










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.57 n.3 Stellenbosch 2021
http://dx.doi.org/10.15270/52-2-950
ARTICLES
Traumatised older persons' experiences of eye movement integration as trauma intervention
Andrea VisagieI; Annaline KeetII
IClinical Social Worker, Knysna, South Africa
IIDepartment of Social Development Professions, Nelson Mandela University, Summerstrand, Gqeberha, South Africa
ABSTRACT
The world's population is ageing and older people may be exposed to traumatic experiences during their lifetime. Symptoms are often regarded as part of the ageing process and not treated as trauma. Little is known about eye movement integration (EMI) as intervention for symptoms of trauma in older people. This article reports on older people's experience of EMI as an intervention for their symptoms of trauma. The qualitative study employed an exploratory-descriptive research design with a purposive sampling method. Participants considered EMI as positive and beneficial. Suggestions are made to improve EMI when working with older people.
Keywords: age, ageing, eye movement integration (EMI), older person, post-traumatic stress disorder (PTSD), trauma
INTRODUCTION
Life expectancy has increased dramatically over the past few decades, particularly in Western societies (Bürgin, Boonmann, Schmid, Tripp & O'Donovan, 2020), with an expectation that it will still rise substantially. Globally it is estimated that the population living longer than 60 years of age in 2019 will double by the year 2050 (UN DESA, Population Division, 2019). South Africa is described as a developing country (O'Dowd, 2014), meaning that there are limited resources available along with low socioeconomic development. In South Africa citizens 60 years and older, with no other financial means, qualify for an older person's grant (DSD, 2017). In 2021, this amounted to R1,890 per month (South African Government, 2021) and is paid out to the older individual. Families do not receive additional financial support to care for older family members, including those who need assisted-living and frail-care attention, putting enormous strain on the family. While the state makes provision for institutional care, the South African elder care policy stresses the importance of ageing in the community instead (Kelly, Mrengqwa & Geffen, 2019). Dealing with physical needs such as food security, housing and transportation is often the priority when facing resource limitations instead of addressing psychological needs (Fulmer, Reuben, Auerbach, Fick, Galambos & Johnson, 2021). Olofsson (2014), Bürgin et al. (2020) and Arpino, Gumà and Julià (2018) suggest that early-life circumstances influence physical and psychological health in later life. These include social experiences, and do not have to involve physical experiences, to impact on health status. Peterson (2021) indicates that adults can easily recall memories from their early childhood years as far back as the age of two to three, positing that older people may be living with traumatic memories from events that happened in their earlier years. However, many older adults may not have received any intervention for their symptoms of trauma.
This paper reports on results from a larger study that looked at older people's responses to EMI as an intervention for their symptoms of trauma, as well as to determine its value as an area for further investigation. This paper specifically reports on the older people's experience of EMI as an intervention for their symptoms of trauma.
TRAUMA AND OLDER PEOPLE
The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (American Psychiatric Association, 2013) refers to trauma as the experience of an event that includes exposure to actual or threatened death, serious injury or sexual violence. Davidson (2018) refers to trauma as a serious and unexpected event that is experienced by the individual as overwhelming. The emphasis is on the individual's perception and experience of the event which causes it to be traumatic for them.
Older people are vulnerable to certain types of traumas. They are likely to experience unexpected deaths of people close to them, the loss of a life partner that signals diminishing social support networks, and other normative life events like retirement and changes in their living arrangements (Ogle, Rubin & Siegler, 2014). Symptoms of trauma start to develop when the sensory information fails to integrate properly after a traumatic incident (Beaulieu, 2012).
The impact of complex trauma in early life can have a detrimental and long-lasting effect on a person's health and wellbeing (Dye, 2018). When an individual is exposed to high levels of stress or trauma over an extended period, certain hormone levels increase causing changes in brain function (Kim, Pellman, & Kim, 2015). When pain and suffering build up over a period, it impacts negatively on the functioning of the immune system, causing unnecessary distress (Kaiser, Seligowski, Spiro III & Chopra, 2016; Olofsson, 2014; Sadock, Sadock & Ruiz, 2015).
Older people are more inclined to seek medical attention for serious physical symptoms but avoid seeking help for mental health issues (Frost, Nair, Aw, Gould, Kharicha, Buszewicz & Walters, 2019). They may not always be sure when to seek help for their anxiety or depressive mood symptoms. When left untreated, these symptoms can deteriorate (Hiskey & McPherson, 2013). Inexperienced professionals often overlook symptoms of trauma in older people, as such symptoms may easily be regarded as part of the ageing process. A study by Böttche, Kuwert and Knaevelsrud (2012) indicated that although there seems to be an overall decline in the severity of PTSD in older persons over time, there appears to be an increase in avoidance behaviours as a coping strategy to keep recurrent and disturbing memories under control. Social workers and other health professionals could play an active role in promoting different trauma interventions for older people. Several evidence-based trauma interventions are available. Watkins, Sprang and Rothbaum (2018) recommend the following when dealing with trauma: cognitive behavioural therapy (CBT), cognitive processing therapy (CPT), prolonged exposure (PE), eye movement desensitisation therapy (EMDR) and narrative exposure therapy (NET). A brief discussion on each one follows below.
CBT works especially well with children, including young children and adolescents (Brown, Cohen & Mannarino, 2020). The focus is to assist children and their caregivers in developing skills to manage their thoughts, feelings and behaviours in 8-20 sessions (Lewey, Smith, Burcham, Saunders, Elfallal & O'Toole, 2018; Pollio & Deblinger, 2017). EMDR is also an effective short-term trauma intervention with noticeable reduction of symptoms already in one 90-minute session. It is based on a manual whereby exposure and cognitive components are involved in the protocol. EMDR is discussed in more detail later in this paper following a comparison with EMI as they share similar components, although they are two separate kinds of intervention (Lewey et al., 2018). Watkins et al. (2018) highly value PE and CPT as exposure therapy for treating trauma because of its research evidence base. CPT is based on social cognitive theory and informed emotional processing theory. The intervention uses a manual that includes 12 sessions held on a weekly basis individually or in group format. PE is adopted from emotional processing theory. Sessions vary between 8-15 sessions involving psychoeducation, breathing retaining techniques and exposure strategies to address different avoidance behaviours. NET is a form of psychotherapy aiming to reduce anxiety through a process linking the implicit trauma memories with the episodic context. Depending on the trauma complexity, anything between four and 12 sessions of 90 minutes prove to be sufficient (Lely, Smid, Jongedijk, Knipscheer & Kleber, 2019). EMI is regarded as both a neurotherapy and psychotherapy (Van der Spuy, 2014), using guided eye movements with a focus on the relationship between these eye movements and thought processes. EMI is discussed in more detail later in this paper.
