










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.59 n.2 Stellenbosch 2023
http://dx.doi.org/10.15270/59-2-1048
ARTICLES
A needs assessment for social work interventions for children affected by HIV and AIDS
Nomvuyo Lukelelo
Department of Social Work, University of the Western Cape, South Africa https://orcid.org/0000-0001-5216-5681 nlukelelo@uwc.ac.za
ABSTRACT
Children are often left orphaned and without adult supervision when the parent or caregiver dies from HIV and AIDS-related illnesses. There is very little information available in South Africa on the type of interventions to reinforce the care and support provided to children affected by HIV and AIDS (CABHA). This study aimed to explore existing interventions provided to CABHA and the experiences of social workers in implementing interventions. Findings indicate that interventions are a continuous and collaborative process between social workers and stakeholders. A proper needs assessment should be done before implementing interventions to ensure that they benefit the children identified as needing intervention. Community-based interventions should not be underestimated as a significant source of support for CABHA.
Keywords: children affected by HIV and AIDS; HIV and AIDS; intervention; needs assessment; orphaned and vulnerable children; social work
INTRODUCTION
Children affected by HIV and AIDS (CABHA) are described as those "living with HIV, as well as those whose well-being or development is threatened by HIV because they live in HIV-affected households and communities" (UNICEF, 2011). These children are often vulnerable as they become caregivers to HIV-positive parents who are too ill to care for them. Furthermore, they sometimes end up orphaned when the parent dies of AIDS-related illness. UNICEF (2022) estimates that a total of 14.9 million children worldwide have lost one or both parents due to AIDS-related causes. The absence of a caregiver may thus leave the children at risk of exploitation and neglect, and in need of care. This adds pressure on most government resources, already stretched because of the increasing number of HIV-infected persons and the demand for HIV treatment. The global community and individual countries have made progress towards addressing the needs of HIV-affected children and families. Still, support has most often been delivered through targeted programmes, which do not fully meet the needs of CABHA (Kidman & Heymann, 2016). UNICEF (2016) advocates for global solidarity in the AIDS response that must include the most vulnerable children and women, if AIDS is ever to become an issue of the past.
Statistics South Africa (2020) reports that the total number of persons living with HIV in South Africa increased from an estimated 3,8 million in 2002 to 7,8 million by 2020. Statistics South Africa (2020) reports a decline from 12,9 deaths per 1 000 people in 2002 to 8,7 deaths per 1 000 people in 2020 (Statistics South Africa, 2020). This decline is attributed to the increased access to anti-retroviral treatment, which means that people infected with HIV live longer. Li et al., (2014:2052) state that:
as improved treatment strategies continue to prolong the lives of parents living with HIV, more children will have to adopt caretaking roles and learn to cope with shifts in family structure, financial deprivation and stigma.
This highlights a serious development of the problem of orphaned and vulnerable children (OVC) and child-headed homes. These children are more likely to experience negative outcomes as a result of their inability to access essential resources such as education, healthcare, child protection and social services. To deal with the increasing burden of child-headed homes, there is a need for a united global response to the AIDS epidemic and interventions that include children orphaned and made vulnerable by AIDS.
Visser, Zungu and Ndala-Magoroa (2015) argue that during the past decade various interventions have attempted to address the diverse needs of OVC. Several interventions have been implemented across some African countries (Bhana et al., 2014 ; Goodman, Kaberia, Morgan & Keiser, 2014; Han, Ssewamala & Wang, 2013; Karimli et al., 2019) to support children who are vulnerable as a result of various social circumstances, including those affected by HIV. Although CABHA were included as part of these interventions, it is unclear how these interventions cater to their specific needs as these interventions often focus on general issues affecting OVC. The structure of the interventions often depends on the needs and resources available in the community where they are being implemented. Still, very little information is reported on the social worker's role.
Furthermore, section 54 of the Children's Act 38 of 2005 (RSA, 2006) identifies children needing care as requiring social work intervention but refers to children in general and not specifically to CABHA. The literature on social workers' role in interventions for CABHA is very scant. There is extensive literature on the challenges faced by children affected by HIV, but disproportionately less is known about effective interventions to support children and families (Richter, Louw & Naicker, 2015). Previous research (Mann, Long, Delap & Connell, 2012) recommended the need for better information on the kinds of support and interventions in place to strengthen the emotional, physical, economic and social care that families and communities provide to children living with and affected by HIV. The focus of this study was thus to explore the current interventions provided to CABHA by various organisations and the experiences of social workers in implementing interventions.
METHODOLOGY
The study used a qualitative research approach with an exploratory research design, and the data were collected in two stages using semi-structured interviews. Qualitative research is a research methodology where researchers are interested in knowing how people understand and experience their world at a particular time and in a particular context (Merriam & Grenier, 2019). Qualitative research was applied to this study as this methodology allows the researcher to explore the problem being researched and to give detailed explanations based on the responses gathered from participants. In qualitative studies, researchers "enter the setting with open minds, prepared to immerse themselves in the complexity of the situation and interact with the participants" (Fouché, 2021:40). The interviews used to collect data provided the researcher with the opportunity to engage with the participants and gain in-depth information. An exploratory research design was deemed appropriate for the study since this type of research design, according to Fouché (2021), is normally used when there is a lack of basic information or the researcher has only a few studies for reference.
