), all contributed to the difficulty of keeping the camps clean in the early months.
By 1902 the situation was very different. Although shortages remained, the camp authorities had the money to install better latrines and to disinfect on a large scale. In order to stem the tide of mortality in Mafeking, 400 sanitary pails and 12 tons of disinfectant were ordered.42 Night latrines were provided in all the Transvaal camps and the main latrines were transformed with hard flooring and proper removal systems.43 By 1902 in the Transvaal, a ratio of 10 people to a latrine was advocated and cleanliness was implemented through constant inspection and some coercion.44
Even more important was the need to persuade the women and children to abide by camp regulations. The ability of the camp superintendents to manage the families revealed much about relationships within the camps. Some of the camp superintendents, who were South Africans, were untroubled by a degree of untidiness and dirt in the camps; others were fanatically concerned about keeping their camps spotless and orderly. The Boers themselves valued 'kindness', but it was 'firmness' that kept the mortality rate low. Those camp superintendents who could combine tact with discipline usually had the most successful camps, in which the inhabitants were contented and healthy. The contrast between the Bethulie and Norvals Pont camps illustrates this.
Russell Deare, the superintendent of Bethulie camp, was much loved by the camp inmates. But Bethulie was the archetypal 'bad' camp, with soaring mortality rates (Figure 8), demoralised inmates and incompetent doctors.29 Norvals Pont was very different. The superintendent, St John Cole Bowen, showed little overt sympathy for the Boers, dealing briskly with those he regarded as troublemakers and insisting that a rigorous regime of inspection be followed. Consequently, the camp administration thought highly of him. 'Mr Cole Bowen is a level headed man', chief superintendent Trollope noted on one occasion.45 But, strikingly, Emily Hobhouse was also impressed by him, as was the Ladies Committee thereafter. Emily Hobhouse reported that he possessed 'marked administrative powers; his rule was firm, just and kind and he seemed possessed of unlimited resources'.45 Not surprisingly, although Norvals Pont did not entirely escape the measles epidemic, the mortality rate was well below the national camp average (Figure 8).
Effective sanitation and low mortality, then, depended as much upon the character of the camp staff as it did upon cleanliness. Firmness and discipline combined with tact and compassion usually persuaded the Boer families to accept sanitary regulations relatively willingly. It is impossible to know the long-term effect of these measures on the Boers but, at the very least, camp life served to familiarise them with a more modern sanitary regime.
WATER SUPPLY
One of the most critical elements in the establishment of the camps in a water-short South Africa was a good water supply. Before the war, many of the republican towns, with their tiny populations, had been able to depend on local streams and springs. But the war brought thousands of soldiers and their horses and military encampments placed a heavy burden on these slender stocks as these camps were always sited nearby. Streams which had been adequate for 1000 people could not serve an additional 10 000. Therefore, a major consideration in the location of the concentration camps was the availability of water. By 1902, the cost of engineering works formed a large part of the camp budgets. In his estimates for 1902, Milner anticipated that engineering, sanitation and water would cost the camp £17 000 a month, out of a total budget of £182 000 a month. By comparison, £10 000 was budgeted for doctors and nurses and £115 000 for food.46
In Bloemfontein, however, every water source became polluted with typhoid and this compounded the overall water shortage, which meant that camp inmates received only a pint (about half a litre) of boiled water a day, hopelessly inadequate in the summer heat. Worse still, was the lack of wood available for the fires required to boil the water. Camps like Standerton, on the Vaal River, had ample fuel and water, but the river was heavily polluted with disease and, in any case, the Boers disliked the taste of boiled water.17
The British were well aware that a clean water supply was the foundation of preventive health care. As a result, they often tested questionable water. In the case of Kroonstad, the camp was supplied from the municipal waterworks, pumped from a weir on the Valsch River and passed through two filter beds. Nonetheless, the colonial medical officer of health, Dr Pratt Yule, considered this an entirely inadequate system for purifying the water. The filters often became clogged with mud, resulting in turbid water that was full of vegetable matter and microorganisms.47 The Aliwal North camp water was sent to Professor P.D. Hahn in Cape Town for analysis. With some filtration, he believed that this supply was harmless.48 In March the following year, Dr Parry Edwards, one of the camp doctors with a diploma in public health from Cambridge, undertook to analyse the water in all the ORC camps. Although he concluded that most camp water was safe to drink, it was often unpalatable, like the Kroonstad water.49 By this time, the Transvaal camp system was contemplating the establishment of its own laboratory to analyse water and milk.50
