










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work/Maatskaplike Werk
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.60 n.1 Stellenbosch 2024
http://dx.doi.org/10.15270/60-1-1254
ARTICLES
Experiences of social workers in working with health care practitioners: a multidisciplinary team approach
Zama MaxhakanaI; Mbongeni Shadrack SitholeII
IUniversity of KwaZulu-Natal, Department of Social Work, Durban, South Africa https://orcid.org/0000-0002-5794-9001 zmaxhakana@gmail.com
IIUniversity of KwaZulu-Natal, Department of Social Work, Durban, South Africa https://orcid.org/0000-0003-4075-0677 sitholem3@ukzn.ac.za
ABSTRACT
This article uses role theory as a lens to explain the experiences of social workers working within healthcare multidisciplinary teams, which are characterised by interprofessional dominance and subordination. A qualitative case study design was used to explore and describe the experiences of social workers in working with other healthcare practitioners in multidisciplinary teams. A purposeful sampling technique was used to select sixteen participants from a particular health district. Data were collected through interviews and analysed using thematic analysis. Professional power dynamics, a sense of agency with a need for collaborative contribution, and a lack of understanding of the social work profession are three themes that summarise the findings. The article concludes that the ineffective management of multidisciplinary themes creates a barrier to different professionals' ability to communicate, work and learn together. The article recommends preparatory training for multidisciplinary team members and the need for a structured framework for interprofessional engagement.
Keywords: collaboration; healthcare; healthcare practitioner; multidisciplinary team; social worker; teamwork
INTRODUCTION
The multidisciplinary team approach provides a platform for addressing the fragmented functioning in the healthcare setting. The multidisciplinary team approach makes it clear that there is no single professional who can unilaterally provide healthcare for all patients (Vasudevan, 2015). Giles (2019:25) describes a multidisciplinary team as "a group of health professionals from different disciplines working in particular settings such as wards, clinics, rehabilitation centres, assessment centres, or delivery suites". The value of collaboration and teamwork in improving patient care and outcomes is well documented in the literature (Gehlert & Browne, 2012). The literature also reveals that, while multidisciplinary teams have potential benefits, the bringing together of members from different backgrounds can be challenging (Frost, Robinson & Anning, 2005; Zajac et al., 2021). In the main, the multidisciplinary team approach serves as an effective tool to facilitate collaboration among different professionals in pursuit of the best possible patient care and outcomes (Keefe, Geron & Enguidanos, 2009). Braveman and Gottlieb (2014) assert that the influence of healthcare outcomes extends beyond medical and even social factors.
"Globally and in the South African context, the role of social work in health care has been of great value and importance because of its unique position in the health sector" (Petersen & Pretorius, 2022:133). The decentralisation of health care delivery in South Africa has seen the emergence of the multidisciplinary team approach (Lehmann & Gilson, 2013). This approach plays an increasingly important role in providing and managing the integrated quality care of patients. Fraher, Richman, Zerben and Lombardi (2018:176) describe integrated care as the "interprofessional practice that includes both behavioural and physical health". In this regard, practitioners from different backgrounds are expected to make and implement decisions in accordance with their respective scope of practice. Fraher et al. (2018) assert that the role of social workers in integrated healthcare services is not well understood. As members of the allied healthcare workforce, social workers are expected to collaborate with other healthcare practitioners such as doctors, nurses, psychologists, psychiatrists, dieticians, physiotherapists, audiologists, speech therapists and occupational therapists (McLaughlin, 2015). Despite their different professional training, multidisciplinary teams provide the various professionals with the space to communicate, work and learn together. While social workers are responsible for advancing their professional autonomous existence and functioning, they simultaneously share a common responsibility and accountability with the other practitioners in enhancing the patients' wellbeing. The recent study on social work in health care suggests that despite the value of social work practice in counselling and addressing the social determinants of health and the recognition of the profession in multidisciplinary team, social workers are still finding that they are excluded in the consultation process (Petersen & Pretorius, 2022).
This article sought to explore and describe the social workers' understanding of their roles and experiences working with other healthcare practitioners in multidisciplinary teams within the healthcare setting. The research informing this article was mainly guided by the need to effectively integrate social workers into the functioning of the healthcare workforce and subsequent contribution to multidisciplinary teams. The participants in the study were social workers employed by the KwaZulu-Natal Provincial Department of Health. Social workers in various health facilities form part of and work within multidisciplinary teams in their respective districts.
BACKGROUND
Health outcomes are influenced by the interaction of multiple various categories of factors, including medical and social factors. For instance, in relation to the latter, the growth of the social determinants perspective on health could be described as having fostered a crucial place for social work in health (Masi, 2012). Social determinants of health are non-medical factors that can affect a person's overall health and health outcomes, influencing a person's wellbeing, health risk and life expectancy (World Health Organization [WHO], 2010). They can result in an onslaught of emotional, financial and social needs. Social workers are adept at helping patients meet these sorts of needs, hence, the "person-in-environment" configuration becomes relevant (Whitaker & Clark, 2006). While Zapf (2010) regards the notion of "person-in-environment" to have played a valuable role in social work, he advocates for a slightly different metaphor "people as place". Zapf (2010:40) further suggests that the world needs to be "understood as a process of continuous co-creation involving people and the natural world". This means the social work profession is better positioned to understand the co-existence and interactive nature of social factors that influence patients' vulnerability.
In 2018, the KwaZulu-Natal Provincial Department of Health hosted a conference for health social workers for the first time, which was themed "Breaking barriers and building bridges in social work practice within the health sector" (KZN Health, 2018). One of the key findings from the conference was that social work practitioners in the healthcare setting were not receiving the recognition they deserved. There was also a predominant view that clinicians have limited knowledge, particularly about the social work profession's role and its contribution to the healthcare setting. The consequence is that this view has impacted the social work profession's day-to-day roles and responsibilities.
LITERATURE REVIEW
Ranjit (2019) posits that the literature review's central role is to enhance and consolidate the knowledge base and to integrate findings within the existing body of knowledge. In this article, the literature is contextualised and summarised with reference to the roles and experiences of social workers in healthcare multidisciplinary teams. The literature review in this section covers aspects ranging from providing a brief insight into the origin of a multidisciplinary approach in health to outlining the boundaries and the nature of collaboration in a multidisciplinary context.
The origin of multidisciplinary approach in health
It is worth noting that the concepts 'multidisciplinary team' and 'interdisciplinary team' are often used interchangeably, whereas, in fact, they are related but slightly different. Although it is beyond the scope of this article to explain the two concepts, it is worth examining the relationship between the two and providing a brief history of the development of a multidisciplinary team approach. The latter is applicable where each category of professionals works within its particular scope of practice and interacts formally. In contrast, in interdisciplinary teams, there is a significant overlapping of professional roles, communication and shared problem-solving for the patient's good (Sheehan, Robertson & Ormond, 2007). In a multidisciplinary team, one can think about a parallel additively juxtaposing disciplines, whereas interdisciplinary work is characterised by integrated functioning.