Participants
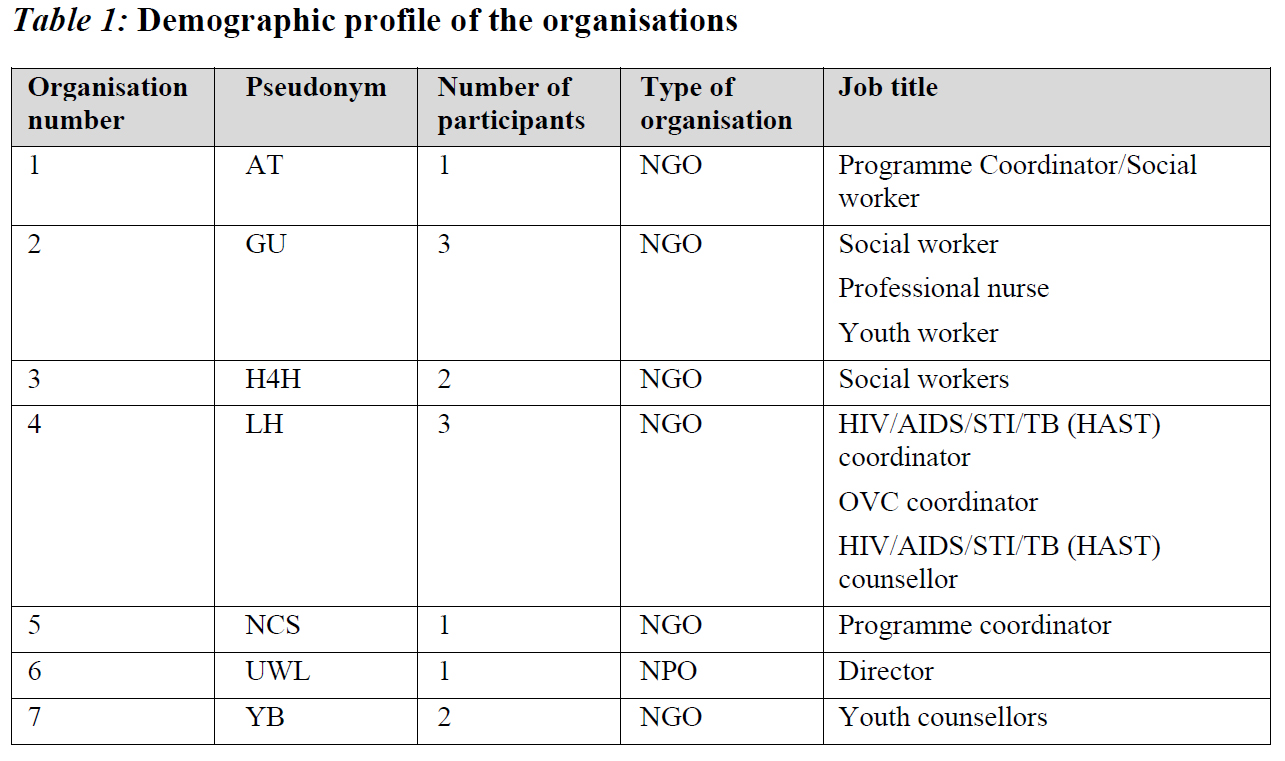
Stage one of the selection process was done through purposive sampling, as the researcher had to select organisations that met the specific criteria for inclusion. Purposive sampling comprises elements that contain the most typical attributes of the population being studied (Strydom, 2021). The organisations that were chosen had to meet the following selection criteria: work with general OVC and those made vulnerable by AIDS; provide psychosocial support programmes aimed at CABHA; have designated persons who can explain the programmes of the organisation. Seven organisations were identified within the Cape Town Metropolitan area, and 13 participants were interviewed from these organisations. The demographic details of the organisation are summarised in Table 1.
Most of the organisations were non-governmental organisations (NGOs), and one was a non-profit organisation. The participants who represented the organisations were people responsible for either managing, coordinating or facilitating interventions for OVC or CABHA in their organisations and had different job titles depending on the structure of each organisation. Some organisations had one person responsible for the overall management of the organisation and its programmes, while others had teams responsible for managing the different programmes offered. For example, organisations 1, 5 and 6 each had only one person representing their organisation. Two of these people occupied the roles of the programme coordinator, and the other participant occupied the role of director. Teams of people represented the remaining organisations; some came in pairs (social workers and youth counsellors), while others came in groups of three consisting of professional staff. Out of the total number of 13 participants, there were at least four social workers and one of those social workers occupied a dual role of coordinator and social worker.
The participants of stage two of data collection were exclusively social workers who were identified through a snowball sampling method. Snowball sampling occurs when the researcher recruits the participants by referral from other participants who are already participating in the study. According to Strydom (2021), in snowball sampling the participant is requested to refer others with similar experiences to gain information on similar persons who could make up the sample. Participants in organisations that participated in stage 1 were approached and asked to refer the researchers to social workers with whom they usually work and who provide interventions to CABHA. Once the social workers had completed their interviews, they were requested to provide a recommendation of other social workers whom they deemed met the study's criteria. The inclusion criteria for the study were social workers who were:
- Registered with the South African Council of Social Service Professions;
- Working with children under the age of 18;
- Working/have worked with OVC and CABHA for a minimum period of one year.
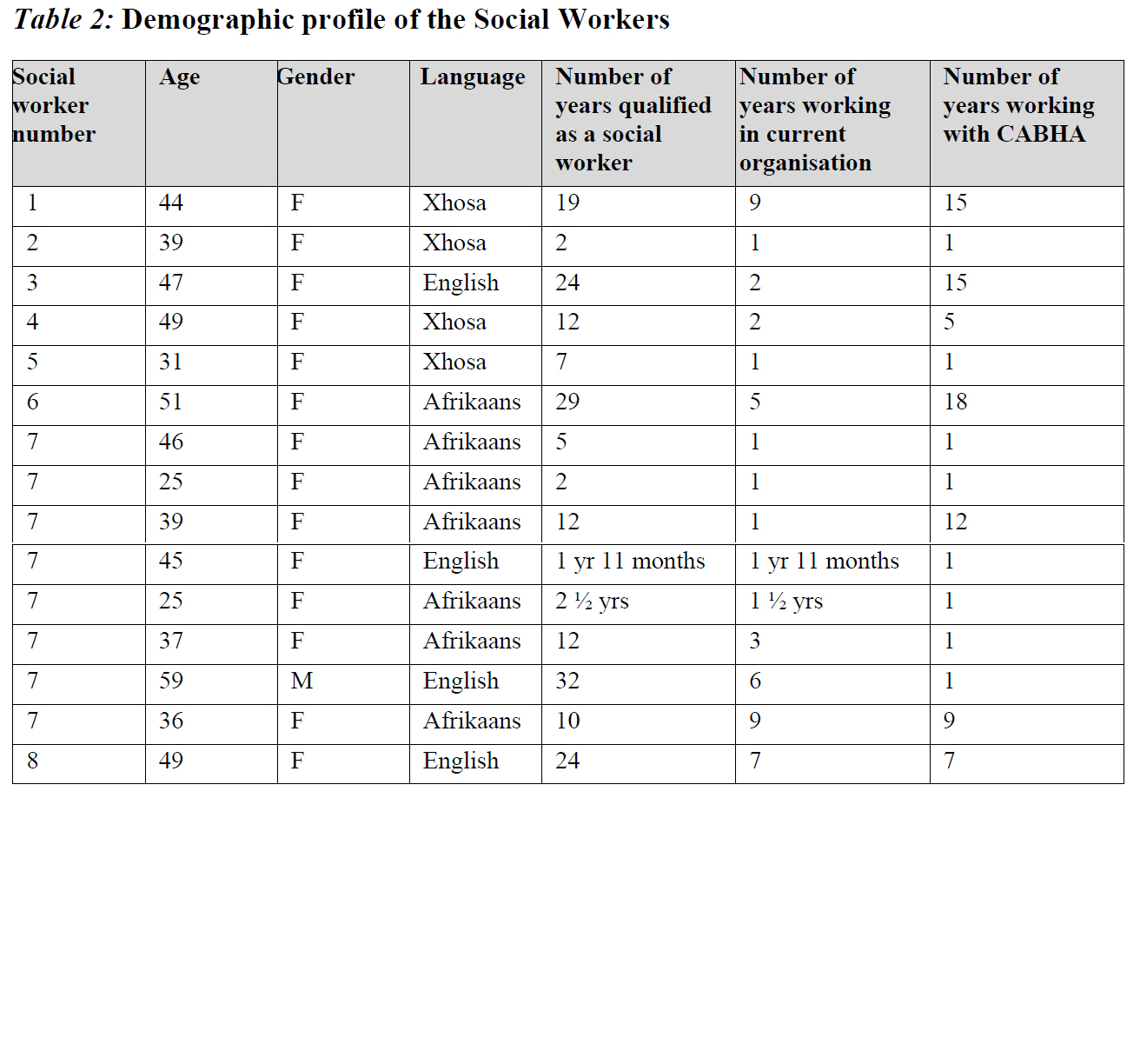
15 social workers participated in the study. The demographic profile of the social workers is detailed in Table 2.