PROBLEM STATEMENT
Research studies indicate that there is a large amount of information available on older people's previous exposure to trauma and its impact on later life (Arpino et al., 2018; Dye, 2018; Bürgin et al., 2020; Lindwall, Berg, Bjälkebring, Buratti, Hansson, Hassing, Henning, Kivi, König, Thorvaldsson & Johansson, 2017; Ogle et al., 2014; Sadock et al., 2015). Yet there is a lack of recorded knowledge concerning effective intervention strategies for treating trauma in older persons. Symptoms of trauma may be the result of sensory information that failed to properly integrate after a traumatic incident (Beaulieu, 2012). Given that older people may have encountered some form of trauma in their lives, these untreated symptoms of trauma can negatively affect their overall health and wellbeing. Older adults are an ideal population from whom to extract information for research around trauma. They have lived long enough to potentially have experienced some form of trauma (Ogle et al., 2014; Osborne, 2012) and are mostly able to describe their experiences.
The life stage of late adulthood can be regarded as a phase of transition. How well older people adjust to their new lifestyle after retirement largely influences their psychological wellbeing (Lindwall et al., 2017). Osborne (2012) asserts that previous developmental issues can be triggered when struggling to successfully make the transition, causing various psychological effects, including feeling disengaged or anxious about death. According to Bürgin et al. (2020), a relatively high proportion of older people were exposed to life-span trauma and they argue that a combination of childhood adversity and adult trauma increase their chances of becoming ill, leading to premature mortality.
The results of the application of EMI on adults (Beaulieu, 2003) and on children (Struwig & Van Breda, 2012; Van der Spuy, 2014; Van der Spuy & Van Breda, 2018) reflect a drastic reduction in their symptoms of trauma. To date, no research on the use of EMI on older people has been documented in South Africa or internationally. Given the life stage that older people find themselves in, EMI as short-term trauma intervention may be beneficial for this age group. In EMI the client is secure and focused on the present, creating a sense of safety and security. The words "just take note of it" are often used during the EMI protocol. According to Levine (2015), those are important words in effective trauma interventions because they help the client notice what is going on inside of them. This observation allows the left (rational) and right (emotional) parts of the brain to connect. Depending on the amount and complexity of the trauma experience, only one session of EMI may be sufficient to reduce symptoms of trauma in older people. It may also be used in conjunction with other interventions. EMI is addressed further later in this paper.
Feedback on the personal experiences of older people concerning the effectiveness of EMI can contribute to the body of knowledge. This paper reports on how older people experienced EMI as a trauma intervention and incorporates their suggestions for further use with the older population. This brief, cost-effective intervention could potentially ENHANCE their overall health and emotional wellbeing. In the South African context, this may provide social workers with material for appropriate trauma interventions for older individuals.
LIFE COURSE THEORY AS THEORETICAL FRAMEWORK
Life course is individual and at the same time social (McDaniel & Bernard, 2016). According to Elder Jr., Johnson and Crosnoe (2003), the order in which individuals participate in events and roles that are socially defined over time is referred to as a life course. Life course theory recognises the relationship between individuals and their historical, biographical and socio-economic contexts. It attempts to better understand the social pathways and refers to the trajectories or routes that individuals follow through society regarding education, work, family, residences and career, and how these concepts are shaped by their circumstances. In its broader outlines, the theory examines an individual's life history and investigates how early events influence future decisions and events concerning marriage, divorce, engagement in crime or the incidence of disease. In other words, a combination of early and midlife events has a significant influence on later life (Hendricks, 2012).
Life course theory is used as a theoretical lens to speak to the experience of trauma for older people. It provides a lens for understanding how early-life experiences shape health across an entire lifetime as it systematically directs attention to the role of the social and physical context along with biological factors over time (Olofsson, 2014). McDaniel and Bernard (2016) assert that our daily experiences fit within a bigger process throughout our lifetime and they provide an appropriate summary of the three main ideas around life course. Firstly, biological, psychological and social processes are ever present during a lifetime and therefore form part of ageing. Secondly, social and environmental factors influence a person's life-course pattern. Finally, new life course patterns bring about new social structures and help shape individual life courses.
EYE MOVEMENT INTEGRATION (EMI)
EMI is known as both a neurotherapy and psychotherapy (Van der Spuy, 2014) and has its roots in neuro-linguistic programming (NLP) (Beaulieu, 2003). According to Beaulieu (2012), neuro-linguistic programming posits that our thought processes are neurologically based. This approach implies that our nervous system continuously transmits information to and from our brain. Our five senses help to gather, filter and store the information. Our perceived reality is a result of how information is processed through our nervous system, leading to our understanding of the experience. There is therefore a direct link between our thoughts and experience of reality, and how information is received through our senses. Connirae and Steve Andreas developed EMI in 1989 and Danie Beaulieu modified it in 2003 with their permission (Beaulieu, 2012). Since eye movements are part of our built-in resilience and a natural way to process information on a subconscious level, EMI is based upon guided eye movements and focuses on the relationship between eye movements and thought processes (Struwig & Van Breda, 2012). In EMI, the clinician works with the client to consciously address their symptoms of trauma by accessing and integrating multi-sensory information from their memories. The aim is to integrate traumatic memories resulting from unintegrated sensory information of a traumatic experience and reduces symptoms and distress (Beaulieu, 2012; Struwig & Van Breda, 2012). EMI assists people to integrate their explicit memories from the hippocampus with their implicit memories in the amygdala to enhance their emotional wellbeing (Struwig & Van Breda, 2012).
The clinician uses a manual on the protocol applied during the 60-90-minute EMI session. A detailed explanation of the entire process and protocol of EMI is provided in Beaulieu (2012), while a summary on the application is included in Beaulieu (2005) and Struwig and Van Breda (2012). A brief outline on the process and its application follows below.
An in-depth clinical assessment is conducted to determine whether EMI would be suitable for the client seeking help. Preparation is done by explaining the working of EMI to the client. The clinician creates and uses a secure anchorage by deciding along with the client on ways of anchoring for times when the client might need to be grounded. The client identifies a troubling memory and describes the internal representation of that memory in his or her own words from their perspective as they recall the traumatic event. The clinician determines the client's visual range, preferred distance of the hand from the eyes, as well as the preferred speed of eye movements in accordance with the protocol. The clinician applies the EMI protocol by making use of 22 eye-movement patterns to assist the client in providing new patterns to access cues. The protocol specifies some aspects in terms of the sequence, number, duration, rhythm of the movements and technical details of the hand movements. However, the intervention is not entirely rigid and allows for some modifications to fit people's needs. For instance, EMI sessions with the older age group took longer than the anticipated 60-90 minutes to complete. The clinician answers questions that the client may have and explains to them what to expect after the EMI session. A follow-up session after two weeks is recommended to assess changes and establish a way forward. The assessment and preparation can be done together in one session prior to the EMI intervention session.