The Mayo Clinic is a collaborative organisation credited with the origin of the "multidisciplinary team approach" (Berry, 2004). In the 1920s the organisation first introduced the concept based on the collaborative nature of different professionals. On the other hand, the origin and development of interdisciplinary healthcare teams in the United States (US) could be traced to the World War II successes with multidisciplinary medical and surgical teams (Berry, 2004). This suggests that the multidisciplinary approach preceded the emergence of the interdisciplinary approach. "Interdisciplinary teams in health care originated in the early 1900s with Richard Cabot, who suggested that the social worker, doctor, and educator work together on patient issues" (McAuliffe, 2009: 126).
In South Africa it only been since 1994 that improving the quality of care on a nationwide scale has occupied the governmental agenda (Hlongwa & Rispel, 2021). Although it is still unclear when the concept of a multidisciplinary team was adopted, it stands to reason that this might have emerged with the release of the White Paper for the Transformation of the Health Sector in South Africa in 1997 (Republic of South Africa, 1997).
Social workers' experiences of working within a multidisciplinary team
The literature shows that the presence of "adequate, well-trained, fairly distributed and motivated health workers" is critical to improving the health of a population (Ahmat et al., 2022:1). There are several international studies on the experiences of social workers who are working with healthcare practitioners within a multidisciplinary healthcare setting. A study on healthcare social workers revealed negative workplace experiences that increased the subjective experience of distress (Negura & Levesque, 2021). This is supported by a study on the medical profession's attitude towards the professional practice of healthcare social workers, which found that physicians did not recognise social workers as a group of professionals who can give scientific advice to improve a patient's health (Sierra, 2020). In both instances, social workers have been excluded from the workforce planning team.
Such lack of recognition has resulted in a paucity of information about the scope and functions of social workers employed in healthcare settings (Fraher, Richman, Zerben & Lombardi, 2018). This means that the misunderstanding of social work identity hindered the functionality of social workers within the health sector. Limon's study outlines how each profession in multidisciplinary teams develops its own perspective and scope of practice (2018). Among the main findings is the challenges related to the influences of different professions' scope of practice within the interdisciplinary teams and a lack of effective collaboration. In an ideal situation, social workers play an essential role in patient-centred care at different stages of the rehabilitation process, depending on the problems the patient and his/her family may have (Brannan, Manso & Brownsell, 2009).
Collaborative practice as an ideal towards the management of disease
Collaborative care in patient management can potentially improve health outcomes and reduce the disease burden and healthcare costs for those with chronic conditions (Tapp et al., 2012). Since the care of patients with multiple chronic disorders, such as diabetes and depression, entails high healthcare costs, an effective team approach to manage such complex care is needed (Sierra, 2020). Different health professionals work closely with each other, engaging in discussions during ward rounds and between such occasions, so that there is collaborative patient-centred care in accordance with the patient's needs, instead of individualised services (Saint-Pierrea, Herskovica & Sepúlvedaa, 2018). The dynamic nature of healthcare practice and the work of the related multidisciplinary teams often involves a whole range of professionals. Siant-Pierrea et al. (2018:132) report that the multidisciplinary teams may include "up to 30 professionals, including physicians, nurses, midwives, dentists, physiotherapists, social workers, psychiatrists, dietitians, pharmacists, administrative staff and managers". However, in practice, this kind of ideal is often not achieved without some unintended challenges.
A multidisciplinary team has further proven to enhance clinical outcomes among patients with a range of illnesses. The multidisciplinary team care model for treating HIV infection improved clinical outcomes among HIV patients (Elgalib et al., 2018). Team members work together through care pathways to support patients going through the HIV care continuum from diagnosis to viral suppression. The team members servicing cancer patients are reported to communicate and consult using various tools, including patient health records (Heather, Jasmine, Goffrey, Dunn, & Latini, 2020). For example, the wide range of needs necessitates a multidisciplinary approach towards the care of cardiac patients because of their congenital condition. A collaborative approach not only necessitates a detailed grasp of the patient's underlying cardiac disease, but also open communication among team members. The multidisciplinary team should work closely to ensure integrated quality service delivery (Hussain & Wooller, 2004).
Boundaries and collaboration in multidisciplinary teams
Social work has a history of interactions and decision-making with members of its profession and those from other disciplines. This form of networked sense-making plays a fundamental role in professional judgement. Perriam (2015) reports that hospitals are viewed as medical facilities controlled by medical professionals. Choi and Pak (2006: 355-356) describe multidisciplinarity as "an approach when experts from different fields work together on a common subject within the boundaries of their own discipline". As a secondary profession in the healthcare environment, social workers find themselves having to operate within the boundaries and hierarchies often set up and dictated by the medical profession. The question of power determines the degree to which effective collaboration can occur. Health social work is performed in the healthcare sector, particularly in a hospital setting, where the agency's primary role is medical treatment rather than social work. In this regard, social workers are responsible for providing secondary services. When disciplinary groups are seen to be afforded unequal status, the dominant group can set the expected performance criteria and practices in ways that limit the contribution of other group members (Atwal & Caldwell, 2005). The subordination of social workers in multidisciplinary teams could be viewed as depriving them of the opportunity to contribute towards the success of medical and social intervention.
ROLE THEORY
Role theory was found to be relevant as an explanatory lens focused on the experiences of social workers who are working with other healthcare practitioners in multidisciplinary teams. In the process, they are able to describe their role and the roles of their counterparts in multidisciplinary teams. In general, role theories aim to "examine how individual behaviour is shaped by prevailing social roles and provide insights into how behaviour is perceived by others in light of such roles" (Anglin, Kincaid, Short & Allen, 2022: 1469).
Biddle (1986) described the term 'role' as suggesting that the theory began life as a theatrical metaphor. Unlike theatrical contexts, where actors perform parts predetermined by written scripts, social contexts enable social actors to perform their roles as understood within specific contexts (Biddle, 1986). Biddle (1986) also points out that the role theorists agree that role in social contexts is associated with three basic concepts: role, social position and expectations depicting the characteristic behaviours, parts to be played, and scripts for behaviour. However, the theorists are reported to differ primarily on the modality of expectation. "Whereas many role theorists assume that expectations are norms (i.e. prescriptive in nature), others assume them to be beliefs (referring to subjective probability), and still others view them as preferences (or 'attitudes')" (Biddle, 1986: 69).
ETHICAL CONSIDERATIONS
Polit and Beck (2021) describe ethics as a set of moral principles and values that would apply during the research project. In this study, the ethical principles adhered to are outlined below.
Permission to conduct a study
The study was conducted in the King Cetshwayo Health District situated in DC28 Northern KwaZulu-Natal. The District Director of King Cetshwayo Health District granted permission to conduct the study. The ethical approval was secured from the Department of Health, KwaZulu-Natal Provincial Health Research and Ethics Committee (PHREC - 202001-009) and the University of KwaZulu-Natal's Humanities and Social Sciences Research Ethics Committee (HSSREC-00000603/2019).