All the social workers were interviewed individually, except in the case of one organisation. Eight social workers were interviewed as a group due to operational demands that made it impossible for them to be available individually at separate times. The social workers in this organisation are allocated the same number in Table 2 (7). The responses from this group are labelled SW7 since they were captured as part of the focus group interview. Most of the participants in the sample were female (n=14), with only one male participant. The age range was between 25 and 59 years, with the oldest being a male participant. The reason for this can be attributed to the fact that there were no male social workers in all the organisations that were approached. Just over half (n=8) of the social workers had more than ten years of being qualified as social workers. Five social workers indicated that their social work experience did not directly relate to children affected with HIV, but focused on general OVC. At the same time, the remaining group had some experience with children affected by HIV.
Data collection
Data were collected in two stages. The first stage focused on interviewing service providers to identify and describe the intervention models used by various organisations working with CABHA. The service providers selected by the organisations were people they felt would best represent them, and they included different categories of staff, such as social workers in some organisations. The second stage consisted of interviews with only social workers, and it aimed at exploring the experiences of social workers using interventions aimed at CABHA. These were social workers who did not participate in stage one. Each stage had a different set of participants who were interviewed. The interview type depended on the number of people available for the study in an organisation. In both stages of the study, data were collected through either one-on-one interviews or focus groups with participants from organisations that provide services to CABHA. In organisations with one participant, one-on-one interviews were used, and when more than two participants were available, data were collected through focus group interviews. Interviewing participants in groups allows the researcher to engage participants in a discussion and gather diverse perspectives (Geyer, 2021). Permission was sought from the participants' employers for the researcher to gain access. Once permission was granted, the researcher contacted the participants and they voluntarily agreed to participate in the interviews. Participants were assured that the information shared would be kept confidential and were made aware of their right to withdraw from the study at any given point in time. The option of counselling by a registered social worker was offered to participants, if they needed it after participating in the study, but none of them felt the need for this. Interviews took place in venues chosen by the participants, which was their place of employment in all the instances, and the interviews lasted between 60 to 90 minutes. All of the interviews were conducted in English as all the participants were comfortable conversing in English.
Data analysis
The data from the interviews were recorded, transcribed and analysed through thematic analysis. Creswell and Creswell (2018:193) urge researchers to "look at qualitative data analysis as a process that requires sequential steps to be followed, from the specific to the general and involves multiple layers of data analysis". This approach to data analysis involves five steps. The first step is organising and preparing data for analysis. This involved going through the transcripts, giving pseudonyms and linking them to fieldnotes made during the interviews. As explained in the previous section, there were 15 social workers, but there were 8 transcripts because of the different interviewing methods used. Each transcript was allocated a number between 1 and 8, and the transcript where a focus group of eight participants was used was labelled as number 7. The second step involved reading through all the data to get a sense of all the information in the transcripts, trying to see if participants answered the questions in the interview schedule and understanding the responses. This stage involved going back to the interview schedule, looking at the questions and assessing the responses in each transcript to check if the participants had answered the questions. The responses in the transcripts were compared to the field notes to check if the information corresponds. Where there was uncertainty or gaps, the researcher returned to the recordings to check if any information was missed.
The third step is where the coding process starts. This is where similarities in the participants' responses were noted, and this was done by creating a table to write down the information. This table contained responses given by participants to each question from the interviews. Where common elements were found in responses to each question, a keyword that summarised the participants' main point was noted. These keywords helped compare participants' responses with similar group responses to check if participants were alluding to the same thing. The differences in responses were also noted down. The fourth step was made by summarising the common elements identified to generate a description of the words described in the third step. This was done to ensure that there was no repetition and to merge some of the keywords or separate them further into different ones. This process resulted in developing themes and sub-themes from the participants' responses. The fifth step involved checking for interrelating themes. This is the process of rechecking if some of the themes identified could be merged or separated further and deciding which parts become sub-themes or categories. Some of the words used for subthemes were either too general or could be interpreted differently, which is why categories were added to clarify the subthemes. These became the final themes that were deemed appropriate for the study. An explanation of the themes is given in the results section.
ETHICAL CONSIDERATIONS
Permission to conduct the study and ethical clearance was granted by the Department of Research Development of the University of the Western Cape (UWC), with an ethical clearance number of 15/6/30. All information about the study was shared with the participants before they engaged with the research to discuss the aim, objectives, risks, benefits and questions that they wanted to raise participants. Participation in the study was voluntary, and participants were allowed to withdraw from the study at any point should they wish to do so.
All personal information of the participants was kept confidential, and the hard copies of information shared were kept in a locked cupboard. Soft copies and recordings were stored on a password-protected laptop.
RESULTS
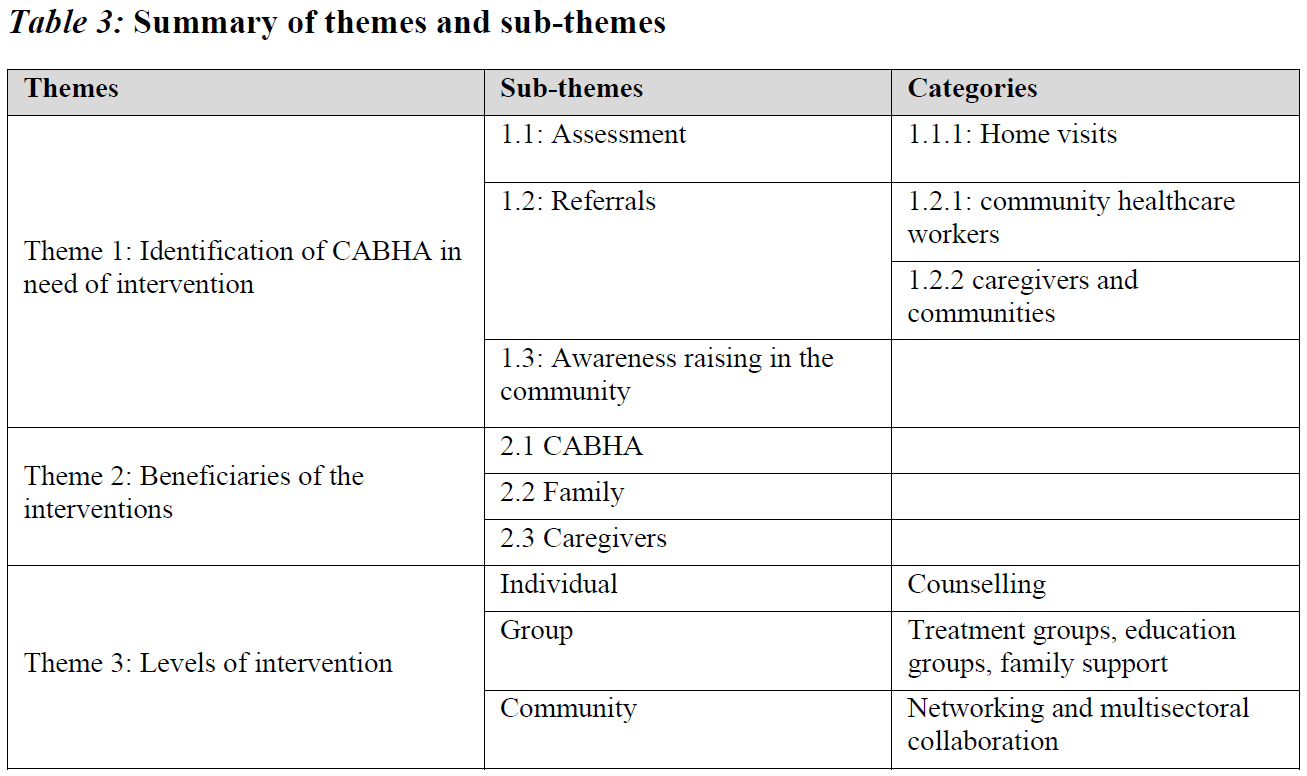
The study results provide detailed reflections by the participants on their experience of the interventions. There were some similarities in the participants' responses in both stages of the data collection. The responses were grouped into three major themes that specifically focus on identifying the need for interventions for CABHA, beneficiaries of the interventions and the levels of intervention. A summary of the themes is presented in Table 3, followed by a discussion.
