










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.59 n.4 Stellenbosch 2023
http://dx.doi.org/10.15270/59-4-1171
ARTICLES
Locked down in the rainbow nation: alleviating the loneliness of South African older persons
Stephan GeyerI; Jill ChonodyII; Barbra TeaterIII
IUniversity of Pretoria, Department of Social Work and Criminology, Pretoria, South Africa https://orcid.org/0000-0002-3765-3051 Stephan.geyer@up.ac.za
IIBoise State University, School of Social Work, Idaho, United States of America https://orcid.org/0000-0001-6859-0826 jillchonody@boisestate.edu
IIICity University of New York, Graduate Center, College of Staten Island, New York, United States of America https://orcid.org/0000-0003-1503-0096 Barbra.Teater@csi.cuny.edu
ABSTRACT
The literature on the biopsychosocial effects of COVID-19 on older persons has originated predominately from the Global North, with a dearth of studies focusing on the loneliness of older persons in the developing world, such as South Africa. This cross-sectional study explored the loneliness of South African older persons (N = 118) before and during COVID-19 to inform gerontological social work. The survey incorporated a standardised scale of loneliness and items to assess the type and quantity of contact with others, physical health, mental health and socio-demographic variables. Bivariate and multivariate analyses explored the factors that contributed to overall loneliness, emotional loneliness and social loneliness. Results indicated a statistically significant increase in social, emotional and overall loneliness from pre- to during COVID-19. Considered from a socio-ecological resilience perspective, gerontological social work services are recommended for alleviating loneliness amongst South African older persons during a pandemic, such as COVID-19.
Keywords: COVID-19; developmental social welfare; gerontological social work; loneliness; older persons; socio-ecological resilience; South Africa
INTRODUCTION
COVID-19 (officially known as SARS-Cov-2) caused an international pandemic with a substantial impact on the biopsychosocial health of older persons (i.e. 60 years and older) across the globe. Many older persons live with medical conditions (e.g. arthritis, diabetes and hypertension) that made them susceptible to infection (Fuller & Huseth-Zosel, 2021; Sattari & Billore, 2020). The physical and social distancing (informally referred to as 'lockdown') introduced as part of the public health measures to limit the spread of the disease had a negative impact on older persons' mental health, with an increased risk for anxiety and depression as well as limitations on their social interaction and concomitant loneliness (Emerson, Kim, Mois & Beer, 2023).
In South Africa, colloquially known as the Rainbow Nation1 since democratisation, 9.2% (± 5.59 million) of the population are older persons (Statistics South Africa [StatsSA], 2022). Despite some of the strictest COVID-19 public health measures in the world (World Health Organization [WHO], 2021), and the availability of vaccines for older persons starting in June 2021, the country suffered an estimated 85,000 COVID-19-related deaths among older persons (Stent, 2021). During the time of this study, the lockdown regulations included the closure of public spaces and non-essential businesses, a ban on the sale of alcohol and cigarettes, a prohibition on gatherings (including religious meetings, marital ceremonies and funerals), restrictions on movement, a cessation of public transport, physical distancing of 1.5 meters, and compulsory wearing of face masks (Republic of South Africa [RSA] & Department of Health [DoH], 2022; WHO, 2021). These measures left numerous South African community-dwelling older persons, especially those not living with a partner or in an extended household, experiencing increased emotional and social loneliness as they could not have regular contact with children, grandchildren, and significant others (Gorenko et al., 2021; Guerra et al., 2022; Vahia, Jeste & Reynolds, 2020; WHO, 2021).
Scholars such as Ojembe et al. (2022) and Sattari and Billore (2020) highlight that, in contrast to the Global North, there was a dearth of studies focusing on the loneliness of older persons in the developing world, such as South Africa, during COVID-19. From the scoping review conducted by Ojembe et al. (2022), it would appear that earlier studies that focused on loneliness among older persons on the African continent date from the pre-COVID-19 era. Furthermore, with continuing climate change, increasing international travel and a growing world population, new variants of the COVID-19 virus, the development of new public health crises and natural disasters are inevitable (Siddiqui, Hasnain, Alam & Fatima, 2022), which often leaves older persons most vulnerable. Hence, this study aimed to investigate the loneliness of South African community-dwelling older persons before and during COVID-19 to propose gerontological social work practices appropriate for collectivist societies, in a country characterised by resource-constrained settings, during a global pandemic and/or public health crisis. Gaining greater insight into how older persons were impacted by social restrictions and how this affected their experiences of loneliness supplements the literature and informs gerontological social work services.
The remainder of the article consists of a literature review, an overview of the theoretical framework informing the study, research questions and research methods, followed by the results, discussion and implications for gerontological social work. Lastly, some limitations are identified and recommendations are offered.
LITERATURE REVIEW
Loneliness among older persons
Loneliness can be described as a negative feeling associated with a longing for greater connection (Dykstra, 2009). Loneliness is often accompanied by social isolation, which is defined as having fewer relationships than desired. However, this feeling may also be experienced regardless of the number of people within one's social network (De Jong Gierveld, 1987). Growing global concerns about loneliness have led to campaigns aimed at addressing this social issue, even though multitudes of ways of having relationships with others are widely available (Prohaska et al., 2020). Creating connections with others is interwoven in our humanness, and the need to be seen by others is strong. When these kinds of connections are missing, the effects can be deleterious. The impact on health has been likened to that of smoking, as those who experience loneliness have decreased longevity (Holt-Lunstad et al., 2015). Furthermore, the impact of loneliness includes lower cognitive functioning (Boss, Kang & Branson, 2015) and poorer mental health. A contemporary study in Germany indicates that loneliness also affects the way that people think about their longevity; that is, those who are lonely believe that they will die sooner (Hajek & König, 2021). Results of two recent metaanalyses demonstrate the relationship between loneliness and depression (Erzen & Çikrikci, 2018), as well as lower levels of overall wellbeing (Park et al., 2020). Moreover, results from a longitudinal study also indicate that decreased social size along with physical functioning predicted greater loneliness, which in turn also predicted greater depressive symptomatology (Domènech-Abella et al., 2021).