Eye movement desensitisation and reprocessing (EMDR) is another form of psychotherapy suitable for treating trauma in adults (Lenferink, Piersma, De Keijser, Smid & Boelen, 2017). Although EMDR and EMI are different forms of trauma interventions, they share similarities worth mentioning. Both EMI and EMDR employ eye-movement techniques and can retrieve the trauma memory in its full intensity (Beaulieu, 2012). The differences between the two interventions include the following: EMI uses many different eye movements across the entire visual field of the client; it follows the speed of the client; it facilitates multi-sensory integration; and it accesses the unconscious aspects of the trauma. EMDR maintains the same eye-movement pattern or segment until no more change is observed in the client's responses, and only then does it change to another direction; the speed is as fast as possible; there are slower movements with resource activation; and the emphasis is on conscious cognitive restructuring. The main distinctions lie in the differences in protocol and in the processing and restructuring of the trauma memory, which seems to be done more comprehensively during EMI. Because EMI depends on facilitated multi-sensory integration during the protocol, unlike EMDR, it creates new synaptic reactions and fewer sessions are necessary (Beaulieu, 2012). In EMDR the therapist relies on an eight-stage process which encompasses bilateral stimulation (Rubin, 2014) and has an element of conscious cognitive restructuring to it (Beaulieu, 2012).
The co-founder of EMI, Dr Danie Beaulieu, shared EMI as a trauma intervention with many social workers and psychologists in different countries. It can therefore be accepted as an international concept. In the context of South Africa, two research studies on the effectiveness of EMI were conducted and documented, suggesting that it is useful as an intervention for treating trauma in adolescents (Struwig & Van Breda, 2012) and young children aged five to seven years (Van der Spuy, 2014; Van der Spuy & Van Breda, 2018). The research on children reflected a drastic reduction in their symptoms (Van der Spuy, 2014; Van der Spuy & Van Breda, 2018). No research on the use of EMI on older people is documented at this time in South Africa or internationally.
METHODOLOGY
The data for this paper were extracted from a broader qualitative study with ethical approval from the academic institution concerned. The research design is explorative and qualitative descriptive in nature (Sandelowski, 2000), focusing on older people's experience of EMI as an intervention for addressing their symptoms of trauma. It reflects their views on how the intervention facilitated the processing of their symptoms of trauma. This paper reports on the findings around their experience of EMI as trauma intervention.
Exploratory research designs are ideal when little is known about a phenomenon, in a way working your way through a research topic (Swedberg, 2020). Some research on EMI is available, but little is known about its use with older people. A qualitative descriptive design (Sandelowski, 2000) provides a complete summary of events, where researchers can provide an accurate account of what took place. Sandelowski (2000) refers to this as descriptions that both researchers and participants can agree is an accurate interpretation of events, thus contributing to interpretive validity. The research thus offers an account of older people's experience of EMI (Sandelowski, 2000; Rubin & Babbie, 2005).
The study population was made up of older adults aged between 60 and 75 years old who applied EMI to address traumatic experiences. An invitation was sent to people who had already made use of the service to participate in the research. Using this purposive sampling technique, ten older people agreed to participate in the research. Their EMI intervention had been concluded at the time of the research. Inclusion criteria for the research were that they were living in the George, Knysna and Plettenberg Bay area, have no cognitive impairment, concluded EMI intervention for traumatic experience(s) and volunteered to participate in the research. Ethical considerations such as avoidance of harm, voluntary participation, informed consent and confidentiality guided the study. Only participants who volunteered to participate were selected for the study. Informed consent was managed by the research assistant, who also assisted with the interviews. Interview transcripts were anonymised by the research assistant. These measures were included to deal with the potential power imbalances that can occur when someone who provides the intervention also engages in the research. Provision was made for participants to be referred to a counsellor in their area in the event of their experiencing emotional strain as a result of the interviews. None of the participants needed the additional assistance. As indicated earlier, ethical clearance was obtained from the respective academic institution before data collection took place.
A combination of data-gathering techniques was used for the broader study, that is, qualitative interviewing, document study and secondary analysis. To cover the first objective of the main study, participants were subjected to a semi-structured one-on-one qualitative interview to determine their experience of EMI as an intervention for their symptoms of trauma. This paper reports on these findings.
Since the primary researcher provided the EMI interventions, a research assistant, who is a clinical psychologist, assisted with the interviews. The interviews were conducted in English and participants could answer honestly about their personal experience and their views of EMI. Questions guiding these interviews focused on their experience of the intervention, how it was different from other interventions they had engaged in, and the impact on their symptoms of trauma. Participants also provided feedback on aspects that they did not find useful, their views on it as an intervention and the impact of the intervention on their emotional and physical wellbeing. A qualitative content analysis process was employed. Roller (2019) explain this as a process where data are systematically reduced into categories, and analysed with a specific focus on the context in which they were shaped. Themes were identified to elicit meaningful interpretations of the data. An independent coder sorted and coded the data from the qualitative interviews and divided them into segments that helped to identify themes.
RESULTS
This set of results, derived from the larger study, reflected older people's experience of EMI as an intervention as well as their suggestions for its use with older people.
BIOGRAPHICAL INFORMATION
Ten participants took part in the study. They had already received an EMI intervention and subsequently volunteered to participate. One male and nine females participated in the study.
AGE
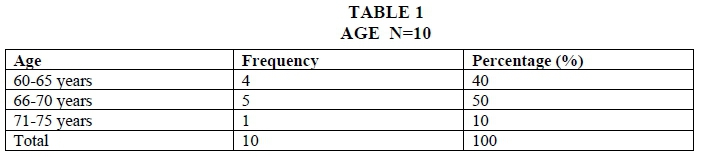
The effect of age on physical and emotional wellbeing is an important factor to consider in trauma work. Stuart-Hamilton (2011) highlights the point that older people are a vulnerable group because later life is a period of physical and/or mental deterioration. From Table 1 it is evident that 50% of the participants were aged between 66 and 70 years. Only one participant was between the ages of 71 and 75 years.
Civil status
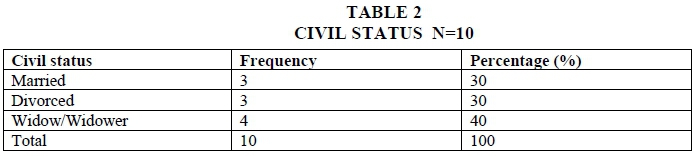
Table 2 indicates that an equal number of participants were either married (30%) or divorced (30%). Having been exposed to the unexpected deaths of people close to them and/or experiencing the loss of a life partner is not unusual for people in this age group (Ogle et al., 2014). Almost half (40%) are unattached as their spouses had passed away.
