










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.59 n.1 Stellenbosch 2023
http://dx.doi.org/10.15270/59-1-1089
ARTICLES
Factors influencing relapse in individuals with substance use disorders: an ecological perspective
Nobuhle NdouI; Priscalia KhosaII
IDepartment of Social Work, Stellenbosch University, South Africa https://orcid.org/0000-0002-7053-8442; nobbs00@gmail.com
IIDepartment of Social Work, Stellenbosch University, South Africa. http://orcid.org/0000-0001-7453-4417; priscalia@sun.ac.za
ABSTRACT
Substance abuse is a global problem that has generated considerable concern among patients, families, clinicians and researchers. Existing research has not explored the views of social workers as treatment professionals but has focused on the service users and their significant others. A qualitative study was conducted to explore the factors influencing relapse in individuals with substance use disorders (SUDs) from a social work perspective. The findings revealed that various factors play a role in relapse at the different levels described from the ecological perspective. The study contributes towards the development of strategies to combat relapse and help in formulating relapse prevention programmes.
Keywords: relapse; social workers; substance use disorder; ecological perspective
INTRODUCTION
Substance abuse is a worldwide issue ranked among the top contributors towards crime, reduced productivity, unemployment, dysfunctional family life, political instability and escalation of chronic diseases, injuries and death (Liebenberg, du Toit-Prinsloo, Steenkamp & Saayman, 2016; McCann, Lubman, Boardman & Flood, 2017). According to the United Nations Office on Drugs and Crime (UNODC), statistics reveal that an increased number of people abuse drugs and substances, with children as young as 12 years being treated for drug dependency (UNODC, 2014). The World Drug Report (UNODC, 2017) states that five percent of the global adult population used drugs at least once in 2015 and an estimated minimum of 190 000 people died prematurely from drug usage. In South Africa cannabis, nyaope and heroin are the most common primary substances abused, with young people under the age of 20 years (ranging between 13% -27%) increasingly using substances (South African Community Epidemiology Network on Drug Use [SACENDU], 2022).
Data collected by SACENDU in 2017 showed an increase in the number of admissions to treatment centres for individuals with SUDs. Relapse rates were also observed to be on the rise (SACENDU, 2017). Most recently, SACENDU (2022) reported an increase in the number of persons admitted for treatment from 9 394 in 2020 to 10 938 in 2021 across 94 treatment centres in South Africa. A significant increase in the number of persons seeking treatment was found in Gauteng and KwaZulu-Natal. Research in different provinces around the country has revealed that most individuals treated for SUDs are not first-time admissions into treatment centres (Stokes, Schultz & Alpaslan, 2018; Swanepoel, 2014), establishing that there is an increase in the prevalence of relapse. Relapse is defined as an ongoing use of substances following a period of remission, detoxification or abstinence (Menon & Kandasamy, 2018). According to Marlatt and Donovan (2005), relapse is a formidable challenge in the treatment of all behaviour disorders, especially SUDs. This is mainly because individuals working on their behaviour change are often faced with cravings, cues and thoughts related to the very same maladaptive behaviours they are attempting to change. Connors, DiClemente, Velasquez and Donovan (2013) concur that there are solid indications that relapse is not determined by a singular factor but influenced by several factors that act concurrently. This study seeks to answer the research question: What are the views of social workers employed at treatment centres on factors influencing relapse in substance use disorders? This contrasts with most research, which has focused on the views of service users on the factors that influence relapse (Appiah, Danquah, Nyarko, Ofori-Atta & Aziato, 2017), or has explored how individuals recovering from a SUD experience and sustain their recovery (Stokes et al, 2018). Thus, there is a research gap on the voices of social workers within treatment centres even though they play a significant role on the treatment and support of substance abusers.
LITERATURE REVIEW
Relapse in SUDs can occur because of many factors. Perkinson (2004) argues that about thirty-five percent of patients who relapse do so when they are experiencing negative feelings of frustration, loneliness, anxiety, anger or depression. While exploring relapse prevention strategies in the United States, DiClemente, Holmgren and Rounsaville (2011) suggested that the leading causes of relapse are either intrapersonal or interpersonal factors that further generate high-risk situations which may see the individual going back to using substances after maintaining a period of sobriety. Similarly, a South African study by Voskuil (2015) explored individual (intrapersonal) and socio-cultural (interpersonal) factors potentially associated with relapse among adult substance users discharged from a treatment facility in Cape Town. Intrapersonal factors are those generated by the individuals themselves and may include negative effects such as anger, grief or depression, whereas interpersonal factors are environmental influences such as peer pressure or conflict in interpersonal relationships (DiClemente et al, 2011; Voskuil, 2015).
Daley, Marlatt and Douaihy (2011) argue that although some studies have demonstrated that substance abuse treatment is associated with a major decline in substance abuse, other studies have also shown that the bulk of individuals do relapse at some point following treatment. Moeeni, Razaghi, Ponnet, Torabi, Shafiee and Pashaei (2016) found that two thirds of patients relapse within a year of receiving treatment. Therefore, intertwined with the problem of substance abuse, there is a problem of relapse among patients treated for SUDs. In South Africa, SACENDU reported that 62 percent of patients in the northern region, i.e., Limpopo and Mpumalanga provinces, and 56 percent in the Western Cape treated for heroin abuse had been readmitted for treatment following a relapse (SACENDU, 2017). Afkar, Rezvani and Sigaroudi (2017) maintain that substance abuse gives rise to complications in the psychological, physical and social functioning of a person and treatment should therefore focus on all these areas to minimise the chances of relapse.
Relapse is a problem that has given rise to considerable concern among patients, families, clinicians and researchers alike. Witkiewitz and Marlatt (2011) state that relapse is the most widely noted outcome following treatment for SUDs. Available research has largely explored the perspective of the service users and devoted attention to relapse in relation to specific substances such as alcohol and cannabis in a specific age group, especially among the youth (Mudavanhu & Schenck, 2014; Setlalentoa, Ryke & Strydom, 2015; Swanepoel, Geyer & Crafford, 2016; van der Westhuizen, Alpaslan & de Jager, 2011). Chetty (2011) focused on relapse among members of the South African Police Services, while Swanepoel (2014) concentrated on the causes of relapse among youths in the Gauteng province. Another study in Gauteng explored how individuals recovering from a SUD experience manage to sustain their recovery journey (Stokes et al, 2018). Notably, the studies mentioned concur that there is a dearth of research on the causes of relapse within the South African context. Hence, the aim of this study is to explore the views of social workers employed in treatment centres on factors influencing relapse in SUDs from an ecological perspective.
THEORETICAL FRAMEWORK
The theoretical framework adopted in this study is the ecological perspective. The ecological perspective was developed and defined by Bronfenbrenner (2005) to promote the scientific study of the relationship between human beings and their environment. The cornerstone of the ecological perspective rests on three aspects of human behaviour. Firstly, the individual responds to events according to the way they perceive them; secondly, the individual is an active role player in their environment; and thirdly, human behaviour must be understood in the light of the individual's interaction with their environment (Cook, 2012; Greene, 2008). The ecological perspective is often referred to as the person-in-environment perspective and is foundational in social work practice (Chiarelli-Helminiak, McDonald, Tower, Hodge & Faul, 2021).
