










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.55 n.1 Stellenbosch 2019
http://dx.doi.org/10.15270/55-1-695
ARTICLES
The needs of caregivers of bipolar patients
Ilse Annemarie van der Walt; Charlene Laurence Carbonatto
Department of Social Work & Criminology, University of Pretoria, Pretoria, South Africa. Charlene.Carbonatto@up.ac.za
ABSTRACT
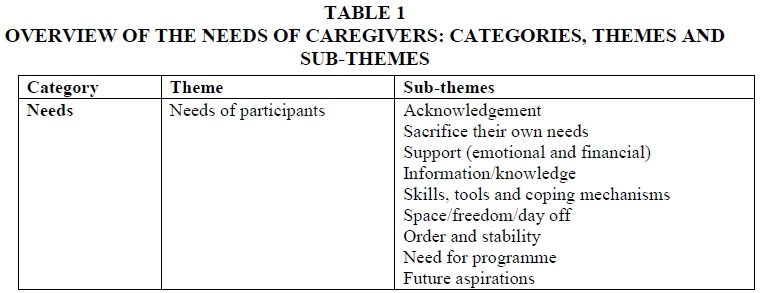
Bipolar disorder (BD) is a mental health disorder that affects not only the person living with this chronic disease, but also the family and caregiver. Caregivers, often family members, do not realise how caregiving will impact on them and the rest of the family, until they experience it first-hand. This qualitative study used a collective case study and one-to-one interviews. Non-probability purposive sampling was used with selection criteria. One of the themes generated from the study was the needs of caregivers of patients with BD. Sub-themes included: acknowledgement, sacrificing their own needs, support (emotional and financial), information/knowledge, skills, tools and coping mechanisms, space/freedom/day off, order and stability, need for a programme and future plans. It was found that it is essential to address the needs of caregivers.
INTRODUCTION
Bipolar disorder (BD) is a highly complex, chronic, relapsing and heterogeneous psychiatric condition characterised by both a variety of symptoms and marked variability in course (Michalak, Murray, Young & Lam, 2010:254; Colom & Vieta, 2006:3). Patients, their families and society tend to oversimplify this psychiatric condition. It is associated with a considerable degree of illness-related morbidity, profound suffering, occupational impairments and social burdens (Goossens, Van Wijngaarden, Knoppert-Van der Klein & Van Achterberg, 2008:303). Hayden and Nürnberger (2006:69) add that the frequent manifestation of BD, in conjunction with suicidality, psychiatric comorbidity and pronounced impairment in psychosocial functioning, exacts a great toll on patients and their families. Even with adequate treatment by way of a mood stabilizer, one-third of bipolar patients relapse within 3 years.
Comparable to many chronic illnesses, BD afflicts one person but affects many in the family. It is important that all those affected, especially the caregiver, receive the help, support and encouragement they need (Mondimore, 2006:258). Caregivers have a broad range of needs, which will be discussed below, but if these are not met, caregiver burden can occur. Caregiver burden can be experienced by the impact of the mental illness of one family member on the emotional wellbeing of other family members and on the family members' use of time and general living conditions. Ogilvie, Morant and Goodwin (2005:25).
Dore and Romans (2001:48) found that studies on how family factors influence the outcome in BD are scarce, while (Ogilvie et al, 2005:25) explain that despite the extent of the impact of BD, very little work has been done to define more precisely the caregiver's burden associated with this illness. Thus the goal of this study was to conduct an exploratory descriptive study of the needs and challenges of the caregivers of individuals diagnosed with BD. The research question was: What are the needs and challenges of the caregivers of individuals diagnosed with BD?
The study on caregivers by Terkelsen (1987a: 128) hits the nail on the head; when a caregiver was asked in an interview: "What have you missed most as a result of having a mentally ill relative at home with you? " The participant answered: "My life ".
RESEARCH METHODS
This applied study was explorative and descriptive in nature, adopting a qualitative approach that used qualifying words and descriptions to record aspects of the world of the caregiver, providing a sensitive and meaningful way of recording human experiences (Bless, Higson-Smith & Kagee, 2006:43, 44).