Quantity was as important as quality. Effective sanitation depended on ample water to boil hospital linen and disinfect cooking utensils. By 1902, the camps were employing water engineers to inspect the camps regularly, dig wells and dams and install pumps and pipes. As early as April 1901, the Bethulie camp asked permission to employ a water engineer to lay pipes because the local 'spruit' was likely to dry up in summer.51 The Brandfort camp ran into difficulties in May 1902, when a new borehole, complete with pipes and taps, ran dry. They had to resort to the old bore, worked by a horse engine, but this was inadequate and the camp had to be supplied by water carts. Brandfort's superintendent begged that one of the two water engineers, now in the employ of ORC camp administration, be sent urgently.52 Standerton, on the polluted Vaal River, struggled with water until the Transvaal camp water engineer arrived to install an elaborate system of tanks, pipes and engines.53 By April 1902, the Klerksdorp camp had 10 tanks for boiling water, ensuring that no river water was used at all.54,55 Aliwal North, on the confluence of the Kraai and Orange Rivers, could have been expected to have ample water, but, by 1902, an extensive water scheme had been installed, including five miles of pipes, an engine which supplied 20 000 gallons (90 921 litres) a day and £3150 worth of storage tanks. Since this elaborate scheme, which also included a sand filter, was well beyond the needs of the camp, the authorities began negotiations to supply the town as well. They hoped that the whole apparatus could be sold to the town at the end of the war.56
By May 1902, the scale of engineering was so large that a number of villages inherited relatively sophisticated water systems. In this way, at least, the camps left a practical legacy.
NUTRITION
Food is one of the most misunderstood aspects of the camps as it is deeply affected by cultural and social values. Camp inmates prized fresh meat above all, which was vital in the camps because it was the main source of nutrients. Boer families disliked the unfamiliar tinned corned beef and considered even the frozen meat, which they received later, to be unpalatable. The widespread stories about hooks in the tinned meat, which continues to circulate among the more conservative Afrikaners, had more to do with this prejudice than with the reality, although some tins probably were contaminated.57 By 1902, the ORC camps, alone, were consuming at least one million pounds (453 592 kilograms) of meat every month.58
By 1900, ration scales were commonplace in many British institutions. In the previous hundred years, chemical and medical research, much of which was conducted in prisons and workhouses, had greatly advanced the understanding of the relationship between food and health.59,60 The importance of proteins and carbohydrates was well established, as was that of fats, but vitamins had not yet been discovered. It was perfectly possible, therefore, to draw up adequate ration scales for the camps. Unfortunately, other considerations often intervened. In workhouses, for instance, the principle of 'less eligibility' meant that food should always be more unpalatable than the poor could obtain outside, lest they be 'pauperised'. Moreover, diet scales were often drawn up by people with little knowledge of nutrition. As late as the 1890s, therefore, the supply of calories in these places was usually inadequate.61
It is not known who created the initial ration scales for the camps but military doctors were probably consulted. The full ration scale for adults per week in the Transvaal in February 1901 was: 7 lb meal or flour, 4 oz salt, 6 oz coffee, 12 oz sugar and 2 lb meat (children less than 12 years old received half).17 When the civilian administration took over in February 1901, economy was the watchword and food was the most expensive item in the budget. At first, the Transvaal had two ration scales, including the notorious meatless ration scale for the families of men on commando. But many camp superintendents refused to implement this 'Scale B' at all and it was officially abandoned within a month.17,62 Meatless diets for White inmates was not, therefore, an issue. However, the case was very different for Black inmates, who often did not have meat included in their diets.62 The ration scales were compiled by military men with little appreciation of the needs of women and children. Even teenage boys like young George Brink, the son of the Vredefort Road superintendent, were always hungry.30 Babies simply could not eat the coarse food and fresh milk was difficult to acquire, thus condensed milk, usually sweetened but sometimes skimmed, took its place, but was either insufficiently or overly watered down and lacked fat, as well as vitamins A and D.63 Moreover, tough meat took long to cook and that was impossible when fuel was short; half-cooked food was one explanation for the frequent digestive problems in the camps, the Ladies Committee observed.64