Restrictions related to COVID-19 left many people increasingly isolated socially. Research in the United States of America (USA) indicates that across all age groups, participants reported greater levels of loneliness and they employed a variety of technologies to combat it (e.g. social media, virtual meetups) (Teater, Chonody & Hannan, 2021). Social media and talking on the phone were associated with lower levels of loneliness among older participants (Teater et al., 2021). A multi-national study (i.e. Asia, Europe and the USA) that examined the impact of COVID-19 on older persons' wellbeing found that they were negatively impacted by social isolation (Sepúlveda-Loyola et al., 2020). A Dutch study found that older persons who had experienced personal losses were worried about the virus, had lost trust in social institutions and felt greater emotional loneliness (Van Tilburg et al., 2021). Another study that examined loneliness amongst older Dutch persons during COVID-19 found that having a partner was a protective factor (Van Tilburg, 2022). It would therefore appear that the availability of a social network is a key protective factor for preventing loneliness, which in turn affects health and wellbeing (Zebhauser et al., 2015). When social supports are readily available, longevity (Holt-Lunstad, Smith & Layton, 2010) and emotional regulation (Killgore, Cloonan, Taylor & Dailey, 2020; Rosenberg et al., 2021) are reinforced, whilst research has also demonstrated that without these types of support, the physical and emotional health of older persons can deteriorate (e.g. Holt-Lunstad et al., 2015; Queen, Stawinski, Ryan & Smith, 2014). From this brief overview of the literature it is apparent that several studies in the Global North focused on the experience of loneliness among older persons during COVID-19, while studies from the Global South seem non-existent.
Social welfare services for South African older persons during COVID-19
Social welfare services have the potential to alleviate loneliness among older persons. However, during the pandemic, community-based social services (e.g. luncheon clubs, income-generating projects and service centres) were suspended in South Africa (WHO, 2021). As a result of physical distancing measures, frontline social workers could often not reach out to older persons. One of the consequences was certainly an increased experience of loneliness among older persons. South African older persons do not often make use of, or cannot afford, information and communication technologies (ICTs) (Chipps & Jarvis, 2017); hence, it was also not possible to easily adopt telehealth (social) services to alleviate, among other things, the loneliness experienced by community-dwelling older persons.
The pandemic had a negative impact on the social wellbeing of older persons. Many older persons experienced financial pressure to support children and family members who had lost their income as a result of the economic ramifications of COVID-19. Others had to take care of grandchildren who could not attend (pre-)school, resulting in burnout, while reports of elder abuse, especially physical and financial abuse, increased (WHO, 2021). In addition, ageist practices were witnessed as the triage models at hospitals favoured the admission of younger patients to intensive care units for the treatment of COVID-19 (Erasmus, 2020).
From the literature the authors identified only one South African study reporting on a creative example of service delivery to address mental health risks, including the prevention of loneliness and boredom among older persons during COVID-19 (Jarvis et al., 2022). This population of older persons resided in Durban, and all were in residential care. Thus, it would appear that there is a gap in studies on social welfare services targeted at the experience of loneliness among community-dwelling older persons in South Africa during COVID-19.
According to the WHO (2021), the social welfare services offered to South African older persons included priority for vaccines, dedicated days for the 3.1 million beneficiaries to collect government older persons' grants from pay-out points, and the delivery of chronic medicine at home. The private sector also did its part. That is, supermarkets opened early to allow older persons to do shopping, and many farmers donated fresh produce to needy older persons.
Current study: Resilience theory and research questions
The current study adopted resilience theory, which is increasingly used in gerontological social research (Angevaare et al., 2020). Resilience theory is not limited to the exploration of pathogenic processes, such as the levels of loneliness endured by older persons during COVID-19. It also offers scholars an opportunity to explore salutogenic processes, such as abilities, internal and external promotive and protective factors and processes (PPFPs), and resources that enable older persons to thrive in the face of adversities (Ungar & Theron, 2020; van Breda, 2019). Resilience can be defined as:
[T]he capacity of a biopsychosocial system (this can include a person, a family, or a community) to navigate to the resources necessary to sustain positive functioning under stress as well as the capacity of systems to negotiate for resources to be provided in ways that are experienced as meaningful (Ungar, 2019:2).
Resilience is not narrowly understood to be a trait, specific outcome, or ultimate goal, but rather a process where older persons navigate toward resources and individually (or collectively) negotiate for resources that they consider meaningful during the pandemic (see Ungar, 2011). More specifically, the present study adopted a socio-ecological perspective on resilience according to which older persons are considered bio-psycho-social-spiritual beings who interact with their social and physical environment (van Breda 2019) to navigate towards better-than-expected outcomes. Considered from this perspective, resilience research explores the interactions of the micro, meso, exo, macro and chrono systems that could either be sources of adversities or risks that inhibit resilience (e.g. emotional and social loneliness), or systems that could be PPFPs (e.g. face-to-face and online/virtual contact with significant others, social interaction in groups/organisations, good physical and mental health) that enable mediating processes where older persons could achieve their desired outcomes during the pandemic (see Ungar, Ghazinour & Richter, 2013; van Breda, 2018). This perspective is reconcilable with developmental social welfare which has been the adopted welfare approach in South Africa since 1997 (Patel, 2015; van Breda, 2018).
From a socio-ecological resilience perspective, this study aimed to answer the following research questions:
• What was the level of social loneliness, emotional loneliness and overall loneliness pre-and during COVID-19?
• Was there a statistically significant difference in levels of loneliness pre- and during COVID-19?
• To what extent did different types of social contact, the number of close friends, physical health, mental health and socio-demographics contribute to overall loneliness during COVID-19?
