










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.58 n.1 Stellenbosch 2022
http://dx.doi.org/10.15270/58-1-995
ARTICLES
Challenges faced by social workers in rendering services to nyaope substance users
Vusi KhanyiI; Kgashane Johannes MalesaII
ISocial Worker, Life Healthcare, Johannesburg, South Africa. mthethwagv@gmail.com
IIDepartment of Social Work, University of South Africa, South Africa. maleskj@unisa.ac.za
ABSTRACT
Use of nyaope amongst South Africans has risen dramatically. Concerns have been expressed about the negative effects this illicit drug has on communities. Currently, there is a dearth of scientific evidence on the challenges facing social workers rendering services to nyaope users. This study adopted a qualitative approach guided by ecological systems theory; data were collected through semi-structured interviews through purposive sampling and analysed through identifying themes. The study established that there are many challenges facing social workers working with nyaope substance users such as dishonesty and unreliability of clients; dealing with reluctant and nonvoluntary clients and dealing with clients who return to using illicit opioids.
Keywords: challenges, non-voluntary clients, nyaope, social workers, substance abuse, substance users
INTRODUCTION
Opioid use is a major chronic health and social problem worldwide that is difficult to treat (Kalula & Nyabadza, 2012). It is estimated that 162 to 324 million across the world population between the ages of 15 to 64 use or abuse substances or have tried them (UNODC, 2013). In the Asia Pacific region, illicit opioid use is common; it has been reported that more than half of the world's opioid-using population lives in Asia (Dargan & Wood, 2012). Nyaope, also known as Whoonga, is a specifically South African illicit drug that is both dangerous and highly addictive (Slater, 2010). This illicit drug is now used in many urban and rural areas in South Africa (Mokwena, 2015). According to Daily News, a lot of young Black and poor people have become addicted to this substance (Tuwani, 2013).
Afghanistan recorded the highest annual opioid use in the world, with 2.7% of its population aged 15 to 64 years; Iran follows Afghanistan with 2.3%. China, Pakistan, Iran and India are said to have the highest consumption of heroin in Asia. In Singapore, Malaysia, Vietnam and Myanmar, heroin use is also a significant problem. Cannabis use in Asia is below the world average, ranging between 2.8 to 4.5 % (Dargan & Wood, 2012:297). Thailand, with a considerable population of people who inject drugs and are infected with HIV, has invested massively in efforts to discourage substance abuse (Dargan & Wood, 2012).
In Africa, concern over substance trafficking and use is a recent phenomenon. A major change seems to have taken place about 40 years ago when trafficking and use entered into mainstream society and there has been a speedy acceleration over the past 30 years (Mbwambo, McCurdy, Myers, Lambdin, Kilonzo & Kaduri, 2012). The troubling use of substances such as heroin and cocaine is new, having been noticed about 25 years ago in some African countries. This is also evident for substances like nyaope, which emerged in the early 2000s (Mokwena, 2015). Social breakdown is accelerating under the adverse influences of increasing poverty, civil war, ethnic conflicts, droughts and other natural catastrophes which have spurred famine and massive displacement of populations, creating a situation in which substance use worsens rapidly (Mbwambo et al, 2012). In spite of these realities, there is inadequate scope for intervention activities addressing both substance trafficking and substance use, stressing the imperative for all-inclusive interventions at all levels in affected countries (Mbwambo et al, 2012). The 2017 World Drug Report highlighted that Africa is at present experiencing the sharpest rise in heroin use worldwide, and this has been linked to Africa's role in the southern trafficking route (Haysom, Gastrow & Shaw, 2018). In Kenya there are nearly 55,000 people who inject heroin, a method that carries the highest health risks associated with this substance; the figure is above 32,000 in Tanzania and above 75,000 in South Africa. Cities with the biggest consumer markets like Mombasa, Cape Town and the Johannesburg/Pretoria metropolitan area are also affected by violence linked to the drug trade (Haysom et al, 2018).
South Africa has a deeply-root substance abuse situations in the region, and illicit substance use is subject to continuous monitoring and analysis. From the time of South Africa's transition to democracy in 1994 there have been significant shifts in the opening of the country's borders, and there has been an inflow of illicit substances and a mounting burden of associated harms (Mbwambo, et al, 2012). In fact, South Africa stands out as the main destination for much of the heroin that enters the region, both as an end destination for local dealing and consumption, and for onward shipment because traffickers apparently find it easy to ship products from South Africa to Europe. For that reason, it is not surprising that South Africa evinces a worrying increase of substance use and addiction (Ramlagan, Pelzer & Matseke, 2010). Fernandes and Mokwena (2016) state that around 15% of South African young people use and are addicted to substances. They are mainly exposed to nyaope, which is a mixture of dagga and heroin (Fernandes & Mokwena, 2016). Illicit substance use appears to be concentrated in the large urban centres of the country, with many of the rural provinces still unaffected by the use of illicit substances that have the potential to be injected (Mbwambo et al, 2012). Notably within the large urban centres of the country the use of illicit substances that have the potential to be injected such as cocaine and heroin is on the rise (Mbwambo et al, 2012).
Social workers have historically been, and will continue to be, among the primary service providers to individuals who experience substance use disorders such as dependency on nyaope (Wells, Kristman-Valente, Peavy & Jackson, 2013). While information on the prevalence of nyaope use in South Africa is currently not reliable, the number of persons accessing treatment is increasing (Lize, 2010) and social work intervention is increasingly becoming a desirable protocol.
SOCIAL WORKERS' CHALLENGES IN SUBSTANCE USE
There are general challenges that social workers face regardless of where they perform their duties. A recent account of such challenges suggests that their job requirements include increasing paperwork, excessive caseloads, dealing with difficult clients, staff shortages and irregular supervision (Center for Workforce Studies, NASW, 2006). Furthermore, unclear legislation and related guidelines have increased the number of conflicting and incompatible demands on social workers. Adamson, Beddoe and Davys (2014) concur with Hombrados-Mendieta and Cosano-Rivas (2014) that workplace adversities also stem from agency pressures that are reflected in the burgeoning caseloads, limited resources, poor organisational culture and constantly changing social policies. It is suggested that the following factors are among the reasons for burnout among social workers: growing bureaucratisation, lack of resources, role ambiguity and intense contact with the clients. Social work, as a caregiving profession, has as its main instrument the professionals themselves. Hence, the quality of service they provide is a key element in reaching their external goals, which is improving the social wellbeing of the general public (Hombrados-Mendieta & Cosano-Rivas, 2014)
THEORETICAL FRAMEWORK
This study employed ecological systems theory (EST) to understand social workers' challenges of dealing with nyaope substance users. This is one of the classic theories developed by Bronfenbrenner Urie in 1979, and further refined in 1989 and 2002 (Ryan, 2001). The theory suggest that every person is influenced by their different environmental systems. EST helps us understand why we act the way we do in different circumstances or environments. EST suggests that human problems are rooted in the mutual relationships between psychological, social, economic, political and physical forces. Ebersohn and Bouwer (2015) maintain that the environment in which we live influences our behaviour. Various scholars such as Neal and Neal (2013) and Darling (2007) note that EST operates on multidimensional levels, described as micro, meso and macro systems. These systemic levels are in continuous interaction with each other, and they influence and affect the actions and responses as well as personal growth and development.
