










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.58 n.3 Stellenbosch 2022
http://dx.doi.org/10.15270/58-3-1061
ARTICLES
The perceptions and experiences of families dealing with substance use disorders: implications for holistic employee wellness programmes
Eldene BraafI; Nicolette RomanII; Hamilton PharaohIII
ISocial Worker (Employee Wellness Programme), Sol Plaatje University, South Africa https://orcid.org/0000-0002-1810-5965; eldene.braaf@spu.ac.za
IICentre for Interdisciplinary Studies of Children, Families and Society, University of the Western Cape, South Africa. https://orcid.org/0000-0002-4506-437X; nroman@uwc.ac.za
IIIDiscipline of Physiotherapy, University of KwaZulu-Natal, South Africa. https://orcid.org/0000-0001-9681-4911; PharaohH@ukzn.ac.za
ABSTRACT
Neglecting the significant role played by family members in the post-rehabilitation trajectory of substance abusers can pose a significant challenge in supporting intervention programmes in the workplace. This paper reports on a small-scale qualitative investigation that used focus group interviews with family members to explore their perceptions and experiences of being confronted with family members with substance use disorders. The findings are presented through three themes: 1) emotional burden; 2) coping and avoidance strategies; and 3) support needs of family members. Recommendations highlight how employee assistance programmes can provide a comprehensive suite of holistic support systems.
Keywords: bio-ecological systems theory, concerned significant others, employee assistance programmes, occupational social work, substance use disorder.
INTRODUCTION
The negative and detrimental effects of substance abuse on the family unit are well acknowledged in the literature. Copello, Velleman and Templeton (2005) describe a solid evidence base for the negative impacts of substance abuse on the family, especially among parents, spouses and children. In support of these findings, McCann, Lubman, Boardman and Flood (2017) similarly reported on high rates of family aggression and violence within the context of substance abuse. While research into the impact of substance abuse on the family is well documented (Schultz & Alpaslan, 2016), apart from for a few studies, there is limited insight into the perspectives of affected family members supporting a member with a substance use disorder (SUD). Stokes, Schultz and Alpaslan (2018:2) define substance use disorder as the "physical, mental and emotional compulsion to use mind- and mood-altering substances (drugs and alcohol)."
Schultz and Alpaslan (2020:430) capture these all-encompassing consequences when they state that "a family member's substance use disorder affects the social, psychological, physical, financial functioning and wellbeing of the family system, often putting them at risk of family violence". Mafa and Makhubele (2019) assert that substance abuse addiction and its consequences reach beyond the individual addict, negatively affecting families and the functioning of the family unit. Similarly, McCann et al. (2017) argue that it is not necessarily the frequency of substance use that is the primary problem, but the adverse consequences it has in the user's life and that of other family members. This might include the consequent social, financial, psychological, physical and legal problems the substance abusers or their family might have to face. Denning (2010) concurs with this assessment and notes how having to deal with a family member's alcohol and drug abuse can be an unbearable experience. Perkinson (2008) explains that to be in a relationship with a partner with an SUD is to find oneself in an environment that is sporadically and at times even extremely out of control. Residing in an addictive home is compared to living in a whirlwind. Additionally, concerned significant others (CSOs) frequently experience profound helplessness, frustration, anger and fear (Denning, 2010). While the impact of substance abuse on an individual certainly requires intervention, the effects on the family of the substance abuser are equally serious and have especially long-lasting emotional consequences.
There is a growing body of literature that has highlighted how therapeutic interventions and support associated with SUDs tend to focus primarily on the substance abuser or the recovering addict (Hudson, Kirby, Clements, Benishek & Nick, 2014). The needs of the family or CSO are thus frequently neglected (Schultz & Alpaslan, 2020). This is a view supported by Copello et al. (2005), who assert that little attention is given to families in national and international alcohol-related policies. Furthermore, there is little mention of family involvement in interventions, either as part of successful treatment for those with alcohol abuse problems or as concerned individuals who need support. Scholars and those working in the substance abuse disorder field as addiction specialists agree that alcohol and drug problems affect not only those using the substances, but also the family members of the substance user and can extend to friends and work colleagues (Copello et al., 2005; McCann et al., 2017). As a result, it is often the CSOs, who might be intimate partners, parents, siblings, offspring, other relatives or close friends, who feel the effects of the substance abuser's behaviour or have to shoulder the responsibility of supporting and advocating for the person with an SUD. Furthermore, the CSO also has to manage issues of stigma and social isolation, and respond to and cope with the negative consequences such as family arguments, relationship breakdowns, abuse, aggression and violence (McCann et al., 2017). Commenting on how the impact of substance abuse affects not only the individual with an SUD, Hussaarts, Roozen Meyers, van de Wetering and McCrady (2012) estimate that approximately five individuals suffer the direct consequences of the behaviour of one substance abuser. The adverse effects on family members often encompass multiple problems in different life areas, including economic, psychological, familial and intimate relationships. The needs of CSOs have not received the attention they deserve. CSOs are additionally affected as they face a long-lasting increase in responsibilities when living with an addict (Hussaarts et al., 2012).