RESEARCH METHODS
This cross-sectional study consisted of an online survey amongst community-dwelling South African older persons during lockdown Levels 2, 3 and 4 in 2021 (Babbie, 2021). With the outbreak of COVID-19, the South African government announced a state of disaster and introduced a five-level alert system, with Level 5 representing the strictest protective measure down to Level 1 being much more relaxed. Level 5 of the alert system included extensive protective measures, such as physical distancing of at least 1.5 meters, compulsory wearing of face masks, social distancing (e.g. not leaving the house for reasons other than medical treatment, shopping and work), restricted business, closure of schools and universities/colleges for contact education, a ban on social gatherings including funerals, restricted travelling both nationally and internationally, and a ban on the sales of legal drugs (e.g. alcohol and cigarettes) (RSA & DoH, 2022).
Eligible respondents were either registered volunteers of a welfare organisation or members of a service centre for older persons across five of the nine South African provinces. Furthermore, they had to be 60 years of age or older, had to have access to a smartphone or computer and an e-mail address, and had to be able to read and write in either Afrikaans or English, two of the official languages in South Africa. To ensure the respondents' privacy and confidentiality, the respondents were invited to participate in the study through an e-mail from the organisation/centre, which provided a link to the online survey in QualtricsXM. The invitation was sent to the respondents on three separate occasions to improve participation in the study (Adler & Clark, 2015). A total of 139 respondents completed the survey.
Data collection
The questionnaire consisted of items that determined the degree of loneliness, types of social contact (e.g. face-to-face; online/virtual; groups/organisations), number of close friends/relatives, subjective physical health, subjective mental health, and socio-demographics of age, gender, home language, area of residence, province, highest qualification, employment status, relationship status, living arrangements, number of children, and religious or spiritual beliefs.
Dependent variables
The dependent variable in this study was loneliness as measured on the loneliness scale (De Jong Gierveld & Kamphuis, 1985; De Jong Gierveld & van Tilburg, 1999). Apart from overall loneliness, the scale measures two sub-scales, namely social loneliness and emotional loneliness. The 11-item instrument consists of five statements on social loneliness (e.g. "I can call on my friends whenever I need them") and six statements on emotional loneliness (e.g. "I often feel rejected"). The scale asks respondents to indicate the extent to which they agree with the statements (1 = Strongly disagree to 6 = Strongly agree). After reverse scoring the five social loneliness items, the response to each item is summed to produce an overall loneliness score (between 11 and 66) with higher scores indicating higher levels of loneliness. Additionally, the six items on emotional loneliness can be summed to produce an overall emotional loneliness score (between 6 and 36), and the five items on social loneliness can be summed to produce an overall social loneliness score (between 5 and 30). If a respondent scored one or more missing values, the particular respondent was deleted from the analysis. Cronbach's alpha indicated a very good level of internal consistency for the social loneliness subscale (pre-COVID-19: α = .80; during COVID-19: α = .87), the emotional loneliness subscale (pre-COVID-19: α = .85; during COVID-19: α = .87), and the overall loneliness scale (pre-COVID-19: α = .84; during COVID-19: α = .89) in this study.
Independent variables
Three different types of social contact were explored individually by asking the following questions:
•"On average, how many days per week do you have face-to-face contact with others (family, friends)?"
• "On average, how many days per week do you have online/virtual via text message or video with others (family, friends)?"
• "On average, how often do you have contact with groups or organisations (hobby group, social club, church) per week?".
The respondents were asked to indicate the number of close friends/relatives by answering the question: "How many close friends and/or close relatives do you have (people you feel at ease with and can talk to about what is on your mind)?"
Two additional independent variables explored the extent to which physical and mental health contributed to loneliness. Physical health and mental health were explored through self-report by completing the following two questions on a six-point scale (1 = Very poor to 6 = Excellent):
•"How would you describe your physical health?"
• "How would you describe your mental health?"
Data analysis
Quantitative data analysis was implemented as described next. Descriptive statistics were employed to determine percentages, frequencies (f), and measures of central tendency for the sociodemographic variables and the items measuring social, emotional and overall loneliness, types of social contact, and physical and mental health. Bivariate analyses were run to explore the relationship between the two variables. Variables found to be significant at the bivariate level were included in the ordinary least squares (OLS) regression analyses to determine which factors contributed to overall loneliness during COVID-19. The predictor variables were physical health, mental health, face-to-face contact, online/group contact, group/organisation contact, and the number of close friends/relatives. The variables were entered simultaneously. Missing data were addressed through listwise deletion. Alpha was set at the 5% level (p < 0.05).
Ethical considerations
The respondents had to provide informed consent before accessing the online survey. The informed consent included the details of social workers who were available for counselling, should the survey result in any emotional harm to any respondent (Strydom & Roestenburg, 2021). However, no respondent required counselling. Ethical approval for this study was obtained from the Research Ethics Committee of the university where the first author is employed (Ref no.: HUM003/0321). Additionally, the management of the participating organisation and centre provided written permission for the study.
RESULTS
Sample socio-demographics
After removing cases with missing items, the total sample consisted of 118 respondents. The mean (M) age of the respondents was 72.6 (Standard deviation (SD) = 7.1) (range 60 to 90), with 72% identifying as female. The majority of respondents (92.3%) indicated their home language as Afrikaans, followed by English (6.8%), and Setswana (0.9%). Over 85% resided in urban or semi-urban areas, followed by 14.7% in rural areas. Nearly 70% of respondents held a qualification of B Degree/Honours Degree/Professional Degree, National Diploma, or Grade 12/Matric. The majority (79.5%) were retired/pensioners. The largest percentage of respondents were married/partnered (45.3%) and were living with a spouse/partner (46.6%), followed by 40.5% of respondents who were living alone. The mean number of children for the respondents was 2.8 (SD = 1.4) (Range 0 to 11). Nearly 98% of the respondents reported Christianity as their religion or spiritual belief. Table 1 reports the socio-demographics of the sample.

Health and social contacts during COVID-19
The study explored older persons' self-reported physical and mental health on a six-point scale. Physical health (M = 4.4; SD = .92) and mental health (M = 4.7; SD = .92) were reported to be between "good" and "very good" at the time of completing the survey. Social contacts were explored by focusing on older persons' face-to-face contact, online/virtual contact and contact via groups/organisations. The respondents had, on average, 5.3 days (SD = 1.9) of face-to-face contact a week, 5.9 days (SD = 1.5) of online/virtual contact a week, and 2.5 days (SD = 1.9) of contact via groups/organisations a week. Asking about close friends/relatives, the respondents reported a mean of 7.1 close friends or relatives (SD = 7.3).