EST enabled the researcher to explore how the surrounding environment contributes to nyaope substance users' behaviour that leads to the challenges experienced by research participants. The application of this approach further assisted the researcher to explore and understand the role of three different environmental system (microsystem, mesosystem and macrosystem) that have an influence and effect on an individual's life. Application and interpretation of these three environmental systems enabled the researcher to arrive at an in-depth understanding of social workers' challenges experienced in their day-to-day activities when working with nyaope substance users as clients. The ecological factors were systematically considered in the development of the interview guide, which seeks to provide answers to the research question.
RESEARCH METHODOLOGY
This research used a qualitative approach, which allows for the identification and elaboration of the breadth and depth of the participants' subjective experiences (Funk & Kobayashi, 2014). Exploratory, descriptive, phenomenological, and contextual designs were applied. An exploratory design was used to investigate challenges, whereas the descriptive design was relevant for providing an accurate account of challenges experienced by social workers while rendering services to nyaope substance users (Grove, Burns & Gray, 2013). A descriptive phenomenological design was employed in order to give the researchers an insight into the experiences and challenges of social workers working with nyaope substance users from the perspective of the social workers themselves. The contextual design ensured that participants are given the opportunity to choose comfortable place for the interviews to be conducted.
The goals of this study are two-fold, namely (i) to gain an in-depth understanding of the social worker's challenges and experiences with regard to working with nyaope substance users within the Community-Oriented Substance Use Programme (COSUP); and (ii) to identify possible gaps and strengths within COSUP. In order to accomplish the goals of the study, the following research objectives were formulated:
• Explore and describe social workers' experiences and challenges of working with nyaope substance users within the COSUP programme;
• Identify possible gaps and strengths within COSUP;
• Draw conclusions and make recommendations for social workers' on how to tackle the challenges experienced when working with nyaope substance users within the COSUP programme.
Typically, a qualitative investigation emphasises the importance of formulating research questions from the outset rather than relying on hypotheses (Creswell & Poth, 2016). This research responds to one main research question: What are social workers' challenges and experiences of working with nyaope substance users within Community Oriented Substance Use Programme (COSUP)?
In order for social workers to participate in the study they had to meet the following criteria for inclusion:
• Social workers working with or who have worked with nyaope substance users within the COSUP programme in Tshwane;
• They should have more than one year of working experience within the specified substance abuse programme;
• They should be able to express themselves in English, Setswana or IsiSwati.
With regard to exclusion criteria, social workers from the same office as the researchers were completely excluded to avoid undue influence and researchers' possible subjectivity.
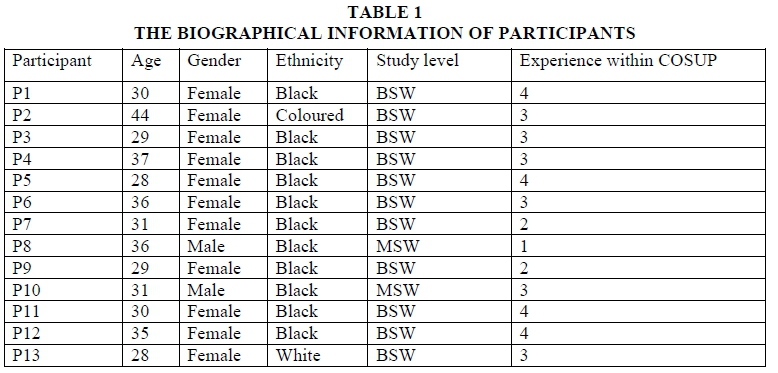
The choice of the City of Tshwane as the research site and context was informed by the fact that COSUP is run by the University of Pretoria which is within the Tshwane region (Renkin, 2015). Du Toit (2010) contends that in South Africa the concentration of homeless people is most evident on the streets of metropolitan cities such as Pretoria, with more of them being nyaope substance users. Face-to-face semi-structured interviews were conducted to generate data and data saturation was reached after 13 social workers were interviewed. Each interview took between 30-45 minutes and was conducted in Setswana, IsiSwati or English, as per the participant's choice. The SiSwati interviews were translated by the Language Department of the University of South Africa and verified by the first researcher, whereas the second researcher verified the Setswana translations. The intended outcome of the translations was to clarify the meaning and not necessarily achieve literal equivalence. To provide a comparable translation and interpretation, the researchers had to apply their knowledge and understanding of the aforementioned indigenous languages.
A purposive sampling technique was utilised to draw the sample. The data were thematically analysed following Tesch's approach (Creswell, 2014). To ensure the credibility of the findings, triangulation was applied by consulting with various knowledgeable sources on the studied phenomenon. Documenting ideas during data collection and analysis assisted in achieving confirmability. To ensure dependability, an independent coder in the data analysis validated the findings. In this study the element of transferability was enhanced by providing thick descriptions of the findings with appropriate quotations. The study was ethically approved by the College of Human Sciences Research Ethics Committee of the University of South Africa (Ref: 69239584_CREC_CHS_ 2020). The following ethical considerations were observed: obtaining written informed consent, assuring confidentiality, protecting participants from harm by following COVID-19 guidelines for researchers, and management of the research data. Participants were informed about the purpose, the risks, and benefits of participating in the study. The concept of confidentiality is linked to anonymity as confidentiality is operationalised when anonymity is maintained when reporting the data (Mahlangu & Kgadima, 2021). In adherence to the principle of confidentiality, participants' identities were not revealed, and pseudonyms were used. The participants were reminded of the service of a debriefer before and after the interview; however, no participants expressed a need for such service.