Furthermore, the ecological perspective encapsulates the complex interplay between the physical, psychological, biological, social, economic and political forces that play a role in relapse. Lewis, Dana and Blevins (2015) argue that no service user can be treated effectively unless their social interactions are considered. People influence their social environment and are in turn influenced by their social environment. When they develop SUDs, there is a reciprocal effect on the maintenance and resolution of the problem. Effective intervention therefore occurs when all the familial, social and cultural factors that affect the individual's social functioning are considered (Greene, 2008).
RESEARCH METHODOLOGY
Research approach and design
This article reports on the views of social workers on the factors that influence relapse from an ecological perspective. To attain the goal of the study, a qualitative research approach with an exploratory and descriptive research design was employed. Creswell and Poth (2018) state that qualitative research is a way of describing and understanding the meanings that individuals and groups attach to social problems. This was the preferred approach, because it gave the social workers the platform to share their views on the factors influencing relapse into SUDs. Due to limited research on relapse, an exploratory and descriptive research design were found suitable to answer the research question. An exploratory and descriptive design helped attain deeper insights into the causes and nature of relapse, and to understand the reasons why and how it happens from the social workers' viewpoint based on an ecological perspective.
Sampling
The research sample consisted of 20 social workers who work in the field of substance abuse. As professionals who render services daily to individuals with SUDs, social workers were considered as appropriate informants for this study. Non-probability purposive sampling was used in the selection of the research participants. Strydom (2021) states that purposive sampling allows the researcher to choose participants who are representative of the study population. The participants who were selected met the inclusion criterion of being employed in substance abuse treatment centres for a minimum of one year in the Limpopo, Mpumalanga and Gauteng provinces of South Africa. Prior to recruiting participants, ethical clearance was sought and received from the Research Ethics Committee (REC) at Stellenbosch University (Project number: 7665). The principles of informed consent, voluntary participation and confidentiality were adhered to as key ethical considerations in the study. Permission to conduct the research in the selected treatment centres was also requested and granted prior to interviews being conducted with participants.
Data-collection tool
Data were collected using semi-structured individual in-depth interviews. A semi-structured interview guide was used as a data-collection tool. Galleta (2013) maintains that a semi-structured interview helps elicit data grounded in the experience of the participant. Data were collected in May 2019 after receiving permission from four treatment centres and the social workers confirmed their willingness to participate in the study. The interviews were audio-recorded with participants' permission and transcribed to aid the data-analysis process.
Data analysis
Gibbs (2007) points out that qualitative data analysis involves transforming a voluminous amount of data and processing it through analytical procedures into a clear, understandable, perceptive, dependable and original analysis. Thematic content analysis was used to identify the different themes that emerged from the interview transcripts and further broken down into sub-themes, as suggested by Braun and Clarke (2006). The different themes that emerged from the research interviews were placed together and compared to results in the literature before presenting the key findings of the research in a systematic and coherent manner (Schurink, Roestenburg & Fouché, 2021). The main themes that were identified were the levels of the ecological perspective, namely microsystem, mesosystem, exosystem and macrosystem. Moreover, factors that contribute to relapse at these four levels were categorised as sub-themes.
Rigour in qualitative research
Schurink et al. (2021) note that credibility, transferability, dependability and confirmability are four important constructs that reflect the assumptions of the qualitative paradigm. The credibility of the study was ensured through member checking; some of the participants were given their transcripts to check whether they were a true reflection of what was gathered during the interviews. To ensure transferability, interviews were conducted with participants in different provinces to broaden the study's context and enhance the ability to transfer the findings of the study to similar settings. The dependability of qualitative research study hinges on a logical, well-documented and audited process. Thus, the research process employed and the procedures followed are clearly documented as illustrated in the methodology section of the article. Confirmability entails another person other than the researcher objectively confirming the findings of the study (Schurink et al, 2021). Thus, direct quotes from the participants and interpretations of the findings are synthesised and integrated with the literature in the discussion section.
Study limitations
It is acknowledged that the context in which the interviews were conducted in 2019 might have changed because of the COVID-19 pandemic. With that in mind, the findings remain relevant and offer social workers and other health care professionals in the field of substance abuse treatment an opportunity to adapt the recommendations provided when intervening in relapse cases. This can include, among other things, assessing the influence of COVID-19 on patients with SUDs.
RESULTS AND DISCUSSION
Relapse is an unsystematic, complex, and dynamic occurrence that is often determined by a wide range of factors interacting with one another (Gonzales, Anglin, Beattie, Ong & Glik, 2012). Participants' views on factors that influence relapse are presented under the different interrelated ecological levels nested as systems (Bronfenbrenner, 2005), based on the ecological perspective as the theoretical point of departure in this study. The ecological perspective conceptualises the individual's environment as a set of nested structures hierarchically arranged in concentric circles - at four levels around the individual from the closest to the furthest (Healy, 2014). The four system levels of the ecological perspective postulated are the microsystem, mesosystem, exosystem and the macrosystem, which were identified as key themes in this article. However, before discussing the study findings, it is important to present the demographic data of participants to offer context regarding the participants and promote transferability.
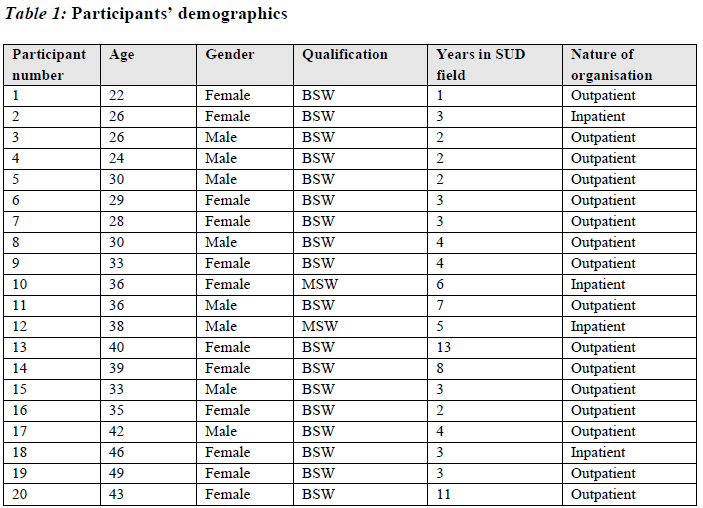
Participants' demographic information
As professionals who render services to individuals with SUDs, social workers were considered suitable participants for this study as presented on the table below.
As shown in Table 1, most of the participants were between the ages of 20 and 40 years, with only four participants above the age of 40 years. Twelve participants were female while the remaining eight were male. Two social workers from the study sample indicated that they had a master's degree in social work while 18 indicated that they had a Bachelor of Social Work (BSW) degree qualification. Most of the social workers had been in the field of substance abuse treatment for five years or less, which establishes that all the participants met the inclusion criterion to participate in the study. Participants were able to share their diverse perspectives on factors that influence relapse based on their experiences working within the field of substance abuse and employed at either an outpatient or inpatient treatment centre. Participants' views on factors leading to relapse amongst individuals with SUDs are discussed next.