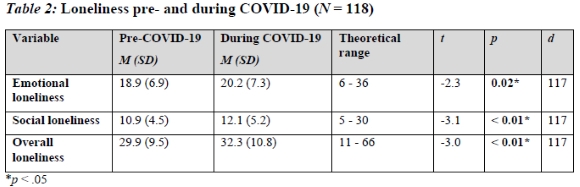
Social, emotional and overall loneliness pre- and during COVID-19
Table 2 reports the descriptive statistics of the social, emotional and overall loneliness constructs both pre- and during COVID-19. Social, emotional and overall loneliness increased from pre- to during COVID-19 among the sample. Paired-sample i-tests indicated the observed decreases pre- to during COVID-19 were statistically significant at p = .02 - p < .01. The effect sizes (d) for these changes in loneliness were small (d = .2 - .3), according to Cohen's (1988) guidelines.
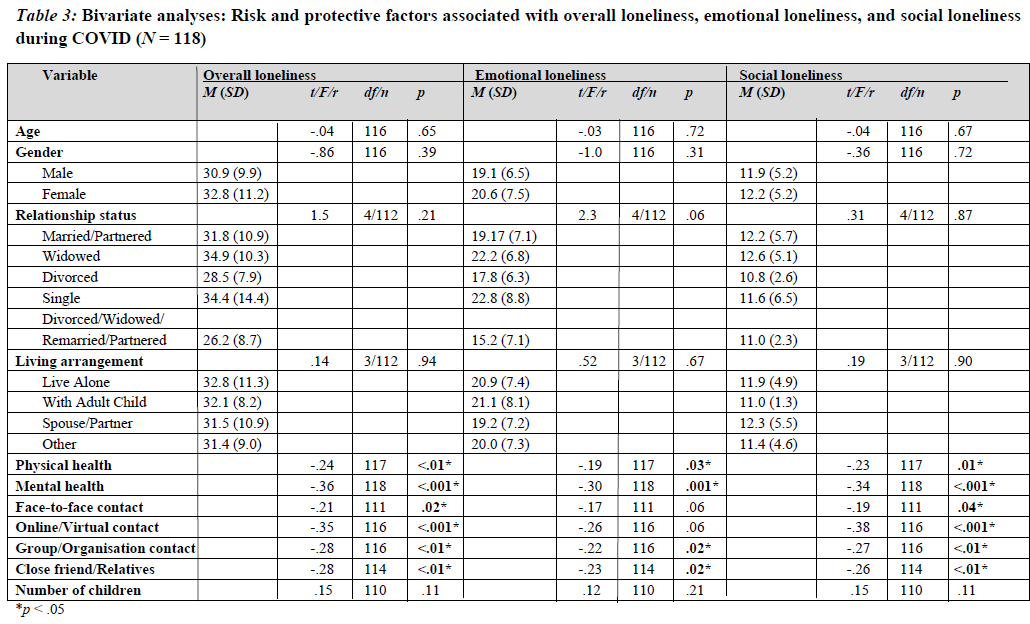
Relationship between socio-demographics, risk and protective factors, and loneliness
Table 3 reports the bivariate analyses between socio-demographics, physical and mental health, different types of social contact, the number of close friends/relatives and children, and overall loneliness, emotional loneliness and social loneliness. The analyses revealed statistically significant negative relationships only between physical health, mental health, face-to-face contact, online/virtual contact, group/organisational contact, and the number of close friends/relatives with at least one or more of the three loneliness constructs. In particular, greater overall loneliness was significantly associated with poorer physical health, poorer mental health, less face-to-face contact, less online/virtual contact, less contact with groups/organisations, and fewer close friends/relatives.
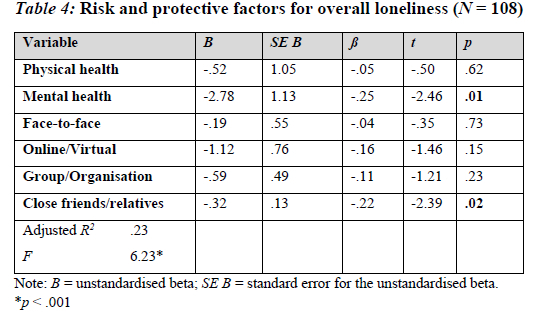
Risk and protective factors contributing to loneliness
The results of the regression analysis for overall loneliness indicated that two variables explained 52% of the variance. As Table 4 depicts, a higher subjective rating of mental health and more close friends/relatives were associated with lower levels of overall loneliness. Collinearity diagnostic tests indicated no problems with multicollinearity in this model (Field, 2013).
DISCUSSION
This study sought to explore the experiences of loneliness pre- and during-COVID-19 among community-dwelling older persons in South Africa. With reference to the first and second research questions that examined the level of social loneliness, emotional loneliness and overall loneliness pre- and during COVID-19, the results indicated that all three variables of loneliness increased from pre- to during COVID-19 among the sample and the noticeable increases were statistically significant. Interestingly, the effect size for change was small. Previous studies in the USA (e.g. Luchetti et al., 2020; Teater et al., 2021) found that younger people experienced greater loneliness both before and during the pandemic. It could be that older persons are already getting their needs met in ways that younger people have yet to develop, or they are coping in different ways. Studies in the Global North have found that older persons had better coping methods than younger persons and experienced lower stress levels (Chonody, Teater, Hannan & Hall, 2022; Pearman, Hughes, Smith & Neupert, 2021). While the current study did not examine loneliness across the life spectrum, the sample was largely married/partnered and reported on average seven close friends with whom they could confide. Quality of contact with others during COVID-19 is negatively associated with loneliness in that loneliness decreases as quality increases (Teater et al., 2021). The study results suggest, at least in part, that these characteristics do serve as PPFPs for loneliness during the social restrictions experienced during the pandemic.