EMPIRICAL DATA ON CHALLENGES FACED BY SOCIAL WORKERS IN RENDERING SERVICES TO NYAOPE SUBSTANCE USERS
Providing services to nyaope-dependent users can be complex and challenging. The research participants identified the challenges they experience in delivering services to users. These challenges include the dishonest and unreliability of nyaope substance users, dealing with non-voluntary clients, lack of family and community support, dealing with relapse cases, untraceable clients, clients health problems/issues, clients' criminal record as a challenge, and the level of literacy as a determinant towards development access, all of which will be discussed next.
The presentation of the results is guided by the different levels of the ecological systems theory focusing on the micro, meso and macro perspectives.
Micro level
The effects of using nyaope on clients ' discernment
Nyaope substance users are a group of people that is not easy to plan for as they come late for sessions, if they do come at all. They invariably have excuses on why they did not attend or why they will not attend. They are always in a rush to make money to feed their addiction. Nyaope substance users lie and manipulate, raising questions around the authenticity of the information they provide during assessment to initiate therapeutic sessions with the social workers. When they join the rehabilitation programme, they do not stick to psychosocial and clinical intervention programmes, but they continue taking nyaope. This happens under the pretence of adhering to the programme interventions. To benefit maximally from rehabilitation programmes, it is necessary to attend meetings and engage in recovery activities, yet, as noted, attendance and engagement may be limited, inconsistent and sporadic, according to Dennis, Ingalsbe, Benbow and Daley (2013). The following extracts illustrate the unreliability of nyaope substance users that participants experience in the COSUP programme:
Most of the challenges is clients do not follow up for appointments. Some of them have psychosocial ills, problems, psychological problems, but they don't follow up so the challenge for me is I make appointment, the patient does not pitch and they come the following day when you had already booked another appointment. And you know our clients expect you to help them when they see you. (P2)
P9 reported that the freedom users have in the out-patient programme makes it unlikely for them to honour appointments:
The challenges that I used to face while working for COSUP was the fact that, remember now that COSUP is an outpatient programme. So, they don't remain in the clinic or whatever, they are not inpatient, so now you find out that the consistency is not there in terms of them now attending the sessions, you know. So, you will see the person, maybe you will say okay the follow up appointment maybe will be tomorrow or the day after tomorrow and that person will miss out those appointments. And then they will come after some time. (P9)
Social workers in the COSUP programme find it hard to assist nyaope substance users with practical help such as providing them with food and other material needs, because nyaope substance users take these things and sell them to feed their addiction, including food and medication that they get from COSUP.
We get information from other clients and community members who tell us that our clients are selling medication on the street and sometimes they mix it with water to get more money. So, they come and fetch medication not to use it, but to sell it and buy drugs. (PI2)
Social workers are lied to, deceived and manipulated by nyaope substance users and sometimes they use their unfortunate situation like lack of food to get money from social workers to buy nyaope to smoke or inject.
The deceit, the manipulation, the lies, theyoh! It takes dedication and commitment to workwith substance abuse patients. You need to have patience; you need to understand where they are coming from. You need to understand that sometimes what they are going through is not what we are going through. But is not easy, is not easy at all, is not easy remember most of our [users] have got a criminality element. (P4)
When nyaope substance users come to social workers seeking help, they express their wishes and goals of seeking help to quit using nyaope. After being on the programme, they continue using which makes them, according to one participant, uncommitted and ungrateful. This would mean social workers feel that they are not doing their work because nyaope users are almost the same before and after joining the programme, that is, still using nyaope.
Substance use field is different from other field because one will assume that if a client come to my office and is telling me they want to stop, you know, so other people come, tell you they want to stop three months down the line they are on treatment, but they continue using, so from myself at times personally I feel that people are playful, they don't recognise this opportunity that they are being given. (P10)
Dealing with involuntary clients
Therapeutic intervention with involuntary clients can be considered a big challenge for social workers, including the clients (Sotero and Relvas, 2012), for a number of reasons, such as ethical dilemmas, motivational concerns, and collaboration problems. The psychotherapeutic work carried out with clients who do not freely apply for assistance but who are referred or are compelled or mandated to participate in treatment is usually complex or frustrating (Sotero, Major, Escudero & Relvas, 2014). Professional teaching in therapy, if not in professions such as social work, normally assumes that clients are self-selected, although in fact most social workers eventually work with clients who come to treatment because of a court order or through the pressure of referral sources, other people, employers or family members. COSUP gets a lot of clients who are forced by their parents or family members to join the programme, because family members are no longer able to tolerate their behaviour, which includes stealing from them and committing petty crimes in the community, putting themselves in danger of landing in the hands of mob justice. Nyaope substance users in this study are described as non-cooperative and most of the time forced to seek professional help with regard to their substance use problems. Social workers find it hard to work with users who come involuntarily, because these users do not adhere to the treatment programmes:
We have clients coming voluntarily and then we do have clients coming in with their parents you know, and that is the ones who are being forced to come. It is difficult when they are forced to come; you know it is not sustainable, because the client is not ready. We also have clients that is being sent by court or by their employees, you know, to go and seek help. So those clients we kind of work a different way with them. We try to get them to a point where they can accept that they do have a problem. Because if there are being forced, they will say they do not have a problem. (PI)
One of the issues highlighted in the literature on non-voluntary intervention concerns the difficulties in forming and sustaining a good therapeutic collaboration with such clients. The assessment of the therapeutic collaboration with these clients becomes even more relevant when we consider the findings of other studies that show the collaboration as a substantial predictor of the success of the treatment, predominantly when measured at the beginning of the intervention (Sotero et al, 2014:2). Nyaope substance users who do not come voluntary do not attend counselling and group sessions with the social workers, although some come to the sites to simply sign the register but then they are not actively participating in the COSUP programmes for their recovery.
Services users don't want to attend counselling sessions; they say they always in a hurry, you know (laughing); they say they don't have time to sit down and have sessions. (P3)
Those who attend because they are forced to make the job of social workers hard, because social workers find it difficult to draw up a schedule for the day. For example, a group or session that was scheduled at 9 am can end up taking place at 2 pm, affecting other social work activities for that day. If they do not come for sessions or groups, it means the social worker for that day did not complete the scheduled tasks, making it impossible to reach their monthly targets.