The case study design provided a deeper understanding of the needs and challenges of caregivers of individuals diagnosed with BD (Nieuwenhuis, 2007a:75), while a collective case study design (Fouché and Schurink, 2011:322) furthered this understanding using various caregivers of patients with BD from private and public health contexts. Semi-structured interviews were conducted, organised around areas of particular interest, which May (in Greeff, 2005:292) refers to as allowing considerable flexibility in scope and depth, thus gaining a rich understanding of their world and appreciating it from their perspective. An interview schedule guided the interviews, exploring caregivers' needs, challenges, lack of skills and knowledge, as well as their possible strengths.
Non-probability purposive sampling included the following selection criteria: caregivers of adult people diagnosed with BD and who must have had the BD diagnosis for at least three months; the caregivers must have been aware of the diagnosis as well as conversant in either English or Afrikaans; they must have expressed the need for more knowledge and skills regarding BD, and could be of either gender, a parent, child, sibling, spouse, partner, colleague or close friend and living with the patient. Participants were generated from three sources: a bipolar support group in the community, patients of a psychiatrist in private practice, and patients at a public health psychiatric hospital. Information letters were used to recruit participants and those interested gave their contact details to the professional involved. They were contacted and appointments for an interview were made, if they met the selection criteria. The interviews commenced once they signed the letter of informed consent and were voice recorded with their permission. Data saturation was reached after interviewing eleven participants. The interviews were transcribed verbatim.
Qualitative data analysis was used to analyse the perceptions, attitudes, understanding, knowledge, values, feelings and experiences of the participants in an attempt to describe their needs, challenges, lack of skills and knowledge, as well as their possible strengths (Nieuwenhuis, 2007b:99). The steps of qualitative data analysis by Cresswell (in Schurink, Fouché & De Vos, 2011:402- 419) guided the analysis through planning for recording of data, data collection and preliminary analysis, managing (organising) data, reading and writing memos, generating categories, themes, patterns and coding the data, testing emergent understandings and searching for alternative explanations, interpretation and developing typologies (systems for categorising concepts), and presenting the data. Clear repetition of themes and sub-themes through all the transcribed interviews occurred, especially with the caregivers who were children or wives of patients.
The quality of the data was ensured through enhancing its trustworthiness, which Nieuwenhuis (2007b: 113) describes as the acid test of one's data analysis, findings and conclusions. Strategies for this included reflexivity, member and credibility checks and peer reviewing, and using the constructs of trustworthiness, namely credibility, conformability, transferability and dependability.
Ethical approval was obtained from the relevant authorities, as well as permission to conduct the study from the applicable support group facilitator, psychiatrist and CEO of the psychiatric hospital. Strydom's (2011:115-126) classification of ethical considerations included voluntary participation, informed consent, confidentiality through using numbers as pseudonyms for each participant to protect their identity, debriefing of participants after the interview, avoidance of harm throughout, with only one participant referred to a colleague social worker for counselling after the interview.
LITERATURE REVIEW
The theoretical framework underpinning this study is firstly the integrated biopsychosocial model, which reminds one that a caregiver must be viewed as a person whose psyche and soma (mind and body) are affected in his/her role of being a caregiver of somebody with BD. Secondly, the ecological systems perspective, based on systems theory, was also used, as it is crucial to view the patient as part of a complex ecological system and not as an isolated entity. The ecosystem is a system of systems, including the individual, family, sociocultural environment and the therapeutic systems (Surdut, 1998:440). The mental health of the individual is interdependent with the ecological health of the larger nationwide system (Smith, 2007:654). From an ecological perspective, the context within which the individual functions is crucial and helps the clinician to identify the sources of stress and contributing events (Surdut, 1998:440). The integrated biopsychosocial model, within an ecological systems perspective, served as the point of departure from which this research was conducted.
Bipolar disorder
The National Institute of Mental Health report (ΝΓΜΗ, 2010:2) states that BD is a brain disorder that causes unusual shifts in mood, energy, activity levels and the ability to carry out day-to-day tasks that must be carefully managed throughout a person's life. The American Psychiatric Association (2000:383-401) defines BD as a severe, chronic, almost invariably recurrent, mood (affective) disorder, which is a relapsing illness, characterised by episodes of mania or hypomania, alternating with episodes of depression.
The DSM 5 American Psychiatric Association (APA, 2013:123-154) differentiates between:
• Bipolar I disorder: It is necessary to meet criteria for a manic episode. The manic episode may have been preceded by and may be followed by hypomanic or major depressive episodes.