Informed consent and use of a recorder
When the participants agreed to participate in the study, they were emailed the informed consent forms. Interview guides were also made available before interviews were conducted. The informed consent form contained a section on permission to record the interviews. The participants were provided an opportunity to indicate whether they agreed or disagreed with the recording of telephonic interviews. None of the 16 participants objected to the recording of interviews.
Avoidance of harm
According to Creswell and Creswell (2018), most of the possible harm to participants in the social sciences is often related to emotional factors. Towards the end of each telephonic interview, a debriefing was conducted with each participant to help them to return to a stable state. In addition, a system was in place for those likely to have more persistent problems to be referred for further intervention.
Voluntary participation
Detailed information was provided to participants before they took part in the study. This enabled them to be clear about what the study entailed and what was expected of them. They were also reminded that they were at liberty to withdraw at any stage of the data-collection cycle, should they decide to do so.
Confidentiality
Polit and Beck (2021) state that a promise of confidentiality is a pledge that any information the participants provide will not be publicly reported in a manner that identifies them, not will it be made accessible to others. The researchers ensured that there was no breach of confidentiality. The information shared was treated with confidentiality, and the identity of the participants was concealed by using alphabetical labels.
METHODOLOGY
This study assumed a relativist ontology. As Rashid et al. (2019: 3) point out, a relativist ontology rejects the existence of the objective world or truth, and argues that "everything is relative and created by social beings". This paradigm served to highlight the relational nature of the interaction between the participants and their counterparts in multidisciplinary teams. Based on the contextual conditions pertinent to a case (Yin, 2018), an exploratory case study design was relevant in exploring the experiences of social workers in collaborating with other healthcare practitioners in a multidisciplinary team context. The participants were not viewed based on their individual existence in multidisciplinary teams, but were defined in terms of their experiences as collective elements of the case.
Locality
The study location was chosen based on its contribution within this particular healthcare setting. King Cetshwayo Health District is the third largest in KZN Province, and the first one serving mostly rural communities. It has a population of 972 856 and consists of six local authority areas (KwaZulu Natal Department of Health, 2018). It is comprised of two regional hospitals, six district hospitals, 57 fixed clinics, 1 Community Health Center and 14 mobile clinics with 66 stopping points (KwaZulu Natal Department of Health, 2018).
Sampling
This study gathered qualitative data from 16 social workers recruited through the King Cetshwayo District Health Forum. The population identification and sampling selection were guided by the nature of the research problem and the relevance of the case study as a research design. Of 216 staff complement, 16 social workers were purposefully selected from the King Cetshwayo Health District health facilities in KwaZulu-Natal. A forum in a public health setting involves a group of social workers that meets on a regular basis as prescribed in the Health Department's policy to discuss the challenges, best practices and new developments associated with their work and profession. The different District Health Fora are accessible to full-time social workers employed by the KwaZulu-Natal Department of Health in terms of the Public Service Act 103 of 1994 (Republic of South Africa, 1994). The forum was informed about the study and those interested in participating were requested to consult the first author. The selection process was undertaken on first-come-first-served basis until saturation was reached.
The inclusion criteria, which could also depict the features of a case, involved the following:
(i) Participant had to be employed as a social worker in the healthcare sector;
(ii) Participant had to be placed in one of the facilities in King Cetshwayo District Municipality;
(iii) Participant had to be a member of one of the social work district fora;
(iv) Participant had to be involved in the multidisciplinary teams;
(v) Participant had to be prepared to participate in semi-structured telephonic interviews.
The informed consent forms and interview schedules were emailed to the participants before the interviews were conducted. The interviews were arranged upon receipt of the signed informed consent forms. Because of the restrictions related to Covid-19, the interviews were held telephonically. Each telephonic interview lasted approximately 30 to 45 minutes. The collected data were transcribed and then analysed using thematic analysis. Braun and Clarke (2006) describe thematic analysis as a method of identifying, analysing and reporting patterns (themes) within data.
FINDINGS
The findings of this study are summarised here using themes and subthemes, in accordance with the principles of thematic analysis. Before presenting the respective themes and subthemes, it is worth outlining the participants' profile.
Participants' profiles
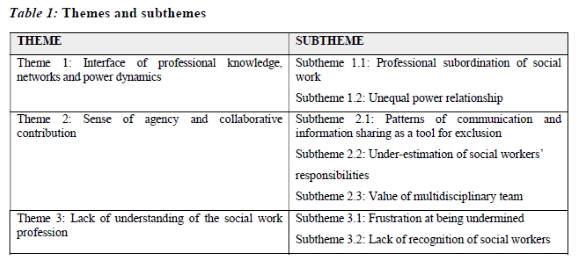
The participants' profile consisted of sixteen participants, namely thirteen females and three males aged between 30 and 50. The participants' years of experience ranged from five to 25 years. Furthermore, most participants reported being exposed to and/or being members of multidisciplinary teams in health care settings. Analysis of the interview data was divided into the theme and subthemes outlined in Table 1.
Presentation of themes
Three themes emerged from this study. Table 1 outlines the respective themes and the related subthemes.
Theme 1: Interface of professional knowledge, networks and power dynamics
Social workers were asked to describe their working relationship with other health practitioners in multidisciplinary teams. From their responses it became apparent that there is an interaction of three elements: professional knowledge, networks and power dynamics. McDonald, Jayasuriya and Harris (2012) describe power dynamics as unfolding through power differences based on unequal professional status. The hierarchical professional dominance and subordination in the health professions is attributed mainly to the traditional deployment of power by health professionals, particularly doctors, to protect their professional autonomy and independence as well as their professional status in their relationships with other healthcare workers (McDonald et al., 2012).
Ideally, the multidisciplinary team approach exposes social workers to networks that enable them to assert their professional roles within prevailing power structures. The harsh reality in health settings is that multidisciplinary teams do not afford different professionals similar status or opportunities to express their professional knowledge. This could be viewed as defeating the philosophy designed to drive teamwork among individuals with different perspectives (McAuliffe, 2009). Long (2001) identifies the cultural and institutional factors that are responsible for uneven development in organisations. Furthermore, Long (2001:170) regards the generation and transformation of knowledge as "an outcome of the interaction, negotiation, interface and accommodation that take place between different actors and their life worlds".
Saint-Pierrea et al. (2018) regard teamwork as providing different types of staff the opportunity to work together to share expertise, knowledge and skills that impact on patient care. While this may sound like an easy, voluntary process, the reality in practice suggests that different professionals are not provided such space in equal measure. The participants in the study described their working relationships as entailing that their professional roles and judgements are subjected to scrutiny. Below are some relevant extracts as expressed by participants.
I think the nature of the environment contributes to the fact that medical practitioners are superior, and that we have to abide by what they say. Hospitals are known to be operated by doctors, as a result they are given more power than any other professionals.
The participants' comments also revolved around the hierarchical nature and power imbalances of the relations in the health settings. Hierarchical power dynamics inhibit team communication and the ability to assert oneself, impacting the team's effectiveness and patient safety. Long (2001) asserts that a social actor or entity can meaningfully be afforded the power of agency -the capacity to process experience, make decisions and act upon them. In another study, Nkuna (2016) recommends ensuring non-hierarchical relations among professionals in multidisciplinary teams.