The difference between nyaope substance users who come voluntarily and those who do not come voluntarily is that the former show signs of change and adhere to treatment programmes, which increases their chances of recovering and decreasing their chances of relapsing. Those who come non-voluntarily are there to impress and please their families or institutions like the judiciary/courts and employers, but this is not sustainable since within a few months they go back to the habit of using again:
So the one who comes at his own at least you can see that this person is ready for a change compared to the person who just came for the sake of his brother or mother or any other family relative. So with those ones who are just accompanied by their families, they end up relapsing; you can see maybe they are serious within the first month, the second month then they relapse, but with the one who just came on his own willingly to change you can see the difference because if let's say, for example, he was living on the street, the social worker will reunite him with his family, go back to his family, ask for forgiveness and then they accept him back. (PL)
The subject of cooperation and engagement is explained using two constructs. The first considers nyaope substance users who are resistant to treatment, as opposed to those who are cooperative. Resistance is characterised through avoiding contact like attending individual and group sessions, not accepting help as some continue using or injecting nyaope even after being given medication, being defensive or confrontational, responding to questions with monosyllabic answers or giving incorrect information. In contrast, cooperation is characterised by a willingness to accept help, come in for appointments, and comply with agreements (Hood, Brent, Abbott & Sartori, 2019).
There are two sets of constructs in this theme which summarise the finding. The first concerns the degree to which relationships with social workers and nyaope substance users are mediated by other people, such as parents, employers, and courts. Unmediated relationships are usually considered advantageous, because of the willingness of the nyaope substance users to get help and make reasonable changes in their lives. Moreover, they adhere to the recommended treatment in COSUP. Social workers who deal with non-voluntary users should consider that people's interests and agendas might not always be aligned (Hood et al, 2019).
Untraceable clients
Nyaope substance users are a group of people who are very mobile, moving from one place to another to make money through recycling, as car guards, and helping taxi drivers to get people in exchange for money. They can be seen in shopping malls and busy places where they can earn quick money. When they move from one place to another, they do not have secure places to stay in, meaning by default that they become homeless. 'Homelessness' includes people sleeping on the streets (rough sleeping) and in insecure or temporary accommodation, including hostels as seen in the Mamelodi West hostels where they stay (Shulman, Hudson, Low, Hewett, Daley, Kennedy, Davis, Brophy, Howard, Vivat & Stone, 2018). One interesting finding in this study is that nyaope substance users become homeless by choice as opposed to other studies that found that many homeless people live on the streets due to circumstances that force them to leave their families. Indeed, there is a high degree of consensus in the UK, North American and Australian literature that many homeless people come from homes where there is some level of physical, sexual or emotional abuse and neglect (Mayock & O'Sullivan, 2011). There is a different finding in this study as indicated below by participants:
...for people that have not been home, they were homeless not because they were actually sent away from home, but they were homeless because they actually chose to leave home and live in the street. (P13)
Nyaope substance users go onto the street to protect their families from their behaviour. Their behaviour can amount to emotional, physical abuse as well as stealing from their families. This is not in line with the behaviour of most homeless people not affected by nyaope, as they are usually the victims of physical, sexual or emotional abuse and neglect from their families. The families become victims of nyaope substance users:
And if there is one thing that worries me about substance abuse again it is that we now have most homeless people who are on the streets because of substance abuse, not that they are homeless; they chose to because they think it's safer and they also protecting their families from being harmed by their behaviour which is induced by substance abuse. (P6)
The homelessness of nyaope substance users makes it hard for them to follow up with social workers for counselling and groups in COSUP. Consequently, social workers are unable to trace them as they move from one street corner to another, making the small amount of money needed to get the next fix. Locating the users becomes a challenge. Mokwena (2016:137) observes that nyaope substance users can be easily identified as they assemble in taxi ranks and shopping malls. Homeless people who are nyaope substance users in this context have to balance competing priorities such as food, shelter and substance dependency, making them move around to satisfy these needs (Shulman et al, 2018).
When nyaope users come to receive help after disappearing for some time, they expect to be assisted quickly without due clinical and COSUP processes. They disregard the reality that a lot has happened in between, for instance, ssome changed from smoking substances to injecting; others have contracted communicable diseases; some of their families have passed on. These new developments need social workers to do their psychosocial assessments in full without bypassing any processes. If social workers were to bypass processes in their assessments and intervention, this might lead to further delays in assisting nyaope substance users to get methadone, as this is mostly their ultimate goal. Poorly managed dependency can lead to medication delays, leading to unpleasant withdrawal symptoms (Shulman et al, 2018). When users experience withdrawal, they are likely to disappear in search of money to feed their addiction. In the process, they become demotivated and only come back for follow-up to avoid the unpleasant feeling of withdrawing.
Client-health problems/issues
Heroin dependence such as that on nyaope is associated with a high incidence of co-morbid medical and mental health complications, which require separate identification and treatment. An overdose is fatal, and heroin is the substance most involved in deadly accidental poisonings in people dependent on substances. Medical complications may arise from non-sterile injection practices or needle sharing as well as skin or systemic infections, HIV or hepatitis B or C transmission, and complications arising from adulterants. Common psychiatric problems include depression and personality disorders, even with long-term abstinence (Weich, Perkel, van Zyl, Rataemane & Naidoo, 2008). The study verified that social workers in COSUP also deal with clients who are not only affected by substance use disorder, but by HIV, hepatitis, TB and mental disorders. In turn, the participants indicated that the programme issues clean needles to curb the spread of HIV and hepatitis. The responsibility and task of the social workers in this case becomes that of the assessor of risk amongst the nyaope substance users (Asquith, Clark & Waterhouse, 2005). Therefore, the challenge is to ensure that nyaope substance users get the medical attention they need by linking them with medical institutions in the community and ensuring that they adhere to their treatment as directed by their medical practitioners. This is difficult for social workers, because users are less likely to take the prescribed medications (Mancini, Linhorst, Broderick & Bayliff, 2008).
With few external supports or resources, many of these individuals return to the street and continue to use substances, resulting in many negative outcomes (Mancini et al, 2008). The negative outcomes for nyaope substance users may include deterioration in their health and poor self-care, which in turn puts at risk the lives of social workers who come into contact with them. This is supported by the following comment from one of the participants:
Some clients come to us when they are very sick, on last stage of AIDS; they have been living on the street without taking their treatment and you will be surprised that most of them don't even know their status. And when they are positive on HIV, they usually have TB as well. These health issues of clients put our lives in danger as well to contract like TB. Others are mentally unstable and it becomes difficult to manage. (P8)
Individuals with dual disorders have complex needs and require intensive, well-coordinated and comprehensive services. Individuals with these dual diagnoses experience a range of psychiatric, legal and health problems that inhibit their recovery. They are more likely to have symptom relapse, higher rates of hospitalisation, higher rates of physical and sexual victimisation, especially among women, higher rates of incarceration, and a higher risk of contracting HIV/ADDS and hepatitis B and C. In addition, they are less likely to take prescribed medication, which may result in increased violence.