• Bipolar II disorder: It is necessary to meet criteria for a current or past hypomanic episode and criteria for a current or past major depressive episode.
• Cyclothymic disorder: The essential feature is a chronic, fluctuating mood disturbance involving numerous periods of hypomanic symptoms and periods of depressive symptoms that are distinct from each other. During the initial 2-year period the symptoms must be persistent and any symptom-free intervals should last no longer than 2 months.
• Substance/medication-induced bipolar and related disorder: The diagnostic features are essentially the same as those for mania, hypomania or depression, but substances/medication play a role in inducing BD.
• Bipolar and related disorder due to another medical condition: The essential features are the presence of a prominent and persistent period of abnormally elevated, expansive or irritable mood and abnormally increased activity or energy predominating in the clinical picture that is attributable to another medical condition.
• Other specified bipolar and related disorder: This applies to presentations in which symptoms characteristic of a bipolar and related disorder that cause clinically significant distress or impairment in social, occupational or other important areas of functioning predominate, but do not meet the full criteria for any of the disorders in the bipolar and related disorder diagnostic class.
• Unspecified bipolar and related disorder: This category is the same as above, but is used in situations in which the clinician chooses not to specify the reason the criteria are not met, and includes presentations in which there is insufficient information to make a more specific diagnosis (e.g. in emergency room settings).
DSM 5 (APA, 2013) specifiers for bipolar and related disorders include: anxious distress, mixed features, rapid cycling, melancholic features, atypical features, psychotic features, with catatonia, peri-partum onset and seasonal patterns. It should also be specified if the illness is in partial or full remission and whether the current severity thereof is mild, moderate or severe.
Aetiology/causative factors of bipolar disorder: theories and perspectives
BD is not "only a brain disease" or "only a psychological problem" (Miklowitz, 2011:75), but it can be both of these things. Most professionals think of the cycling of BD as reflecting a complex interplay among the following factors:
• Genetic vulnerabilities: inheriting a propensity for the disorder from one or more blood relatives;
• Biological agents: abnormal functioning of brain circuits involving neurotransmitters such as dopamine;
• Psychological agents: such as one's beliefs about relationships;
• Stress agents: either events that bring about positive or negative changes, such as transitions in a living situation or job or more chronic problems, for instance, severe family conflicts or taking care of someone who is seriously ill.
Berk, Berk, Castle and Lauder (2008:93) sum this up: "Rather than a single pathway to illness, an interaction between biology as an underlying vulnerability, and a variety of stressors as triggers, may result in an episode of illness for a particular individual".
Holistic treatment of bipolar disorder by the multidisciplinary team (MDT)
BD is a biological illness that deserves proper pharmacological treatment (Colom & Berk, 2010:412; Kilbourne, Goodrich & Bauer, 2010:453). Medication is the first-line of treatment for BD and treatment without appropriate medication is doomed (Miklowitz, 2011:98; Taylor, 2006:15). Both Miklowitz (2011:100) and Vieta (2009:50,52) distinguish between an acute phase (during which the goal is to treat and stabilise the existing illness episode, especially for patients in the manic/hypomanic phase, with the goal of remission) and a maintenance phase, when the goal is to prevent future episodes.
Psychiatric treatment of BD is complicated by the fact that patients vary with respect to the uniqueness of their symptoms, life circumstances and comorbid psychiatric issues. The foundation of treatment for BD is pharmacotherapy, but it has long been recognised that most individuals either achieve only partial symptom control with medication or struggle to adjust to the consequences of developing a "life course illness". Berk et al. (2008:93) observe that a growing body of evidence supports the use of psychological interventions in conjunction with medication in the treatment of BD.
Keck, McElroy and Hawkins (2010:289) are of the opinion that electroconvulsive therapy (ECT) remains an important non-pharmacological treatment option for patients who do not respond well to or tolerate pharmacotherapy or who have severe, psychotic or catatonic symptoms. This treatment, however, remains controversial.
There are numerous treatments for BD (Miklowitz, 2011:132), none of which is perfect, but they can effectively treat a person's acute symptoms and in all likelihood level out the course of his/her illness over time. Adding psychotherapy or support groups to a medication regimen helps to ensure that the person is treated, not just the disorder, and that he or she develops strategies for coping with stress. The selection of therapies ought to be based on patient needs and preferences. As BD may be progressive when episodes accumulate, it may be relatively more responsive to interventions early in the course of illness. Efforts to engage patients early on in the treatment alliance are particularly important (Parker & Ketter, 2010:349, 350).