Microsystem factors contributing to relapse amongst individuals with SUDs
According to Healy (2014), the microsystem refers to informal systems such as an individual's family, friends and the local community. The microsystem level includes face-to-face interactions between the individual and those closest to them such as family members (Bronfenbrenner, 2005; Greene, 2008). Based on participants' responses, factors that fell under the microsystem level included 1) poor social support, 2) the service user's premature termination of treatment, 3) ineffective use of coping skills, 4) stage at which the service user seeks treatment, and 5) lack of aftercare programme attendance.
The findings of the study indicated that poor social support from family and friends was one of the biggest contributors to relapse. Participants of the study emphasised the need for support following treatment, especially at the family level, as articulated by one participant:
Lack of support from the family, some families are not supportive, sometimes whenever they have an argument the person is reminded of where he is coming from as an addict and because most of these people lack anger-management skills, they just end up going back to using drugs. (Participant 2)
The study has shown that service users sometimes relapse because of the stigma they are exposed to when they go back to their families after treatment. Sometimes the family refuses to have anything to do with the service user, right from the beginning of the treatment process until they are discharged. One participant mentioned the rejection of service users by the family after they exited treatment:
Some of them, when they come back from rehab, the family wants nothing to do with them, other family members even refuse to come for family sessions, they still treat the person as an addict and the individual ends up feeling like there is no point in changing since the family does not see the difference. (Participant 4)
Appiah et al. (2017) aver that service users often relapse because they were met with resentment and hostility, which could include withdrawal of financial, educational and other support structures by family members, leaving them feeling isolated and vulnerable. Swanepoel et al. (2016) also found that many service users relapse because of the absence of family support. On the other hand, Stokes et al. (2018: 1) identified "self, situation, strategies and support' as key factors that enable individuals recovering from SUDs to transition from addiction to sobriety. The authors state that an individual's internal psychological and spiritual resources, support from family and church, strategies to combat cravings and avoiding risky situations lead to a successful journey to recovery. However, social support is not only the responsibility of the significant others in the service user's environment, but the service users have a responsibility to seek other available support structures.
It is evident from the findings that social support plays a key role in the treatment success of the service user. Often, when the family unit is supportive and does not stigmatise the service user, the chances of lasting change outweigh those of relapse. Furthermore, to strengthen family support, social workers need to employ holistic intervention strategies that also target the service user's family, because often significant others such as children or a partner of an individual with an SUD are also directly or indirectly affected by a family member's substance abuse (Schultz & Alpaslan, 2020). However, Panebianco, Gallupe, Carrington and Colozzi (2016) argue that social support can sometimes actually facilitate continued drug use by providing substance purchasing advice, money to buy drugs, and creating an environment conducive to the use of substances. Hence, the support given should reinforce the service user's attempts to abstain as opposed to feeding old habits.
Participants also suggested that overestimation of treatment success is a strong precipitating factor in relapse, whereby the service user exits treatment prematurely because they feel that they can maintain sobriety on their own. Participants pointed out that service users usually become overconfident when they no longer feel the withdrawal symptoms and assume that they can manage independently of the treatment system. Some of the participants' views concerning the effects of premature termination of treatment include:
When they attend the three to four months of treatment, they now feel they are ok, and they don't continue with treatment ... they feel like they are ready to face the world and they go home, and they relapse. (Participant 9)
Another participant further explained that service users downplay the chronic nature of SUDs and therefore tend to believe that it is easy to retain treatment gains.
They believe that once the withdrawal symptoms have subsided, they are ok ... not understanding that this is a chronic illness that requires great commitment. (Participant 4)
In line with the study findings, Swanepoel et al. (2016) found that service users relapsed because they had misperceptions about their ability to control their drug use after treatment. Several scholars observe that the longer the service user stays in treatment, the better the chance they might retain treatment gains (Basu, Ghosh, Sarkar, Patra, Subodh, & Mattoo, 2017; Jhanjee, 2014). However, Basu et al. (2017) argue that the treatment approach should be matched to the treatment needs of the service user. The authors found that some of the individuals with SUDs, who were employed, were more likely to drop out of longer-term treatment interventions because of work commitments. Thus, shorter treatment interventions can be applied for service users who are more susceptible to dropping out. This means that, for service users to be able to sustain treatment gains and avoid relapse, they should adhere to the treatment programme specifically tailored according to their needs.
The study also showed that service users may relapse because they do not know how to deal with the stressors or frustrations they encounter. An example of ineffective coping skills was mentioned by one participant:
Some people don't know how to deal with frustrations, because in here, they have us for 8 hours, if not 24 hours, they have us as their support system, we are always here to listen but, on the outside, they are on their own. (Participant 10)
The application of effective coping skills is regarded as a vital component in relapse prevention and has often been addressed as part of treatment interventions (Kuper, Gallop & Greenfield, 2010). Swanepoel et al. (2016) observed that most participants in their study relapsed because they lacked effective coping mechanisms when faced with stressful events. As suggested by the participant above, some service users learn coping strategies during treatment, but they lack the ability to implement them when faced with an actual high-risk situation. Consequently, they lose motivation and feel as if they have not learnt how to deal with high-risk situations at all, which often leads to their feeling powerless over the situation and relapsing. Isobell, Kamaloodien and Savahl (2015) assert that without motivation, even in an 'ideal' environment where funds, facilities and support are made available, there can be no progress. Some service users relapse because they simply do not believe in themselves (Njoroge, 2018), which suggests the need for the cultivation of greater self-esteem. Thus, what is crucial to the recovery process is the service user's ability to apply the skills and strategies they learn during treatment to avoid relapse.
Service users sometimes relapse because they access treatment at an advanced stage of SUD (severe SUD), which makes it difficult to maintain sobriety (American Psychiatric Association, 2013). Dennis and Scott (2007) believe there is a need for early diagnosis and intervention if treatment is to achieve lasting results. The authors add that the age of substance use initiation and the duration of use before starting treatment are directly related to the time it will take to reach abstinence, as noted by participant 7, "Some of them, by the time [they access services] they are very much advanced in the process of addiction". The participant added that, "Some will not come to the facility until they are compelled by law or family members and sometimes by then, it is too late" (Participant 7).
Moeeni et al. (2016) agree with the participants' views that the longer the service user takes to access treatment, the harder it is for treatment to be effective. Freedman (2018) argues that what further exacerbates the late entry into treatment is the fact that most service users do not willingly present themselves for treatment; they are usually compelled to do so by circumstances. As also found in this study, Freedman (2018) observes that some service users do not voluntarily access treatment but are referred through the justice system or family members as a condition for reintegration into society. Van Wyk (2011) also found that although SUD is chronic in nature, early treatment has the potential to avert a lot of negative effects. Van Wyk (2011) maintains that most practitioners trust that providing treatment at an early stage has the potential to yield positive results before SUD as an illness becomes more severe and more challenging to treat. It can therefore be deduced that early access to treatment has a positive correlation with a later onset of relapse or maintaining sobriety for a longer period.