Identification of CABHA in need intervention
Participants were asked to explain the type of intervention they provide to CABHA. It became apparent that most responses pointed towards the importance of identifying these children in need of intervention before doing the actual work. The participants reported that they follow certain processes that help identify CABHA in need of intervention, including assessment, referral and awareness raising.
Assessment
The participants identified assessment through home visits as their primary method of identifying their clients. Some assessments are done informally through information provided by non-professional staff who conduct home visits and discover that there are OVC in those homes who need care. Social workers conduct some assessments formally. The home visits are either done solely for assessment by social workers or, in some instances, they form part of the daily duties of community workers who may accidentally come across a child needing care while visiting a home for a different purpose. The assessment done by social workers is often referred to as a formal assessment, while the 'accidental' assessment done by other service providers is called an informal assessment. The participants' responses below indicate the different types of assessments.
We also do home assessment, train and refer foster parents. (SW5)
Through my assessment is where I identify that the parent is HIV positive, not only working with children affected by HIV. (AT)
When they [community workers] identified that there is something that needs social work intervention, they send a referral, so it comes straight to us. (SW1)
You pick up the child that is at risk there [during home visits] and the life skills educators then refer them to the OVC programme. (LH)
Regardless of who makes the initial contact, it is clear that the primary practice in most interventions is an assessment to determine the actual needs of CABHA. The results also show that if other service providers or non-professional staff have done the informal assessment, a referral to the social worker is done for further assessment. This means that a social worker does the formal and final assessment. Assessment involves "gathering and interpreting information to understand a person and their circumstances; the desirability and feasibility of change and the services and resources which are necessary to effect it" (Milner, Myers & O'Byrne, 2015:1). Sherr, Skeen, Hensels, Tomlinson and Macedo (2016) argue that if HIV-affected children are to receive evidence-based interventions to maximise their potential, it is important to monitor them within a community setting. The findings of the study, also confirm the importance of monitoring CABHA within their communities and further highlight home visiting as a common practice for the assessment of CABHA who are in need of intervention. The participants' responses indicate that sometimes assessment takes place through home visits and this provides opportunities to identify CABHA in need of intervention. The following comment alludes to this.
The carers go out into the community to go do home visits as well. So, they might come there to take the granny's blood pressure because they were referred from hospital, this person needs a weekly blood pressure or sugar test. When you come there, you find the situation is of such a nature that these children are vulnerable or they are orphans, their parents left them or died from HIV/AIDS. (LH)
It thus becomes important for social workers to assess CABHA within their home environment in order to be able to identify the specific nature of their vulnerability. Godberg and Short (2016) argue that HIV-affected children present with distinct vulnerabilities as a result of living with HIV-infected adults or people ill with AIDS. Home visits, therefore, provide social workers with an opportunity to identify problems in the homes of CABHA, assess how these problems affect their wellbeing and whether they are serious enough to merit intervention (Kirst-Ashman & Hull, 2012). This will ensure that the planned intervention addresses the identified problem and that the organisation provides relevant services to CABHA. Thurman, Kidman and Taylor (2014) argue that community-based home visiting is a common mechanism for providing support services to HIV-affected families. Home visiting is a popular component of programmes for HIV-affected children in Sub-Saharan Africa, but its implementation varies widely (Kidman, Nice, Taylor & Thurman, 2014). Similarly, Betancourt et al. (2014) agree that home visiting enhances access by allowing counsellors to reach many HIV-affected children at once and reduces the barriers that many vulnerable families face when trying to access healthcare or centre-based psychosocial interventions. This highlights the need for service providers to invest in home visiting as a valuable strategy to identify CABHA in need of intervention. On the other hand, Thurman et al. (2014) caution that home visiting may be ineffective at times, which means that there is a need for a thorough and more structured assessment to be done that does not depend only on home visiting.
Referrals
As mentioned above, referrals were also identified as a sub-theme and an important part of identifying CABHA in need of intervention. The most common referrals of CABHA identified by the participants come from healthcare facilities such as clinics or hospitals. Still, there were also referrals from other service providers that were identified. The statements below show the participants' explanations about referrals.
The process is that we get children referred by clinics, by schools and some are brought by their own parents. (SW8)
The community people, the caregivers and manager of community centre refer clients. (SW2)
We receive referrals for children affected where the mother is in the hospital, or the parent can't disclose to the children about HIV-positive status. (SW1)
The participants' statements above reflect the importance of the referral process to ensure that CABHA receive the necessary assistance. Kirst-Ashman (2017) stresses the importance of referral to other professionals, who have the knowledge and skills necessary for making progress with clients. This will ensure that CABHA receive the services that they need from agencies which have the competency to provide such services. This means that identification of the need for intervention is a process that needs to be well coordinated between those involved in conducting the initial assessment and other stakeholders working with CABHA to ensure that proper referrals are made. This will ensure that CABHA are directed to relevant service providers for intervention. Collaboration between the different stakeholders working with CABHA is fundamental to proper identification of CABHA who are in need of intervention. Section 54 of the Children's Act 38 of 2005 (RSA, 2006) requires that children in need of care be referred to a designated social worker for investigation and intervention. Referral to other service providers with the necessary expertise in the field is very important because, according to Thurman et al. (2014), home visitors who are not formally trained have limited counselling skills. Even their own psychological challenges may inhibit their ability to address clients' emotional needs. It thus becomes very important for the non-professional staff who conduct informal assessments, with their limited counselling skills, to refer CABHA to a social worker for a formal assessment and intervention in line with legislation and to ensure that there is proper follow-up.