Supplies were dependent on a single railway line that ran northwards, which was regularly disrupted by guerrilla raids, creating endless problems and thus military needs took priority. At first, meat came from the animals requisitioned from Boer farms, but the stock had often travelled long distances and, as winter grazing deteriorated, so did the animals. There is no doubt that fresh meat often lacked any fat and was diseased or inedible. Lucy Deane of the Ladies Committee commented on one occasion that the meat was
[v]ery scarce and dear, and awfully nasty; either 'trek Ox' which is so near the verge of starvation before it is killed that the carcase looks like a concertina drawn out fully with all the wind knocked out, just rib-bones with their flabby skin drawn over them, and no flesh at all ... I saw scores of sheep weighed before me in the Camps as they arrived for the rations; and 16, 17, 18 lbs. [7.25, 7.7, 8.16 kgs] was the total weight of each sheep! Fowls are almost unobtainable luxuries ...65
Emily Hobhouse emphasised the unsuitability of the ration scales in her report published in June 1901. As a result, the pro-Boer, Dr J.S. Haldane, father of the scientist J.B.S. Haldane, wrote to the Colonial Office with a very thorough analysis of the diet scales. Women, he stated, required at least 2800 calories a day but, as far as he could establish from the varied practices in the camps, they were not receiving enough. He concluded that,
[w]ith reference to various remarks by Superintendents and doctors about listlessness and disinclination of the inmates to work, it should be clearly understood that the adult diets are quite insufficient for an adult to do work upon ... The great predisposing cause of the enormous mortality is in all probability the inadequacy of the food supply.66
The Colonial Office forwarded Haldane's report to its own consultant, Dr Sidney Martin, who reached very similar conclusions. Even with the improved ration scales that had been introduced following the investigations of the Ladies Committee, the Transvaal diet for adult women was still nearly 700 calories below that which they required and showed a great deficiency in 'proteids'. In every case there was little or no fat.67 All of these investigations led to greatly improved diet scales.
As long as children were fed on tinned milk, however, difficulties probably remained, for the condensed milk of the day was lacking in nutrients and was often unsterilised. Babies fed on such tinned milk only, could become severely malnourished.12 At least some of the camp authorities tried to ensure that 'Ideal' milk was used. Since it was unsweetened, however, this milk sometimes soured. 'Milkmaid' or 'Sledge' brands, the latter sweetened, were occasionally used instead, but fresh milk was almost impossible to obtain.17,68,69
Nevertheless, not all of the inmates suffered. The camps had stores where those with money could supplement their rations with rice, tinned fish or jam. Since most of the men and a number of the women were paid for work in the camps, many were able to take advantage of this facility and some stores earned as much as £1000 a month. Enterprising Indian traders, when allowed into the camps, sold fruit and vegetables, which were even more valuable. The more percipient superintendents established vegetable gardens early on, but this practice had become commonplace by the end of 1901. Even so, scurvy was regularly present in the camps and was almost certainly under-reported. By 1902, lime juice was introduced as a prophylactic but the Boers often considered it too sour and refused to drink it without sugar. By the end of 1901, soup kitchens had been established to ensure that even the most indigent children were adequately nourished. Bakeries and public ovens also made more effective use of fuel.
These steps were considered necessary because the camp officials were also critical of Boer cooking practices. They disliked the Boer habit of drying out the meat for biltong and they considered that many Boer mothers had little idea of how to feed their children, giving them heavy bread, meat and stewed coffee, as Pratt Yule complained.16 There was probably some truth in their observations since both the Transvaal Indigency Commission of 1908 and Louis Leipoldt, in his submissions to the Carnegie Commission in 1932, commented on the poor quality of Boer meals.70 By 1902, the more energetic camp officials were giving lectures on childcare and nutrition to the mothers.71,72 In this, they were anticipating work in Britain, published in 1903 and 1904, which concluded that the most important factor in preventing diarrhoea and wasting in children was sterile food.12,27
CONCLUSION
Lord Milner, who placed a higher value on the public role of women than many of his colleagues, was also more sensitive to the function of the camps in his project for the reconstruction of South Africa than earlier historians have recognised.5,73 Given the place of the camps in the post-war creation of Afrikaner nationalism, at first glance the camps, as a project of anglicisation and assimilation, were a monumental failure. In less obvious ways, however, the legacy of the camps may have been more effective. Able men like Dr Graham of Vredefort Road and St John Cole Bowen stayed on, to work all their lives amongst the people they had served in the camps. Some inland villages acquired better sanitary facilities and water supplies.