The social workers expressed a prevailing sense of powerlessness and lack of confidence within the multidisciplinary team. This pattern of subservience could be viewed as detrimental to the very sense of multidisciplinary, namely the pursuit of a common goal. Biddle (1986) describes such conformity as compliance with some pattern of behaviour. This behavioural pattern could be viewed as sustained through the principle of a "self-fulfilling prophecy" (Biddle, 1986:80).
The comment below conveys a sense of protest at accepting the perceived elevated role of doctors over other professions.
Only doctors have a right to discharge patients. There is nothing as heartbreaking as finding your patient discharged without being informed.
"Kunzima ukuba usonhlalakahle esibhedlela" - meaning it is difficult to be a social worker in a hospital setting.
Another participant shared similar sentiments:
It is frustrating, draining and emotionally exhausting, not because of the nature of our work but because of the treatment we receive from MDT.
The two participants described social workers in the healthcare setting as experiencing the challenges of exclusion from decision-making processes. The two quotes reflect the kind of treatment they go through and the extent to which the exclusion impacts them. They revealed how they were excluded from participating in decision-making processes involving their cases. For instance, the patients would be discharged without anyone seeking their professional opinion. This also contributed to a lowering of morale with regard to the multidisciplinary team approach.
In the main, this theme depicted the challenges associated in a multidisciplinary environment with social work as a profession perceived to be subservient and within a context of unequal power relations, as substantiated in the subthemes below.
Subtheme 1.1: Professional subordination of social work
The participants were asked to state how their services were perceived in multidisciplinary teams.
The participants did not only state that their profession was perceived as subservient by the entire healthcare sector, but also that other healthcare practitioners unjustifiably gave them instructions on what they needed to do. Perriam (2015) states that the medical model provides doctors with the space to run the hospitals, which in turn reinforces their status and power over other professions. This could be attributed to the perceived devalued voices of members of non-medical disciplines.
Our profession is wrongly perceived. We have to report to the medical teams, and sometimes they instruct us. We end up not doing our assessment, intervention and plan of action.
This statement confirms the findings in a study conducted at Charlotte Maxeke Academic Hospital on social workers' experiences working within multidisciplinary teams, revealing that social workers are undermined and disrespected (Nkuna, 2016). Some participants' responses revealed that they were aware of the constant actions aimed at undermining their profession and the subservient position in which the profession has been placed. Seemingly, they also appear to lack the power to remedy the situation.
Most of my referrals will be telling me what to do. For example, "Please find a placement, the patient has been discharged with no relatives; poor compliance; provide counselling; SAM case assesses home circumstances". We do not tell doctors what to do about their patients and profession, why must we be told?
We are always asked to do things that are out of the scope of practice. Often indigent patients will be referred to our offices for bus fare, yet we are not given petty cash. When we refuse to do it, we would be questioned about our role.
Subtheme 1.2: Unequal power relations
The participants' responses to the question about relations in multidisciplinary teams, tended to be influenced by their interaction with other healthcare practitioners as well as the context in which they operate. Lehmann and Gilson (2013) assert that understanding the operations of power allows a more nuanced understanding of the roles and influences of multiple actors in social relations. Key in this regard is understanding that the power relations are relationally and contextually dependent. To some participants, the multidisciplinary teams tended to foster power inequities, with medical professionals having more authority over non-medical professionals. Power inequality affected social workers' voices and contributions within the multidisciplinary team. Medical doctors, in particular, were found to be afforded greater power comparatively.
I feel my work is less valued because my contribution would never be considered. There is a lot that we do; no one will recognise our work, even the extra efforts we put [in].
Unlike medical teams who work in consultation with senior members of their profession, social workers in healthcare are reported to be working in silos, without support. As a result, individual members enter the multidisciplinary teams with different levels of understanding of the capabilities of other professions.
We feel left behind, as if we are less important. Sometimes, our contributions and efforts are not recognised, which lowers our morale when working within a multidisciplinary team.
The above comments reveal a shortcoming in attempts to make a meaningful contribution to their teams. Multidisciplinary team members are valued for their complementary skills, qualifications and experience. Participants spoke about the importance of collaboration between health professionals and social workers as the National Association of Social Workers (2021) reiterated that social work is not an individual effort but a team effort.
Theme 2: Lack of multidisciplinary collaboration
the multidisciplinary team approach is an essential basis for collaboration in resolving real-world or complex problems (Choi & Pak, 2006). Choi and Pak (2006) distinguish multidisciplinarity from interdisciplinarity and transdisciplinarity by stating that, while all draw on knowledge from different disciplines, multidisciplinarity tends to enable different disciplines to stay within their boundaries. The healthcare setting ideally needs to be an effective space and vehicle for collaboration and engagement. Saint-Pierrea et al. (2018:133) describe collaboration in the healthcare context as a complex process, involving "problem-solving, shared responsibility for decision-making and the ability to carry out a care plan while working towards a common goal". Most participants acknowledged a multidisciplinary team approach as being ideal for promoting optimal patient care and outcomes. However, they shared concerns that a lack of effective collaboration in multidisciplinary teams demotivated them from functioning fully in the teams. Lehmann and Gilson (2013) regard collaboration not only as a relational phenomenon, but also as being context-dependent.
The collaborative structures and processes, therefore, became the essential points of focus in this study. Löwe, Mark, Sommer and Weltermann (2022) regard patient-centred case management as central to professional collaboration. Taberna et al. (2020:2) describe case management as the "systematic effort to coordinate patient and family care in this complex pathology". While the literature emphasises collaboration, the situation in practice proved to be the opposite.
One participant shared the following:
The relationship is poor because they remember our existence when they encounter challenges that require our expertise.
The absence of social workers' input in the teams could indicate the missing piece of the puzzle. Failure in this respect could, therefore, imply the compromised identification of social needs, inadequate access to support and a hindrance to full recovery. The participants expressed concern that the patients' rights to be involved in the decision-making process would be undermined in their absence.
I always receive late referrals. Health practitioners will be working with the patient all the way and notice on discharge that the patient has social issues. I will be pushed to finalise my cases because of bed status.
This theme noted decisions about hospital discharges being made on the grounds of costs, availability of beds and the needs of the hospital rather than the patients' needs. Participants also pointed out that ongoing patient care is best provided when various health professionals work together.
Subtheme 2.1: Patterns of communication and information sharing as a tool for exclusion
Communication and shared information are essential tools to influence and sustain relations in teams. Sheehan et al. (2007) state that the members of multidisciplinary teams are expected to understand the communication protocols within their scope of practice, and to simultaneously relate to other members across disciplines. Unless members are mindful of this, the communication gap often widens. The participants revealed that a lack of effective communication within multidisciplinary teams impacts their service delivery.
The responses from the participants included comments on their exclusion, ranging from not receiving invitations to meetings or receiving invitations after meetings have been concluded, to the use of medical jargon exclusive to members of the medical profession.
I have learned to do and focus on what I am paid to do. Communication is a two-way street.