The mental health social worker is an essential member of the MDT, responsible for assessment and providing these therapies, including psychotherapy and psycho-education. Trials have indicated that social work is at least as effective as psychological or pharmacological approaches to mental health problems. However, the evidence base for social interventions that are at the disposal of mental health social workers is small, incomplete and disproportionate in size to that available to psychologists or psychiatrists (Webber, 2010:108, 111). In the South African context, psychiatric services are still fragmented and it is often the mental health social worker in the MDT who becomes the link to the community resources and even the coordinator of services within the MDT. If the rest of the team is 'stuck', the patient's problem often becomes a 'social' issue and other team members may become frustrated with the lack of progress.
As hospitalisation of psychiatric patients has become increasingly brief (nationally and internationally) and as patients are discharged in quite unstable clinical states, the burden on the caregivers has become considerable. In this environment caregivers need support, education and advice in coping with the patient's ups and downs (Miklowitz & Goldstein, 1997:5).
Vieta (2009:50, 52) emphasises the importance of establishing and maintaining a therapeutic alliance. Treatment should be based on a collaborative relationship with the patient and family. It is clear that an integrated, holistic approach is essential. It has been observed that the MDT focuses mainly on the patient, whereas the partners, families or caregivers are often neglected. An important role of the mental health social worker in a psychiatric hospital is to reach out specifically to the significant others, because they are the secondary sufferers of the mental illness. If their needs are addressed, the patient also benefits. How well families do in the face of a severe mental illness may depend to a significant extent on how well their needs for support are met (Hatfield, 1987b: 191).
Caregivers and caregiver burden
A caregiver can be considered as any lay person who cares about and is in frequent contact with the person diagnosed with BD. Caregivers of people who have been diagnosed with BD have certain emotional reactions to the illness, but also certain needs that pose definite challenges. These needs can include developing an ability to deal with their own emotions in relation to the illness, to be educated about the BD and. most importantly, a need for knowledge. The emotions, needs and challenges will differ, depending on the role of the specific caregiver in the system. One important psychosocial area to investigate is the patient's interpersonal environment (Lam, Donaldson, Brown & Malliaris, 2005:431). The patient must be observed within the context of his or her interpersonal environment and the stressors within this environment. The caregiver is part and parcel of the patient's environment.
Ostacher, Nierenberg, Losifescu, Eidelman, Lund, Ametrano, Kaczynski, Calabrese, Miklowitz, Sachs and Perlick (2008:50) suggest the following criteria for identifying the primary caregiver (caregiver must meet at least three of these criteria): he/she should be a spouse, parent or spouse equivalent; have the most frequent contact with the patient; help to support the patient financially; most frequently been a collateral in the patient's treatment; and/or be the one to be contacted by treatment staff in case of an emergency. A caregiver can also be a child of the person diagnosed with BD.
Caregiver burden is described as the presence of problems, difficulties or adverse events which affect the life (lives) of the psychiatric patient's significant other(s), e.g. members of the household and/or the family, although significant others can be considered to include close and supportive friends. In addition to the adverse effects of caregiving on the caregivers themselves, caregiver burden has been correlated with poorer clinical outcomes for patients (Colom & Vieta, 2006:20; Ostacher et al, 2008:50).
Caregivers' perceptions of stigma also contribute to caregiver burden and perceived stigma may represent a greater source of distress to caregivers than has previously been recognized (Perlick, Rosenheck, Clarkin, Maciejewski, Sirey, Struening & Link, 2004:1031, 1034). The stigma associated with mental illness has been found to increase the burden on caregivers (Van der Voort, Goossens & Van der Bijl, 2007:683), and people in the surrounding community appear to devalue patients with a mental illness, as do their caregivers.
Family, caregivers and needs
The ways in which families respond to mental illness varies as a function of time. Any response undergoes its own patterned temporal development, a pattern that transcends individual differences in response disposition (Terkelsen, 1987b: 151). Terkelsen (1987b:152-164) mentions the following stages: ignoring what is coming, the first shock of recognition, stalemate, containing the implications of illness, transformation to official patient status, the search for causes, the search for treatment, the collapse of optimism, surrendering the dream, picking up the pieces.