Neglecting the significant role played by family members and CSOs in the post-rehabilitation trajectory of substance abusers can pose a significant challenge to support intervention programmes in the workplace. Research that relies on the bio-ecological systems theory (see, for example, Schultz & Alpaslan, 2020) has been particularly useful in helping to provide a holistic account by acknowledging how the individual and their behaviour are influenced by factors in the adjacent ecosystems. From this perspective, the roots of SUDs can be investigated systematically and their causes located in intrapersonal, interpersonal and environmental factors uncovered. The bio-ecological systems theory is also able to compellingly show how substance addiction affects not only the addict but those around them such as CSOs as well as indicate the continued influence on other microsystems and meso levels. Schultz and Alpaslan (2020) argue that through the exploration of the experiences, challenges and coping strategies adopted by CSOs living with partners with SUDs, attention can be drawn to the multisystem involvement of the extended family system, the neighbourhood and other critical social systems. Also displayed are the interventions required to facilitate the enhancement of the social functioning of CSOs and their partners or family members with SUDs (Schultz and Alpaslan, 2020).
Lander, Howsare and Byrne (2013) argue that the effects of SUDs are felt by the whole family. Additionally, the family context holds information about how SUDs develop and are maintained, and what can positively or negatively influence the treatment of the disorder (Lander et al., 2013). Bronfenbrenner (2005) explains that human behaviour is best studied from a personal and individual perspective, within human social contexts. The bio-ecological systems theory also relates to a fundamental principle of human development, namely that the individual is at the centre of five major environmental contexts, structured as a network of systems. These systems are referred to as the micro-, meso-, exo-, macro- and chronosystems (Bronfenbrenner, 2005). Rich (2017) describes the bio-ecological systems theory as being best suited to examine the phenomenon of drug use as it views human development from a personin-environment context. The bio-ecological systems theory, therefore, offers a productive lens for seeking to understand the impact of SUDs on families and devise suitable support interventions (Rich, 2017).
This paper aims to report on the perceptions and experiences of families dealing with SUDs with the intention of assisting the work employee assistance programmes. The work of occupational social workers involved in supporting post-rehabilitation substance abusers can benefit from a holistic understanding of the interrelationship between the individual, their family and CSOs.
Employee assistance programmes and occupational social work deal with work-related, personal, interpersonal and productivity issues. They also address a range of concerns, including substance abuse, stress, trauma, financial difficulties, conflict, absenteeism, employee development and bereavement (Terblanche, Gunya, Maruma, Mbuyisa, Maseko, Mojapelo, Pretorius & Tyson, 2021). Terblanche et al. (2021) distinguish between an employee assistance programme and occupational social work. These two support mechanisms available within the context of workplaces in South Africa assist in offering distinct guidelines for employers when seeking services, on the one hand, to support the psychosocial functioning and productivity of employees, and on the other, to support the successful operations of the workplace at large (Terblanche et al., 2021).
The influence of the family and CSOs in understanding SUDs and the vital role they can play in the holistic treatment and support of, especially, employees who have returned to work after a period of rehabilitation is readily acknowledged (Denning, 2016; Terblanche et al., 2021). What is less clear is the extent to which employee support initiatives for employees with an SUD can reasonably involve family members and CSOs in these support strategies. The specific therapeutic and resource mechanisms that might underpin a holistic employee invention are not fully understood. Research in the broader field of occupational social work has not fully investigated the experiences and perceptions of CSOs when confronted with the consequences of a family member's SUD and how such understanding might be integrated into more holistic workplace substance abuse support interventions.
This paper reports on an exploratory investigation that used a qualitative research approach to explore the experiences of CSOs of substance abusing family members. By placing a specific focus on the experiences, coping strategies and concerns of CSOs, the research aimed to advance current understandings of the interrelationship between the individual and CSOs and the implications for substance abuse intervention programmes in the workplace.
THEORETICAL FRAMEWORK
The theoretical framework for this study draws on Bronfenbrenner's (2005) bio-ecological systems theory to account for the conceptualisation and explanation of human behaviour as a complex process, with the individual seen as essentially a product of their immediate and wider social context. The theory is regarded as useful when attempting to understand the complex interactions associated with human development and how the individual is impacted by the social environments they encounter and interact with (Jaeger, 2016; Tudge, Payir, Mercon-Vargas, Cao, Liang, Li & O'Brien, 2016). Vélez-Agosto, Soto-Crespo, Vizcarrondo-Oppenheimer, Vega-Molina and García Coll (2017) claim that the bio-ecological systems theory is one of the most widely known theories of human development. The theory has been used in various fields of study, including literacy studies (Jaeger, 2016) and psychological studies and culture (Vélez-Agosto et al., 2017). Bio-ecological systems theory has been taken up in social work practice and is fruitful in helping to explore and attend to some of the major concerns defining the field. The works of Swick and Williams (2006) and Rudd, Neuendorf, Atkin, Romano, Gross and Ray (2019) are two insightful examples. These studies explored the impact of homelessness, violence and chemical dependency on the family system and parent-child relationships in the context of imprisonment. In the study reported here, this theory forms the theoretical framework that assists in the exploration of the perceptions and experiences of CSOs with their family member's SUD.