Few of the camp inmates left any record of the way in which the camp experiences described here subsequently impacted on their lives. Whatever they learned in the way of sanitation or infant care, however, was reinforced after the war by the emergence of women's organisations and journals that attempted to inculcate middle-class values as they strove to unite Afrikaner women under the umbrella of the volksmoeder (mother of the nation) ideology (for the classic work on the volksmoeder concept, see Brink74). Die Huisvrou, Die Boerevrou and organisations such as the Afrikaanse Christelike Vroue Vereniging and the Suid-Afrikaanse Vroue Federasie, all carried modernist messages of preventive health care, along with 'welfare feminism' and Afrikaner nationalism.74,75,76 By the 1920s, when Afrikaner women were beginning to enter the nursing and teaching professions in larger numbers, these ideals had become thoroughly embedded in Afrikaner consciousness.
ACKNOWLEDGEMENTS
I gratefully acknowledge the assistance of the Wellcome Trust for funding the research on which this article is based. They are, however, in no way responsible for my opinions. My appreciation also goes to Dr Iain Smith for his support and stimulating discussion and to Professor Richard Mendelsohn for his helpful suggestions.
REFERENCES
1. Denoon D. A grand illusion. The failure of imperial policy in the Transvaal colony during the period of reconstruction 1900-1905. London: Longman; 1973. [ Links ]
2. Davenport TRH. South Africa: A modern history. 3rd ed. Johannesburg: Macmillan, 1987; p. 225-228. [ Links ]
3. Van Heyningen E. Costly mythologies: The concentration camps of the South African War in Afrikaner historiography. J South Afr Stud. 2008;34(3):495-513. [ Links ]
4. Van Heyningen E. Women and disease. The clash of medical cultures in the concentration camps of the South African War. In: Cuthbertson G, Grundlingh A, Suttie M-L, editors. Writing a wider war. Rethinking gender, race, and identity in the South African War, 1899-1902. Cape Town: David Philip, 2002; p. 186-212. [ Links ]
5. Riedi E. Teaching empire: British and dominions women teachers in the South African War concentration camps. Engl Hist Rev. 2005;CXX(489):1316-1347. [ Links ]
6. Low-Beer D, Smallman-Raynor M, Cliff A. Disease and death in the South African War: changing disease patterns from soldiers to refugees. Soc Hist Med. 2004;17(2):223-245. [ Links ]
7. Curtin P. Disease and empire: The health of European troops in the conquest of Africa. Cambridge: Cambridge University Press, 1997; p. 210. [ Links ]
8. De Villiers JC. Healers, helpers and hospitals. A history of military medicine in the Anglo-Boer War. Pretoria: Protea, 2008; p. 111. [ Links ]
9. Marais P. [The woman in the Anglo-Boer War 1899-1902]. Pretoria: JP van der Walt, 1999; p. 106-108. Afrikaans. [ Links ]
10. Godby M. Confronting horror: Emily Hobhouse and the concentration camp photographs of the South African War. Kronos. 2006;32:34-48. [ Links ]
11. Stanley L. Mourning becomes... Post/memory, commemoration and the concentration camps of the South African War. Manchester: Manchester University Press, 2006; p. 127-133. [ Links ]
12. Fildes V. Infant feeding practices and infant mortality in England, 1900-1919. Contin Chang. 1998;13(2):268,273. [ Links ]
13. Lewis M. The problem of infant feeding: The Australian experience from the mid-nineteenth century to the 1920s. J Hist Med. 1980;35(2):174-187. [ Links ]
14. Warwick P. Black people and the South African War 1899-1902. Cambridge: Cambridge University Press, 1983; p. 150-151. [ Links ]
15. Kessler SV. The Black concentration camps of the South African War 1899-1902. PhD thesis, Cape Town, University of Cape Town, 2003. [ Links ]
16. Free State Archives Repository (FSAR). SRC 133, 134. Refugee camps mortality statistics, 1901, 1902. [ Links ]