Belardinelli, Hatch, Olvera, Fonseca, Caetano, Nicoletti, Pliszka and Soares (2008:299) are of the opinion that BD is a familial disorder which is influenced by genetic and environmental factors. Among the environmental factors considered as most important is the family environment. Previous studies link a disordered family environment with a poor prognosis for BD. Mondimore (2006:225) and Aiken (2010:121, 125) agree and refer to the fact that BD does not affect just the individual with the diagnosis of the illness. Inevitably, family and friends are affected in countless ways, both directly and indirectly. When a family member has BD, the illness may profoundly affect the whole family. It is a sad fact, but BD not only destroys the mind; unfortunately, due to lack of understanding, it can also destroy the dynamics of relationships.
Lefley (1987:52) refers to the necessity of what cross-cultural researchers call the "emic" approach; that is, the outsider must learn to perceive the situation through the eyes of the subject, rather than superimposing his or her own external model of reality. This involves learning the family's experience of the illness, their theories about causes and their views of roles. Rather than observing a putatively maladaptive "system" through the lenses of theory, the therapist helps the family build survival skills within the framework of their expressed needs. In this study it was also very important to discover the real needs of the caregivers.
In 1979 the seminal study by Hatfield assessing the needs of families of mentally ill patients (Hatfield, 1987a:21) found the following needs were most prominent:
• Assistance in understanding the patient's symptoms;
• Specific suggestions for coping with patient's behaviour;
• Opportunities to relate to persons with similar experiences;
• Substitute care for family respite;
• A different living situation for the patient.
If the professional is aware of these needs, there is a better chance that unrealistic expectations will not be placed on the caregivers and that professionals too will have more tolerance towards the demands presented by caregivers.
RESEARCH FINDINGS
Profile of participants
Participants in the collective case study encompassed a wide spectrum of people:
• Ages of caregivers varied from 24 years to 58 years, while those of the patients ranged from 24 years to 60 years;
• Gender and ethnicity: caregivers were mainly females (9), with only 2 males; while patients were mainly males (6) with only 3 females; caregivers and patients were from diverse ethnic groups;
• Education: All the participants were well educated and held good jobs;
• Marital status: 1 husband and 4 wives.
It is argued that women perform the role of caregiver better, although this would be a generalisation. Children are severely affected by a mentally ill parent - even when they are adults. This was clear when the children of mentally ill persons reflected on their lives. The parent participants were all mothers and their unconditional love for their children was clear. There were two families involved in the study where the wife and child of the patient were interviewed, providing different perspectives.
Thematic analysis
The category needs, with the theme needs of participants and sub-themes derived from the transcribed interviews, is presented in Table 1. These are supported by narrative verbatim quotes from the interviews and literature to substantiate the findings.
Theme: Needs of participants
As suggested by Ogilvie et al. (2005), there is a need to understand caregivers' views and perceptions of the stresses and demands arising from caring for someone with BD in order to develop practical, appropriate and acceptable interventions and to improve the training of professionals working with bipolar patients and their caregivers. This theme contains nine sub-themes.
Sub-theme 1: Acknowledgement
This sub-theme is reflected in the participants' comments below.
"I think that is why I am so glad that you are doing this study because it sounds "egosentries "/egocentric, but it is like there is always such a lot of focus on this person with bipolar, always about helping him and how can you support your husband. But what about the person, do you think that is just superwoman or super husband standing there? "
"There is always such a lot of focus on the person with the illness that people just tend to forget what about the people around them. "
Participants felt that the patient always receives all the attention and that the caregiver is often ignored. They put the patient's interests above their own.
Sub-theme 2: Sacrificing one's own needs
The participant comments below reflect this sub-theme.
"That is it, I didn't care about myself I don't, if it happens tomorrow, I will again not care about myself I will just want her to be better and to be OK. "
"I have not bought a new pair of "tekkies/sneakers" in four years. Her needs are more important than mine. Hers are much more intense than mine. "
Caregivers must remember their own needs, should share responsibilities with others and stop BD from taking over family life Centre for Addiction and Mental Health (CAMH, 2000:39). This effect of this illness may lead to the carer losing his/her social life, which in turn may make him/her feel extremely lonely and isolated. Supporting a person with BD who is very ill may prove exhausting, often to the point where a person might neglect their own needs (Aiken, 2010:121).
Sub-theme 3: Support (emotional and financial)
The participant comments below support this sub-theme.