Participants spent much time talking about the importance of communication in multidisciplinary teams. The key issue raised in this regard was the use of communication by the dominant professions as a way to exclude other professions, or a lack of any communication at all.
There is no relationship between social workers and healthcare professionals. We are sometimes informed later after the meetings about multidisciplinary teams. Nobody recognises our existence. Even when there is a record of our interventions in the patient's file, the medical practitioner would continuously ask for a feedback report.
My challenge is the medical terminology used during MDT meetings and engagement with the health practitioners. I believe medical practitioners should take responsibility for providing information and clarity on medical terms. This is a clear indication of poor collaboration.
Participants expressed concern about the nature of the collaboration between professionals and added that they have to work hard to maintain their authority over their expertise.
Subtheme 2.2: Underestimation of social workers' responsibilities
The participants were asked to describe their roles in the multidisciplinary team. The response was that their roles were to provide psychosocial assessments and interventions, to advocate for patients and their families, and to provide counselling and emotional support to patients who experience poor social functioning. However, social workers felt that their roles were underestimated, in the sense that they would receive late referrals close to discharge and be pushed to finalise cases.
Despite many years of experience in the health setting, I have learned coping skills to work under stressful conditions whereby medical practitioners would tell me what to do and how to do it.
Role clarity is described as important in work groups (Hassan, 2013). Whilst social workers may be expected to clarify and educate team members on their roles, the stressful nature of their work situation, tends to push them to find some coping mechanisms.
Our assessments are unfairly scrutinised. For example, looking for placement of a patient is time-consuming, requiring active involvement of stakeholders and external resources. While working on the cases, social workers often subjected to unreasonable demands to produce the action plans.
Both statements reflect that the participants are aware of the significance of role clarification in multidisciplinary teams. However, they appear to have learnt not to address that shortcoming. In the healthcare setting, healthcare practitioners' focus is on medically-related patient needs, while social workers' focus is contribution to psychosocial interventions for the benefit of patients and their immediate families. Role clarification may prevent unnecessary role ambiguity and, therefore, "lead to beneficial outcomes in workgroups" (Hassan, 2013:722).
Subtheme 2.3: Value of the multidisciplinary team
As to how they envision the value of multidisciplinary teams in patient-centred care, the participants were clear about what a functional multidisciplinary team should look like.
Of course, we have a role to play in a multidisciplinary team, but this can only be effective when there is collaboration.
A multidisciplinary team produces better patient outcomes. Without team members working together as a team, there will be no functionality in multidisciplinary teams.
A few participants revealed how much multidisciplinary teams can contribute to patient care for better service delivery outcomes. However, concerns about the lack of teamwork within multidisciplinary teams were raised. Okpala (2020) reiterates that the unequal power balance among professionals in healthcare influences their effectiveness.
Theme 3: Lack of understanding of the social work profession
The participants revealed varying opinions on how multidisciplinary teams viewed the role of social workers. The prevailing constructs of the role of social work demonstrated misunderstanding, misconception, misinterpretation and confusion. According to Stevens, Hulme and Salmon (2021), the negative consequences of these limitations may be manifested when health professionals in positions of power were found, whether intentionally or not, to influence their colleagues to perform inappropriate or unsafe actions, or disregard appropriate advice. The participants in this study emphasised serious misinterpretations of the social work profession particularly by the medical professions.
I receive inadequate support because my role is not understood. Lack of support includes even the lack of appropriate resources. I am expected to provide transport fare for indigent patients, yet there is no budget allocated for this responsibility.
Beder (2008) states that social workers have been providing services in hospitals for over 100 years; the function of the hospital is primarily to provide medical care, not social services. As such, social workers are often perceived as secondary professionals in this host setting. On the other hand, professional power, authority and prestige are accorded to physicians (Gregorian, 2005). As Petersen and Pretorius (2022) assert, in rendering their services, social workers often draw on interventions guided by anti-discriminatory practices. There seemed to be no indication that they were able to do that in situations impacting directly on them.
Due to different views and understanding, we sometimes fight over the best suitable patient treatment.
This participant acknowledged the fact that since team members have different backgrounds and levels of expertise, this might inhibit team communication, and hence social workers discovered that little is known about their role and their contribution to the healthcare setting. This subsequently led to the profession being considered as providing a non-critical and non-essential service. Lack of recognition impacted on the quality of collaboration within the multidisciplinary team.
Subtheme 3.1: Frustration at being undermined
In relation to this exploration of how satisfied the participants were with the multidisciplinary team understanding of their role, one could have expected that, at least, the healthcare sector would be comparatively ahead of other sectors in embracing this phenomenon. As Choi and Pak (2006) assert, multidisciplinarity is about drawing on knowledge from different disciplines, while allowing them to remain within their boundaries. The participants revealed that patients would be discharged while they were still working on the case without them being informed.
It is quite overwhelming not to be involved at the beginning of the process or planning. When they feel that they cannot solve a problem, it is only then they would call us to intervene.
In this regard, social workers expect to be treated as a key resource, instead of being a last resort called upon when there are cases that other team members are unable to handle. The participant's response does not only reflect the dominance of traditional healthcare professions over social work profession, but also that, in the process, such relations pose a threat to effective support to patient care.
In the true sense, multidisciplinary team meetings are supposed to be the platform where all members gather and share their involvement in patient care. The lack of a coordinator for a multidisciplinary team results in poor information sharing. Doctors and nurses care for the patients' physical needs, but are not trained to deal with other issues. There is much focus on authority and less focus on clarity of roles in multidisciplinary teams.
Social workers were distressed that other team members did not see the value of social workers being part of the team. This was because there was a demonstrably limited understanding of the social worker's role.
Subtheme 3.2: Lack of recognition of social workers
Lack of recognition was one of the biggest challenges for the social workers in the multidisciplinary teams. Frost (2005) argues that professionals need the space to provide their services with a degree of freedom and discretion.
I believe that the reason we are not supported relates to being supervised by the medical manager, who has no idea of what social work is.
Some of the social workers acknowledged that the field of social work is broad and expansive, and as a result the nature of the profession can be difficult to grasp in full. The conflict within the teams could be attributed to the prevailing professional hierarchy. The participants' frustration regarding the disrespect afforded their profession cannot be overemphasised. In this regard, social workers do not only feel overlooked in terms of being appreciated and acknowledged, but they feel that such disregard often amounts to contempt for their profession. For instance:
One doctor said social work renders services that can be rendered by anyone. Sometimes we are expected to drop everything we do to attend the multidisciplinary team meetings that were planned without us being involved.
A recent review by Okpala (2020) identified five domains that influence team power dynamics in healthcare: team-related factors, role allocation, communication, trust and respect, and individual traits. The implication is that effectively managed multidisciplinary teams are essential in ensuring the achievement of functional patient care and outcomes.