The bio-ecological systems theory offers insight into the central processes aligned to life-span development (Darling, 2007). A central idea is that the conceptualisation of human development is intricately patterned by multiple levels of influence from social systems that operate simultaneously and progressively over time (Jaeger, 2016). Schultz and Alpaslan (2020:432) emphasise that the theory locates "the individual in relation to other ecosystems". As mentioned above, the ecological systems model includes five distinct systems: the microsystem, mesosystem, exosystem, macrosystem and chronosystem (Rich, 2017). According to Rich (2017), these interrelated systems describe the influence of environmental factors on human behaviour. Therefore, the varying rules, conventions, and practices, which define and structure the different systems, determine the psychological and behavioural development of an individual. The model has generative explanatory power in that it can account for how an individual's development and behaviour are a composite of the interplay between internal, biological, socio-cultural and wider environmental factors (Kail and Cavanaugh, 2010). As Rich (2017:20) notes, theoretically it can conceptualise human development "from a person-in-environment context". Moreover, growth and development are regarded as taking place within the context of relationships. Rich (2017) argues, an individual's biological disposition and the quality and context of their environmental forces come together to shape their development. Factors such as culture, power, interpersonal relationships, group value systems and social norms are regarded as central elements that can facilitate and aid in understanding how the lives of individuals, families and societies are interdependently linked.
The value of employing the bio-ecological systems theory to examine SUDs and the consequences for individual substance abusers and their immediate families and CSOs is well documented (Rich, 2017; Schultz & Alpaslan, 2020). Schultz and Alpaslan (2020: 432) argue that a holistic framework able to capture "the experiences, challenges and coping strategies of CSOs living with partners with SUD" clearly shows how multiple factors and systems are involved, including "the extended family system, the neighbourhood, and other critical social systems".
RESEARCH APPROACH AND DESIGN
This study utilised a qualitative research approach to explore the perceptions and experiences of concerned significant others when confronted with family members with substance abuse disease. Drawing on phenomenological research traditions, the study attempted to give primacy to the experiences of CSOs and understand their lived, everyday realities (Braun & Clark, 2006). This is particularly evident in the main research question that informed the study, namely: "What are the experiences of concerned significant others who have a family member with a SUD?"
Participants and sampling
Given the nature of the phenomenon being investigated and the geographic location of the study, a combination of convenience (Maree & Pietersen, 2016) and purposive sampling was employed (Abrams, 2010; Reybold, Lammert & Stribling, 2012). Additionally, CSOs of those with an SUD could reasonably constitute what Abrams (2010:541) refers to as "hard to reach" populations, who are of particular interest to social work researchers. Typically, such populations are recruited through agencies and rely on a combination of sampling strategies (Abrams, 2010). A local non-profit organisation specialising in out-patient treatment and support for substance abusers in central Kimberley, South Africa, was approached. It was the only registered intensive outpatient treatment centre of its kind in the broader Kimberley area. As part of the various services it offers, the centre also runs a formal support group for CSOs of substance abusers. These factors meant the centre represented a relatively accessible research site. The manager of the centre was approached and informed about the aims of the research study with a view to seeking access to the existing support group. As the family support group held at the centre had regular meetings, it was recommended that the researcher select this group. This ensured that data would be collected in a natural setting, while being minimally disruptive as well as unobtrusive to those attending the sessions (Abrams, 2010). Furthermore, Abrams (2010) describes purposive sampling as a strategy that relies primarily on the researcher's judgment about which participants would be best suited to provide insights and contribute to the phenomena under investigation. These respondents are then invited to participate in the study. The support group, which had been in existence for more than a decade, was typically attended by parents, partners and siblings of substance abusers. On average the family support group, which the centre hosts once a month, is attended by 15 group members. Many attend regularly and have done so over several years, but the group itself can be characterised by its transient nature (Abrams, 2010). On the day when the focus group interviews took place, the group consisted of nine participants - six females and three males, who mostly identified as being parents. The participants resided in a range of residential areas in the city, and this can be seen as indicative of their varying socioeconomic status, suggesting that they were representative of a cross-section of communities in the Kimberley area. Table 1 presents an overview of the profiles of the participants.
Data collection and analysis
The study used a focus group as the main data-collection tool. Focus groups are described as "small structured groups" (Litosseliti, 2003:1) that consist of selected participants who together discuss or explore a specific topic, usually under the guidance of a facilitator or moderator (Robinson, 1999). In this way, focus groups allow for individual views and experiences to be expressed through group interaction. Typically, group "participants share and respond to comments, ideas, and perceptions" (Litosseliti, 2003:1). Robinson (1999) further notes that focus groups help explore underlying assumptions that inform particular perceptions and views about a specific topic or phenomenon, i.e. in the case of this study the way that CSOs experienced their family members' substance abuse behaviours and their consequences. Attempting to harness a key advantage of focus groups as a method, which Robinson (1999) argues allows for the collection of data in a natural setting, the researcher joined one of the support group meetings and acted as the facilitator for that session. In keeping with the naturalistic approach, a few general and open-ended prompt questions were prepared in advance, for example, "What is it like to be a family member of a substance abuser?" and "What does it feel like?" However, the direction of the discussion was allowed to develop holistically. The facilitator merely offered short statements to clarify points made or sentiments expressed, while also attempting to encourage group members to contribute to the discussion. A digital recording of the focus groups was made and a verbatim transcript was prepared. As group members often spoke in Afrikaans, these segments were translated as part of the transcription process.