Participants observed that some service users relapse because they do not attend aftercare programmes. One participant stated, "it's a disease that requires constant maintenance, but they don't attend aftercare" (Participant 5). Dennis and Scott (2007) assert that individuals with SUDs require a variety of support services and can benefit from involvement in aftercare services. Similarly, Mutlu, Demirci, Yalcin, Kilicoglu, Topal and Karacetin (2016) noted that treatment retention tends to decrease over the months following discharge from treatment, especially if service users do not attend aftercare programmes. A study by Burleson, Kaminer and Burke (2012) that investigated aftercare services for adolescents with alcohol use disorders found that active aftercare intervention slows post-treatment relapse more effectively compared to non-attendance. However, Manuel, Yuan, Herman, Svikis, Nichols, Palmer and Deren (2016), after interviewing individuals from a long-term residential substance abuse treatment programme in New York City, noted that only about half of the service users referred for aftercare services access these services, even though aftercare services have been proven to help maintain treatment gains. Moreover, there is lack of adequate monitoring to make sure that service users follow through with recommendations, resulting in their relapsing. Burleson et al. (2012) concur that some service users are simply not willing to attend aftercare, while some are hindered by issues such as travelling arrangements. However, the authors also note that the effectiveness of aftercare largely rests on the motivation of the service user to attend in the first place. In other words, the service user must be motivated to attend aftercare and believe that they will benefit from it.
Burnhams and Parry (2015) suggest that aftercare services are essential; they are usually less costly and more flexible than mainstream treatment, allowing the service user to continue receiving the necessary support and care. Notwithstanding, it has been found that most service users do not continue with aftercare programmes after treatment and there is no follow-up; this often leads to relapse as service users find themselves idle and mixing with the same substance-abusing company (Keen, Sathiparsad & Taylor, 2015; Mahlangu, 2016). Ramlagan, Peltzer and Matseke (2010) contend that lack of funds to continue with aftercare services and the lack of aftercare centres and services are among the reasons why service users do not attend aftercare, which consequently exacerbates factors leading to relapse.
Mesosystem factors contributing to relapse amongst individuals with SUDs
The mesosystem level includes the interactions between the microsystems of the individual's environment such as the school, the family and social services that have a direct impact on the service users' lives (Bronfenbrenner, 2005; Healy, 2014). Factors that were mentioned by participants on this level include 1) exclusion of families from intervention, 2) social stigma from society, and 3) the availability of substances in the service user's immediate environment. The mesosystem forms a vital part of the service user's environment and as such, when they are rejected at this level, their social functioning is negatively affected (Paat, 2013).
The study showed that the exclusion of families in the provision of services was another factor contributing to relapse. One participant shared the following views on the lack of involvement of the family:
One thing I know for sure causes relapse is, when we do the treatment processes, we forget to involve their families ... the family should be involved from the beginning so that they provide the support needed. (Participant 9)
And another said:
Most families do not want anything to do with the service user when he/she is in treatment ... sometimes even when he/she goes back home, he/she is not welcome ... what would you do? ... obviously they go back to using again. (Participant 6)
A study by Paat (2013) on the application of the ecological perspective with immigrant children and their families in the United States demonstrated that family members and peers serve as an important source of support because of the interpersonal relations developed at this level of the mesosystem. The same can be said about the mesosystem structures of individuals with SUDs such as children and their intimate partners (Schultz & Alpaslan, 2022). From a different perspective, Homberger and Smith (2011) observe that families are often seen as part of the problem rather than part of the solution in SUD treatment, even though family involvement should be an essential part of intake, treatment and recovery planning. The authors maintain that families should be furnished with the right information to understand the importance and the gains possible through their involvement in the treatment process. When the family does not understand the trajectory of SUDs, they are most likely not going to be able to support the service user, which leads to the possibility of imminent relapse. Menon and Kandasamy (2018) contend that the lack of knowledge about SUDs within the family unit makes it even harder for the family to deal with the service user; as a result, they avoid the affected family member, which leads to further substance use by the service user.
Sometimes society stigmatises relapsed service users to the point where they no longer have any sense of belonging. In other words, they write themselves off before anyone else can judge them based on their disorder. One participant said:
Society is very judgmental and unforgiving ... it's a sad fact that society will name and shame and not give an opportunity to a person who is saying now I have stopped... that's what really drags them backwards, that the society doesn't really believe that everything is ok now. The service users are willing to stop but immediately [when] they go back to their communities, they are rejected. (Participant 4)
Participants' views show that some people with SUDs do not seek treatment because of the stigma associated with seeking treatment (Amoore, 2016; Sorsdahl, Stein & Myers, 2012). Makhubele (2013) is of the view that society has little empathy for SUD service users and views them as less deserving of treatment compared to individuals with mental or physical disorders, because SUD is regarded as a self-inflicted disorder. As a result of the judgement and social stigmatisation, service users tend not to divulge the severity of their SUD, often to a point that they do not seek help at all (Freedman, 2018). It can also be argued that those who relapse after receiving treatment would be faced with much greater stigmatisation if they even try and access treatment once more, and as a result they relapse 'in silence'. Van Wyk (2011) states that such self-stigmatisation is a major impediment to successful retention of treatment gains.
The findings revealed that the availability of substances in the communities where the service users live makes it hard to keep sobriety. Service users who must interact with the same people in the same environment while accessing treatment are faced with the daily challenge of coming across substances, as indicated by one participant: "an environment where there is a lot of drugs in the area. If there are drugs on every corner, it's very hard" (Participant 10).
Afkar et al. (2017) also found that an environment where substances are readily available and where friends also encourage substance use paves the way for relapse. It can be argued that although the service user has learned of ways to deal with high-risk situations through treatment, they are faced with the same circumstances that first led them to substance use in the first place. They are still in the same environment, spending time with the same people. A study that investigated contributory factors to nyaope use in three provinces of South Africa found that while communities can be effective resources for drug abuse prevention exercises, they can also propagate drug use (Mokwena & Morojele, 2014). Mokwena and Morojele (2014) found that, in addition to easy access to nyaope, high unemployment rates and an unfavourable social environment seem to be contributing to nyaope use amongst youths in various communities of Gauteng, North West and Mpumalanga provinces. Thus, if service users are discharged into the same environment with similar challenges without strong coping mechanisms, they are likely to relapse. Nyege, Dike, Nkamare, Robinson-Bassey and Wokne-Eze (2017) concur that the availability of drugs in the service user's community or surroundings contributes to relapse. Similarly, Meade, Towe, Watt, Lion, Myres, Skinner, Kimani and Pieterse (2015) maintain that service users are easily influenced in the environment, especially those in outpatient treatment, where the helping professionals have little control over their daily lives.