Awareness raising
Raising awareness in the community is the third process in identifying children in need of care; this relates to self-referrals that are the result of the organisations creating awareness and publicising their services in the community. Organisations identified awareness raising through different mediums of communication as playing a significant role in recruiting community members to take part in the interventions or referring those in need of intervention. The participants reported that:
We are based at the clinics, we made boards on the clinics to make people aware, we give information to people, so that people can be aware of us. (YB)
Usually, it 's word-of-mouth like if we work in the community there 's always word-of-mouth that's going out. (GU)
Handing out flyers in the community so that there 's just awareness that this programme will be happening for the children and the teenagers. (LH)
The method of raising awareness differs for each service provider as each use the resources they have at their disposal to ensure that the public knows about their services. Raising awareness in the communities about interventions aimed at CABHA means that the community members are indirectly involved in the interventions and are part of the recruitment process. This may create a sense of trust in the community and ensure that community members take ownership of the interventions happening in their communities (Tumwesige et al., 2021). This process enhances the referral process to ensure that CABHA can access the services that they need. Kumakech, Cantor-Graae, Maling and Bajunirwe (2009) and Mueller et al. (2011) advocate for the importance of the participation of affected communities in interventions that affect CABHA in the communities, as this ensures that the communities embrace these interventions. If communities are aware of the services provided by the different organisations, they will be able to direct CABHA and families to the correct service providers. This strengthens the process of identification of CABHA who are in need of intervention. Awareness raising makes it easy for the information to reach the potential beneficiaries, because community members are most likely to spread the word, which will encourage CABHA to seek access to the needed services.
Beneficiaries of the interventions
The participants explained that after identifying the need for intervention, they need to decide who the beneficiaries of the intervention will be. All the participants identified children as their main beneficiaries of interventions, and the differences lay in the way the programmes were implemented and whether they included other people in interventions. Two types of beneficiaries identified are CABHA and families.
Children affected by HIV and AIDS
Organisations mostly use the term orphaned and vulnerable children (OVC) to describe the types of children who are beneficiaries of interventions implemented. CABHA were identified as part of OVC, since they are also vulnerable as a result of exposure to parental HIV. The term OVC is described by Wood and Goba (2011:276) as referring to:
any child whose level of vulnerability has increased as a result of HIV and could include any child under the age of 18 who falls into one or more of the following categories: has lost one or both parents or experienced the death of other family members; is neglected, destitute, abandoned or abused; has a parent or guardian who is ill; has suffered increased poverty levels; has been the victim of human rights abuse; is HIV positive themselves.
According to the above description, CABHA meet the criteria to be called OVC as they may be experiencing a parent/caregiver who is ill or died as a result of HIV and may end up destitute or neglected because of the absence of a parent/caregiver. Research shows that it is clear that CABHA face particular difficulties that require an inclusive approach. When explaining who the beneficiaries of the interventions were, the participants reported that:
We provide a safe home and environment and family to orphans and vulnerable children. (H4H)
There is a lot of children who are living as orphans with parents who died because of HIV and AIDS. (SW7)
In the Children 's Act it doesn't say differentiate between a HIV and non-HIV child, so we look at the best interest of the child always. (SW7)
The aim is looking at OVC, this OVC can either be HIV negative or HIV positive and provide holistic issues or holistic approach in making sure that all their needs are being met. (NCS)
Some participants explained that they include CABHA as part of the services offered to all OVC, while others explained that their services are specifically aimed at CABHA. The above comments show that the organisations do not separate CABHA from other OVC, as these children are also vulnerable as a result of parental HIV illness/death, but they may have specific needs that are different from other OVC. This means that the organisations do not discriminate between HIV-positive and -negative children, as all children are affected by HIV regardless of their own HIV status. They acknowledged the different needs that CABHA have compared to the rest of the OVC, such as antiretroviral (ARV) medication for those infected, dealing with HIV-infected and ill parents as well as stigma and discrimination. The issues that are specific to CABHA are described in the following comments:
We work directly with the kids, those affected and infected, what we found is as the kids get old, they start wanting to know why they have to take tablets always, that creates a stigma which we try to work around dealing on that. (SW3)
There is fear attached to HIV and AIDS, they meet other children that are HIV positive, they understand that they are not alone in this and it's not the end of the world if you're HIV positive. (SW2)
It is clear that issues related to the vulnerabilty of CABHA cannot be ignored, as Godberg and Short (2016) argue that one group of HIV-affected children with distinct vulnerabilities are those living with HIV-infected or AIDS-ill adults. This shows that there is still a need for interventions for CABHA.
Families
Furthermore, in explaining the inclusive nature of their interventions, the participants also mentioned including other family members such as parents or caregivers. The following responses were given regarding the inclusion of family members in the intervention:
We encourage parents to go to workshops of parenting. (SW1)
We work with parents as well, we have a disclosure support group. (SW6)
We have a programme for men, we call it 'life skills for men and young men'. It's a mentoring programme because you know that men often feel that it 's difficult for them to speak out. (AT)
Visser et al. (2015) explain that in Africa orphans and vulnerable children are often cared for in extended families or child-headed households and are vulnerable to poverty. Thus, interventions must include family members who may not necessarily be immediate family. Still, other family members may also be included in interventions, as HIV in the family affects everyone. Sherr et al. (2014) agree that this is especially true in Sub-Saharan Africa for younger children. The care input comes from the wider extended household and may not be vested exclusively in a single caregiver. This shows the importance of considering the extended family context when providing services and interventions for CABHA and that interventions for CABHA are not isolated, but are included as part of general interventions for OVC. Involving the family in interventions ensures that the relevant and affected systems within the family are also part of the solution. Furthermore, this ensures the long-term sustainability of the support and coping methods in the absence of the social worker after the intervention has ended.
Levels of intervention
The participants reported that they approach their service delivery at different levels of intervention, depending on the needs of their clients. These levels of intervention identified were micro (individual), mezzo (group) or macro (community) levels.
Micro level
The most common intervention mentioned by the participants is the micro level, which involves working with an individual client. Zastrow (2017: 42) explains that micro practice is aimed at:
helping individuals on a one-to-one basis to resolves personal and social problems and may be geared to help clients adjust to their environment or to changing certain social and economic pressures that adversely affect them.
In their responses, the participants often used the term 'children' to refer to CABHA, since the interviews focused specifically on CABHA. In explaining the type of counselling services that they offer, the participants reported:
Psycho-social service is about counselling for kids, but we also support families, we also have disclosure counselling. (GU)
We also give the ongoing support because the children [CABHA] are growing so they go to a certain age of becoming teenagers, so they need to get the [correct] information about HIV. (YB)
I do individual counselling for children and some families. (SW6)
We also run therapeutic counselling for them individually, because of their age, early childhood, I use a lot of play therapy. (SW4)
Children affected by HIV and AIDS, including "those orphaned by AIDS and those living with HIV/AIDS, often find themselves at the intersection of HIV/AIDS, poverty, and mental health challenges" (Tumwesige et al., 2021:2). The issues highlighted by the participants indicate that CABHA are often faced with problems that affect their emotional wellbeing and requires them to receive professional counselling. These are problems that afflict mainly CABHA as their vulnerability is exacerbated by the effects of their parental HIV. Previous studies (Breckenridge, Black-Hughes, Rautenbach & McKinley, 2019; Nabunya et al., 2019; Schenck, 2009; Sherr et al., 2016; Tucker et al., 2016; Visser et al, 2015) have shown that children affected by caregiver and household HIV often face adverse outcomes in relation to their psychological wellbeing. Furthermore, children experience increased levels of distress and anxiety, and may suffer a variety of psychological reactions following the disclosure of parental HIV status and illness (Murphy, Marelich, Graham & Payne, 2015; Richter et al., 2015), which may in turn subsequently affect the present and future functioning of HIV-affected children. When children's level of functioning is affected, the social worker needs to intervene and provide counselling to assist the child in adjusting to their changing environment to deal with the pressures that adversely affect them. These counselling issues mentioned by the participants are matters that contribute to the vulnerability of CABHA. Murphy et al. (2015) argue that the risk of psychosocial maladjustment in children living with an HIV-positive parent extends through late childhood into early and middle adolescence. This indicates that there are longterm psychological consequences for children affected by parental HIV, which thus necessitates interventions to assist these children in dealing with those issues.