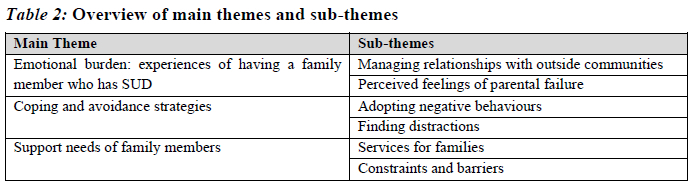
Thematic analysis of the data was undertaken, guided by the approaches outlined by Braun and Clark (2006) and Creswell (2014). Braun and Clark (2006:78) observe that "thematic analysis provides a flexible and useful research tool which can potentially provide a rich and detailed, yet complex, account of the data". Aside from being widely employed within qualitative methodological traditions, because the thematic analysis is not aligned to any theoretical framework, it represents a versatile analytical tool (Braun & Clark, 2006). Initial codes were developed through a combination of the emerging information and insights provided by the focus group participants and predetermined codes informed by the theoretical framework (Creswell, 2014). These included negative experiences and feelings towards the substance abuser, relationships between family members, coping mechanisms, community involvement, and the needs of and support for CSOs. Preliminary broad patterns were identified across the initial codes before three distinct themes (and six supporting sub-themes), that revealed a clear connection to the primary research question, were identified (Braun & Clark, 2006). These themes are: 1) emotional burden: experiences of having a family member who has SUD; 2) coping and avoidance strategies; and 3) support needs of family members. An outline of the themes and sub-themes is presented in Table 2.
Trustworthiness
Lincoln and Guba (1998) maintain that trustworthiness in qualitative enquiries assists in ensuring that the findings are regarded as valid and worth paying attention to. Accordingly, they note that data trustworthiness has four major components: credibility, transferability, dependability and conformability (Lincoln & Guba, 1998). These measures were implemented to increase the trustworthiness of the findings. Member or stakeholder checking was also used to check for consistency of interpretations. An independent coder was used to independently code data to ensure higher inter- and intra-coder reliability (Creswell, 2014).
Ethical considerations
The main ethical considerations for this study involved the need to ensure participant confidentiality and privacy (Babbie, 2017; Creswell, 2014). Given the sensitive nature of the topic and the characterisation of participants as "hard to reach" (Abrams, 2010), access to the research site was negotiated with care (Creswell, 2014). Informed consent was sought from the key gatekeeper at the centre and from the focus group participants, who were assured that their participation was voluntary and that they could freely withdraw from the study at any stage. Ethical clearance was obtained from a Humanities and Social Sciences Research Ethics Committee (Ref No: 130416-047).
FINDINGS
Three broad themes emerged from the data analysis with a further set of corresponding sub-themes. These are presented in Table 2.
Theme 1: Emotional burden: experiences of having a family member who has SUD
Most participants described their experiences of having a family member with a SUD in negative terms. They described the emotional and psychological burden they experience and used terms such as 'traumatised', 'upset', 'deep depression', 'humiliation', 'embarrassment', 'failure' and 'anger' to articulate the detrimental impact on their psychological wellbeing.
Ifeel in my personal opinion that you as parents and as a family are more traumatized than the person using substances because they are in another world, they don't realise the impact and the damage that they caused the family... because you have to endure the embarrassment and the humiliation... And it feels like a misfortune and sometimes a person can go into a deep depression. (Participant 4)
You feel upset because the children do you a great injustice. (Participant 9)
These experiences of participants confirm the detrimental effects that SUDs can have on the family unit and CSOs established by scholars such as Copello et al. (2005), Denning (2010), and more recently Schultz and Alpaslan (2016, 2020). Many of these negative emotional reactions shared by the participants appear to be commonly reported in other studies and seem to especially reflect the experiences of parents with adolescents battling SUDs (for example, Hlungwani, Ntshingila, Poggenpoel & Myburg, 2018; Mafa & Makhubele, 2019). The burden shared by parents when their offspring have an SUD which disrupts the functioning of the family unit is consistent with the structural functionalist position which posits that the family is fulfilling a key socialisation function (Hudson, 1978; Barker & Hunt, 2004). When the SUD of a family member causes the level of 'damage' the participants allude to above, the notion of the family as being a fundamentally positive and beneficial institution (Hudson, 1978) is then undermined.
Managing relationships with outside communities
The negative effects of their family member's SUD extended beyond the confines of the immediate family unit and started to have negative consequences on how families interacted with their neighbours and the wider community. In response to developing feelings of self-doubt and negative self-worth, family members frequently removed themselves from their wider community structures. The perceived sense of shame or 'scandal' brought upon them as a result of the drug abuser's behaviours led to their isolation and even confinement to the family home.
You tend to develop anger towards that person also, you understand and you begin to doubt yourself, doubt yourself as a parent, as a person in the community because your self-worth, your self-worth has been broken down by another person you tend to distance yourself from other people and because of that you don't want to talk to other people, we don't reach out to other people because you feel that this thing, it is 'n skande [source of shame/scandal]. (Participant 7)
You face the problem at home as well as work and it's difficult to talk, not speak up ... because Kimberley is such a small place, so everyone sort of knows everyone's business you know... so it's actually a very difficult situation so I then withdrew myselffrom the community as well as from my family and so I'm just there at home. (Participant 3)
Thing is now, you as a person go into isolation; I mean you don't go to family; you don't go to friends, you have no friends anymore. You are just at home because you are ashamed because you don't know what the people know and people talk, they gossip if I may put it bluntly and you know that you are the topic of discussion. (Participant 4)
The experiences and observations of the participants are consistent with points made in the literature which suggest that frequently CSOs shoulder immense burdens, stigma and shame associated with the consequences of the family member's SUD (McCann et al., 2017; Schultz & Alpaslan, 2020). The findings further echo those of studies conducted by Mafa and Makhubele (2019), and Schultz and Alpaslan (2020), which both report on how CSOs frequently withdrew and isolated themselves from the extended family, as well as from their external social life and activities outside the immediate family unit. Participants in the phenomenological study by Hlungwani et al. (2018), which attempted to explain how parents experienced their adolescents' substance abuse behaviours, also reported elevated levels of humiliation and shame because of their offspring's addiction.