Exosystem factors contributing to relapse amongst individuals with SUDs
The exosystem level consists of elements that have a profound impact on the service user, even though the service user may not be directly involved with them (Bronfenbrenner, 2005; Greene, 2008). Examples of the exosystem can be the treatment facility, whereby some decisions taken, such as the duration of inpatient treatment, may not include the service user but affect them immensely. Among the factors influencing relapse is the length of time spent in treatment. Some participants specifically referred to certain inpatient treatment programmes whereby the service user stays for only a month and a half, which is not long enough, given the chronic nature of SUDs, "Sometimes due to the high demand for treatment, we are forced to implement short-term treatment programmes ... it could be another reason for relapse" (Participant 8). Another participant echoed this view and said that "thesepeople [service users] need to stay in [treatment facilities] longer for them to completely rehabilitate ... otherwise we release them too early when they are not yet ready" (Participant 12).
Similar observations were noted in a study conducted with heroin-dependent adolescents aged 14-18 years hospitalised in a substance treatment centre at Bakirkoy Research and Training Hospital in Turkey (Mutlu et al, 2016). The aim of the study was to evaluate a one-year retention treatment programme and abstinence among heroin-dependent adolescents through self-reporting and regular urine drug screening. Mutlu et al. (2016) found that service users who stayed longer in treatment exhibited a significantly lower risk of relapse compared to those who stayed for shorter periods. Therefore, spending more time in treatment gives the service user enough time to rehabilitate and be sufficiently prepared to return into mainstream society. Njoroge (2018) supports this view by pointing out that the length of stay in a treatment facility has been observed to have a positive bearing on treatment outcomes, as the success rate of treatment rises with the length of stay in treatment. Temmingh and Myers (2012) are of the view that South Africans in SUD treatment centres spend far below the minimum time of ninety days required to attain meaningful treatment gains. On the other hand, Myers, Williams, Govender, Manderscheid and Koch (2018) argue that shortening the treatment period can promote treatment completion. The authors suggest that for service users to strike a balance between treatment completion and maintenance of treatment gains, they can be linked to lower-care services such as aftercare. The quality of treatment services is the determining factor with regards to the retention of positive treatment outcomes rather than the length of time spent in treatment. Appiah et al. (2017) assert that some issues such as shortages of medication and health workers, non-adherence to the treatment schedule and negative staff-service user interactions also contribute to relapse. These could lead to service users choosing to leave the treatment facility earlier than recommended, which culminates in premature termination of treatment as discussed under the microlevel.
The findings revealed that comorbid disorders can be aggravating factors for relapse, especially if only SUD is identified and treated to the exclusion of other underlying disorders. Comorbid disorders are disorders that are experienced simultaneously, resulting in the service user being diagnosed with one or more mental disorder as well as a substance use disorder. For example, the service user may be diagnosed with a certain mental disorder such as schizophrenia over and above the SUD (David & Frenz, 2016). Individuals who seek treatment for one disorder are very likely to have a comorbid disorder and, as such, it is the helping professional's responsibility to do a thorough assessment of the service user to identify such issues. SACENDU (2022) reported that 14% of persons admitted to treatment facilities presented with a comorbidity such as hypertension, liver diseases and mental health problems across different regions in South Africa, demonstrating a need to provide intervention strategies that cater for service users with comorbid disorders. Keen et al. (2015) point out that programmes which focus only on treating SUDs to the exclusion of other comorbid disorders are inadequate to meet the treatment needs of the service users, which may in turn lead to relapse. The participants believed underlying disorders should be identified and brought to the fore, because if they are not addressed, relapse will be unavoidable as noted by one participant:
Some people leave rehab, and you'find that some of the underlying issues have not been addressed ... or even identified. If they are not identified, they will not be addressed, meaning that the service user will seek treatment again. (Participant 5)
The participants' views show that, if the comorbid disorder is not identified and the treatment focuses only on the SUD, this could lead to a relapse and the service user seeking treatment again. When investigating substance abuse treatment approaches in South Africa, Temmingh and Myers (2012) found that an integrated treatment approach, whereby comorbid disorders are treated simultaneously, is beneficial for the service user. Meanwhile, David and Frenz (2016) observe that the presence of comorbidities such as schizophrenia with SUD often results in poor treatment outcomes and subsequent relapse. David and Frenz (2016) further found that comorbidity often results in higher treatment costs as the service user will need specialised psychological and medical care. It can be argued that the financial burden may lead to the service user quitting treatment and relapsing, especially given that most service users are unemployed by the time they access treatment.
Participants indicated that many service users relapse because of poor quality of services rendered at the treatment facilities. While some felt that the lack of quality services was due to the chasing of ever-rising targets demanded by the government from subsidised treatment facilities, others pointed to the issue of Once-off therapy sessions as opposed to carefully planned and long-term treatment plans. As one participant noted:
Most social workers especially those in government, provide crisis intervention instead of [sustained] intervention; they conduct once-off sessions instead of continuing services and checking what is the root cause of the problem. (Participant 19)
One of the participants also pointed to the lack of training and specialised knowledge in rendering substance abuse treatment services as the main reason for poor quality services:
Number one, the quality of therapy. I just feel in the profession of social work it is very rare to come together where we get deep into the gist of what is therapy... you have got so many social workers who cannot conduct a therapeutic session nowadays. (Participant 2)
South Africa is one among many countries where there has been an outcry about the quality of SUD treatment (Meade et al, 2015). Temmingh and Myers (2012) maintain that although the government has responded positively to the outcry at the lack of resources in the substances treatment field by allocating more money, there is still a lack of quality in the services provided, mainly a lack of monitoring and evaluation of services rendered in the country. Myers, Govender, Koch, Manderscheid, Johnson and Parry (2015) add that the field of treatment for addictions in South Africa lacks adequate measurement tools and this has a negative impact on the quality of substance abuse treatment. It can be inferred that a combination of various factors such as of lack of monitoring, chasing targets, lack of knowledge and lack of continuous therapeutic intervention leads to low-quality services rendered, which consequently exposes the service user to relapse.
Macrosystem factors contributing to relapse amongst individuals with SUDs
The macrosystem is the broader social context, which may include public policy, legislation, political systems and large social institutions like government and business (Bronfenbrenner, 2005; Healy, 2014). On this level of the ecological system, the key factor that was discussed was lack of adequate inpatient treatment facilities because of limited fiscal investment from government. Participant 5 said, "Sometimes the service user is ready to go for inpatient, but they have to wait in a long queue to be admitted and by then, they are suffering, and they end up relapsing". Another participant made the point, "I think we just worried that there are not enough resources to cover the demands and we need more registered professional treatment centres" (Participant 10).
Confirming the participants' views, research by Voskuil (2015) that investigated relapse indicators in a treatment facility in Cape Town, South Africa found that the demand for treatment of SUDs is disproportionately high compared to the available services, a problem which is further compounded by readmissions of service users who relapse. Lack of inpatient treatment centres is therefore one of the biggest contributors to relapse as there is no balance between demand for treatment and admission space. Myers et al. (2018) contend that the demand for treatment in South Africa far exceeds the available resources in terms of service providers and inpatient treatment services. Furthermore, Myers et al. (2018) found that service users seeking readmission are not given priority, like those seeking first-time treatment. Van Wyk (2011) asserts that the South African government has always struggled with allocating enough funds to increase the number of treatment facilities in several provinces where there is a high demand for SUD treatment.