Forms of trauma
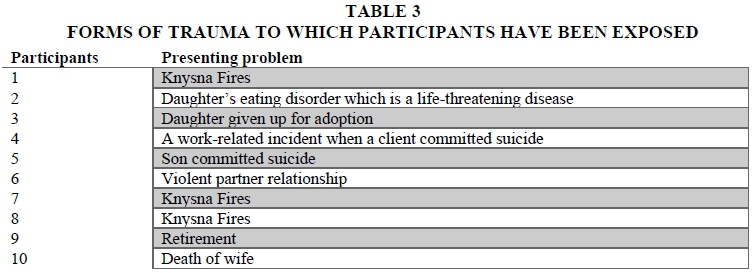
Considering the cumulative exposure to traumatic events most older adults would have experienced during their lives, some participants were more vulnerable to adverse post-traumatic outcomes than others (Arpino et al., 2018). During the assessment, people had the opportunity to identify a troubling memory that they felt needed reviewing. The forms of trauma differed significantly from one person to another, except for three participants who shared a similar traumatic experience, the Knysna fires in 2017. Over the past few years several natural disasters have occurred in South Africa (Geldenhuys, 2017). In 2017 and again in 2018 many people, including participants from this study, saw some of the most destructive open wildfires in and around the Knysna area. The fires spread rapidly and destroyed homes and businesses as well as causing loss of lives.
One participant raised retirement as a form of non-integrated trauma that had a considerable impact on her physical and emotional wellbeing. Not everyone finds the transition to adapt to their new lifestyle to be easy (Lindwall et al., 2017). Those who are faced with challenges such as giving up a career, facing financial difficulties, feeling isolated, experiencing a loss of identity and so forth may have a difficult time adjusting to this new way of living. These challenges can be experienced as stressful and older people may be subject to psychological effects that could over time impact on their health (Osborne, 2012).
Participants identified and chose to work on different traumatic incidents that significantly affected their wellbeing. The following results were obtained from the qualitative interviews. A comprehensive discussion on the following two themes follows, namely older people's experience of EMI and suggestions for further use of EMI with older people.
Theme 1: Older peoples experience of EMI
It was important for the researcher to understand how older people experience EMI as a trauma intervention as this guides its use. From the participants' views on their experiences of the trauma intervention, four subthemes emerged. A comprehensive discussion of the subthemes follows.
Subtheme 1.1: EMI was experienced as completely new and different from previous experiences or expectations of trauma intervention
Although EMI has already been introduced internationally, it seems to be a relatively unfamiliar concept to many people in South Africa. To date, only three publications on two studies on EMI are documented in South Africa (Struwig & Van Breda, 2012; Van der Spuy, 2014; Van der Spuy & Van Breda, 2018). The focus of these studies was on children. No research is yet available on the use of EMI on older people in South Africa or internationally.
Nine of the ten participants indicated that they were unfamiliar with EMI as an intervention, having never heard of it before. Only one knew about EMI prior to her receiving the intervention and described her experience as follows: "It was just refreshing to find something different from what I've been trying" (Participant 4). Participants 6-10 reported that they had not had any trauma interventions before EMI and therefore did not have anything with which to compare it. Those who have had trauma interventions before reported that they experienced EMI as something completely different compared to other therapeutic interventions. Participant 2 described the experience by saying: "I found it a little bit unusual, but you know, it did help." Participant 10 reported that "yes, it certainly was interesting for me." Participants 4 and 5 admitted to feeling uncertain about the intervention in the beginning because it was so new to them. Participant 5 indicated that "it was something completely new and totally different for me and I was perhaps a bit cynical as to whether it would really work."
Subtheme 1.2: Older people enjoyed the experience of receiving EMI
Several participants indicated that they enjoyed the experience of receiving EMI. Seven individuals specifically pointed out that EMI had been positive for them and that the interventions were beneficial. For example, participant 5 described her experience as having an epiphany: "Different … because I didn't expect it to have the results that it did have. That I found was quite a sort of an "Aha" moment."
Levine (2015) suggests that by asking the client to notice what happens next without discussing details helps to activate brain pathways that connect the rational and emotional parts of the brain. In this way, the client can deliberately rearrange the brain's perceptual system. This process seems to have happened for participant 4, who elaborated on her experience of EMI as being positive by saying that she "was not forced to go into depth/detail… So, exceeded any expectations I ever had… There was an emotional release that I never ever experienced with counselling." Participant 2 shared that it was easy for her to express herself, and participant 10 said that "certainly, it makes you relax and gets you to talk." Participant 9 said that the intervention made her focus on herself for a change: "this whole actual thing made you focus more on yourself… and I think that helped me a lot."
Some other aspects that also appeared to add to the positive experience were the fact that the participants felt that a safe space was created (Participants 1 & 3) and that the therapist came across as organised and professional (Participants 6, 7 & 9).
… such good listeners, you've been trained I suppose to do that and you are so compassionate that it's always a nice place to be… and somebody is actually interested in how you're feeling and that's always a nice thing to be able to share. (Participant 1)
She was very precise about how to place me and whether I was comfortable. (Participant 3)
She put it across very well and she was very organised… I thought that it was very good… she was very professional. (Participant 9)
Subtheme 1.3: The repetitiveness of the technique had an impact on older people's experience of EMI
As part of the EMI protocol, the clinician uses 22 eye-movement patterns to assist the client in providing new patterns of accessing cues. The eye movements assist the client to access information about the traumatic incident stored in the relevant multi-sensory modalities. To help the brain remember, there is an eye movement in each visual field. The eye movements repeat until the clinician knows that the integration of the trauma material has taken place (implicit and explicit memories have reconnected and integrated) and there is a transformation in the content (Beaulieu, 2012; Struwig & Van Breda, 2012).
The EMI protocol is one of the most influential factors in how the participants viewed their experience of EMI. The repetitiveness of the eye movements as part of the protocol brought forth two perspectives: some participants felt they needed more of a challenge, others reported that it helped them focus and concentrate. This suggests that even though they had an overall positive experience, there are still some aspects to the interventions that were less enjoyable.