Also evident is how the disruption caused within the individual family unit starts to affect the way that CSOs function in other spheres of life. In an earlier study, which focused on the way in which sibling relationships were negatively impacted by SUD, Schultz and Alpaslan (2016:90) note that "the family as a system becomes involved in a process of physical and emotional detachment, and individual members become socially distant from each other." This resonates strongly with the bio-ecological model, which suggests that behavioural and psychological actions and functions are influenced by multiple individuals, as well as biological and socio-environmental factors (Kail & Cavanaugh, 2010).
Perceived feelings ofparental failure
Parents were particularly affected by their offspring's SUD. Frequently they attributed substance abuse behaviours and lifestyles to their failures as parents. They also expressed feelings of hopelessness, disillusionment and disappointment in response to the actions of their children.
It's not a nice feeling because you remember the child that you raised and you remember the type of child with the mannerisms, his attitude, the principles and the values that you instilled in that child you see, and you watch those principles and those values, you watch, you watch them change into something that you yourself don't even recognise any more. (Participant 7)
...makes you as a parent feel, you know, you are a failure cause sometimes you will ask yourself, where did I go wrong?... it's really very heart-breaking if your child is involved in those kind of things and it breaks you as a person and people don't even know, yes it really feels like a failure. (Participant 2)
The findings provide some support for the conceptual premise of the role and function of parents in the family unit. The strong negative reactions and experiences of parental failure expressed by participants can in part be explained by their understanding of the primary socialisation function they serve in the family unit. An offspring's SUD is thus seen as an inability on the part of the parents to inculcate the appropriate values, norms and behaviour, and their inadequacy to ensure the induction of the child into suitable adult roles and behaviour (Barker & Hunt, 2004; Hudson, 1978). The perceptions of parents in particular suggest, as Lander et al. (2013) observe, that SUDs represent a moral failing, and as such the emotional consequences for the parent are experienced in more profound and sensitive ways. Such feelings of guilt, shame, and hopelessness in the face of an offspring's SUDs were also reported by Hlungwani et al. (2018), thus suggesting this is a fairly common response experienced by CSOs. These insights about the extent of the guilt parents of offspring with SUD experience may help to understand the ways that they deny themselves and their own needs.
Theme 2: Coping and avoidance strategies
Family members employed various strategies that enabled them to manage and cope with the negative impact that the SUDs had on their lives. These strategies included resorting to behaviours identified as psychologically negative, relying on distractions such as taking on additional work, or using medicinal interventions. Participants also reported engaging in more supportive strategies such as seeking spiritual comfort. Balmores-Paulino (2018) notes that the term 'avoidance coping' describes a type of coping strategy that allows an individual to deal with various life stressors. Unlike other forms of coping mechanisms, avoidance coping is characterised by attempts by the individual not to address the problem or stressor they are confronted with, but rather they engage in behaviours that help relieve their distress. The individual is thus able to live or cope with the difficult situation they are encountering (Balmores-Paulino, 2018). Avoidance coping is therefore an appropriate way of referring to the strategies family members employ to deal with the negative consequences of SUDs in their families.
Adopting negative behaviours
Participants identified and described several reactive behaviours in response to their family member's substance abuse. Feelings of frustration, sadness and hurt often resulted in expressions of anger, frequently directed at others such as co-workers, a spouse and members of their immediate family like their children or a daughter-in-law. While participants showed self-awareness about these reactive behaviours, they appeared less able to mediate or adjust their behaviours in more appropriate ways. Extreme negative responses were also mentioned, including the possibility of resorting to substance abuse themselves or suicidal thoughts.
And you feel that you are totally worthless, some of us might even resort to using an other substance to give us that assurance, because people use it as something to say, no this thing will make me feel like a good person, if I must take myself, I'm not using... but it will come to a place where I will now start drinking heavily. (Participant 7)
The battle that we are fighting within us not to go to that extent is a very hard battle because there are some of us that are thinking, there came times when we were thinking that we want to kill ourselves, that our death will better that child's life if I just die, maybe this child will see that because of what he did, he lost me because of what he did, maybe he will pull his life right. (Participant 2)
I don't have to be cross at my son, sometimes I go to work and I will lash out at somebody else. Maybe me and my wife, instead of me comforting my wife, I would lash out at my wife, I would even do that to my daughter-in-law when my son does something wrong. (Participant 1)
I forget about the other siblings in the house and sometimes they feel neglected, they can also go through a worse period because they doing good, I'm doing good but julle focus net op hulle, op hom of haar. Wat van my?[you just give all your attention to them (i.e. the substance abuser). What about me?]. You understand, so we neglect sometimes the other siblings now because of this problem, this problem is not just there, but basically attacking the whole family. (Participant 5)
Confirming the results of the study by Copello et al. (2005:370), the findings here point to how SUDs can negatively alter "a range of family systems and processes, including family rituals, roles within the family, family routines, communication structures and systems, family social life and family finances". Mafa and Makhubele (2019) report that a common emotional reaction of parents in response to their offspring's substance abuse behaviour was to strike out in anger towards other members of the family. They further suggest that such anger "could be compounded by the blame that parents put on themselves and everyone close to them" (Mafa & Makhubele, 2019: 14120). Also confirming the findings of Copello et al. (2005) are the indications of the manifestation of psycho-clinical and psychological symptoms by participants in this study. The same applies to the symptoms identified by Denning (2010) such as the lack of self-care on the part of CSOs and enabling the substance abuser.