The third research question aimed to examine the extent to which different types of social contact, number of close friends, physical health, mental health and socio-demographics contributed to overall loneliness during COVID-19. Bivariate and multivariate analyses found protective factors and socio-demographic characteristics that buffered older persons against overall loneliness during COVID-19 as follows: better perceived physical and mental health, more face-to-face and/or online/virtual contact, increased contact with groups/organisations and an increased number of close friends/relatives. While the number of close friends was consistently found to be important across all three types of loneliness, only the number of close friends and mental health status were significant in the regression results for overall loneliness. This suggests that having better quality or more close relationships may be more important than marital status or living arrangements, both of which were not significant in the analysis. In a study of older persons from the United Kingdom (UK), USA, and Australia in a long-term relationship, respondents (n = 1565) indicated more often the emotional support components of their relationship were what made them feel appreciated. Moreover, in the regression analysis, relationship happiness was the strongest factor in explaining the maintenance of the relationship (Chonody & Gabb, 2019). This study, amongst many others in this substantive literature, points to the role of closeness versus partnership per se in explaining the benefits of coupledom. It is likely that the respondents who had this type of closeness in their relationship included their partners in the total number of people with whom they feel close. Future research should seek to parse this intricate web of interrelationships between partnerships as a protective factor for loneliness and what characteristics are essential, particularly during times of heightened stress.
Relatedly, good self-reported mental health contributed to less loneliness among respondents. Perhaps those who experienced less loneliness had less experience with mental health concerns and were thus able to cope better during the pandemic with feelings of loneliness. From a resilience perspective, it thus confirms that good mental health serves as a PPFP to enable older persons to navigate toward better-than-expected outcomes during the pandemic (van Breda, 2018). Again, the interrelationship between mental health and loneliness is complex, and future research should seek to investigate causality as this study was correlational.
IMPLICATIONS FOR GERONTOLOGICAL SOCIAL WORK
Since democratisation in 1994, South Africa has had a new political dispensation and a liberal Constitution. Yet older persons endure numerous social welfare challenges, such as elder abuse and violence, food insecurity, inadequate finances, lack of basic health services, and poverty (Noyoo, 2017; Patel, 2015). The COVID-19 pandemic created additional challenges, such as loneliness. The unique context of the country, with many rural areas which are resource-constrained, requires context-specific gerontological social work services. In particular, innovative ways to reach older people in rural places is of the utmost concern, given that reliance on the internet is not always feasible in these areas. Thus, social workers will need to think about case and group work, where services are brought to the community in safe and reliable ways.
In addition, aligning services with the country's adopted developmental social welfare model is a key issue. Services are to be informed by principles of accessibility, the right to self-determination, equality, non-discrimination and the promotion of human rights. Social workers should bridge the micro-macro divide in the implementation of methods. That is, group and community work are the primary focus for social workers, although casework does remain permissible (Patel, 2015). Gerontological social work services underpinned by a developmental social welfare model and operationalised through a socio-ecological resilience perspective in a developing country require creativity and ingenuity. For example, creating groups that address loneliness would be one way to achieve both the goal of community work and address a problem that occurs at the micro-level.
In times of crisis, people on the African continent 'flock' to support one another (Ebersöhn, 2019). Of course, the COVID-19 precautions hindered such flocking. Therefore, social workers, while rendering casework in an attempt to establish a sense of connectedness, should make use of telephone calls or physically distanced doorway visits to counter the social loneliness of older persons (Conroy, Krishnan, Mittelstaedt & Patel, 2020; Gorenko et al., 2021). While practising social distancing and adhering to public health protocols, psychoeducational group work services could be rendered. Through community work (e.g. community education), printed material could be developed and distributed to attend to older persons' emotional loneliness and alleviate their stress or anxiety by educating them about the pandemic itself (Chonody et al., 2022; Conroy et al., 2020; Gorenko et al., 2021). Furthermore, therapy/support groups could be offered to attend to the bereavement of older persons who lost loved ones. These recommendations are specifically feasible in resource-constrained settings and in situations where older persons do not have access to or make use of ICTs and so direct service delivery is required. As research in the Netherlands has shown, older persons who had experienced personal losses were worried about the virus and lost their trust in social institutions, had greater emotional loneliness (van Tilburg et al., 2021).
Moreover, supporting relationships and their maintenance is essential for social workers who work with older persons. One way to approach this is through casework by reinforcing those elements of the relationship that are working (i.e. promotive factors) and enabling older persons to reach their desired outcomes (Chonody & Gabb, 2019; Ungar et al., 2013). Creating greater relationship satisfaction is an important PPFP for supporting behaviours that help to maintain desired relationships (Ogolsky & Bowers, 2013; Ungar et al., 2013). This in turn will support the protective mechanism of relationships for health and wellbeing, including loneliness.
The non-significant findings regarding face-to-face and virtual meetings as well as contact with groups/organisations highlight how the emotional support of a relationship perhaps supersedes the need to be together. The socioemotional selectivity theory, which suggests that older persons seek out others in this life stage who are most able to meet their emotional needs (Carstensen, Fung & Charles, 2003), could serve as a possible explanation for the finding. That is, when we are younger we look for novelty and information, but as we age, we find what we want is emotional support from other people.
More affluent older persons can afford ICTs and they often have the necessary technological literacy to make use of online services. Therefore, the use of ICTs should not be underestimated to address the loneliness of older persons during a pandemic and enable them to achieve better-than-expected outcomes. The social wellbeing of older persons could be maintained or improved through, amongst other things, the use of social media, telehealth, mHealth programmes, and visual chat/video calls (Garfin, 2020; Jarvis, Sartorius & Chipps, 2020). In the South African context, Chipps and Jarvis (2017) with reference to nursing, developed a technology-assisted (cell phone) communication to address acute mental health challenges among older persons. In psychology, Roos and van Greunen (2022) report on the development of the Yabelana application on cell phones that offers a central point where context-specific information about health care and social service providers is accessible. Social workers should equally explore the potential use of ICTs in addressing the social welfare needs, such as addressing loneliness, of South African older persons during a pandemic. A first step may be to address the negative attitudes and anxieties of older persons when it comes to technology (Jarvis et al., 2020) through community education programmes. After that, telehealth and video call services could be introduced (Gorenko et al., 2021). During times of physical distancing, phones could be used to assess the risks of exposure/factors in older persons' lives as well as the protective factors that could be activated to mediate a process towards achieving better-than-expected outcomes during the pandemic. Although gerontological social work service cannot eliminate a pandemic, it has the potential to reduce older persons' exposure to the virus by addressing their social behaviour and improving their experience of and ways of coping with loneliness (cf. Ungar, 2019).