SUMMARY
This article discussed factors leading to relapse amongst individuals with SUDs based on the different systems of the ecological perspective: the microsystem, mesosystem, exosystem and the macrosystem. The findings revealed that many factors influencing relapse fall within the microsystem level of the ecological perspective. Poor social support from family members was identified as one of the major contributors to relapse into SUDs at the microsystem level. It can be concluded that over and above what the significant others in the service user's environment can do to help them maintain sobriety, the service user also has a responsibility to make a deliberate effort themselves to make sure that they succeed. For instance, applying effective coping skills as learnt through the treatment process and attending aftercare are some of the responsibilities that are linked to the personal efforts of the affected individual.
Factors that mostly influenced relapse on a mesosystem level are social stigma and the availability of substances in the service user's immediate environment. When service users are stigmatised, they lose a sense of 'fit' in the community, and when substances are easily accessible, they fall back into the same pattern of use, losing the gains of treatment. The study concludes that the exclusion of family in the treatment process can also be an aggravating factor, as the family is left clueless on how to assist or support the affected individual.
On the exosystem level, factors included inadequate time spent in treatment, inadequate diagnosis of comorbid disorders, and poor-quality treatment services. Comorbid disorders make it difficult to maintain treatment gains, especially if only the SUD has been addressed to the exclusion of the comorbid disorder. Moreover, the time spent in treatment has a bearing on the effectiveness of the treatment. Depending on several factors such as the severity of the SUD and the substance of choice, some service users may need to stay in treatment longer than others. On a macro level, the inadequacy of inpatient treatment facilities, particularly inpatient centres, was among the leading contributors to the relapse of service users.
Sometimes when service users are placed on a lengthy waiting list because inpatient treatment centres can deal with only limited numbers, they eventually give up on the whole idea of getting treatment and living a life of sobriety. Thus, government should invest more in the establishment of public inpatient facilities based on the needs and demands for treatment in communities. This will enable service users to have timely access to inpatient treatment, which will in turn impact positively on their treatment process.
IMPLICATIONS FOR SOCIAL WORK PRACTICE
The study showed that most factors that precipitate relapse fell under the microsystem level. There could be two reasons for this: first, because social workers mostly render services to individuals (microsystem) and families (microsystem) within the larger community which includes churches and schools (mesosystem). It is therefore important for social workers and social service providers to understand how individual behaviour can be influenced or influence family dynamics when intervening in substance abuse cases. Moreover, knowledge of the various contributing factors under each level of the ecological perspective will assist social workers to formulate relevant treatment programmes and intervention strategies to minimise relapse and alleviate the scourge of substance abuse in communities, which has left so many families dysfunctional because of its influence on gender-based violence, child abuse and crime. Social workers also have a key role to play in establishing and maintaining collaborative relationships between the different stakeholders or government departments concerned with the social welfare of communities to facilitate holistic substance abuse treatment programmes.
RECOMMENDATIONS
Recommendations are presented in accordance with the levels of the ecological perspective flowing from the factors discussed.
Recommendations on a microsystem level
• Treatment programmes offered within substance-abuse treatment facilities should include the service users' family from the beginning to the end; this would help families to gain optimal understanding on the nature of SUDs and the importance of their support to the service user. This could be fostered by helping them to understand that the treatment success benefits not only the service user, but also the family unit.
• Life skills programmes should form most part of the service user's treatment programme to foster their assertiveness and coping skills. This is feasible if funds can be allocated for skills training at the end of each treatment programme. Thus, funding from government, non-government organisations (NGOs) and the private sector such as businesses is essential to invest in the development of technical and social skills among service users to build resilience that could limit the chances of their relapse.
• Social workers should also motivate and encourage service users to attend aftercare programmes consistently through intervention strategies such as motivational interviewing. Treatment professionals may also encourage service users to attend aftercare by keeping contact and arranging follow-ups with the service users after treatment. In addition, family members can play a significant role by offering the necessary financial and/or emotional support.
Recommendations on a mesosystem level
• Society should be well informed about the nature and trajectory of SUDs so that they refrain from stigmatising service users who have received treatment and are in the recovery process. This can be achieved through dissemination of information about SUD treatment widely to society to gain knowledge and understanding of the nature of SUDs. In line with the information age and the advancement in technology as well as the popularity of different social networking platforms, dissemination of credible information via social media campaigns and the audio-visual media can have an impact as most people have access to either radio, television or social media.
• A society free of drug and substance abuse is possible by eradicating harmful substances from communities. This can be done through collaborative work between community members and law enforcement, while social workers can facilitate the collaboration as advocates for social change.
Recommendations on an exosystem level
• Social workers in the field of substance abuse should be trained regularly on new developments and trends related to SUDs to help improve the quality of services rendered to service users. Training of social workers involved in the treatment of SUDs should start at the tertiary level. Thus, social work educators have a role to play in curriculum development by advancing evidence-based approaches to the treatment of SUDs.
• Substance-abuse treatment facilities should also embark on regular in-service training for their staff to keep them abreast of the latest developments in the SUD field.
Recommendations on a macrosystem level
• There is a need for government to invest in the establishment of public inpatient facilities based on the needs and demands for treatment in various communities. This will enable service users to have timely access to inpatient treatment, which will in turn impact positively on their treatment process.