"So sometimes I bottle it up and then it gets too bad. At times I feel just that I could go and talk to somebody who knows precisely how I am feeling, who has got the same, who knows precisely how a person with BD or depression works, or who can give me practical advice on how to sort out my own feelings. I don't know and you sort offeel, where am I going now? "
"At that stage I just felt I had it. I just had enough of being the strong one all the time, being the mother andfather of this child and know that I don't have any support at that stage of any emotional or yes the financial means of an income, but the emotional support I really needed more at that stage. "
It is evident from these quotes that caregivers need support on different levels. Families need opportunities to relate to persons with similar experiences. How well families do in the face of a severe mental illness may depend to a significant degree on how well their needs for support are met (Hatfield, 1987a:21, 1987b:191).
Sub-theme 4: Information/knowledge
The following participant comments reflect this sub-theme.
'Absolutely, anything that I could get or absorb to use and to make her quality of life better. Actually I will grab them with both hands for sure. "
"It is just if I had a little black book in my pocket that's got a couple of answers that I don't have, maybe I will say things that will help her. The little book doesn't exist but that would have been nice. "
"There are things I don't know, that I don't know, that I don't know them ".
Participants' need for initial and ongoing psychoeducation on a practical, understandable level was indicated. They also need to know how to access information. Families need to know about their relative's illness if they are to be informed consumers and expected to help the recovering individual (McElroy, 1987:227). Family members of people with BD are usually hungry for information about the disorder, particularly during or after a manic or depressive episode, whether or not the episode involves hospitalisation. Relatives may harbour many misconceptions about the illness. Well-meaning relatives who do not understand the disorder may view drug treatment or psychotherapy as crutches. They should understand that at least a portion of the patient's behaviour is biologically and chemically determined (Miklowitz, 2011:5, 283, 284, 286). It is important that everyone in the family learns as much about the illness as possible in order to know what they are dealing with (Aiken, 2010:121).
Sub-theme 5: Skills, tools and coping mechanisms
The participant comment below supports this sub-theme.
"I want some help, to say to me what I should do in these circumstances. I need to have the correct way of how to deal with it and I think I will never have enough knowledge to see what am I supposed to do and not to do and to have 'die sekerheid'/the surety of what I am doing is alright. And Ifind that it is more practical for me if somebody tells me I did this and this. "
Participants were unsure of what to do - sometimes not realising that there is no recipe. Caregivers do have a need for skills such as how to communicate with the ill BD patient or what to do if the patient becomes suicidal, as well as other coping skills.
Sub-theme 6: Space/freedom/day off/respite
The participant comment below reflects this sub-theme.
"But I get my four to five hours on a Sunday. That is what our agreement is. I am very glad that she is offering me that time. I think if she wasn't offering me that time, it wouldn't have gone the way it is going now. It would have been a big issue because I can't be there 24/7. I can't. I have got my outlet, four hours on a Sunday that is a little bit of an outlet. "
It became clear that caregivers need some time away from the caring situation.
Sub-theme 7: Order and stability
The following comment reflected the participant's need for order and stability.
"I really don't know. If he just was stable. At the moment the only way I see that stability will come is when he is not around. But where does he go? "
Caregivers long for stability in their own lives amidst the chaos that can be created by a bipolar patient.
Sub-theme 8: Need for programme
This sub-theme is reflected in the participant comment below.
"If it is available I will do it, because I might just learn something or I might be able to share something with somebody and they would learn something. "
So the need for training in the form of a specific programme was expressed.
Sub-theme 9: The future
This sub-theme is substantiated by the following participant comment.
"I think for me it is like I am scared that I might also have it, I think because you sort of, I know a while back it was it is 'oorerflik en dit is geneties '/it is inherited and it is genetic, so I think that thing is always there with me. What if I have it?
CAMH (2000:38) refers to the caregiver's fear about what the future holds. The uncertainty of the future thus may create anxiety with relatives (Miklowitz, 2011:283). Caregivers may also be concerned about the future because bipolar illness is largely a genetic disorder and might affect the couple's children. The unpredictable nature of this illness can be a huge obstacle to making future plans. Uncertainty about the future may cause a caregiver to feel as if they are in limbo (unable to move forward owing to the fear that the illness will spring up) (Last, 2009:3, 31). On occasion, it can prove impossible to plan ahead of time because of the varying episodes of the sufferer's mood (Aiken, 2010:121).