LIMITATIONS AND RECOMMENDATIONS
The results of this study should be considered in the light of its limitations. First, given the online nature of the survey, older people who did not have access to the internet were essentially excluded. However, surveying older persons in person during the pandemic would not have been a feasible method given that they are more vulnerable to serious illness or death from COVID-19 (Sattari & Billore, 2020). Second, the sample was mostly comprised of women who were nearly all Christian and held a degree. Understanding differences in loneliness related to these socio-demographic factors is important for programme development, and future research should find ways to sample other groups and have the survey readily available in all the official languages of the country. Third, the independent variable related to children likely did not capture what was intended. That is, this item should have inquired about closeness to children rather than the number of children one has in ascertaining loneliness. This may have been captured, at least in part, by another independent variable, which asks respondents to indicate the number of close relationships that they have with friends or relatives. Additional knowledge about the closeness of familial relationships may be important when considering programme and policy development as mediating processes to enable older persons to reach their desired outcomes. This study focused on community-dwelling older persons. Future research should focus on South African older persons in residential care. Their experience of loneliness and the gerontological social work service they may require are context-specific and unique, and may differ from those living in a community.
REFERENCES
Adler, E. S. & Clark, R. 2015. An invitation to social research: How it's done. 5th ed. Stamford, CT: Cengage Learning. [ Links ]
Angevaare, M. J., Roberts, J., van Hout, H. P. J., Joling, K. J., Smalbrugge, M., Schoonmade, L. J., Windle, G. & Hertogh, C. M. P. M. 2020. Resilience in older persons: A systematic review of the conceptual literature. Ageing Research Reviews, 63: 101144. [ Links ]
Babbie, E. 2021. The practice of social research. 15th ed. Boston, MA: Cengage Learning. [ Links ]
Boss, L., Kang, D. H. & Branson, S. 2015. Loneliness and cognitive function in the older adult: A systematic review. InternationalPsychogeriatrics, 27(4): 541-553. https://doi.org/10.1017/S1041610214002749. [ Links ]
Carstensen, L. L., Fung, H. H. & Charles, S. T. 2003. Socioemotional selectivity theory and the regulation of emotion in the second half of life. Motivation and Emotion, 27(2): 103-123. [ Links ]
Chipps, J. & Jarvis, M. A. 2017. Technology-assisted communication in older persons in a residential care facility in South Africa. Information Development, 33(4): 393-405. https://doi.org/10.1177/0266666916664388. [ Links ]
Chonody, J. & Gabb, J. 2019. Understanding the role of relationship maintenance in enduring couple partnerships in later adulthood. Marriage & Family Review, 55(3): 216-238. https://doi.org/10.1080/01494929.2018.1458010. [ Links ]
Chonody, J., Teater, B., Hannan, K. & Hall, K. 2022. Stress during the early months of COVID-19 in the U.S.: The role of fear and health status across the age spectrum. Advances in Social Work, 22(3): 1046-1065. https://doi.org/10.18060/25790. [ Links ]
Cohen, J. 1988. Statistical power analysis for the behavioral sciences. 2nd ed. New York, NY: Lawrence Erlbaum Associates, Publishers. [ Links ]
Conroy, K. M., Krishnan, S., Mittelstaedt, S. & Patel, S. S. 2020. Technological advancements to address elderly loneliness: Practical considerations and community resilience implications for COVID-19 pandemic. Working with Older People, 24(4): 257- 264. https://doi.org/10.1108/WWOP-07-2020-0036. [ Links ]
De Jong Gierveld, J. 1987. Developing and testing a model of loneliness. Journal of Personality and Social Psychology, 53(1): 119-128. https://doi.org/10.1037/0022-3514.53.1.119. [ Links ]
De Jong Gierveld, J. & Kamphuis, F. 1985. The development of a Rasch-Type loneliness scale. Applied Psychological Measurement, 9:289-299. https://doi.org/10.1177/014662168500900307. [ Links ]
De Jong Gierveld, J. & van Tilburg, T. 1999. Manual of the loneliness scale. Amsterdam: Vrije Universiteit. [ Links ]
Domènech-Abella, J., Mundo, J., Switsers, L., van Tilburg, T., Fernández, D. & Aznar-Lou, I. 2021. Social network size, loneliness, physical functioning and depressive symptoms among older adults: Examining reciprocal associations in four waves of the Longitudinal Aging Study Amsterdam (LASA). International journal of geriatric psychiatry, 36(10): 1541-1549. https://doi.org/10.1002/gps.5560. [ Links ]
Dykstra, P. A. 2009. Older adult loneliness: Myths and realities. European Journal of Ageing, 6(2): 91-100. https://doi.org/10.1007/s10433-009-0110-3. [ Links ]
Ebersöhn, L. 2019. Flocking together: An indigenous psychology theory of resilience in South Africa. Cham, Switzerland: Springer Nature. [ Links ]
Emerson, K. G., Kim, D., Mois, G. & Beer, J. M. 2023. "At first it wasn't so bad": How adults aged 60 and older feel about social distancing during COVID-19. Journal of Gerontological Social Work, 66(3): 339-353. https://doi.org/10.1080/01634372.2022.2111741. [ Links ]