REFERENCES
Afkar, A., Rezvani, S. M., Sigaroudi, A. E. 2017. Measurement of factors influencing the relapse of addiction: A factor analysis. International Journal of High-Risk Behaviours and Addiction, 6(3): 1-9. [ Links ]
American Psychiatric Association. 2013. Diagnostic and Statistical Manual of Mental Disorders (DSM-V). Washington DC: AΡA. [Online] Available: www.psychiatry.org/patients-families/addiction/what-is-addiction [Accessed: 2018/10/05]. [ Links ]
Amoore, N. 2016. Co-ordinated care of substance use disorders: Re-thinking the treatment paradigm. Mental Health Matters, 3(4): 32-34. [ Links ]
Appiah, R., Danquah, S. A., Nyarko, K., Ofori-Atta, A. & Aziato, L. 2017. Précipitants of substance abuse relapse in Ghana: A qualitative exploration. Journal of drug issues, 47(1): 104-115. [ Links ]
Basu, D., Ghosh, A., Sarkar, S., Patra, B. N, Subodh, B. N, & Mattoo, S. K. 2017. Initial treatment dropout in patients with substance use disorders attending a tertiary care de-addiction centre in North India. The Indian Journal of Medical Research, 146(8): 77-84. [ Links ]
Braun, V. & Clarke, V. 2006. Using thematic analysis in psychology. Qualitative Research in Psychology, 3: 77-101. [ Links ]
Bronfenbrenner, U. 2005. Making human beings human: Bioecological perspectives on human development. New Delhi: SAGE. [ Links ]
Burleson, J. A., Kaminer, Y. & Burke, R. H. 2012. Twelve-month follow-up of aftercare for adolescents with alcohol use disorders. Journal of Substance Abuse Treatment, 42(1): 78-86. [ Links ]
Burnhams, N. H. & Parry, C. D. H. 2015. The state of interventions to address substance-related disorders in South African workplaces: Implications for research, policy, and practice. South African Journal of Psychology, 45(4): 495-507. [ Links ]
Chetty, M. 2011. aCauses of relapse post treatment for substance dependency within the South African Police Services. Pretoria: University of Pretoria. Master's Thesis. [ Links ]
Chiarelli-Helminiak, C. M., McDonald K. W., Tower, L. E., Hodge, D. M. &. Faul, A. C. 2021. Burnout among social work educators: An eco-logical systems perspective, Journal of Human Behavior in the Social Environment. 931-950. [Online] Available: https://doi.10.1080/10911359.2021.1977209 [Accessed: 2022/03/23], [ Links ]
Connors, G. J., DiClemente, C. C, Velasquez, M. M. & Donovan, D. M. 2013. Substance abuse treatment and the stages of change: Selecting and planning interventions. New York: Guilford Press. [ Links ]
Cook, E. P. 2012. Understanding people in context: The ecological perspective in counselling. Alexandria: American Counselling Association. [ Links ]
Creswell, J. W. & Poth, C. N. 2018. Qualitative inquiry and research design: Choosing among five approaches. Los Angeles: Sage. [ Links ]
Daley, D. C, Marlatt, A. G. & Douaihy, A. 2011. Relapse prevention. In: Ruiz, P. & Strain, E. C. (eds.). Lowinson and Ruiz's substance abuse: A comprehensive textbook. Philadelphia: Lippincott & Wilkins. [ Links ]
David, A. & Frenz, M. D. 2016. Diagnostic comorbidity in DSM-5: Origins, current status, and potential solutions. [Online] Available: https://pro.psychcentral.com/diagnostic-comorbidity-in-dsm-5-origins-current-status-and-potential-solutions/ [Accessed: 2019/06/06]. [ Links ]
Dennis, M. & Scott, C. K. 2007. Managing addiction as a chronic condition. Addiction Science and Clinical Practice, 4(1): 45-55. [ Links ]
DiClemente, C. C, Holmgren, M. A. & Rounsaville, D. 2011. Relapse prevention and recycling in addiction. In: Johnson, B. A. (ed.). Addiction medicine: Science and practice. New York. Springer. [ Links ]
Freedman, M. J. S. 2018. Coming clean about substance use disorder: Factors affecting treatment-seeking and compliance, and strategies to overcome them. Occupational Health Southern Africa, 24(1): 4-8. [ Links ]
Galletta, A. 2013. Mastering the semi-structured interview and beyond: From research design to analysis and publication. New York: New York University Press. [ Links ]
Gibbs, R. G 2007. The nature of qualitative analysis. In: Flick, U. (ed.). Analysing qualitative data. London: SAGE. [ Links ]
Gonzales, R., Anglin, M. D., Beattie, R., Ong, C. A. & Glik, D. C. 2012. Understanding recovery barriers: Youth perceptions about substance use relapse. American Journal of Health Behaviour, 36(5): 602-614. [ Links ]
Greene, R. R. 2008. Ecological perspective: An eclectic theoretical framework for social work Practice. In: Greene, R. R. (ed.). Human behaviour: Theory and social work practice. New Brunswick: Transaction Publishers. [ Links ]
Healy, K. 2014. Social work theories in context: Creating frameworks for practice. 2nd ed. London: Palgrave-Macmillan. [ Links ]
Homberger, S. & Smith, S. L. 2011. Family involvement in adolescent substance abuse treatment and recovery: What do we know? What lies ahead? Children and Youth Services Review, 33(1): 70-76. [ Links ]
Isobell, D., Kamaloodien, K. & Savahl, S. 2015. A qualitative study of referring agents' perceptions of access barriers to inpatient substance abuse treatment centres in the Western Cape. Harm Reduction Journal, 12(36): 1-14. [ Links ]
Jhanjee, S. 2014. Evidence based psychosocial interventions in substance use. Indian Journal of Psychological Medicine, 36(2): 112-118. [ Links ]
Keen, H, Sathiparsad, R. & Taylor, M. 2015. Prevalence of multiple addictions and current treatment by drug treatment centres in Durban, South Africa. Social Work/Maatskaplike Werk, 51(2): 244-261. [ Links ]
Kuper, L. E., Gallop, R. & Greenfield, S. F. 2010. Changes in coping moderate substance abuse outcomes differentially across behavioural treatment modality. The American Journal on Addictions, 19(6): 543-549. [ Links ]
Lewis, J. A., Dana, R. Q. & Blevins, G. A. 2015. Substance abuse counselling. Stamford, Connecticut: Cengage Learning. [ Links ]
Liebenberg, J., du Toit-Prinsloo, L., Steenkamp, V. & Saayman, G. 2016. Fatalities involving illicit drug use in Pretoria, the capital of South Africa, for the period 2003-2012. South African medical Journal, 106(10): 1051-1055. [ Links ]
Mahlangu, S. H. 2016. The aftercare needs of Nyaope users in the Hammanskraal community. Pretoria: University of Pretoria. Master's Thesis. [ Links ]
Makhubele, J. C. 2013. Concoction of harmful substances in homemade alcoholic beverages in rural areas of Mopani District in Limpopo Province-RSA: Implications for social work practice. Journal of Evidence-based Social Work, 10: 435-446. [ Links ]
Manuel, J. I., Yuan, Y, Herman, B. D., Svikis, D. S., Nichols, O.,Palmer, E. & Deren, S. 2016. Barriers and facilitators to successful transition from long-term residential substance abuse treatment. Journal of Substance Abuse Treatment, 74: 16-22. [ Links ]
Marlatt, G. A. & Donovan, D. M. 2005. Relapse prevention: Maintenance strategies in the treatment of addictive behaviours. New York: Guilford Press. [ Links ]
McCann, T. V., Lubman, D. I., Boardman, G. & Flood, M. 2017. Affected family members' experience of, and coping with, aggression and violence within the context of problematic substance use: A qualitative study. Bio Med Central Psychiatry, 17: 209-220. [ Links ]