17. Cd 819. Reports etc. on the working of the refugee camps in the Transvaal, Orange River Colony, Cape Colony and Natal. London: H.M.S.O., 1901; p. 21, 150-152, 164, 194, 331, 333. [ Links ]
18. Cd 853. Further papers relating to the working of the refugee camps in the Transvaal, Orange River Colony, Cape Colony, and Natal. London: H.M.S.O.; 1901. [ Links ]
19. Cd 902. Further papers relating to the working of the refugee camps in the Transvaal, Orange River Colony, Cape Colony, and Natal. London: H.M.S.O.; 1902. [ Links ]
20. Cd 934. Further papers relating to the working of the refugee camps in South Africa. London: H.M.S.O.; 1902. [ Links ]
21. Cd 935. Statistics of the refugee camps in South Africa, 1902. London: H.M.S.O.; 1902. [ Links ]
22. Cd 936. Further papers relating to the working of the refugee camps in South Africa. London: H.M.S.O.; 1902. [ Links ]
23. Cd 939. Statistics of the refugee camps in South Africa. London: H.M.S.O.; 1902. [ Links ]
24. Cd 942. Statistics of the refugee camps in South Africa. London: H.M.S.O.; 1902. [ Links ]
25. Cd 1161. Statistics of the refugee camps in South Africa. London: H.M.S.O.; 1902. [ Links ]
26. National Archives South Africa (NASA), Pretoria. Reports on the Transvaal concentration camps, Director of Burgher Camps, 11-14; no date. [ Links ]
27. Dwork D. The milk option. An aspect of the infant welfare movement in England, 1898-1908. Med Hist. 1987;31:51-52. [ Links ]
28. British concentration camps of the South African War. Mafeking camp [homepage on the Internet]. c2010 [cited 2010 Feb 24]. Available from: http://www.lib.uct.ac.za/mss/bccd/index.php [ Links ]
29. British concentration camps of the South African War. Bethulie camp [homepage on the Internet]. c2010 [cited 2010 Feb 24]. Available from: http://www.lib.uct.ac.za/mss/bccd/index.php [ Links ]
30. British concentration camps of the South African War. Vredefort Road camp [homepage on the Internet]. c2010 [cited 2010 Feb 24]. Available from: http://www.lib.uct.ac.za/mss/bccd/index.php [ Links ]
31. British concentration camps of the South African War. Kimberley camp [homepage on the Internet]. c2010 [cited 2010 Feb 24]. Available from: http://www.lib.uct.ac.za/mss/bccd/index.php [ Links ]
32. Otto JC. [The concentration camps]. Pretoria: Protea Boekhuis, 2005, orig. 1954; p. 139. Afrikaans. [ Links ]
33. Hobhouse EH. War without glamour. Bloemfontein: Nasionale Pers, 1924; p. 127. [ Links ]
34. NASA, MGP 121.1 and 2. Complaints regarding the doctor in Johannesburg camp; 1901 July. [ Links ]
35. NASA, DBC 12. Transvaal camp reports for March 1902; 1902. [ Links ]
36. FSAR, SRC 18/RC 7070. Superintendent Nowers to the Chief Superintendent Refugee Camps; 1902 Feb 7. [ Links ]
37. FSAR, SRC 20/RC7600. Recommendations by Dr Tonkin; 1902 Feb 14. [ Links ]
38. FSAR, SRC 22/RC8215. Views of camp medical officers on the training of probationers; 1902 Mar 21. [ Links ]
39. Marks S. Divided sisterhood. Race, class and gender in the South African nursing profession. London: Macmillan, 1994; p. 68. [ Links ]
40. FSAR, MG 2. Report of Capt. Ross, DC Boshoff; 1900 June 7. [ Links ]
41. FSAR, MG 3. Report for Harrismith district; 1900 Dec. [ Links ]
42. NASA, DBC 12. Report of Inspector N.J. Scholtz on Mafeking camp; 1901 Nov 22. [ Links ]
43. NASA, DBC 12. Director of Burgher Camps report for March 1902; 1902 Apr 18. [ Links ]
44. NASA, DBC 12. Report of the Sanitary Inspector on Krugersdorp camp; 1902 Feb 19. [ Links ]
45. British concentration camps of the South African War. Norvals Pont camp. [homepage on the Internet]. c2010 [cited 2010 Feb 24]. Available from: http://www.lib.uct.ac.za/mss/bccd/index.php [ Links ]
46. National Archives United Kingdom (NAUK), CO 879/75/687, 5359. Lord Milner to Joseph Chamberlain. No. 188; p. 245. 1902 Feb 6. [ Links ]