Finally, individuals dually diagnosed with psychiatric and substance use disorders are at an increased risk of homelessness (Mancini et al, 2008).
While there are concerns around the health of nyaope substance users, the following extract from the data shows when nyaope substance users start receiving treatment from COSUP including social and medical services, they also start taking other chronic and non-chronic medication. This stabilises the users' health and social functioning:
There has been people who are actually receiving treatment for HIV, people who are receiving treatment for Heps (hepatitis), people who are receiving treatment for TB, people that are actually in the programme receiving treatment for substance use. (P8)
The data indicate that the users' health issues directly affect the social workers. When nyaope substance users die due to overdose or to medical complications associated with substance use like HIV or TB, their demise affects social workers emotionally because they already have a close relationship with nyaope substance users:
And the saddest part is having to lose clients. Clients who die because they are sick and they took long to be on other chronic medication, it gets difficult once you build the relationship with the client. (P12)
Meso level
Lack of family and community support
Data analysis indicates that one of the challenges of COSUP for social workers is lack of support from family members or significant others of nyaope substance users and the community. The researchers assess the first part of the theme, which concerns lack of family support and then offer an interpretation of the second part of the theme related to lack of community support. In general, social workers work with few family members of nyaope users, depending on each user, as one participant reported. It can be hypothesised that social workers see more of families of nyaope substance users who have just started using nyaope as opposed to those who have been using for a while and have experienced several relapses. Even when families show support to users, it is because they are looking at benefiting in some way, hat is, helping the client deal with behavioural issues that affect the family as a whole not necessarily for the benefit of the nyaope substance users, as indicated below:
It depends on each client I think, but in general I think I do work with quite a few family members but not all substance user family members want to participate and even if they do it depends on the level of relationship. (P7)
While family members can influence the development and maintenance of substance use disorder, they can also play a role in successfully intervening and assisting a user to achieve abstinence. Participants pointed out that with family support their work becomes easier as they witness the speed recovery as opposed to those who lack family support. Researchers demonstrate that the relationship between substance use and relationship distress is transactional in nature, rather than linear, quoting evidence indicating that substance use increases relationship distress, and on the other hand, that relationship distress may lead to increased levels of substance use behaviour (Wells et al, 2013).
A study conducted with 21 parents from a long-term, family-based teenage rehabilitation programme in Canada established that in practice parents felt unsupported by social workers and other social service professionals (Choate, 2015). Most parents spoke about wanting information that would allow them to make sense of what was happening and how they might respond most effectively (Choate, 2015). Parents felt that nothing is done by the government and social workers to help them manage living with a user (Masombuka & Qalinge, 2019). Although this study did not explore the relationship between family members of nyaope users and social workers in COSUP, a conclusion can be drawn from this Canadian study that another reason family members do not support social workers and nyaope users in COSUP is that they feel unsupported by social workers in COSUP.
One participant also spoke about families being clueless on how to manage nyaope users:
COSUP is doing well because it's touching a lot clients and helping a lot families and communities, because a lot of people in our communities especially in Soshanguve are from poor backgrounds. They don't know how to help people who are using substances, they don't know how to manage people who are using substances, so COSUP is here to educate people about how to manage substances, even families because we have a lot of families that come here and they have no idea how to manage someone who has a substance use disorder. I feel like COSUP is here to educate and also help people that are using substances. (P11)
In this regard, Van der Westhuizen, Alpaslan and De Jager (2011) confirmed that the family of the substance user lacks knowledge about recovery from substance dependency, and highlighted the necessity to make services available to them as well. Similarly, Mahlangu (2016) confirmed that the significant others of users need to be educated on how to give support to the nyaope substance user. In addition, parents and family members need professional support to improve communication between different subsystems in order to strengthen the family system (Masombuka & Qalinge, 2019).
The lack of family support to nyaope substance users also contributes to the high levels of nyaope substance users relapsing. When nyaope substance users decide to go homeless, according to one participant, families of users move on with life including taking up the user's space in the family/house. When users start seeking professional help and their lives stabilise, family members are reluctant to reintegrate the users back to the family.
While the lack of family support contributes to relapsing of nyaope substance users, relapsing of nyaope substance users is a confirmation to family members that nyaope users are not serious about their lives and enjoy taking the substance when they go back and forth. This leads to families giving up on the users and not supporting them, even when they voluntarily seek help as indicated below:
That is why I said it is still a struggle with them relapsing and families because of they don't have much knowledge about substances; they end up trying at first, trying and then giving up; sometimes they no longer come even when you call family group sessions. In addition, some of these families are disadvantaged families so they do not have money to come for sessions every week; yah it becomes a problem. (P2)
What can be noted is that nyaope users who lose contact with their families when they go to COSUP do want to be reunited with their families, because often they do not have close relationships with family members and thus lack the essential support. They have been dependent on substances, spent more time on these rather than communicating with their families and therefore affecting their relationship with family members. However, they desire to be accepted and want to be part of their families, although some of them have totally lost contact with their relatives (Sarnon, Baba, Mohamad, Wan Azreena, Lukman, Subhi, Hoesni, Fauziah, Nen, Rusyda & Nur Saadah, 2011). Unfortunately, because of lack of resources in COSUP, reuniting with their families does not happen. This discussion on lack of family support indicates that there is a need to make social workers aware that families ought to be involved during the treatment process of the dependent individual so that it eases supporting the individual after professional intervention (Mzolo, 2015).
The data show that participants' responses were on the lack of community support to the COSUP project in general and not lack of support to social workers and the services they offer to nyaope substance users. Community participation is primarily beneficial for health service organisations like COSUP, because it helps to plan health services that address the needs of the community (Ridley & Jones, 2002). Participation implies residents' and service providers' active involvement, appropriate governance and decision-making structures, since the project utilises community centres such as clinics and halls to deliver services and understands how to create and sustain partnerships (Nimegeer, Farmer, Munoz & Currie, 2016). The premise is that divulging and sharing knowledge leads to better-informed perspectives on challenges and solving problems like substance use disorders that COSUP strives to treat and manage in the community. Recent literature reviews summarise community participation outcomes from individual and collective perspectives. Community outcomes include the growth of social capital, partnerships and empowerment of not just nyaope substance users in this context, but also the community itself with regard to substance use. Individual outcomes include perceived physical and psychosocial health and positive social outcomes for nyaope users (Nimegeer et al, 2016).