Finding other distractions
A common coping strategy reported by many of the participants was finding other distractions to divert attention away from the problems caused by the substance abuse behaviours of their family members. Often keeping busy, especially devoting extra time to work, was a mechanism they adopted. Mention was also made of relying on medicinal interventions to control insomnia, anxiety and depressive thoughts.
How I cope is, I try to keep busy. I constantly work so I don't have to think because as soon as I sit still then it overwhelms me like an ice-cold bucket of water over me. So I try to stay busy... I work and if I don't work then I sleep and then calming tablets or depression tablets keep me going. As soon as I don't take tablets then my tears just start flowing uncontrollably. I can't handle myself. So it's constantly keeping busy, calming tablets, depression tablets or sleep. (Participant 4)
I don't want to go home because I know if I go home, I know what I must go face so I'd rather work right through and come late home when everyone is asleep and then sleep. In the morning I get up early and go (back to work). (Participant 3)
These experiences are consistent with the insights in McCann et al. (2017), who note how CSOs often attempt to disengage from the person with the SUD. When this person is living in the family home, withdrawal or avoidance of the home can still occur. Similar findings were also reported by Schultz and Alpaslan (2016:104), who noted that many of their participants used "avoidance as a behavioural coping strategy". In similar ways, as reported here, such disengagement took the form of physical distancing, withdrawal of communication, and in more extreme instances leaving the family home (McCann et al., 2017). Similarly, the Schultz and Alpaslan (2020) study also reports the use of coping strategies used by CSOs that attempted to avoid engagement with family members with SUDs. Papalia, Olds and Feldman (2007) suggest that such coping strategies as observed by participants above might be an attempt to maintain the peace in the home, but may in effect act to enable the addictive behaviour. Devoting more time to work was also a strategy reported by Papalia et al. (2007). In both the Hlungwani et al. (2018) and Mafa and Makhubele (2019) studies, parents reported how their offspring's SUD caused specific mental health problems and forced them to either seek medical advice or rely on mediation. These behaviours could all be classified as avoidance coping strategies that not only allow family members to cope with the immensely difficult and physical or emotionally charged family environment, but might also act as protective strategies on their part to avoid potential aggression, violence, or further stress.
Theme 3: Support needs of family members
Participants identified the need for specific support that addressed their experiences of having a family member with SUD. Areas of support regarded as particularly beneficial were primarily individual and group-based counselling therapies. The inclusion of mentorship-type services that could include house visits and sponsorship-like support were also recommended. Participants acknowledged distinct challenges they faced because of their geographic location in the Northern Cape, one of the less populous regions of South Africa. This meant they were unable to access an extensive range of support services.
Services for families
Most participants were able to describe the benefits they derived from the support group services they currently used. Participation in these group-based counselling inventions was attributed to providing members with the necessary skills, enhancing their understanding of SUDs, and increasing their willingness to become more open about the problems they experience as family members. These interventions also served a dual role of also supporting the person with SUDs in their family. Furthermore, these types of services and interventions allowed certain participants to get relief from the overwhelming burden and responsibility they felt for their offspring's or family members' substance abuse and addiction.
...I must say that also in the centre here, that could assist, that gives me the sense that I've got help. (Participant 3)
So it's helped me to have the support here and also I might becoming aware of the things that I have missed at home, I feel more able to cope...from all of this that in a way I've become aware of where I let the boy go and also aware of where I can pull, I can reign these things back together again. I found comfort of having this centre and having people to speak to about this. (Participant 2)
... get the assistance you need to help the person [substance abuser] stay on the path and that is where we as families can come in and assist our siblings ... understanding what is happening and how we can assist going forward ... where we can see we are not to blame for the disease of addiction. (Participant 8)
The support that I will be looking for is more a setup like this, where I can come and speak. (Participant 7)
...that people do house visits, sometimes a phone call, just to find out what is your state of mind, you see, and also sessions whereby you are having people that can assist you to open up, to talk to your child. (Participant 1)
These group sessions are extremely helpful; it can really help a lot. (Participant 6)
The findings confirm the crucial role of support and timely interventions for all affected by SUDs, while also providing evidence of the lack of direct inventions with families affected by SUDs and their negative consequences (Copello et al., 2005). The findings further support the notion that CSOs and their needs for dealing with the SUD of family members are neglected (Schultz & Alpaslan, 2020). However, these insights suggest the positive impact and efficacy of support interventions aimed at CSOs and family members.