47. FSAR, SRC 15/RS5979. Report of Dr Pratt Yule; 1901 Nov 1. [ Links ]
48. FSAR, SRC 18/RS7190. Report of Prof PD Hahn; 1902 Jan 8. [ Links ]
49. FSAR, SRC 18/RS7017 (i). Report on the analysis of the Springfontein camp water. 1902 Mar 20. [ Links ]
50. NAUK, CO 879/77/697, 16251. Director of Burgher Camps to the Assistant Secretary to the High Commissioner. No 104; p. 212. 1902 Mar 24. [ Links ]
51. FSAR, SRC 6/RS1683. Superintendent to the Chief Superintendent Refugee Camps; 1901 Apr 29. [ Links ]
52. FSAR, SRC 24/RC8635. Correspondence between Superintendent and Chief Superintendent Refugee Camps; 1902 May 25. [ Links ]
53. NASA, DBC 12. Report of Inspector Captain Bentinck; 1902 Jan 10. [ Links ]
54. DBC 12. Klerksdorp monthly report for April 1902; 1902. [ Links ]
55. DBC 12. Report by Mr. Hall (engineer to Eastern System); 1902 Mar 1. [ Links ]
56. FSAR, SRC 22/RC8243. Proposed water scheme for Aliwal North Refugee Camp; 1902 Apr 18. [ Links ]
57. Raath AWG. [The Boer woman, 1899-1902]. Vol 2. Bloemfontein: Volkskomitee vir die Herdenking van die Tweede Vryheidsoorlog, 2003;backcover. Afrikaans. [ Links ]
58. FSAR, SRC 23/RC8459. Re supplying meat to Refugee Camps; 1902 May 10. [ Links ]
59. Guggenheim KY. Basic issues of the history of nutrition. 2nd ed. Jerusalem: The Magnes Press; 1995. [ Links ]
60. Carpenter EJ. Edward Smith (1819-1874). J Nutr. 1991;121:1515-1521. [ Links ]
61. Johnston VJ. Diet in workhouses and prisons 1835-1895. New York: Garland; 1985; p. 149, 189-190. [ Links ]
62. FSAR, SRC 2/RC486. Report for Edenburg refugee camp; 1901 Mar 1. [ Links ]
63. Drummond JC, Wilbraham A. The Englishman's food. A history of five centuries of English diet. London: Jonathan Cape, 1939; p. 356-359, 449. [ Links ]
64. Cd 893. Report on the concentration camps in South Africa by the committee of ladies. London: H.M.S.O., 1902; p. 167. [ Links ]
65. London School of Economics, LSE 2/11, Streatfield collection; 1901 Sep 22. [ Links ]
66. NAUK, CO 879/75/687, 45124. Memorandum by Dr J S. Haldane on the rations in the concentration camps. No. 79, 1901 Dec 2; p. 66-80. [ Links ]
67. NAUK, CO 879/75/687, 882. Report of Dr Sidney Martin to the Colonial Office. No. 129, 1902 Jan 6; p. 96-101. [ Links ]
68. FSAR, SRC 21/RC7899. CW Champion, Contractor to Chief Superintendent Refugee Camps, Bloemfontein; 1902 Mar 24. [ Links ]
69. NASA, DBC 12. Inspection report on Irene camp; 1902 Jan 16. [ Links ]
70. Murray WA. Health factors in the poor White problem. Stellenbosch: Carnegie Commission. Vol. 4, 1932; p. 3, 31. [ Links ]
71. NASA, DBC 14. Supplementary medical report for Heidelberg camp; 1901 Nov 22. [ Links ]
72. FSAR, SRC 24/RC8498. Suggestions for lady superintendent of camps; no date. [ Links ]
73. Van Heyningen E. The healing touch. The guild of loyal women of South Africa, 1900-1912. S Afr Hist J. 2002;47:24-50. [ Links ]
74. Brink E. Man-made women: Gender, class and the ideology of the volksmoeder. In: Walker C, editor. Women and gender in southern Africa to 1945. Cape Town: David Philip, 1990; p. 273-292. [ Links ]
75. Kruger L-M. Gender, community and identity: Women and Afrikaner nationalism in the volksmoeder discourse of 'Die Boerevrou' (1919-1931). MA thesis, Cape Town, University of Cape Town, 1991. [ Links ]
76. Du Toit M. Women, welfare and the nurturing of Afrikaner nationalism: A social history of the Afrikaanse Christelike Vroue Vereniging, c.1870-1939. PhD thesis, Cape Town, University of Cape Town, 1996. [ Links ]
 Correspondence to:
Correspondence to:
Elizabeth van Heyningen
Postal address:
Department of Historical Studies, University of Cape Town
Private Bag, Rondebosch
7700, South Africa
email: evh@iafrica.com
Received: 30 Nov. 2009
Accepted: 24 Mar. 2010
Published: 08 June 2010
This article is available at: http://www.sajs.co.za


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}