Mezzo level
Participants reported that when dealing with clients who are CABHA, it becomes necessary to bring together groups of CABHA who have similar experiences and provide interventions at the group level. The experiences that most CABHA share relate to living in an environment where the caregiver/parent is HIV-infected. Interventions provided with groups are sometimes referred to as the mezzo level of intervention. Zastrow (2017) explains that when working at the mezzo level of intervention, a social worker seeks to facilitate the intellectual, emotional and social development of the individual through group activities. The participants highlighted different types of group activities that they conduct with the CABHA of different age groups and that the type of groups being facilitated depends on the needs being addressed. Participants explained the reasons for group intervention:
We work directly with the kids, those affected and infected. What we found is that as the kids get older, they start wanting to know why they must take tablets always and that creates a stigma which we try to work around dealing with that. (SW3)
There is fear attached to HIV, they meet other children that are HIV positive, they understand that they are not alone in this, it 's not the end of the world if you 're HIV positive. (SW4)
The participants' explanation of the focus of the groups suggests that the types of group sessions conducted with CABHA are treatment groups, since the focus is on helping them deal with HIV stigma and the associated fears. Previous studies (Nabunya et al., 2019; Visser et al., 2015) identify stigma as a common experience for CABHA in communities and other social spaces, which often leads to mental health issues such as stress and anxiety. Children who live in poverty and have lost a parent due to HIV-related illness are more likely to have weaker coping mechanisms (Breckenridge et al., 2019). Treatment groups provide CABHA with a space for support from other children who might have gone through similar experiences. Popa (2017) explains that treatment groups aim to treat and heal their members' socio-emotional distress and bring together persons with similar needs. According to Popa (2017), the functions of treatment groups can be divided into the following categories: socialisation, recreation, education and self-support or mutual support groups. The type of treatment group identified in the study is mutual support groups. Mutual support groups are meant to assist members in overcoming stressful life situations. Popa (2017: 51) explains that the benefits of these groups are "the mutual help offered between members, support to solve different issues and new approaches to resolve problems". Mutual support groups, therefore, provide a space for CABHA to share their experiences with peers who have gone through similar circumstances. Previous studies (Kumakech et al., 2009) suggest that peer-group support intervention has a significant impact on helping AIDS orphans deal with psychological problems. When group members give and receive support and help from each other, this mutual aid empowers them to feel useful, while learning to accept help and support from others (Garrett, 2004). With this support, group members may feel encouraged to deal with the stressors they experience in their communities.
Macro level
The macro level of intervention was also mentioned by most participants, who indicated that they work with communities where the children affected by HIV are coming from.
Networking with other organisations was mentioned as one way of providing intervention at the macro level.
I am also networking on other organisations because we deal with referrals, so I keep in touch with them. (GU)
We also run consultative meetings or forums. It's more like all the partners within the community or within the district come together to tackle various issues or various topics or various things that relate to kids. (YB)
We have a child-care forum, do community dialogues, and NGOs get to gather and discuss specifics areas [of service delivery]. (SW2)
These findings indicate that collaboration amongst the existing organisations in different sectors working with CABHA and with the communities where interventions are implemented is key to the running of successful interventions. Organisations need to collaborate with organisations in different service delivery sectors to ensure holistic service delivery. Tumwesige et al. (2021) support collaborations with communities and argue that creating and sustaining community collaborations and partnerships are especially critical when implementing interventions for HIV-affected children and families. Breckenridge et al. (2019) argue that the HIV and AIDS orphan epidemic appears to be the shared responsibility of those at a community level. Sherr et al. (2016) agree that if HIV-affected children are to receive evidence-based interventions to maximise their developmental potential, it is important to monitor them within a community setting and to understand how community-based organisations are positioned as potential providers of support. This confirms the finding that interventions for CABHA need to be collaborative efforts between all the stakeholders involved in the care and management of CABHA and communities. Therefore, it makes sense that social workers planning interventions for CABHA should collaborate with community members to ensure transparency as well as support from communities.
DISCUSSION
This study aimed to explore the existing interventions provided to CABHA by service providers and the experiences of social workers in implementing such interventions. Interventions aimed at CABHA must be well structured to ensure that they provide the correct and relevant services to those needing them. The initial stage of ensuring the relevance of the intervention is first to identify CABHA who need the services through assessment, referral and creating awareness in communities. The assessment is usually done by the person who comes into initial contact with the child in need of care. The results of this study indicate that regardless of the position of the person who identifies the need, most organisations follow the general guidelines as provided by the Children's Act 38 of 2005 (RSA, 2006) stipulating that children in need of care must be referred to a designated social worker for investigation and intervention. The explanations given by the participants suggest that a needs assessment is done before deciding on the intervention. However, the fact that some of the initial assessments of CABHA are done by non-professional staff needs to be carefully reconsidered, since there was no mention of how this process is monitored. Thurman et al. (2014) argue that caution should be exercised when using untrained staff to work with CABHA, as they may not have the necessary skills to deal with the complex issues entailed in attending to CABHA. CABHA often face "developmental, psychosocial and economic adversities, less social support, fewer education opportunities, and higher risk for mental health challenges and risk-taking behaviours, compared to the general population" (Tumwesige et al., 2021:2). Furthermore, parental illness may lead to mental hardship and loss of freedom for CABHA who need to care for a sick loved one, as well as disruptions to their education, isolation, the possibility of familial exploitation, and the stigmas associated with being an AIDS orphan (Tucker et al., 2016). These issues require a person who is skilled enough to be able to deal with such problems. This means that organisations rendering interventions to CABHA need to ensure that those responsible for informal assessments of CABHA in need of intervention have adequate training and supervision provided to them on issues pertaining to CABHA.
Furthermore, these organisations must train their staff in all legislation related to children and make sure that their programmes align with the Children's Act 38 of 2005 (RSA, 2006). This will ensure that when they identify CABHA in need of intervention, they are directed to the correct intervention. Once the need for the services and intervention has been established, the organisation can decide how the intervention should be structured. There is no universally correct way to conduct interventions aimed at CABHA, and each organisation structures interventions based on the needs identified. The problem, though, is that most organisations include CABHA as part of their service provision to OVC, which means that the specific needs of CABHA may be overlooked. This highlights a need for organisations to revisit their interventions to establish how to accommodate needs relating specifically to HIV and AIDS vulnerability. Even though the child is the centre of the intervention, the beneficiaries often involve the caregivers/parents and other family members. It is also clear that the levels of intervention at the micro level can benefit the child as an individual. Still, there is also an added benefit on the mezzo level of intervention, where CABHA often learn from those who have gone through similar experiences through support groups. Group members can learn that they are not alone in dealing with problems and can gain hope by observing others resolve their concerns (Popa, 2017). Previous studies have shown some benefits for CABHA who attend group sessions as they may feel supported by peers (Kumakech et al., 2009). Furthermore, Murphy et al. (2015) argue that there is a critical need to develop evidence-informed interventions that assist children in coping with parental HIV infection in a developmentally appropriate way. Participating in group sessions may therefore assist CABHA in dealing with the stress associated with having a parent who is ill.