In the community, it is not just the ordinary members who offer no support to COSUP, but also stakeholders such as the South African Police Service, who are unwilling to work with social workers and COSUP. This is, however, to be expected because nyaope substance users use illicit substances. This is compounded by the observation that users commit petty crimes to support their addiction as indicated below:
This community here is not supportive here at Oliven so most of the time we are alone, the counsellor, oh the clinic is supporting nyana, but the police station is just like, it's a mess. They arrest our clients for because they are chasing stats and the clients expect me to go there and take them out, which sometimes is not possible, so it's a lot of things man, it is a lot of things. (P4)
In addition, shelters that house homeless people are not keen to work with social workers that house nyaope substance users who are homeless. It emerged that the shelters want to take people who are not using substances at all or who are off substances. This means social workers are unable to help nyaope substance users to find shelter even if there is space, just because these people are dependent on nyaope. It could be inferred from the discussion above those discussions were not held with community 'gatekeepers', including the police, other professionals working in shelters, community and local councillors, and informal local leaders. Without their support, it is difficult for COSUP to 'enter' the community and offer services as the data show that police confiscate syringes and shelters deny nyaope substance users access to their facilities for homeless people (Nimegeer et al, 2016). Nimegeer et al. (2016) note that a negative impact can arise if community participation is poorly conducted, including tokenistic consultation. Specific to COSUP, community participation outcomes would enhance awareness of COSUP services, learning new skills and strengthened relationships (Nimegeer et al, 2016).
Subsequently, the stigmatisation by society leads to nyaope substance users' isolation from and discrimination in the community. Therefore, nyaope substance users embrace NGOs such as COSUP, which provide social support and services to tern Sarnon et al., 2011). According to participant P10, they then form their own community of users in order to belong somewhere. This formation of a sub-community transgresses the mainstream values and principles of life.
As discussed under the first part of lack of family support, in practice parents felt unsupported by social workers and other social service professionals (Choate, 2015). This is apparently the same for the community as one participant pointed out that, due to workload in the office, they end up neglecting the community, leading to injustice because the community then gets entangled in the stigmatisation and rejection of nyaope users. It appears that educating the community about addiction as a treatable medical condition, the availability of evidence-based treatments, what to expect during treatment and the need for ongoing aftercare is necessary to address the lack of support and misperceptions in the community (Meade, Towe, Watt, Lion, Myers, Sinner, Kimani & Pieterse, 2015).
Level of illiteracy as a determinant of development access
With reference to the South African Community Epidemiology Network on Drug Use (SACENDU, 2018), the youngest onset age for substance dependency ranges between 10 to 19 years, which is atypical age group of primary and high school learners; the numbers increased by 29% in 2017. The consequence of this is that the majority of recovering service users have dropped out of school because of their substance use from an early age. Therefore, the recovering service user population consists not only of people with no employment history and with criminal records, but of people that have failed to complete their secondary education. This reality is problematic for recovering service users, because there is little opportunity available for employment, and access to resources to complete secondary and tertiary education are limited. This challenge is one of the leading reasons that recovering service users lack motivation and commitment to maintain sobriety. P10 raises concerns around admission of nyaope substance users in skills development centres:
So as a social worker I'm encouraging that, the reading culture among the clients, and we try to link them with skills development centres that are not prejudice in terms of their requirement because some skills development centres they have exclusion criteria, you know, you must come write this test, if you fail you cannot get admitted. You have other skills development centres that do not subject the client to that, but they teach them in an interactive session and you know that helps because it helps to develop the confidence of the client, you know. But if you subject them to a test, chances are if they can't write they are not going to benefit, but if they should have sat in the session because they can listen, you know, they could have benefited a lot from that interaction. We are trying also to get life skills development centres that are not really prejudicial in terms of exclusion criteria. (P10)
In a study on addiction and treatment experiences among active methamphetamine users recruited from a township community in Cape Town, South Africa, it was found that the population is relatively uneducated (with only 27% of adults completing high school), largely unemployed (with a 40% unemployment rate), and poor (with 45% of households earning less than R600 per month, well below the poverty line. The large majority of the sample were unemployed and had not completed high school. The participants described a setting of high poverty, with little opportunity for economic and social advancement. The relationship between poverty and methamphetamine use was perceived as cyclical, with individuals initiating use due (in part) to lack of future prospects, and in turn methamphetamine use undermining their economic and social wellbeing (Meade et al, 2015).
Social workers in the COSUP try to deal with the challenge of illiteracy through empowering nyaope substance users with practical skills like gardening, helping them start small businesses, which involve skills that they already possess from selling things at traffic intersections. Social workers tried earlier to open skills centre that they believe would have addressed the needs of their clients who have criminal records and low literacy. This needs COSUP to link clinical factors with social factors of nyaope substance users that could either hinder or foster improvement and development.
Macro level
Clients' criminal records as a challenge
Substance use and criminal behaviour are closely linked, and a large percentage of substance users commit crimes. While some part of criminal behaviour is likely to take place in order to finance substance use, substance use is also clearly associated with violent crime (Hakansson & Berglund, 2012). Substance users in general have been found to be either awaiting charges, trial or sentencing, or they have a criminal record for assault, substance-related offences, burglary or larceny, parole violations, shoplifting or vandalism, robbery, forgery or arson (Deane, Wootton, Hsu & Kelly, 2012). This statement is supported by the following comment from one participant with regard to nyaope substance users:
My challenge ... with these guys is that the majority of them have criminal records associated with possession of illicit substances, robbery and shoplifting. Others are serving community imprisonment and yet they continue with criminal activities including sell nyaope, which I believe they are selling for their drug lords. Their criminal records make our job hard to help them live a genuine life and get money genuinely and for the fact that they are used to making quick money than to wait for month end while they still have to support their addiction on a daily basis. (P1)
There is increasing evidence for the association between substance use and criminality, including a high prevalence of substance use disorders in prison populations (Kinyanjui & Atwoli, 2013). A criminal record has been identified as a stigmatised social status that can result in unfair treatment and daily indignities across a variety of social settings. Discrimination based on a criminal record has been firmly established in employment, housing and receipt of other social services not only through self-reports from former prisoners, but also by multiple audit studies and other experimental designs (Agan & Starr, 2017; Schneider, 2018). Given this body of evidence, it is plausible that patients with a history of incarceration also anticipate and perceive discrimination in the healthcare settings. A history of incarceration may be documented in a patient's medical record or shared directly with a health professional, potentially leading to a discussion of other commonly stigmatised conditions such as mental illness, substance abuse or HIV risk behaviours (Frank, Wang, Nunez-Smith, Lee & Comfort, 2014).