DISCUSSION
The discussion revolves around the notion of partnership across professional and organisational boundaries in multidisciplinary teams. From the outset, it became apparent that one of the main challenges in effectively implementing a multidisciplinary team approach in healthcare is a lack of integration and collaboration among the parties providing care. The study revealed that partnerships in multidisciplinary teams are shaped mainly by professional power dynamics and communication, or the lack thereof. Common in this regard are the differential decision-making processes and statuses afforded to different professionals. Haines, Perkins, Evans and McCabe (2018) revealed that multidisciplinary teams tend to be characterised by traditional hierarchal power relations. Social workers in the multidisciplinary teams perceived themselves to be afforded a low status in the hierarchy.
Several factors were found to hinder collaboration among the multidisciplinary teams. Among others were the organisational characteristics such as power dynamics and the actions of individuals and the perceived status of their profession (Steihaug et al., 2016). This is supported by Nkuna (2016), who revealed that although social workers are important actors in the health sector, they are still not fully recognised as important role players in multidisciplinary teams. Similarly, social workers in this study reported having been alienated in the multidisciplinary teams because of the team members' lack of understanding of the social work profession and its role. This exclusion could be attributed to the predominant perception that social workers in healthcare settings are responsible for providing only secondary services. In this regard, participants felt undermined when they were told what to do by other team members. Based on their experiences, the social workers came to understand that the other health professionals saw the status of their profession in the health setting as subordinate. The analysis further revealed a consistent pattern of inappropriate wielding of power by other healthcare practitioners, particularly doctors in multidisciplinary teams: their dictating in social work practice, exerting of stereotypes among health professionals, and their assumption of greater recognition and acting as the sole decision-makers regarding patient care. As Petersen and Pretorius (2022:133) assert, even though the mandate of the social worker in healthcare
focused on counselling to sustain emotional and physical wellbeing and address the impact of disease, attending to the SDH [social determinants of health] (i.e. discharge planning, addressing compliance and other social issues) may be more important.
Addressing the social determinants of health to enable compliance and adherence to treatment regimes, marks the comprehensive responsibility unique to social work in health care.
Holder, Kumpunen and Castle-Clarke (2018) emphasise that health care and social work care are dependent on one another to succeed. Yet Steihaug et al. (2016) found that lack of appropriate collaboration among the teams caused division among members. This means that for effective collaboration to happen, health and social work practitioners need to address the barriers between them to have an impact on quality patient care. Clwyd and Wood (2013) identified various difficulties social workers face when working in a multidisciplinary team. For instance, to be heard by medical colleagues, social workers frequently have to pound on the metaphorical door. Secondly, managers of social work organisations are frequently excluded from key decision-making processes. The content elicited from the participants reflected how their role is underestimated as well as the difficulties they experienced in functioning and collaborating with different disciplines, particularly the medical discipline. This research suggests that the participants viewed their experiences in multidisciplinary teams in a negative light and appeared to develop a reluctance to be part of the team.
Lack of collaboration negatively impacted the working relations within a multidisciplinary team. Macdonald et al. (2010) assert that knowledge of the professional role of others is one of the key competencies of inter-professional, collaborative practice for patient-centred care. Furthermore, knowledge of the professional roles of others is associated with behaviour related to inter-professional practice. The lack of awareness specifically about the role of social workers impacted the effectiveness of their social work intervention outcomes. In his study on the professional identity and knowledge of health social workers, Beddoe (2013) found that the limited knowledge about social work practice had an effect on the respect afforded their professional identity and status in a multidisciplinary setting. A survey conducted with social workers revealed that there is limited understanding of social work practice, by other disciplines as one and this hinders social workers' ability to deliver effective service (Ashcroft, McMillan, Ambrose-Miller & Brown, 2018). By extension, social workers could play a key role in enabling collaboration among client systems. It is unfortunate, then, that in multidisciplinary teams, social workers are not able to evince the professional responsibility considered as essential expertise in their practice (Kennedy, 2019).
CONCLUSION
The participants' experiences of working with other healthcare professionals in multidisciplinary teams appeared to entail more challenges than gains, and more unfavourable consequences than development opportunities. It is worth mentioning that the origin of the multidisciplinary approach was in the health sector, and it is not a coincidence that teamwork involving multiple disciplines is increasingly emphasised in health services. This study not only afforded social workers with a space to share their views, but also provided valuable insights into the functioning of multidisciplinary teams. Since its formation, the healthcare sector has been presented as a structure characterised by the dominance of certain professions and the exclusion of others, and where non-medical disciplines and professionals have experienced a dire sense of being side-lined.
Despite the critical role of social workers in multidisciplinary teams, they still experienced the challenge of dominance and exclusion by other healthcare practitioners. There is no indication of the advancement of inter-occupational functioning in the distribution of health services, and policymakers should take into account social care proposals to allow for the delivery of quality health services. The study also revealed some challenges regarding patient discharge planning. In order to create good working relationships, a clear discharge plan is recommended to serve as a key guideline for all the parties involved.
Lastly, the lack of understanding of other professions in multidisciplinary teams will likely pose challenges for non-medical professionals, in particular. In this regard, the professionals who are privileged with more power and status over others may influence their counterparts into conducting themselves in inappropriate or unsafe ways, or with disregard for appropriate advice.
RECOMMENDATIONS
It became apparent from the study, that a lack of enacting an effective multidisciplinary team approach has a number of consequences for the organisation, professionals and especially for the patients. For multidisciplinary teams to be effective, four recommendations are worth noting. There is a need for the acknowledgement of the essential role of social workers in multidisciplinary teams, instead of perceiving them as merely providing a secondary service. In order to deliver integrated health care, the chairpersons of multidisciplinary teams need to provide guidance in the formulation of standard operational guidelines for collaboration. Secondly, it was evident that the effective administration of multidisciplinary teams was not affected by a lack of integrated services, but by a lack of understanding and embracing of the diverse range of professional roles. The domination of some professional voices and suppression of others could be attributed to this challenge. There is a need to provide preparatory training for multidisciplinary team members to ensure effective engagement and shared communication. This can be done by developing interprofessional training programmes, namely workshops, seminars and related interventions.
Thirdly, social workers cannot continue wearing the victim cap. Having been trained in advocacy roles, they have a responsibility to advance their professional interests within the healthcare setting.
Lastly, the multidisciplinary team approach is, by design, understood to be a complex process, not without implementation barriers. In this regard, there is a need for a restructured framework for interprofessional engagement. This may be realised through reorganisation and framing of power and authority relations among different professions within multidisciplinary teams, so as to provide space for their equal and effective participation.
LIMITATIONS
The researchers acknowledge two main limitations of the study. A case study method was used in the study involving one out of eleven health districts in the province of KwaZulu-Natal. The findings from this case were too limited for them to be generalised, but may be tested and replicated in situations of a similar nature taking into account the essential role of context in multidisciplinary teams. Secondly, as depicted in the literature review section above, the multidisciplinary team approach is acknowledged to have been only recently formalised in the KwaZulu-Natal Department of Health. It is, therefore, no accident that there are still no clear processes followed.
ACKNOWLEDGEMENT
The researchers acknowledge the supportive role played by the King Cetshwayo Health District in granting permission to undertake the study and particularly the health social workers' willingness to share their views through participation in this study.