Constraints and barriers
Various constraints and barriers that acted against family members gaining the type of support they needed were also identified by participants. These were often related to the geographical location of Kimberley, which prevented the town from acquiring the level of support in dealing with substance abuse and rehabilitation evident in more populous and urban centres in South Africa. One participant also noted the lack of support from government services and departments, which was again ascribed to Kimberley's scarcity of resources.
There isn't much help available, especially here in Kimberley. One cannot even go to the police. It feels as if your hands are tied because they say they can do nothing, so you feel helpless and more upset. (Participant 8)
You face the problem at home as well as work and it's difficult to talk, not speak up but to talk to a person who has the same problem, they can easily tell you, because Kimberly is such a small place, so everyone sort of knows everyone's business you know. (Participant 2)
A major problem in Kimberley itself, in fact in Northern Cape, there isn't a lot of activities outside that we can do, or what your parents can do, what their kids can do, like today I wanted to take my kids out but my kids are in Kimberley so, that is also another problem faced within Kimberley so if we as a community can get together ... (Participant 8)
Confirming some of the results of the research by Schultz and Alpaslan (2020), the findings here point to clear barriers, such as transport, infrastructure, and finances, which can derail the type of support mechanisms and interventions regarded as beneficial to CSOs. Furthermore, the significance of enlisting support mechanisms across multiple systems when addressing the negative consequences of SUDs is evident from the findings.
CONCLUSIONS AND RECOMMENDATIONS
The paper aimed to report on the perceptions and experiences of families dealing with SUDs and also draws attention to some of the detrimental consequences of SUD on CSOs and other family members. Furthermore, it intended to provide employee assistance programme practitioners and occupational social workers working with employees who have returned from substance abuse rehabilitation with a more holistic and realistic sense of the interrelationship between the individual, their family and the CSO. The study employed bio-ecological system theory as a means of understanding the interrelationship between an individual and other social systems that influence and shape their development and life trajectories. The study confirmed the value of using this theory for investigating SUDs and the consequences of this for individual substance abusers and their immediate families (see, for example Schultz & Alpaslan, 2020). The findings of the study are supportive of existing research as it confirms the negative effects of substance abuse on the family, especially for parents, spouses and children (Copello et al., 2005; McCann et al., 2017).
A particularly salient finding in this study was the lack of support interventions specifically for families and CSOs in the rural areas of the Northern Cape and South Africa in general.
Resources in rural areas are often minimal or non-existent and this hampers the type and quality of support available to CSOs and the family members of those affected by SUDs.
The following recommendations are offered to help ensure that employee assistance programmes and occupational social work support interventions can offer a comprehensive suite of interventions and strategies aimed at assisting the holistic recovery of employees in the post-rehabilitation stages of SUDs:
• Workplace interventions should be cognisant of the influencing role of CSOs and family members in the recovery of employees with SUDs;
• Initiation of multidisciplinary collaborations and networks between private, public and volunteer organisations. This allows for microsystems to interface at a mesosystem level and thus create resources to support family members and CSOs with the necessary health, welfare, judicial, protective and religious/spiritual services;
• Employee assistance programmes could alleviate or act as a resource in rural areas where resources aimed at supporting SUDs and their consequences are limited. Employee assistance programmes can provide effective and reliable referrals and act as a network hub for SUD-related social and therapeutic services within rural communities;
• Employee assistance programmes should ensure that they put in place contingencies such as budget allocations to offset the resources and financial constraints of families and CSOs so that they can access SUD support. For example, the provision of transport to access additional services or additional childcare assistance, or the establishment of support group sessions for employees recovering from SUDs and their families.
REFERENCES
Abrams, L. S. 2010. Sampling "hard to reach" populations in qualitative research: The case of incarcerated youth. Qualitative Social Work, 9(4): 536-550. [ Links ]
Babbie, E. 2017. The basics of social research. Boston: Cengage Learning. [ Links ]
Balmores-Paulino, R. S. 2018. Avoidance coping strategies. In: Zeigler-Hill, V. & Shackelford, T. (eds.). Encyclopaedia of personality and individual differences. Cham: Springer International Publishing. [ Links ]
Barker, J. C. & Hunt, G. 2004. Representation of family: A review of the alcohol and drug literature. International Journal of Drug Policy, 15(6): 347-356. [ Links ]
Braun, V. & Clarke, V. 2006. Qualitative research in psychology using thematic analysis. Qualitative Research in Psychology, 3(2): 77-101. [ Links ]