In a study by Meade et al. (2015) on addiction and treatment experiences among active methamphetamine users recruited from a township community in Cape Town, South Africa, the majority of participants reported getting an income through illegal means, including substance dealing and sex work (Meade et al, 2015). Even though this study was not looking at what economic activities nyaope substance users engage in to earn an income, it can be assumed that with criminal records and a low level of literacy, users are left with few options to earn a genuine income. This is a challenge for social workers who strive to reintegrate nyaope substance users into mainstream society, as the criminal records become a hindrance and for the fact that people do not want to associate with people who are using substances or who have been to prison.
CONCLUDING REMARKS
This study has shown that social workers assisting nyaope users face a range of challenges during the intervention process. The challenges are directly related to the social work duty of care and support for people with a chronic condition that is hard to treat. Also, the effects of stigma and criminalisation have negative impacts on the ability of social workers to support clients to reach their goals. There is a need for decriminalisation and stigma reduction and greater societal support for people who use opioids. What became evident throughout this research is that despite such challenges, there is a room for improving the current programme and intervention to provide users with quality care by providing support to practitioners to meet the challenges they encounter at work.
REFERENCES
ADAMSON, C, BEDDOE, L. & DAVYS, A. 2014. Building resilient practitioners: Definitions and practitioner understandings. British Journal of Social Work, 44(3): 522-541. [ Links ]
AGAN, A. & STARR, S. B. 2017. The effect of criminal records on access to employment. Papers & Proceedings, 107(5): 560-564. [ Links ]
ASQUITH, S., C. CLARK, C. & WATERHOUSE, L. 2005. 'The role of the social worker in the 21st Century - a literature review', Scottish Executive Education Department, Edinburgh. [Online] Available: http://www.scotland.gov.uk/Resource/Doc/47121/0020821.pdf [Accessed 02/05/2021]. [ Links ]
CENTER FOR WORKFORCE STUDIES. 2006. Assuring the sufficiency of a frontline workforce: A national study of licensed social workers. National Association of Social Workers & Centre for Workforce Studies. [Online] Available: https://www.socialworkers.org/LinkClick.aspx?fileticket=QKU6bvt6Rwc%3D&portalid=0 [ Links ]
CHOATE, P. 2015. "Adolescent alcoholism and drug addiction: The experience of parents". Behavioural Sciences, 5(4): 461-476 [ Links ]
CRESWELL, J. W. 2014. Research design: Qualitative, quantitative and mixed methods approaches. 4th ed. Thousand Oaks: SAGE Publications. [ Links ]
CRESWELL, J. W. & POTH, C. N, 2017. Qualitative inquiry and research design: Choosing among five approaches. 4th ed. Thousand Oaks: SAGE publications. [ Links ]
DARGAN, P. I. & WOOD, D. M. 2012. Recreational drug use in the Asia Pacific Region: Improvement in our understanding of the problem through the UNODC programmes. Journal of Medical Toxicology, 8:295-299. [ Links ]
DARLING, N. 2007. Ecological systems theory: The person in the centre of the circles. Research in Human Development, 4(4): 203-217 [ Links ]
DEANE, F. P., WOOTTON, D. J., HSU, C. & KELLY, P. J. 2012. Predicting drop-out in the first 3 months of 12-step residential drug and alcohol treatment in an Australian sample. Journal of Studies on Alcohol and Drugs, 73(2): 216-225 [ Links ]
DENNIS, D. M., INGALSBE, M. H, BENBOW, J. & DALEY, D. C. 2013. 12-step interventions and mutual support programmes for substance use disorders: An overview. Social Work and Public Health, 28: 313-332. [ Links ]
DU TOIT, J. 2010. Local metropolitan responses to homelessness in South Africa. Development Southern Africa, 27(1): 111-128 [ Links ]
EBERSOHN, S. & BOUWER, A. C. 2015. A bio-ecological interpretation of the relationship challenges in the context of the re-constituted family. S.A. Journal of Education, 35(2): 1-11. [ Links ]
FERNANDES, L. & MOKWENA, K. E. 2016. The role of locus of control in nyaope addiction treatment. South African Family Practice, 58(4): 153-157 [ Links ]
FRANK, J. W., WANG, E. A., NUNEZ-SMITH, M., LEE, H. & COMFORT, M. 2014. Discrimination based on criminal record and healthcare utilization among men recently released from prison: A descriptive study. Health and Justice, 2(6): 1-8. [ Links ]
GROVE, S K , BURNS, N , & GRAY, J R 2013 The practice of nursing research: Appraisal, synthesis, and generation of evidence. 7th ed. St Louis: Elsevier Health Sciences. [ Links ]
HAKANSSON, A. & BERGLUND, M. 2012. Risk factors for criminal recidivism - A prospective follow-up study in prisoners with substance abuse. BMC Psychiatry, 12(111): 1-8. [ Links ]
HAYSOM, S , GASTROW, P. & SHAW, M 2018 The heroin coast: A political economy along the Eastern African seaboard. Pretoria, South Africa: ENACT. [ Links ]
HOMBRADOS-MENDIETA, I. & COSANO-RIVAS, F. 2013. Burnout, workplace support, job satisfaction and life satisfaction among social workers in Spain: A structural equation model. International Social Work, 56(2): 228-246 [ Links ]
HOOD, R., BRENT, M., ABBOTT, S. & SARTORI, D. 2019. A study of practitioner-service user relationships in social work. The British Journal of Social Work, 49(3): 787-805. [ Links ]
KALULA, A. S. & NYABADZA, F. 2012. A theoretical model for substance abuse in the presence of treatment. South African Journal of Science, 108(3-4): 96-107. [ Links ]