Meade, C. S., Towe, S. L., Watt, M. H, Lion, R. R, Myres, B., Skinner, D., Kimani, S. & Pieterse, D. 2015. Addiction and treatment experiences among active methamphetamine users recruited from a township community in Cape Town, South Africa: A mixed-methods study. Drug and Alcohol Dependence, 152: 79-86. [ Links ]
Menon, J. & Kandasamy, A. 2018. Relapse prevention. Indian Journal of Psychiatry, 60(4): 473-478. [ Links ]
Moeeni, M., Razaghi, E. M., Ponnet, K., Torabi, F., Shafiee, S. A. & Pashaei, T. 2016. Predictors of time to relapse in amphetamine-type substance users in the matrix treatment program in Iran: A Cox proportional hazard model application. BMC Psychiatry, 16: 265. [ Links ]
Mokwena, K. & Morojele, N. 2014. Unemployment and unfavourable social environment as contributory factors to Nyaope use in three provinces of South Africa: Substance abuse. African Journal for Physical, Health Education, Recreation and Dance, 20(1-2): 374-384. [ Links ]
Mudavanhu, N. & Schenck, R. 2014. Substance abuse among the youth in Grabouw Western Cape: Voices for the community. Social Work/Maatskaplike Werk, 50(3): 370-392. [ Links ]
Mutlu, C, Demirci, A. C, Yalcin, O., Kilicoglu, A. G., Topai, M. & Karacetin, G. 2016. One-year follow-up of heroin-dependent adolescents treated with Buprenorphine/Naloxone for the first time in a substance treatment unit Journal of Substance Abuse Treatment, 67: 1-8. [ Links ]
Myers, B., Govender, R., Koch, J. R. Manderscheid, R. Johnson, K. & Parry, C. D. H. 2015. Development and psychometric validation of a novel patient survey to assess perceived quality of substance abuse treatment in South Africa. Substance Abuse Treatment, Prevention, and Policy, 10(44): 1-15. [ Links ]
Myers, B., Williams, P. P., Govender, R., Manderscheid, R. & Koch, J. R. 2018. Substance abuse treatment engagement, completion and short-term outcomes in the Western Cape province, South Africa: Findings from the Service Quality Measures Initiative. Drug and Alcohol Dependence, 185: 278-284. [ Links ]
Njoroge, M. W. 2018. Review on treatment of substance use disorders. Journal of addiction research and therapy, 9(1): 1-8. [ Links ]
Nyege, S. B., Dike, F. M., Nkamare, M. B., Robinson-Bassey, G. C. & Wokne-Eze, L. 2017. Factors influencing relapse among substance abuse patients attending neuropsychiatrie hospital: Rumuigbo Port Harcourt, Nigeria. International Journal of Development Research, 7(11): 16984-16989. [ Links ]
Paat, Y. F. 2013. Working with immigrant children and their families: An application of Bronfenbrenner's Ecological Systems Theory. Journal of Human Behavior in the Social Environment, 23(8): 954-966. [ Links ]
Panebianco, D., Gallupe, O.,Carrington, P. J., & Colozzi, I. 2016. Personal support networks, social capital and risk of relapse among individuals treated for substance use issues. The International Journal of Drug Policy, 27: 146-153. [ Links ]
Perkinson, R. R. 2004. Treating alcoholism: Helping your clients find the road to recovery. New Jersey: John Wiley & Sons. [ Links ]
Ramlagan, S., Peltzer, K. & Matseke, G. 2010. Epidemiology of drug abuse treatment in South Africa. South African Journal of Psychiatry, 16(2): 40-49. [ Links ]
Schultz, P. & Alpaslan, A. H. 2020. Playing the second fiddle - the experiences, challenges and coping strategies of concerned significant others of partners with a substance use disorder: Informing social work interventions. Social Work/Maatskaplike Werk, 56(4): 430446. [ Links ]
Schurink, W. J., Roestenburg, W. J. H & Fouché, C. B. 2021. The place of literature and theory in research. In: Fouché, C. B., Strydom, H. & Roestenburg, W. J. H. (eds). Research at grass roots for the social sciences and human service professions. 4th ed. Pretoria: Van Schaik Publishers. [ Links ]
Setlalentoa, M., Ryke, E. & Strydom, H. 2015. Intervention strategies used to address alcohol abuse in the North West Province, South Africa. Social Work/Maatskaplike Werk, 51(1): 80-100. [ Links ]
Sorsdahl, K., Stein, D. J., Myers, B. 2012. Negative attributions towards people with substance use disorders in South Africa: Variation across substances and by gender. BMC Psychiatry, 12(101): 1-8. [ Links ]
South African Community Epidemiology Network on Drug Use (SACENDU). 2017. Research brief Monitoring Alcohol, Tobacco and other drug use trends in South Africa. July 1996-June 2017,20(2): 1-27. [Online] Available: https://www.samrc.ac.za/sites/default/files/attachments/2018-03-14/SACENDUbriefDec2017.pdf [Accessed 2018/10/05]. [ Links ]
South African Community Epidemiology Network on Drug Use (SACENDU). 2022. Research update: Monitoring Alcohol, Tobacco and other drug use trends (South Africa). January-June 2021. [Online] Available: https://www.westerncape.gov.za/sites/www.westerncape.gov.za/files/sacendu_research_update_phase_50.pdf. [Accessed 21 July 2022]. [ Links ]
Stokes, M., Schultz, P. & Alpaslan, A. 2018. Narrating the journey of sustained recovery from substance use disorder. Substance Abuse Treatment, Prevention, and Policy,13(35) [Online] Available: Https://Doi.Org/10.1186/S13011-018-0167-0. [Accessed: 21 July 2022]. [ Links ]
Strydom, H. 2021. Sampling techniques and pilot studies in qualitative research. In: Fouché, C. B., Strydom, H. & Roestenburg, W. J. H. (eds). Research at grass roots for the social sciences and human service professions. 4th ed. Pretoria: Van Schaik Publishers. [ Links ]
Swanepoel, I. 2014. The causes of relapse amongst young African adults following inpatient treatment for drug abuse in the Gauteng Province. Pretoria: University of Pretoria. Master's Thesis. [ Links ]
Swanepoel, I., Geyer, S. & Crafford, G. 2016. The causes of relapse amongst young African adults following in-patient treatment for drug abuse in the Gauteng Province. Social Work/Maatskaplike Werk, 52(3): 414-438. [ Links ]
Temmingh, H. & Myers, B. 2012. Clinical treatment of substance use disorders in South Africa. In: Ellis, G. F. R., Stein, D. J. & Meintjies, E. M. (eds.). Substances use and abuse in South Africa. Cape Town: UCT Press. [ Links ]
United Nations Office on Drugs and Crime (UNODC). 2014. World Drug Report 2014. Vienna: United Nations Publications. [ Links ]
United Nations Office on Drugs and Crime (UNODC). 2017. World Drug Report 2017. Vienna: United Nations Publications. [ Links ]
Van der Westhuizen, M., Alpaslan, A. & de Jager, M. 2011. Preventing relapses amongst chemically addicted adolescents: Exploring the state of current services. Social Work/Maatskaplike Werk, 47(3): 350-370. [ Links ]
Van Wyk, C. 2011. The burden of disease: Substance abuse in South Africa: Patients as partners. African Journal of Psychiatry, 14(1): 80-84. [ Links ]
Voskuil, R. 2015. Identifying relapse indicators in a state subsidised substance abuse treatment facility in Cape Town, South Africa. Cape Town: University of the Western Cape. Master's Thesis. [ Links ]
Witkiewitz, K. A. & Marlatt, G. A. 2011. Overview of relapse prevention. In: Witkiewitz, K. A. & Marlatt, G. A. (eds). Therapist's guide to evidence-based relapse prevention. New York: Elsevier. [ Links ]
Article accepted: 28 February 2023


{kind=link}