Three participants reported a somewhat negative experience with the repetition of following the eye movements, and one fell asleep during the EMI protocol and explained it as follows: "I actually fell asleep watching it, and I felt terrible!" (Participant 2). It was further concluded from two other participants that they needed a break during the protocol and needed a bit more of a challenge by stating that "at another stage I said: 'Okay I'm getting fed up now (laughing loud) … Because you know, it was repeating, repeating, repeating. So, I sort of went through all those kinds of emotions with it'"(Participant 8). Moreover, because of the number of repetitions required during the procedure, participant 10 inquired whether EMI had a hypnotic aspect. He added that he would not have minded, but the repetition of the eye movements made him wonder about it.
Despite these more negative experiences, the majority of the participants viewed the repetitiveness as a positive experience and indicated that it helped them to focus and concentrate. Participant 8 said "I found I was focusing...' and '...it made me concentrate ALL THE TIME." Participant 9 compared the intervention to brain gym that she used as a teacher in the classroom to help the children to focus and concentrate. She felt EMI was based on the same principle and she could therefore easily relate to it. She realised her work as a teacher impacted on the lives of those she had taught, which provided her with a sense of purpose. The EMI facilitated that aspect for her as an individual: "…so, this I think helped me to concentrate on me for a change and not worry about everything else" (Participant 9).
Beaulieu (2012) refers to the same idea when she mentions that work done by Bandler and Grinder (1979) demonstrated the connection between guided eye movements and thought processes when they could successfully assist children with their mathematics and spelling by merely redirecting the direction of the children's gaze.
Subtheme 1.4: Older people felt very tired afterwards
EMI requires a lot of physical and emotional energy from the client (Beaulieu, 2012), as was confirmed by the two participants who reported feeling tired the next day after receiving the intervention. Participant 1 indicated that "I actually felt tired the next day after we had our last session' and participant 6 stated that 'I was exhausted!... and I slept a lot...in the afternoon which I never do."
During an EMI session, a large amount of information will arise for the client. This causes much of their energy to be directed towards the physical symptoms and emotions they experience during the session and is the reason for feeling extremely tired after the session. Despite feeling tired, as soon as the troubling memory of the traumatic experience integrates, the client feels a sense of emotional release (Beaulieu, 2012).
From the above subthemes, it became evident that older people experienced an EMI intervention as an unfamiliar and unexpected technique. However, it impressed them as being useful for treating their symptoms of trauma, because of the results that it produced.
Theme 2: Suggestions for further use of EMI with older people
This theme reports on suggestions for further use of EMI with older people. It emerges from the participants' suggestions relating to adjustments/improvements to certain aspects that may result in a more beneficial experience to the integration of their trauma experience. Six subthemes were identified and are discussed below.
Subtheme 2.1: EMI is not complete in itself and should be part of a post-traumatic stress management package
Sadock et al., (2015) state that psychotherapy helps to improve older people's physical and mental symptoms. Cook, McCarthy and Thorp (2017) agree, but add that it does not guarantee a complete recovery from their symptoms of trauma. A valid point raised by one of the participants is that EMI is not complete in itself and suggested integrating it with another type of intervention like traditional counselling. For Beaulieu (2012), EMI is not a panacea intervention that replaces other trauma interventions, because there are aspects of human relations that cannot be changed by EMI. EMI helps the client integrate traumatic memories but does not result in a sudden change in behaviour present for an extended period.
In her assessment session, participant 5 reported that before receiving EMI, she developed destructive behaviours after the traumatic experience. The EMI enabled the participant to make the connection between her past and the present.
…the left side at where I had the blurry vision and the feeling of almost like stepping into water but not knowing where I'm going. That is how it felt, a bit spacy… he was on the left-hand side when I entered the room. And he was on the left-hand side, so obviously that was the impactful area which, I had never given thought to before. The other thing is I discovered at home that instead of sleeping on the left-hand side of the bed which I normally do, I have shifted to the right-hand side of the bed. So now there has been a conscious decision in that now that we have dealt with it, there has been a conscious decision to actually keep working at it… Never related it to the trauma… (Participant 5)
However, her experience with EMI did not help her to deal with the core issue of her trauma:
…the death of my son was dealt with… but the thing that was never dealt with was the anger that I had, because my youngest son found him… and that was where all my guilt lay… Did not lie in the death of my son. It laid in the situation that evolved after that. (Participant 5)
The possibility of dissociation should also be considered. Malmo and Laidlaw (2010) refer to this as a memory disturbance after exposure to extreme trauma. Struwig and Van Breda (2012) state that in this way a person detaches from their perception of time and reality, a survival mechanism that may, with time, become a habit and progress into a maladaptive or pathological process (Malmo & Laidlaw, 2010).
It was proposed by participant 5 that EMI should be practised in conjunction with a team of people, particularly when dealing with PTSD. Participant 4 also saw the potential and agreed that EMI has a place in dealing with PTSD by stating that "it's a technique that I would refer a lot of people to, to use. Especially with post-traumatic stress disorder"(Participant 4).
Participant 5 suggested that the client can start with a few counselling sessions to help them create awareness around their thought processes and emotions associated with those feelings. After that the individual can go for EMI. She further indicated that if it were to be the other way around, the client could be overwhelmed because they would not have thought carefully about the process.
…with the repetitiveness, you're repeating, but you're not... actually dealing with it… you do go home and do that but it's a self-realisation and unless you're good at looking at yourself you're going to sit back. That's how I would see it. You would slide back, uhm its purely because I felt that was an area that I needed to work on… (Participant 5)
EMI is a short-term intervention with a limited number of sessions. Due to the short-term nature of the intervention, EMI can be viewed as not complete on its own yet is has shown significant benefits.
Subtheme 2.2: The time frame between trauma and intervention has an important role in the outcome of the technique
The time between the traumatic experience and receiving the trauma intervention may be a significant factor to consider. Peterson (2021) proposes that older people can recall memories from their early childhood years which may cause unnecessary distress. Two participants specifically referred to the time frame between when the trauma occurred, and when the intervention was received and how this influenced the outcome for them. It is interesting to note that they had opposite views on this.
Participant 3 recommended that for EMI to be more effective, the trauma to be investigated should be recent rather than something that happened a long time ago. She then talked about how she dealt with her feelings over the years and stated that her memories are not that vivid anymore because the incident happened years ago. She said:
I'm looking at 50 years back. 51 years and so much has happened in that time. I don't think that the memories are quite as sharp… the things that upset me probably don't upset me quite as much anymore. It is more distant. It is more detached. So, there has definitely been work done. (Participant 3)
She then added that "I have made peace with a lot of it over the years, but maybe not those trigger words that she wrote down…" (Participant 3)
Another participant, however, advised that there is too much going on in the aftermath of the trauma. Therefore, participant 5 suggested that the victim should not go for EMI immediately and must first come to terms with the experience before receiving EMI. Beaulieu (2012) maintains that after exposure to trauma, coping mechanisms may be utilised to help avoid distress. The more time that passes, the more likely the avoidance behaviour becomes habitual behaviour. However, it is advised that EMI should also not be undertaken directly after the traumatic event, because the brain has a natural capacity to heal by itself. Instead, it may be best to start EMI at least a month after the trauma (Beaulieu, 2012).