KINYANJUI, D.W.C. & ATWOLI, L. 2013. Substance use among inmates at the Eldoret prison in Western Kenya. BMC Psychiatry, 13(53): 1-8. [ Links ]
LIZE, W. 2010. Defeating the dragon - Can we afford not to treat patients with heroin dependence? South African Journal of Psychiatry, 16: 75-79 [ Links ]
MAHLANGU, S. H. 2016. The aftercare needs of nyaope users in the Hammanskraal community. Pretoria: University of Pretoria. (Master's dissertation) [ Links ]
MAHLANGU, T. & KGADFMA, N. P. 2021. Social exclusion and marginalisation of homeless people: A clarion social work call for the spirit of Ubuntu to reign. Social Work/Maatskaplike Werk, 57(4): 455. [ Links ]
MANCINI, M. A., LINHORST, D. M., BRODERICK, F. & BAYLIFF, S. 2008. Challenges to implementing the harm reduction approach. Journal of Social Work Practice in the Addictions, 8(3): 380-408. [ Links ]
MASOMBUKA, J. & QALINGE, L. 2019. Outcry and call for relief: Experiences and support needs of parents with nyaope users. Social work/Maatskaplike Werk, 56(1): 52-62. [ Links ]
MAYOCK, C. & O'SULLIVAN, P. 2011. Homeless young people, families and change: Family support as a facilitator to exiting homelessness. Child and Family Social Work, 16: 391-401. [ Links ]
MBWAMBO, J., MCCURDY, S. A., MYERS, B., LAMBDIN, B., KILONZO, G. D. & KADURI, P. 2012. Drug trafficking, use, and HIV risk: The need for comprehensive interventions. Journal of Social Aspects of HIV/AIDS, 9(3):154-159. [ Links ]
MEADE, C. S., TOWE, S. L., WATT, M. H, LION, R. R, MYERS, B., SINNER, D., KIMANI, S. & PIETERSE, D. 2015. Addiction and treatment experiences among active methamphetamine users recruited from township community in Cape Town, South Africa: A mixed-methods study. Drug Alcohol Dependency, 152: 1-18. [ Links ]
MOKWENA, K. E. 2015. The novel psychoactive substance 'nyaope' brings unique challenges to mental health services in South Africa. International Journal of Emergency Mental Health and Human Resilience, 17(1): 251-252. [ Links ]
MZOLO, M. P. 2015. Exploring family support for adolescents after rehabilitation for drug abuse. Pretoria: University of South Africa. (Master's thesis) [ Links ]
NEAL, J. W. &NEAL, Z. P. 2013. Nested or networked? Future directions for ecological systems theory. Social Development, 22(4): 722-737 [ Links ]
NEVIEGEER, A., FARMER, J., MUNOZ, S. A. & CURRIE, M. 2016. Community participation for rural healthcare design: Description and critique of a method. Health and Social Care in the Community, 24(2): 175-183. [ Links ]
RAMLAGAN, S., PELTZER, K. & MATSEKE, G. 2010. Epidemiology of drug abuse treatment in South Africa. South African Journal of Psychiatry, 16(2): 40-49. [ Links ]
RENKIN, W. 2015. Finding a prophetic response to end homelessness in the City of Tshwane: A transdisciplinary approach. Pretoria. University of Pretoria. (Master's thesis) [ Links ]
RIDLEY, J. & JONES, L. 2002. User and public involvement in health services: A literature review. Partners in Change, Edinburgh: Scottish Government. [ Links ]
RYAN, D. P. 2001. Bronfenbrenner's ecological systems theory. [Online] Available: https://dropoutprevention.org/wpcontent/uploads/2015/07/paquetteryanwebquest_20091110.pdf [Accessed: 27/07/2021]. [ Links ]
SARNON, N, BABA, L., MOHAMAD, M. S., WAN AZREENA, W. J., LUKMAN, Z. M., SUBHI, N, HOESNI, S. M., FAUZIAH, I., NEN, S., RUSYDA, H. M. & NUR SAADAH, M. A. 2011. Characteristics of injecting drug users in needles syringes exchange programme (NSEP). Journal of Social Sciences & Humanities, 19(5): 129-138 [ Links ]
SHULMAN, C, HUDSON, B. F., LOW, J., HEWETT, N, DALEY, J., KENNEDY, P., DAVIS, S., BROPHY, N, HOWARD, D., VIVAT, B. & STONE, P. 2018. End-of-life care for homeless people: A qualitative analysis exploring the challenges to access and provision of palliative care. Palliative Medicine, 32(1): 36-45. [ Links ]
SCHNEIDER, G., 2018. Automating drug discovery. Nature reviews drug discovery, 17(2): 97-113. [ Links ]
SLATER, C. 2010. Nyaope, a New Killer on the Block. [SI]. [Online] Available: www.1ooklocal.co.za/.../bedfordview-edenvmiale-news-general/ [Accessed 09/08/2020]. [ Links ]
SOTERO, L. & REL VAS, A. P. 2012. A intervenção com clientes involuntários: Complexidade e dilemas. Psicologia & Sociedade, 24: 187-196. [ Links ]
SOTERO, L., MAJOR, S., ESCUDERO, V. & RELVAS, A. P. 2014. The therapeutic alliance with involuntary clients: How does it work? Journal of Family Therapy, 1-22. [ Links ]
SOUTH AFRICAN COMMUNITY EPIDEMIOLOGY NETWORK ON DRUG USE (SACENDU). 2018. Publication. News update. [Online] Available: http://www.mrc.ac.za/intramural-research-units/ATOD-sacendu [Accessed 3/02/2021]. [ Links ]
TUWANI, T. 2013. Giving up nyaope is hard; relapse is easy. Daily News, 16 October. [Online] Available: https://www.iol.co.za/dailvnews/opinion/giving-up-nvaope-is-hard-relapse-is-easv-1592562 [Accessed 16/01/2020]. [ Links ]
VAN DER WESTHUIZEN, M., ALPASLAN, A. & DE JAGER, M. 2011. Preventing relapses amongst chemically addicted adolescents: Exploring the state of current services. Social work/Maatskaplike Werk, 47(3): 350-370. [ Links ]
WEICH, L., PERKEL, C, VAN ZYL, N, RATAEMANE, S. T. & NAIDOO, L. 2008. Medical management of opioid dependence in South Africa. SAMJ Forum, 98(4): 598-601. [ Links ]
WELLS, E. A., KRISTMAN-VALENTE, A. N, PEAVYK. M. & JACKSONT. R. 2013. Social workers and delivery of evidence-based psychosocial treatments for substance use disorders. Social Work Public Health, 28(0): 279-301. [ Links ]
UNITED NATIONS OFFICE ON DRUGS AND CRIME (UNODC). World drug report. 2013. [Online] Available: http://www.unodc.org/unodc/secured/wdr/wdr2013/World_Drug_Report_2013.pdf [Accessed on 05/08/2020]. [ Links ]


{kind=link}