Erasmus, N. 2020. Age discrimination in critical care triage in South Africa: The law and the allocation of scarce health resources in the COVID-19 pandemic. South African Medical Journal, 110(12): 1172-1175. http://dx.doi.org/10.7196/samj.2020.v110i12.15344. [ Links ]
Erzen, E. & Çikrikci, Ö. 2018. The effect of loneliness on depression: A meta analysis. International Journal of Social Psychiatry, 64(5): 427-435. https://doi.org/10.1177/0020764018776349. [ Links ]
Field, A. 2013. Discovering statistics using SPSS. 4th ed. London, UK: Sage. [ Links ]
Fuller, H. R. & Huseth-Zosel, A. 2021. Lessons in resilience: Initial coping among older adults during the COVID-19 pandemic. The Gerontologist, 61(1): 114-125. https://doi.org/10.1093/geront/gnaa170. [ Links ]
Garfin, D. R. 2020. Technology as a coping tool during the coronavirus disease 2019 (COVID-19) pandemic: Implications and recommendations. Stress and Health, 36(4): 555-559. https://doi-org.uplib.idm.oclc.org/10.1002/smi.2975. [ Links ]
Gorenko, J. A., Moran, C., Flynn, M., Dobson, K. & Konnert, C. 2021. Social isolation and psychological distress among older adults related to COVID-19: A narrative review of remotely-delivered interventions and recommendations. Journal of Applied Gerontology, 40(1): 3-13. https://doi.org/10.1177/0733464820958550. [ Links ]
Guerra, S., Sousa, L., Carvalho, R., Melo, S. & Ribeiro, O. 2022. Understanding loneliness in older adults: Reports from experts by experience to reach digital solutions. Journal of Gerontological Social Work, 65(7): 728-734. https://doi.org/10.1080/01634372.2021.2019866. [ Links ]
Hajek, A. & König, H. H. 2021. Do lonely and socially isolated individuals think they die earlier? The link between loneliness, social isolation and expectations of longevity based on a nationally representative sample. Psychogeriatrics, 21(4): 571-576. https://doi.org/10.1111/psyg.12707. [ Links ]
Holt-Lunstad, J., Smith, T. B., Baker, M., Harris, T. & Stephenson, D. 2015. Loneliness and social isolation as risk factors for mortality: A meta-analytic review. Perspectives on Psychological Science, 10(2): 227-237. https://doi.org/10.1177/1745691614568352. [ Links ]
Holt-Lunstad, J., Smith, T. B. & Layton, J. B. 2010. Social relationships and mortality risk: A meta-analytic review. PLoS medicine, 7(7): e1000316. [ Links ]
Jarvis, M. A., Pillay, S. R., Norton, L. M., Hiraman, N. & Baloyi, O. B. 2022. Delivering a psychosocial program for older people living in retirement homes during the Covid-19 pandemic: A process evaluation and recommendations for community interventions. Journal of Community Psychology, 51(1): 31-50. [ Links ]
Jarvis, M., Sartorius, B. & Chipps, J. 2020. Technology acceptance of older persons living in residential care. Information Development, 36(3): 339-353. https://doi.org/10.1177/0266666919854164. [ Links ]
Killgore, W. D., Cloonan, S. A., Taylor, E. C. & Dailey, N. S. 2020. Loneliness: A signature mental health concern in the era of COVID-19. Psychiatry Research, 290: 113-117. https://doi.org/10.1016/j.psychres.2020.113117. [ Links ]
Luchetti, M., Lee, J. H., Aschwanden, D., Sesker, A., Strickhouser, J. E., Terracciano, A. & Sutin, A. R. 2020. The trajectory of loneliness in response to COVID-19. The American psychologist, 75(7): 897-908. https://doi.org/10.1037/amp0000690. [ Links ]
Noyoo, N. 2017. Reflecting on the human rights of older persons in South Africa. Journal of Human Rights and Social Work, 2: 108-116. https://doi.org/10.1007/s41134-017-0039-y. [ Links ]
Ogolsky, B. G. & Bowers, J. R. 2013. A meta-analytic review of relationship maintenance and its correlates. Journal of Social and Personal Relationships, 30(3): 343-367. [ Links ]
Park, C., Majeed, A., Gill, H., Tamura, J., Ho, R. C., Mansur, R. B., Nasri, F., Lee, Y., Rosenblant, J. D., Wong, E. & McIntyre, R. S. 2020. The effect of loneliness on distinct health outcomes: A comprehensive review and meta-analysis. Psychiatry Research, 294: 113514. https://doi.org/10.1016/j.psychres.2020.113514. [ Links ]
Patel, L. 2015. Social welfare and social development. 2nd ed. Cape Town: Oxford University Press Southern Africa. [ Links ]
Pearman, A., Hughes, M. L., Smith, E. L. & Neupert, S. D. 2021. Age differences in risk and resilience factors in COVID-19 related stress. Journals of Gerontology: Series B, 76(2): e38-e44. https://doi.org/10.1093/geronb/gbaa120. [ Links ]
Prohaska, T., Burholt, V., Burns, A., Golden, J., Hawkley, L., Lawlor, B., Lubben, J., O'Sullivan, R., Perissinotto, C., van Tilburg, T., Tully, M., Victor, C. & Fried, L. 2020. Consensus statement: Loneliness in older adults, the 21st-century social determinant of health? BMJ Open, 10(8): e034967. http://dx.doi.org/10.1136/bmjopen-2019-034967. [ Links ]
Ojembe, B. U., Kalu, M. E., Donatus Ezulike, C., Iwuagwu, A. O., Ekoh, P. C., Oyinlola, O., Osifeso, T., Makunjuola, J. O. & Kapiriri, L. 2022. Understanding social and emotional loneliness among black older adults: A scoping review. Journal of Applied Gerontology, 41(12): 2594-2608. https://doi.org/10.1177/07334648221118357. [ Links ]
Queen, T. L., Stawski, R. S., Ryan, L. H. & Smith, J. 2014. Loneliness in a day: Activity engagement, time alone, and experienced emotions. Psychology and Aging, 29(2): 297. [ Links ]
Republic of South Africa (RSA) & Department of Health (DOH). 2022. COVID-19 online resource and news portal. [Online] Available: https://sacoronavirus.co.za/ [Accessed: 18/01/2023]. [ Links ]