Multisectoral collaboration amongst the organisations that work with CABHA is also key to the macro level of intervention. This indicates that it is important for organisations working with CABHA to liaise with one another to share their expertise. Collaboration with communities where interventions are implemented ensures that the interventions are adopted and supported by the communities where they are implemented. This is evident in the involvement of communities in marketing the interventions to the potential beneficiaries. Burke et al. (2015) concur that the inclusion of a variety of community-based organisations in the planning of a programme for CABHA helps to develop interventions that are attractive to both community members and the professionals who deliver such programmes. Social networks developed through group and community collaborative processes are important for building protective community environments for children affected by HIV (Tumwesige et al., 2021). Community-based interventions should thus be encouraged by service providers and not underestimated as a significant source of support for CABHA.
LIMITATIONS
The recruitment process was challenging as government social workers could not participate in the study because of staff shortages and increasing work demands. This means that the focus of the study was mainly on NGOs, which restricted the participation of other social workers who might have been eligible for the study. The study findings are largely based on the NGO perspectives and are not transferrable to other research contexts. The sampling techniques used - purposive and snowball sampling - were limited in the sense that they depended on the researcher's ability to identify organisations that met the selection criteria of the research as well as on the referrals made by other participants. The other limitation is a possible bias in the responses of some participants where interviews were conducted in groups, as some interview sessions had both superiors and subordinates in one group. Some participants may consequently not have felt free to give a true reflection of their responses in a group setting because of the prevailing power relations between the different group members, thereby influencing the authenticity of the responses.
RECOMMENDATIONS
A number of recommendations are made on the basis of the findings of this study.
• The assessment and referral processes related to CABHA need to be standardised as they are conducted by non-professional staff and volunteers, who may not possess the necessary skills to conduct proper assessments of children in need of care. Social workers need to take on the role of overseeing the supervision of staff who conduct assessments of CABHA to ensure consistency and that the rights of CABHA are protected.
• Partnerships between service providers and communities need to be formalised to form community advisory boards that coordinate interventions for CABHA.
• Organisations that provide interventions for OVC need to restructure their interventions to accommodate the specific needs of CABHA, while also taking care not to create opportunities for discrimination against CABHA.
• The input of CABHA themselves needs to be incorporated into interventions as they need to have a say in what will work for them.
• The organisations and stakeholders involved in the collaborations should work together with social workers and create referral forms that should be used by all non-professional staff when making referrals to CABHA so that there is consistency in these processes.
• Organisations working with CABHA must provide regular training and capacitate volunteers and non-professionals with skills to develop their careers towards a qualification.
• Future research should focus on evaluating the role of non-professionals and paraprofessionals in the implementation of interventions and determining ways these categories of staff can be utilized optimally in the interventions for CABHA.
CONCLUSION
Children are often left orphaned and without adult supervision when the parent or caregiver ultimately dies from HIV and AIDS-related illnesses. Children who are left vulnerable and with no means of support are in need of social work intervention. The Children's Act 38 of 2005 (RSA, 2006) does not give clear guidelines on how interventions should be implemented with children affected by HIV and AIDS. This study aimed to explore not only the existing interventions provided to CABHA but also the experiences of social workers in implementing these interventions. The findings of this study indicate that interventions for CABHA are a continuous and collaborative process. Social workers must conduct a proper needs assessment before planning and conducting an intervention. A needs assessment involves identifying children needing care and deciding on the structure and beneficiaries of an intervention. The level of interventions - micro, mezzo or macro - that social workers may apply depends on the needs of the CABHA who have been identified. The different levels of interventions benefit the children, families and communities affected by HIV and AIDS in different ways. Most importantly, multisectoral collaborations are highlighted as an important source of support for CABHA.
REFERENCES
Betancourt, T., Kirk, C., Munyanah, M., Mushashi, C., Ingabire, C., Teta, S., Beardslee, S., Brennah, R. T., Zahn, I., Stulac, S. F. R. & Cymatare, F. R. 2014. Family-based prevention of mental health problems in children affected by HIV and AIDS: An open trial. AIDS, 28(3): 359-368. [ Links ]
Bhana, A., Mellins, C., Petersen, I., Alices, S., Myeza, N., Holst, H., Abrams, A., John, S., Chhagan, M., Nestadt, D. F., Leu, C. & McKay, M. 2014. The VUKA family program: Piloting a family-based psychosocial intervention to promote health and mental health among HIV infected early adolescents in South Africa. AIDS Care, 26(1): 1-11. [ Links ]
Breckenridge, T. A., Black-Hughes, C., Rautenbach, J. & McKinley, M. 2019. HIV/AIDS orphans in South Africa: NGO interventions supporting transitions to alternative care. International Social Work, 62(2): 502-517. [ Links ]
Burke, S. M., Shapiro, S., Petrella, R. J., Irwin, J. D., Jackman, M., Pearson, F. S., Prapavessis, H. & Shoemaker, J. K. 2015. Using the RE-AIM framework to evaluate a community-based summer camp for children with obesity: A prospective feasibility study. BMC Obesity, 2(21): 1-11. [ Links ]
Creswell, J. W. & Creswell, J. D. 2018. Research design: Qualitatitve, quantitative & mixed methods approaches. 5th ed. Great Britain: SAGE. [ Links ]
Fouché, C. B. 2021. Introduction to the research process. In Fouché, C., Strydom, H. & Roestenburg, W. J. H. (eds). Research at grassroots for the social sciences and human service professions 5th ed. Pretoria: Van Schaik Publishers. [ Links ]
Garrett, K. J. 2004. Use of groups in school social work: Group work and group processes. Social Work Faculty Publications, 6: 1-28. [ Links ]
Geyer, L. S. 2021. Interviews as data collection method. In: Fouché, C. B., Strydom, H. & Roestenburg, W. J. H. (eds). Research at grass roots: For the social science and human service professions. 5th ed. Pretoria: Van Schaik Publishers. [ Links ]