Subtheme 2.3: EMI does not always show clear benefits
Two participants indicated that EMI does not always show clear benefits. The following points support this subtheme.
Firstly, the need for trauma debriefing is a relative concept. Participants 1 and 2 indicated that older people cope better because of their life experience. Participant 1 indicated that:
…It's life experience and the more life experience you have, I think… obviously the better you can cope with things.
The second point that was raised was that having someone listening to you in itself is also beneficial. Participant 1 indicated: 'I think anybody listening to you compassionately is beneficial…' The same participant further stated that survivors of the same trauma can support each other:
…I still get together with people who have lost their homes and talk about those things that you lost and share… you've got to be careful… of who you talk to because… a non-fire victim will sort of say… get over it already. But it's lovely to have friends who are in the same boat and that you can remember exactly how you felt.
This participant appears to have close relationships with a group of people who went through the same traumatic incident as she did and seems to find it helpful to share her experience with those people with whom she has this in common. Rutten, Hammels, Geschwind, Menne-Lothmann, Pishva, Schruers, Van Den Hove, Kenis, Van Os and Wichers (2013) indicate that close interpersonal relationships and support systems help people to get through difficult times more easily.
Subtheme 2.4: Proper orientation to the technique can be helpful
On completion of the assessment and ascertaining their suitability for EMI, the protocol of eye movement was explained before starting the intervention. However, four participants felt that they did not fully understand the technique and suggested that more comprehensive orientation to the intervention was necessary. Beaulieu (2012) highlights the importance of correctly explaining the technique to the client as part of the preparation and, where needed, repeating some information. This will ensure that the client has a complete understanding of the process, will feel more comfortable, and be more fully engaged.
The uncertainty surrounding the significance of the eye movements suggested that a few of the participants did not fully understand the protocol, even though it was explained to them. Participant 2 shared her experience by saying that the therapist:
…explained it to a point for me… having to look at that pencil and… why I had to do it… and I didn't fully understand it.
Two participants also indicated that they expected the therapist to read something from their eye movements. Participant 10 said:
... I thought she was reading something by my eye movements...I was expecting her to be looking into my eye movement… and reading something… so maybe I've misinterpreted that first part that she explained. The brain and how it works.
Another participant shared similar thoughts:
I didn't fully understand it, obviously she looks at your eyes and you want to know more about it... (Participant 2)
Despite the uncertainty, they became comfortable with the protocol, trusting the natural unfolding of the process. Participant 3 shared that:
…watching the pencil move in different sort of directions and patterns, I didn't quite understand the significance of that. But I could actually feel within me that certain things were being raised.
Participant 9 shared this view:
…she put it across very well, and she was very organised, and I thought it was quite beneficial to me… I was not sure what it was all going to be about, but once she started, I could see what she was trying to get to.
Participant 10 indicated:
…I don't quite understand the eye movement aspect of it, but the whole procedure, I enjoyed it and I think it helped me in acceptance of certain things.
It was suggested that a more in-depth explanation be provided concerning how EMI works to allay uncertainties, specifically focusing on the relevance of the eye movements as opposed to only explaining how the sensory modalities store trauma. Participant 2 suggested that the client receive reading material like an article to read after the assessment and before starting the intervention to gather more information about how it works.
Subtheme 2.5: Utilising neutral tools assist older people to focus during EMI
According to Van der Spuy (2014), the therapist should carefully consider the tool utilised in EMI to assist the client in following guided eye movements. Beaulieu (2012) suggests using two fingers or a marker pen, while Van der Spuy (2014) found finger puppets to be more useful in her study with children because they easily relate to them. In the sessions with all ten participants, the therapist utilised a specific pen with a picture of a face on the tip to assist them in following the eye movements.
During the assessment session, each client was asked if they were comfortable to proceed with the specific pen assisting them to follow the different movements. Only one of the participants experienced the focus instrument, in this case a pen with a face on it, as something that was not neutral and mentioned that she felt that it was a pen for a child. Participant 3 recommended that:
… the tool she uses should change. It should be something a little bit more serious or stylish or I don't know what.
Others were comfortable with the tool.
Subtheme 2.6: The therapist to take the lead in assisting the client to choose the right trauma
One participant indicated that she felt that she did not work on the main problem and would have liked the therapist to help her identify the underlying issue that needed to be addressed.
There's never ever just one thing. It's usually a series of events or something that's happened… for me perhaps the issue was not so much the death as it was perhaps the actual anger about what happened after that. (Participant 5)
During assessment, each client identified a troubling memory and decide which traumatic incident they would like to work through. If the client had experienced multiple traumas, it is essential to start with the first or worst traumatic event. In the case of one traumatic incident with a memory of many distinct images or fragments, the clinician assists the client to identify the most intense image with the highest emotional charge (Beaulieu, 2012). The next step is to describe how they remember it. The client described the event from his or her own perspective and in his or her own words as the traumatic event is recalled (Beaulieu, 2012). From this description, the client selects verbal cues (i.e. keywords or phrases) to help them remain focused on the incident. These cues must capture the troubling memory and remind the client of the traumatic incident (Struwig & Van Breda, 2012). Some traumas are multi-layered with multiple repercussions for the family as was the case for the participant above. Participant 5 continued by saying:
…yes, we have a choice to pick on certain things like what are your key factors, what are your key words and that. I do think there should be a suggestion from the person who's doing the assessment... because they can pick up things that, you can see where there's a problem.
Beaulieu (2012) explains that traumatised people experience different processes in recovering from and overcoming adversity. For some, recovery occurs more naturally than for others. Exposure to more than one trauma may result in experiencing shared emotions for both traumas. Often clients cannot realise the connection between the two traumas based on the facts. The clinician may become aware of some of the distressing thoughts and behaviours that the client experiences, while certain aspects remain hidden. Essentially, having worked through the first trauma, a strong emotional charge may remain concerning the residual unintegrated traumatic experiences. It is best to work towards addressing and integrating one disturbing memory at a time, suggesting that a few sessions may be necessary for multiple traumatic experiences. In this way, the link between the shared emotions and needs of the client should be revealed naturally as the process unfolds. Furthermore, successful integration of the first traumatic memory should lead the client to pursue further help for the remaining problems (Beaulieu, 2012). This seems to have been the case for Participant 5, who decided to pursue further counselling at her church after receiving EMI.