Bronfenbrenner, U. 2005. Making human beings human: Bio-ecological perspectives on human development. California: Sage Publications. [ Links ]
Copello, A. G., Velleman, R. D. B. & Templeton, L. J. 2005. Family interventions in the treatment of alcohol and drug problems. Drug and Alcohol Review, 24: 369-385. [ Links ]
Creswell, J. W. 2014. Research design. 4th ed. Thousand Oaks: Sage. [ Links ]
Darling, N. 2007. Ecological systems theory: The person in the centre of the circles. Research in Human Development, 4(3-4): 203-217. [ Links ]
Denning, P. 2010. Harm Reduction Therapy with families and friends of people with drug problems. Journal of Clinical Psychology, 66(2): 164-174. [ Links ]
Hlungwani, E. N., Ntshingila, N., Poggenpoel, M. & Myburgh, C. P. H. 2020. Experiences of parents with an adolescent abusing substances admitted to a mental health institution in Giyani, South Africa. Curationis, 43(1): 1-9. [ Links ]
Hudson, J. 1978. Structural functional theory, social work practice and education. The Journal of Sociology and Social Welfare, 5: 481-497. [ Links ]
Hudson, C. R., Kirby, K. C., Clements, N. T., Benishek, L. A. & Nick, C. E. 2014. Social adjustment of women with and without a substance abusing partner. Journal of Psychoactive Drugs, 46(2): 106-113. [ Links ]
Hussaarts, P., Roozen, H. G., Meyers, R. J., van de Wetering, B. J., & McCrady, B. S. 2012. Problem areas reported by substance abusing individuals and their concerned significant other. The American Journal on Addiction, 21(1): 38-46. [ Links ]
Jaeger, E. L. 2016. Negotiating complexity: A bioecological systems perspective on literacy development. Human Development, 59(4): 163-187. [ Links ]
Kail, R. & Cavanaugh, J. C. 2010. The study of human development. In: Kail, R. & Cavanaugh, J. C. (eds.). Human development: A life-span view. 5th ed. Belmont: Wadsworth Cengage Learning. [ Links ]
Lander, L., Howsare, J. & Byrne, M. 2013. The impact of substance use disorders on families and children: From theory to practice. Social Work in Public Health, 28(3-4): 194-205. [ Links ]
Lincoln, Y. S. & Guba, E. G. 1984. Naturalistic inquiry. Newbury Park: Sage. [ Links ]
Litosseliti, L. 2003. Introducing focus groups, using focus groups in research. London: Bloombury Publishing. [ Links ]
Mafa, P. & Makhubele, J. 2019. Raising a young addict: Parental narratives on living with a teenager with substance abuse problems. Gender & Behaviour, 17(4): 14116-14124. [ Links ]
Maree, K. & Pietersen, J. 2016. Sampling. In: Maree, K. (ed.). First steps in research. 2nd ed. Pretoria: Van Schaik Publishers. [ Links ]
McCann, T., Lubman, D. I., Boardman, G. & Flood, M. 2017. Affected family members experience of and coping within the context of problematic substance use: A qualitative study. BMC Psychiatry, 17(209): 1-11. [ Links ]
Papalia, D. E., Olds, S. W. & Feldman, R. D. 2007. Human development. 10th ed. New York: McGraw-Hill Publishing. [ Links ]
Perkinson, R. R. 2008. Chemical dependency counselling: A practical guide. California: Sage. [ Links ]
Reybold, L. E., Lammert, J. D. & Stribling, S. M. 2013. Participant selection as a conscious research method: Thinking forward and the deliberation of "emergent" findings. Qualitative Research, 13(6): 699-716. [ Links ]
Rich, E. G. 2017. Exploring perceived reasons and risk factors for illicit drug use among youth in the Western Cape: Implications for primary prevention. Bellville. University of the Western Cape. (PhD thesis) [ Links ]
Robinson, N. 1999. The use of focus group methodology: With selected examples from sexual health research. Journal of Advanced Nursing, 29(4): 905-913. [ Links ]
Rudd, J. E., Neuendorf, K. A., Atkin, D. J., Romano, A., Gross, C. & Ray, G. 2019. The incarcerated parent: Examining mother-child conflict at the margins through a bio-ecological lens. Journal of Family Communication, 19(3): 243-260. [ Links ]
Schultz, P. & Alpaslan, A. H. N. 2016. Our brothers' keepers: Siblings abusing chemical substances living with non-using siblings. Social Work/Maatskaplike Werk, 52(1): 90-112. [ Links ]
Schultz, P. & Alpaslan, A. H. N. 2020. Playing the second fiddle: The experiences, challenges, and coping strategies of concerned significant others of partners with a substance use disorder - Informing social work interventions. Social Work/Maatskaplike Werk, 56(4): 430-446. [ Links ]
Stokes, M., Schultz, P. & Alpaslan, A. 2018. Narrating the journey of sustained recovery from substance use disorder. Substance Abuse Treatment, Prevention, and Policy, 13(1): 112. [ Links ]
Swick, K. J. & Williams, R. D. 2006. An analysis of Bronfenbrenner's bio-ecological perspective for early childhood educators: Implications for working with families experiencing stress. Early Childhood Education Journal, 33(5): 371-378. [ Links ]
Terblanche, L., Gunya, T., Maruma, M., Mbuyisa, K., Maseko, T., Mojapelo, K., Myeni, N., Pretorius, M. & Tyson, W. 2021. Employee assistance programme and occupational social work: Interrelated with distinct features. Social Work/Maatskaplike Werk, 57(1): 16-38. [ Links ]
Tudge, J. R., Payir, A., Merçon-Vargas, E., Cao, H., Liang, Y., Li, J. & O'Brien, L. 2016. Still misused after all these years? A reevaluation of the uses of Bronfenbrenner's bioecological theory of human development. Journal of Family Theory & Review, 8(4): 427445. [ Links ]
Vélez-Agosto, N. M., Soto-Crespo, J. G., Vizcarrondo-Oppenheimer, M., Vega-Molina, S. & García Coll, C. 2017. Bronfenbrenner's bioecological theory revision: Moving culture from the macro into the micro. Perspectives on Psychological Science, 12(5): 900-910. [ Links ]
Article accepted: 10 August 2022


{kind=link}
{kind=link}