REFERENCES
Ahmat, A., Okoroafor, S. C., Kazanga, I., Asamani, J. A., Millogo, J. J. S., Illou, M. M. A. S., Mwinga, K. & Nyoni, J. 2022. The health workforce status in the WHO African Region: Findings of a cross- sectional study. BMJ Global Health, 7: 1-8. [ Links ]
Anglin, A. H., Kincaid, P. A., Short, J. C. & Allen, D. G. 2022. Role theory perspectives: Past, present, and future applications of role theories in management research. Journal of Management, 48 (6): 1469-1502. Doi: 10.1177/01492063221081442 [ Links ]
Ashcroft, R., McMillan, C., Ambrose-Miller, W. & Brown, R. M. 2018. The emerging role of social work in primary healthcare: A survey of social workers in Ontario Family Health Teams. Health & Social Work, 43(2): 109-117. [ Links ]
Atwal, A. & Caldwell, K. 2005. Do all health and social care professionals interact equally? A study of interactions in a multidisciplinary team in the United Kingdom. Scand J Caring Sci, 19(3): 268-273. [ Links ]
Beddoe, L. 2013. Health social work: Professional identity and knowledge. Qualitative Social Work, 12(1): 24-40. [ Links ]
Beder, J. 2008. Evaluation research on social work interventions: A study on the impact of social worker staffing. Social work in health care, 47(1): 1-13. [ Links ]
Berry, L. L. 2004. The collaborative organization: Leadership lessons from Mayo Clinic. Organizational Dynamics, 33(3): 228-242. [ Links ]
Biddle, B. J. 1986. Recent development in role theory. Annual Review of Sociology, 12: 67-92. [ Links ]
Brannan, D., Manso, S. & Brownsell, S. 2009. Telerehabilitation: Enabling the remote delivery of healthcare, rehabilitation, and self-management. National Library of Medicine. StudHealth Techrol Inform, 145(3): 231-248. [ Links ]
Braun, V. & Clarke, V. 2006. Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2): 77-101. [ Links ]
Braveman, P. & Gottlieb, L. 2014. The social determinants of health: It's time to consider the causes of the causes. Public Health Reports, Supplement, 2(129): 19-31. [ Links ]
Choi, B. C. K. & Pak, A. W. P. 2006. Multidisciplinarity, interdisciplinarity and transdisciplinary in health research, services, education and policy: 1. Definitions, objectives, and evidence of effectiveness. Clin Invest Med, 29(6): 351-364. [ Links ]
Clwyd, N. & Wood, M. 2013. All-Party Parliamentary Group on Social work inquiry into the state of social work report. Birmingham Melbourne: British Association of Social Workers. [ Links ]
Creswell, J. W. & Creswell, J. D. 2018. Research design qualitative, quantitative, and mixed methods approaches. 5th ed. Thousand Oak: SAGE [ Links ]
Elgalib, A., Al-Sawafi, H., Kamble, B., Al-Harthy, S. & Al-Sariri, Q. 2018. Multidisciplinary care model for HIV improves treatment outcome: A single-centre experience from the Middle East Aids Care. Journal of Aids Care, 30(9): 1114-1119. [ Links ]
Fraher, E., Richman, E., Zerben, L. & Lombardi, B. 2018. Social work student and practitioner roles in integrated care settings. American Journal of Preventive Medicine, 54(6): 5281-5289. [ Links ]
Frost, N. 2005. Professionalism, partnership and joined-up thinking: A research review of front-line working with children and families. [Online] Available: https://lx.iriss.org.uk/sites/default/files/resources/Professionalism_partnership%20and%20joined%20up%20thinking.pdf. [Accessed 29/08/2022]. [ Links ]
Giles, R. 2019. Social workers' perceptions of multi-disciplinary team work: A case study of health social workers at a major regional hospital in New Zealand. Aotearoa New Zealand Social Work, 28(1): 25-33. [ Links ]
Gregorian, C. 2005. A career in hospital social work: Do you have what it takes? Social Work in Health Care, 40(3): 1-14. [ Links ]
Haines, A., Perkins, E., Evans, E. & McCabe, F. 2018. Multidisciplinary team functioning and decision making within forensic mental health. Mental health review (Brighton, England), 23(3): 185-196. [ Links ]
Hassan, S. 2013. The importance of role clarification in workgroups: Effects on perceived role clarity, work satisfaction, and turnover rates. Public Administration Review, 73(5): 716-725. [ Links ]
Heather, H., Jasmine, E., Goffrey, J., Dunn, M. & Latini, D. 2020. Collaboration between oncology social workers and nurses: A patient-centered interdisciplinary model of bladder cancer care. Seminar in Oncology Nursing, 37(1): 114-151. [ Links ]
Hlongwa, P. & Rispel, L. 2021. Inter-professional collaboration among health professionals in cleft-lip and palate treatment and care in the public health sector of South Africa. Hum Resource Health, 19(25): 98-103. [ Links ]
Holder, H., Kumpunen, S. & Castle- Clarke, S. 2018. Managing the hospital & social care interface: Intervention targeting older adults. Research report, Nuffield trust. [Online] Available at https://wwwnuffieldtrust.org.uk/research/managing-the-hospital-and-social-care-interface [Accessed 23/11/2020]. [ Links ]
Hussain, F. & Wooller, D. 2004. A multidisciplinary approach to cardiac rehabilitation care. Nursing Times, 10(25): 38-40. [ Links ]
Keefe, B., Geron, S.M. & Enguidanos, S. 2009. Integrating social workers into primary care: Physician and nurse perceptions of roles, benefits, and challenges. Social Work in Health Care, 48(6): 579-596. https://doi.org/10.1080/00981380902765592. [ Links ]
Kennedy, J. 2019. The importance of relationships in social work. Care knowledge. Hove: Pavilion Publishing & Media Ltd. [ Links ]
KwaZulu Natal Department of Health. 2018. Breaking barriers and building bridges for social work practice in healthcare. KwaZulu Natal Department of Health Social Workers' conference. [Online] Available: http://healthweb.kznhealth.gov,za. [Accessed 12 November 2022]. [ Links ]
Lehmann, U. & Gilson, L. 2013. Actor interfaces and practices of power in a community health worker programme: A South African study of unintended policy outcomes. Health Policy and Planning, 28: 358-366 doi:10.1093/heapol/czs066. [ Links ]
Limon, E. 2018. Challenges medical social workers face that lead to burnout. Master's thesis. University of California, United States. [ Links ]
Long, N. 2001. Development sociology: Actor perspectives. London: Routledge. [ Links ]
Löwe, C., Mark, P., Sommer, S. & Weltermann, B. 2022. Collaboration between general practitioners and social workers: A scoping review. BMJ Open, 12: 1-10. doi:10.1136/bmjopen-2022-062144. [ Links ]
Macdonald, M., Bally, J., Ferguson, L., Murray, L., Fowler-Kerry, S. & Anonson, K. 2010. Knowledge of the professional role of others: A key inter-professional competency. Nurse Education Practice, 10(4): 238-242. [ Links ]
Masi, C. 2012. Community and health. In: Gehlert, S. & Browne, T. (eds). Handbook of health social work (pp 143-164). 2nd ed. New Jersey: John Wiley & Sons. [ Links ]