From the above, it can be concluded that there is a place for EMI when treating symptoms of trauma in older people if the necessary adjustments are made to better address the trauma for individuals in this age group. These suggestions made by the participants should be considered and are of great value to improve EMI as a trauma intervention when working with older people.
DISCUSSION AND CONCLUDING REMARKS
Since later life is a time of physical and/or mental deterioration (Stuart-Hamilton, 2011), older people especially are a more vulnerable age group in terms of their health and wellbeing, with social workers often involved in their lives (Dye, 2018). With life expectancy predicted to lengthen in the future (Bürgin et al., 2020), it is vital for social workers to understand what enables wellbeing and promotes healthy ageing.
This paper is concerned with older people's personal experience of EMI as a treatment modality for treating their symptoms of trauma. With a lack of knowledge about effective intervention strategies for treating trauma in older persons, this study set out to address this need. EMI is different from other types of interventions such as traditional counselling because it has an element of neurologically based intervention that is not included in typical talk interventions (Struwig & Van Breda, 2012). Instead, taking note of one's inner processes rather than analysing them is applicable.
Older people in this study found EMI beneficial in dealing with trauma, despite it being a new experience. Suggestions are made that it can also work in a complementary way with other trauma interventions. Older people who used EMI and participated in this study made valuable suggestions for practitioners to consider when working with their age group. It is recommended that more research be conducted to broaden the knowledge base of EMI as intervention for older people. Older people should be seen as key informants and social work and other health profession researchers should draw from their experiences to enhance the protocols used in this age category. As a short-term intervention, EMI can be a cost-effective modality when working with older people.
REFERENCES
AMERICAN PSYCHIATRIC ASSOCIATION. 2013. Diagnostic and statistical manual of mental disorders - DSM-5. 5th ed. Washington DC: American Psychiatric Association. [ Links ]
ARPINO, B., GUMÀ, J. & JULIÀ, A. 2018. Early-life conditions and health at older ages: The mediating role of educational attainment, family and employment trajectories. PLOS ONE, Public Library of Science, 13(4):1017. [ Links ]
BANDLER, R. & GRINDER, J. 1979. Frogs into princes: Neuro-linguistic programming. Utah: Real People Press. [ Links ]
BEAULIEU, D. 2003. Efficacy of eye movement integration therapy: A novel therapy for rapid, ecological integration of traumatic memories. [Online] Available: http://www.academieimpact.com/pdf/EMI_article2.pdf [Accessed: 7/09.2020]. [ Links ]
BEAULIEU, D. 2005. An introduction to eye movement integration therapy. European Journal of Clinical Hypnosis, 6(3):2-11. [ Links ]
BEAULIEU, D. 2012. Eye movement integration therapy: The comprehensive clinical guide. Wales: Crown House Publishing. [ Links ]
BÖTTCHE, M., KUWERT, P. & KNAEVELSRUD, C. 2012. Posttraumatic stress disorder in older adults: an overview of characteristics and treatment approaches. International Journal of Geriatric Psychiatry, March, 27(3):230-239. [ Links ]
BROWN, E. J., COHEN, J. A. & MANNARINO, A. P. 2020. Trauma-focused cognitive-behavioral therapy: The role of caregivers. Journal of Affective Disorders, 277:39-45. [ Links ]
BÜRGIN, D., BOONMANN, C., SCHMID, M., TRIPP, P., & O'DONOVAN, A. 2020. Fact or artefact? Childhood adversity and adulthood trauma in the U.S. population-based health and retirement study. European Journal of Psychotraumatology, 11:1-14. [ Links ]
COOK, J. M., McCARTHY, E. & THORP, S. R. 2017. Older adults with PTSD: Brief state of research and evidence-based psychotherapy case illustration. American Journal of Geriatric Psychiatry, 25(5):522-530. [ Links ]
DAVIDSON, D. J. 2018. Evaluating the effects of living with contamination from the lens of trauma: a case study of fracking development in Alberta, Canada. Environmental Sociology, 4(2):196-209. [ Links ]
DEPARTMENT OF SOCIAL DEVELOPMENT (DSD). 2017. Old age pension: Older persons grant. [Online] Available: https://www.westerncape.gov.za [Accessed: 15/10/2020]. [ Links ]
DYE, H. 2018. The impact and long-term effects of childhood trauma. Journal of Human Behavior in the Social Environment, 28(3):381-392. [ Links ]
ELDER, G. H. Jr., JOHNSON, M. K. & CROSNOE, R. 2003. The emergence and development of life course theory. In: MORTIMER, J. T. & SHANAHAN, M. J. (eds.). Handbook of the life course. New York: Kluwer Academic/Plenum Publishers. [ Links ]
FROST, R., NAIR, P., AW, S., GOULD, R. L., KHARICHA, K., BUSZEWICZ, M. & WALTERS, K. 2019. Supporting frail older people with depression and anxiety: a qualitative study. Aging & Mental Health, doi: 10.1080/13607863.2019.1647132. [Online] Available: https://doi.org/10.1080/13607863.2019.1647132 [Accessed: 7/09/2020]. [ Links ]
FULMER, T., REUBEN, D. B., AUERBACH, J., FICK, D. M., GALAMBOS, C. & JOHNSON, K. S. 2021. Actualizing better health and health care for older adults: Commentary describes six vital directions to improve the care and quality of live for all older as. Health Affairs, 40(2):219-225. [ Links ]
GELDENHUYS. K. 2017. Climate change and disasters - is South Africa ready?. Sabinet African Journals, 110(10). doi: 10.10520/EJC-9dd2c89c4. [Online] Available: https://hdl.handle.net/10520/EJC-9dd2c89c4 [Accessed 22/07/2021]. [ Links ]
HENDRICKS, J. 2012. Considering life course concepts. The Journals of Gerontology: Series B: Psychological Sciences and Social Sciences, March, 67B (2):226-231. [ Links ]
HISKEY, S. & McPHERSON, S. 2013. That's just life: Older adult constructs of trauma. Ageing Mental Health, 17(6):689-696. [ Links ]