Roos, V. & van Greunen, D. 2022. Yabelana: Designing and introducing an age-inclusive and context-specific information and communication ecosystem. In: Roos, V. & Hoffman, J. (eds.). Age-inclusive ICT innovation for service delivery in South Africa: A developing country perspective. Cham, Switzerland: Springer Nature. https://doi.org/10.1007/978-3-030-94606-7. [ Links ]
Rosenberg, M., Luetke, M., Hensel, D., Kianersi, S. & Herbenick, D. 2021. Depression and loneliness during April 2020 COVID-19 restrictions in the United States, and their associations with frequency of social and sexual connections. Social Psychiatry and Psychiatric Epidemiology, 56(2021): 1221-1232. https://doi.org/10.1007/s00127-020-02002-8. [ Links ]
Sattari, S. & Billore, S. 2020. Bring it on Covid-19: Being an older person in developing countries during a pandemic. Working with Older People, 24(4): 281-291. https://doi.org/10.1108/WWOP-06-2020-0030. [ Links ]
Sepúlveda-Loyola, W. A., Rodriguez-Sanchez, I., Pérez-Rodríguez, C., Ganz, F., Torralba, R., Oliveira, D. & Rodríguez-Mañas, L. 2020. Impact of social isolation due to COVID-19 on health in older people: Mental and physical effects and recommendations. Journal of Nutrition, Health & Aging, 24(2020): 938-947. https://doi.org/10.1007/s12603-020-1500-7. [ Links ]
Siddiqui, A. H., Hasnain, M. D., Alam, M. M. & Fatima, S. 2022. Climate change: Causes, impacts and solutions. International Research Journal of Engineering and Technology, 9(11): 928-934. [ Links ]
Statistics South Africa (StatsSA). 2022. P0302 - Mid-year population estimates, 2022. [Online] Available: https://www.statssa.gov.za/?p=15601 [Accessed: 18/01/2023]. [ Links ]
Stent, J. 2021. Nearly 85,000 older South Africans have probably died from Covid-19. [Online] Available: https://www.groundup.org.za/article/nearly-85000-older-south-africans-have-probably-died-covid-19/ [Accessed: 18/01/2023]. [ Links ]
Strydom, H. & Roestenburg, W. J. H. 2021. Ethical conduct in research with human participants. In: Fouché, C. B., Strydom, H. & Roestenburg, W. J. H. (eds.). Research at grass roots: For the social sciences and human service professions. 5th ed. Pretoria: Van Schaik. [ Links ]
Teater, B., Chonody, J. & Hannan, K. 2021. Meeting social needs and loneliness in a time of social distancing under COVID-19: A comparison of young, middle, and older adults. Journal of Human Behavior in the Social Environment, 31(1-4): 43-59. https://doi.org/10.1080/10911359.2020.1835777. [ Links ]
Ungar, M. 2011. The social ecology of resilience: Addressing contextual and cultural ambiguity of a nascent construct. American Journal of Orthopsychiatry, 81(1): 1-17. https://doi.org/10.1111/j.1939-0025.2010.01067.x. [ Links ]
Ungar, M. 2019. Designing resilience research: Using multiple methods to investigate risk exposure, promotive and protective processes, and contextually relevant outcomes for children and youth. Child Abuse & Neglect, 96: 1-8. https://doi.org/10.1016/j.chiabu.2019.104098. [ Links ]
Ungar, M., Ghazinour, M. & Richter, J. 2013. Annual research review: What is resilience within the social ecology of human development? Journal of Child Psychology and Psychiatry, 54(4): 348-366. https://doi.org/10.1111/jcpp.12025. [ Links ]
Ungar, M. & Theron, L. 2020. Resilience and mental health: How multisystemic processes contribute to positive outcomes. The Lancet Psychiatry, 7(5): 441-448. https://doi.org/10.1016/S2215-0366(19)30434-1. [ Links ]
Vahia, I. V., Jeste, D. V. & Reynolds, C. F. 2020. Older adults and the mental health effects of COVID-19. JAMA, 324(22): 2253-2254. https://doi.org/10.1001/jama.2020.21753. [ Links ]
Van Breda, A. D. 2018. A critical review of resilience theory and its relevance for social work. Social Work/Maatskaplike Werk, 54(1): 1-18. http://dx.doi.org/10.15270/54-1-611. [ Links ]
Van Breda, A. D. 2019. Resilience. In: van Breda, A. D. & Sekudu, J. (eds.). Theories for decolonial social work practice in South Africa. Cape Town: Oxford University Press Southern Africa. [ Links ]
Van Tilburg, T. G. 2022. Emotional, social, and existential loneliness before and during the COVID-19 pandemic: Prevalence and risk factors among Dutch older adults. The Journals of Gerontology: Series B, 77(7): e179-e184. https://doi.org/10.1093/geronb/gbab101. [ Links ]
Van Tilburg, T. G., Steinmetz, S., Stolte, E., van der Roest, H. & de Vries, D. H. 2021. Loneliness and mental health during the COVID-19 pandemic: A study among Dutch older adults. The Journals of Gerontology: Series B, 76(7): e249-e255. https://doi.org/10.1093/geronb/gbaa111. [ Links ]
World Health Organization (WHO). 2021. Assessing the impact of Covid-19 on older people in the African region: A study conducted for the World Health Organization African regional office. Brazzaville: WHO Regional Office for Africa. [ Links ]
Zebhauser, A., Baumert, J., Emeny, R. T., Ronel, J., Peters, A. & Ladwig, K. H. 2015. What prevents old people living alone from feeling lonely? Findings from the KORA-Age-study. Aging & Mental Health, 19(9): 773-780. https://doi.org/10.1080/13607863.2014.977769. [ Links ]
Article received: 19/1/2023
Article accepted: 6/6/2023
1 The 'Rainbow Nation' is an informal way of referring to South Africa since its democratisation in 1994. It alludes to a population with diverse cultures, languages and religions coming together as one nation within the boundaries of South Africa.


{kind=link}