McAuliffe, C. 2009. Experiences of social workers within an interdisciplinary team in the intellectual disability sector. Critical Social Thinking: Policy and Practice, Vol. 1: 125-143. [ Links ]
McDonald, J., Jayasuriya, R. & Harris, M. F. 2012. The influence of power dynamics and trust on multidisciplinary collaboration: A qualitative case study of type 2 diabetes mellitus. BMC Health Services Research, 12,63: 1-10. https://doi.org/10.1186/1472-6963-12-63. [ Links ]
McLaughlin, J. 2015. Social work in acute hospital settings in Northern Ireland: The review of service users, carers and multidisciplinary professionals. Journal of Social Work, 16(2): 340-342. [ Links ]
National Association of Social Workers (NASW). 2021. National Association of Social Workers Code of Ethics. [Online] Available: https://www.socialworkers.org/About/Ethics/Code-of-Ethics/Code-of-Ethics-English. [Accessed: 13/02/2022]. [ Links ]
Negura, L. & Levesque, M. 2021. Understanding professional distress through social representation: Investigating the shared experience of healthcare social workers in Canada. International social work, 65(6): 1184-1200. https://doi.org/10.1177/0020872820967428 [ Links ]
Nkuna, V. 2016. Social workers ' experiences in working within the multidisciplinary team:A case study at Charlotte Maxeke Academic Hospital (CMAH). Department of Social Work, School of Human and Community Development, Faculty of Humanities, University of the Witwatersrand. [Online] Available: https://wiredspace.wits.ac.za/items/b4f7a378-6d47-48e4-9acc-19ffc66536fa. [Accessed 13/01/2021]. [ Links ]
Okpala, P. 2020. Addressing power dynamics in interprofessional healthcare team. Interprofessional Journal of Healthcare, 14(4): 1-7. [ Links ]
Perriam, C. 2015. Social work is what social workers do: A study of hospital social workers' understanding of their work and their professional identity. [Online] Available: http://ro.ecu.edu.au/theses/1674. [Accessed 20/04/2020]. [ Links ]
Petersen, L. & Pretorius, E. 2022. The social development approach to social work in health care. Social Work/Maatskaplike Werk, 58(2-2): 130 - 145. Doi: http://dx.doi.org/10.15270/58-2-1038. [ Links ]
Polit, D. F. & Beck, C. T. 2021. Nursing research: Generating and assessing evidence for nursing practice. 11th ed. Philadelphia: Wolters Kluwer. [ Links ]
Ranjit, K. 2019. Research methodology: A step-by-step guide for beginners. 5th ed. Angeles: SAGE. [ Links ]
Rashid, Y., Rashid, A., Warraich, M. A., Sana Sameen Sabir, S.S. & Waseem, A. 2019. Case study method: A step-by-step guide for business researchers. International Journal of Qualitative Methods, 18: 1-13. https://doi.org/10.1177/1609406919862424. [ Links ]
Republic of South Africa (RSA). 1994. Public Service Act, Act 103 of 1994. Government Gazette, Vol. 348, No. 15791. (1 June 1994). Pretoria: Government Printers. [ Links ]
Republic of South Africa (RSA). 1997. Department of Health. White Paper for the Transformation of the Health System in South Africa, Notice 667 of 1997. Government Gazette, Vol. 382, No. 17910. Pretoria: Government Printers. [ Links ]
Saint-Pierrea, C., Herskovica, V. & Sepúlveda, M. 2018. Review multidisciplinary collaboration in primary care: A systematic review. Family Practice, 35(2): 132-141. [ Links ]
Sheehan, D., Robertson, L. & Ormond, T. 2007. Comparison of language used and patterns of communication in interprofessional and multidisciplinary teams. Journal of Interprofessional Care, 21(1): 17 - 30. [ Links ]
Sierra, P. 2020. Attitudes of the medical profession toward the professional practice of health social workers. Cuadernos de Trabajo Social, 33(2): 327-330. [ Links ]
Steihaug, S., Jonhannessen, A., Adnanes, M., Paulsen, B. & Mannion, B. 2016. Challenges in achieving collaboration in clinical practice: The case of Norwegian health care. International Journal of Integrated Care, 16(3): 3-5. [ Links ]
Stevens, E. L., Hulme, A. & Salmon, P. M. 2021. The impact of power on health care team performance and patient safety: A review of the literature. Ergonomics, 1-19. DOI: 10.1080/00140139.2021.1906454. [ Links ]
Taberna, M., Moncayo, F. G., Jané-Salas, E., Antonio, M., Arribas, L., Vilajosana, E., Torres, P. E. & Mesía, R. 2020. The Multidisciplinary Team (MDT) approach and quality of care. Frontiers in Oncology, 10(85): 1-16. doi: 10.3389/fonc.2020.00085. [ Links ]
Tapp, H., Phillips, S., Maxman, D., Alexander, M., Brown, R. & Hall, M. 2012. Multidisciplinary team approach to improved chronic care management for diabetic patients in an urban safety net ambulatory care clinic. The Journal of the American Board of Family Medicine, 25(2): 245-246. [ Links ]
Vasudevan, S. 2015. Multidisciplinary management of chronic pain: A practical guide for clinicians. New York: Springer. [ Links ]
Whitaker, T. & Clark, E. 2006. Social workers in child welfare: Ready for duty. Research on social work practice. National Association of Social Workers, 16(4): 412-413. [ Links ]
World Health Organisation. 2010. The World Health Report. Geneva: World Health Organisation. [ Links ]
KwaZulu-Natal Health Districts. (www.kznhealth.gov.za/districts.htm) Retrieved on 12 November 2022. [ Links ]
Yin, R.K. 2018. Case study research and applications: Design and methods. Thousand Oaks: SAGE. [ Links ]
Zajac, S., Woods, A., Tannenbaum, S., Salas, E. & Holladay, C. L. 2021. Overcoming challenges to teamwork in healthcare: A team effectiveness framework and evidence-based guidance. Frontiers in. Communication, 6: 1-20. [ Links ]
Zapf, M. K. 2010. Social work and the environment: Understanding people and place. Critical Social Work, 11(3): 30-46. [ Links ]
Article received: 31/09/2022
Article accepted: 20/06/2023
Article published: 26/03/2024
AUTHOR BIOGRAPHY
Zama Maxhakana is a social work supervisor in the public health facility situated in Ilembe District. Her role includes management and supervision of social work services and facilitating training and developmental programs for 4th-level student block placements. Her study was conducted from April 2019 to July 2021 and was published on the KZN-health website: health research and knowledge management. Her field of specialisation includes the professionalisation of clinical social work within the public healthcare sector.
Mbongeni Shadrack Sithole is a senior lecturer in the Department of Social Work in the School of Applied Human Sciences at the University of KwaZulu-Natal. His research interests involve Afrocentricity, decoloniality, management and administration and inclusive education. He supervised the study, provided guidance in the conception of the article and assisted with the liaison with the Journal.