KAISER, A. P., SELIGOWSKI, A., SPIRO III, A. & CHOPRA, M. 2016. Health status and treatment-seeking stigma in older adults with trauma and posttraumatic stress disorder. VA Health Care, 53(3):391-402. [ Links ]
KELLY, G., MRENGQWA, L. & GEFFEN, L. 2019. "They don't care about us": older people's experiences of primary healthcare in Cape Town, South Africa. BMC GERIATRICS, 19(98):2-14. [ Links ]
KIM, E. J., PELLMAN, B. & KIM, J. J. 2015. Stress effects on the hippocampus: A critical review. Learning and Memory, 22:411-416. [ Links ]
LELY, C. G., SMID, G. E., JONGEDIJK, R. A., KNIPSCHEER, J. W. & KLEBER, R. J. 2019. The effectiveness of narrative exposure therapy: A review, meta-analysis and meta-regression analysis. European Journal of Psychotraumatology, 10:1-13. [ Links ]
LENFERINK, L. I. M, PIERSMA, E., DE KEIJSER, J., SMID, G. E. & BOELEN, P. A. 2017. Cognitive therapy and eye movement desensitization and reprocessing for reducing psychopathology among disaster-bereaved individuals: study protocol for a randomized controlled trial. European Journal of Psychotraumatology, 8(1):1-9. [ Links ]
LEVINE, P.A. 2015. Trauma and memory: Brain and body in a search for the living past. Berkeley: North Atlantic Books. [ Links ]
LEWEY, J. H., SMITH, C. L., BURCHAM, B. SAUNDERS, N. L., ELFALLAL, D. & O'TOOLE, S. K. 2018. Comparing the effectiveness of EMDR and TF-CBT for children and adolescents: a meta-analysis. Journal of Child & Adolescent Trauma, 11:457-472. [ Links ]
LINDWALL, M., BERG, A. I., BJÄLKEBRING, P., BURATTI, S., HANSSON, I., HASSING, L., HENNING, G., KIVI, M., KÖNIG, S., THORVALDSSON, V., & JOHANSSON, B. 2017. Psychological health in the retirement transition: Rationale and first findings in the health, ageing and retirement transitions in Sweden (HEARTS) study. Front. Psychol, 8(1634): 1-13. [ Links ]
MALMO, C. & LAIDLAW, T. S. 2010. Symptoms of trauma and traumatic memory retrieval in adult survivors of childhood sexual abuse. Journal of Trauma & Dissociation, 11(1):22-43. [ Links ]
MCDANIEL, S. & BERNARD, P. 2016. Life course as a policy lens: Challenges and opportunities. Canadian Public Policy / Analyse de Politiques, (37): S1-S13. [ Links ]
O'DOWD, M. 2014. Is South Africa a third world country? [Online] Available: http://www.freemarketfoundation.com/article-view/is-south-africa-a-third-world-country [Accessed: 12/08/2020]. [ Links ]
OGLE, C. M., RUBIN, D. C. & SIEGLER, I. C. 2014. Cumulative exposure to traumatic events in older adults. Ageing Mental Health, 18(3):316-325. [ Links ]
OLOFSSON, N. 2014. A life course model of self-reported violence exposure and ill-health with a public health problem perspective. AIMS Public Health, 1(1):9-24. [ Links ]
OSBORNE, J. W. 2012. Psychological effects of the transition to retirement. Canadian Journal of Counselling and Psychotherapy, 46(1): 45-58. [ Links ]
PETERSON, C. 2021. What is your earliest memory? It depends. Memory, 29(16):811-822. [ Links ]
POLLIO, E. & DEBLINGER, E. 2017. Trauma-focused cognitive behavioural therapy for young children: clinical considerations. European Journal of Psychotraumatology, 8(7):1-8. [ Links ]
ROLLER, M. R. 2019. A quality approach to qualitative content analysis: similarities and differences compared to other qualitative methods. Forum: Qualitative Social Research Sozialforchhung, 20(3):Art.31. [ Links ]
RUBIN, A. 2014. EMDR treatment for trauma. Clinical and Direct Practice, Health Care and Illness. doi: 10.1093/acrefore/9780199975839.013.908. [Online] Available: https://oxfordre.com/socialwork/view/10.1093/acrefore/9780199975839.001.0001/acrefore-9780199975839-e-908?print=pdf [Accessed 22/07/2021]. [ Links ]
RUBIN, A. & BABBIE, E. 2005. Research methods for social work. 5th ed. Australia: Thomson Books/Cole. [ Links ]
RUTTEN, B. P. F., HAMMELS, C., GESCHWIND, N., MENNE-LOTHMANN, C., PISHVA, E., SCHRUERS, K., VAN DEN HOVE, D., KENIS, G., VAN OS, J. & WICHERS, M. 2013. Resilience in mental health: linking psychological and neurobiological perspectives. Acta Psychiatrica Scandinavica, July, 128(1):3-20. [ Links ]
SADOCK, B. J., SADOCK, V. A. & RUIZ, P. 2015. Synopsis of psychiatry: Behavioral sciences/clinical psychology. 11th ed. New York: Wolters Kluwer Publishers. [ Links ]
SANDELOWSKI, M. 2000. Focus on research methods. Whatever happened to qualitative description? Research in Nursing & Health, 93:334-340. [ Links ]
SOUTH AFRICAN GOVERNMENT. 2021. Old age pension. [Online] Available: https://www.gov.za/services/social-benefits-retirement-and-old-age/old-age-pension [Accessed: 22/07/2021]. [ Links ]
STRUWIG, E. & VAN BREDA, A.D. 2012. An exploratory study on the use of eye movement integration therapy in overcoming childhood trauma. Families in Society: The Journal of Contemporary Social Services, 93(1):29-37. [ Links ]
STUART-HAMILTON, I. 2011. The psychology of ageing: an introduction. 4th ed. London & Philadelphia: Jessica Kingsley Publishers. [ Links ]
SWEDBERG, R. 2020. Exploratory Research. In: Elman, C., Gerring, J. & Mahoney, J., (eds.). The production of knowledge. Cambridge: Cambridge University Press. [ Links ]
UNITED NATIONS, DEPARTMENT OF ECONOMIC AND SOCIAL AFFAIRS (UN DESA), POPULATION DIVISION. 2019. World population ageing 2019: Highlights (ST/ESA/SER.A/430). [Online] Available: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf [Accessed 22/07/2021]. [ Links ]
VAN DER SPUY, C. 2014. Treating trauma in early childhood by utilising eye movement integration therapy. Johannesburg : University of Johannesburg. (Master's thesis) [ Links ]
VAN DER SPUY, C., & VAN BREDA, A. D. 2018. An exploratory study on the use of eye movement integration therapy for treating trauma in early childhood in South Africa. Child Care in Practice, 25(2):157-174. [ Links ]
WATKINS, L. E., SPRANG, K. R. & ROTHBAUM, O. 2018. Treating PTSD: a review of evidence-based psychotherapy interventions. Frontiers in Behavioural Neuroscience, 12(258):1-9. [ Links ]
 Correspondence:
Correspondence:
Andrea Visagie
info@beatingtrauma.co.za
Annaline Keet
Annaline.Keet@mandela.ac.za


{kind=link}
{kind=link}
{kind=link}