Godberg, R. E. & Short, S. E. 2016. What do we know about children living with HIV-infected or AIDS-ill adults in Sub-Saharan Africa? A systematic review of the literature. AIDS Care, 28(2): 130-141. [ Links ]
Goodman, M. L., Kaberia, R., Morgan, R. O. & Keiser, P. H. 2014. Health and livelihood outcomes associated with participation in a community-based empowerment program for orphan families in semirural Kenya: A cross-sectional study. Vulnerable Children and Youth Studies, 9(4): 365-376. [ Links ]
Han, C., Ssewamala, F. M. & Wang, J. 2013. Family economic empowerment and mental health among AIDS-affected children living in AIDS-impacted communities: Evidence from a randomised evaluation in southwestern Uganda. Epidemiol Community Health, 67: 225-235. [ Links ]
Karimli, L., Ssewamala, F. M., Neilands, T. B., Wells, C. R. & Bermudez, L. G. 2019. Poverty, economic strengthening, and mental health among AIDS orphaned children in Uganda: Mediation model in a randomized clinical trial. Social Science & Medicine, 228: 17-24. [ Links ]
Kidman, R. & Heymann, J. 2016. Caregiver supportive policies to improve child outcomes in the wake of the HIV/AIDS epidemic: An analysis of the gap between what is needed and what is available in 25 high prevalence countries. AIDS Care, 2(14): 142-152. [ Links ]
Kidman, R., Nice, J., Taylor, T. & Thurman, T. R. 2014. Home visiting programs for HIV-affected families: A comparison of service quality between volunteer-driven and paraprofessional models. Vulnerable Children and Youth Studies, 9(4): 305-317. [ Links ]
Kirst-Ashman, K. 2017. Introduction to social work & social welfare: Critical thinking perspectives. 5th ed. Cananda: Cengage Learning. [ Links ]
Kirst-Ashman, K., & Hull, G. H. 2012. Generalist practice with organizations and communities 5th ed. USA: Brook/Cole. [ Links ]
Kumakech, E., Cantor-Graae, E., Maling, S. & Bajunirwe, F. 2009. Peer-group support intervention improves the psychosocial well-being of AIDS orphans: Cluster randomized trial. Social Science & Medicine, 68: 1038-1043. [ Links ]
Li, L., Liang, L. J., Ji, G., Wu, J. & Xiao, Y. 2014. Effect of a family intervention on psychological outcomes of children affected by parental HIV. AIDS Behavior, 18(11): 2051-2058. doi:10.1007/s10461-014-0744-9 [ Links ]
Mann, G., Long, S., Delap, E. & Connell, L. 2012. Children living with and affected by HIV in residential care. UK: EveryChild. [ Links ]
Merriam, S. B. & Grenier, R. S. 2019. Qualitative research in practice: Examples for discussion and analysis. 2nd ed. USA: Jossey-Bass. [ Links ]
Milner, J., Myers, S. & O'Byrne, P. 2015. Assessment in social work. 4th ed. UK: Palgrave. [ Links ]
Mueller, J., Allie, C., Jonas, B., Brown, E. & Sherr, L. 2011. A quasi-experimental evaluation of a community-based art therapy intervention exploring the psychosocial health of children affected by HIV in South Africa. Tropical Medicine and International Health, 16(1): 57 -66. [ Links ]
Murphy, D. A., Marelich, W. D., Graham, J. & Payne, D. L. 2015. Children affected by maternal HIV/AIDS: Feasibility and acceptability trial of the children united with buddies (CUB) Intervention. Clinical Child Psychology and Psychiatry, 20(1): 117-133. [ Links ]
Nabunya, P., Padget, D., Ssewamala, F. M., Courtney, M. E. & Neilands, T. 2019. Examining the non-kin support networks of orphaned adolescents participating in a family-based economic strengthening intervention in Uganda. Journal of Community Psychology, 47(3): 579-593. [ Links ]
Popa, M. 2017. About groups and group work approaches. Social Work Review, 16(1): 49-63. [ Links ]
Republic of South Africa (RSA). 2006. Children's Act, 38 of 2005. Government Gazette, Vol. 492, No. 28944 (19 June 2006). Pretoria: Government Printer. [ Links ]
Richter, L., Louw, J. & Naicker, S. 2015. Training and capacity development: The foundation of interventions to support young children affected by HIV and AIDS in sub-Saharan Africa. Vulnerable Children and Youth Studies, 10(2): 105-117. [ Links ]
Schenck, K. D. 2009. Community interventions providing care and support to orphans and vulnerable children: A review of evaluation evidence. AIDS Care, 21(7): 918-942. [ Links ]
Sherr, L., Cluver, L. D., Betancourt, T. S., Kellerman, S. E., Richter, L. M., & Desmond, C. 2014. Evidence of impact: Health, psychological and social effects of adult HIV on children. AIDS, 28(3): 251-259. [ Links ]
Sherr, L., Skeen, S., Hensels, I., Tomlinson, M. & Macedo, A. 2016. The effects of caregiver and household HIV on child development: A community-based longitudinal study of young children. Child: Care, Health and Development, 42(6): 890-899. [ Links ]
StatisticsSouthAfrica. 2020. Mid-year polulation estimates 2020. [Online] Available: http://www.statssa.gov.za/publications/P0302/P03022020.pdf [ Links ]
Strydom. H. 2021. Sampling techniques and pilot studies in qualitative research. In: Fouché, C. B., Strydom, H. & Roestenburg, W. J. H. (eds). Research at grass roots: For the social science and human service professions. 5th ed. Pretoria: Van Schaik Publishers. [ Links ]
Thurman, R. R., Kidman, R. & Taylor, T. M. 2014. Does investment in home visitors lead to better psychological health for HIV-affected families? Results from a quasi-experimental evaluation in South Africa. AIDS CARE, 26(1): 2-10. [ Links ]
Tucker, L. A., Govender, K., Kuo, C., Casale, M. & Cluver, L. 2016. Child prosociality within HIV-affected contexts: The impact of carer ill-health and orphan status. Vulnerable Chuldren and Youth Studies, 11(4): 352-362. [ Links ]
Tumwesige, W., Namatovu, B., Bahar, O. S., Byansi, W., McKay, M. & Ssewamala, F. M. 2021. Engaging community and governmental partners in improving health and mental health outcomes for children and adolescents impacted by HIV/AIDS in Uganda. Pediatr Med, 4(2). Doi:10.21037/pm-20-86. [ Links ]
UNICEF. 2011. Taking evidence to impact: Making a difference for vulnerable children living in a world with HIV/AIDS. New York: UNICEF. [Online] Available: https://resourcecentre.savethechildren.net/document/taking-evidence-impact-making-difference-vulnerable-children-living-world-hiv-and-aids/. [ Links ]
UNICEF. 2016. For every child, end AIDS. Seventh stocktaking report, 2016. New York: UNICEF. [Online] Available: https://data.unicef.org/resources/every-child-end-aids-seventh-stocktaking-report-2016/. [ Links ]
UNICEF. 2022. Orphanhood. (Unicef.Org) [Online] Available: https://data.unicef.org/topic/hivaids/orphanhood/ [ Links ]
Visser, M., Zungu, N. & Ndala-Magoroa, N. 2015. ISIBINDI, creating circles of care for orphans and vulnerable children in South Africa: Post-programme outcomes. AIDS Care, 27(8): 1014-1019. [ Links ]
Wood, L. & Goba, L. 2011. Care and support of orphaned and vulnerable children at school: Helping teachers to respond. South African Journal of Education, 31:275-290. [ Links ]
Zastrow, C. 2017. Introduction to social work and social welfare. United States of America: Cengage Learning. [ Links ]
Article accepted: 16 June 2023


{kind=link}
{kind=link}
{kind=link}