CONCLUSIONS
• The integrated biopsychosocial model, within an ecological systems perspective, served as an important theoretical basis for conducting this research.
• BD affects family relationships, and family relationships affect BD. Families' lack of understanding of the mental illness and how to deal with it affects the rehabilitation outcome negatively. The significant other, be he or she the parent, child, spouse or other relative, also has to deal with the multiple losses that accompany the illness.
• It is more the exception than the rule that the mental health service has developed routines for taking care of the family, who often feel overlooked and forgotten.
• There is a growing understanding that BD should be treated as a family condition. It is therefore important to adopt a broad view, as is provided by the integrated biopsychosocial framework.
• Caregivers must remember their own needs, should share responsibilities with others and stop BD from taking over family life.
• Twenty years ago patients were still kept in psychiatric hospitals for decades, but now the emphasis is on acute treatment, stabilisation, discharge and reintegration into the community. This also puts more strain on caregivers. Although hospitalisation can be traumatic for caregivers, discharge of a loved one may also challenge the caregiver, family and patient.
• There is a marked lack of adequately equipped community resources to which mentally ill patients and their families can be referred in South Africa, especially in the more remote rural areas. This sometimes results in caregivers giving up, while families become less vocal - they just become silent.
RECOMMENDATIONS
• An important role of the social worker in a psychiatric hospital or in the community is to reach out specifically to the patient's significant others, because they are the secondary sufferers of the mental illness. If their needs can be addressed, the patient will also benefit.
• Mental health care professionals should not emphasise the pathological, but instead recognise the strengths of a family - the empathy and cohesiveness that still prevails within the system. A non-blaming stance broadens the possibilities of working with families as partners.
• The caregiver should not be so consumed by the illness that he/she ends up losing her/himself.
• Every patient should receive comprehensive care that focuses on the person as a whole (biopsychosocial model).
• Each patient should be encouraged to have a wellbeing plan. It may range from a private decision by an individual to adopt a certain strategy, through to a formal document drawn up by an individual to consult family, friends and health professionals. Suicide prevention could form part of the wellbeing plan. It is also important to develop an advance directive relapse plan. This could empower caregivers and it may help them to feel less guilty should the patient relapse, because it was decided in advance that the patient should also take responsibility for his/her own life.
• Caregivers must be informed about resources in the community.
• Caregivers should feel part of the MDT. It is important to contract with the caregivers in terms of their roles and responsibilities.
• The mental health social worker must know his/her role within the MDT and be visible. He/she should be assertive and not allow abuse by others, e.g. being used just to handle practical problems such as applying for grants and identity documents and finding accommodation. Aspects such as these can be undertaken by an auxiliary social worker and patients should be empowered to do things for themselves. Dependency should never be encouraged.
REFERENCES
AIKEN, C. 2010. Family experiences of bipolar disorder: The ups, the downs and the bits in between. London: Jessica Kingsley Publishers. [ Links ]
AMERICAN PSYCHIATRIC ASSOCIATION 2000 Diagnostic and statistical manual of mental disorders (DSM-IV-TR). 4th ed. Washington, DC: American Psychiatric Association. [ Links ]
AMERICAN PSYCHIATRIC ASSOCIATION 2013 Diagnostic and statistical manual of mental disorders. 5th ed. Arlington, VA: American Psychiatric Association. [ Links ]
BELARDINELLI, C, HATCH, J.P., OLVERA, R.L., FONSECA, M., CAETANO, SC., NICOLETTI, M., PLISZKA, S., & SOARES, J.C. 2008. Family environment patterns in families with bipolar children. Journal of Affective Disorders, 107:299-305. [ Links ]
BERK, L., BERK, M., CASTLE, D. & LAUDER, S. 2008. Living with bipolar: A guide to understanding and managing the disorder. Crow's Nest, Australia: Allen & Unwin. [ Links ]
BLESS, C , HIGSON-SMITH, C & KAGEE, A. 2006 Fundamentals of social research methods -an African perspective. Cape Town: Juta & Co. Ltd. [ Links ]
CENTRE FOR ADDICTION AND MENTAL HEALTH (CAMH). (2000). Bipolar disorder: An information guide. Toronto. [ Links ]
COLOM, F. & BERK, L. 2010. Psychoeducation as a core element of psychological approaches for bipolar disorders. In: YATHAM, L.N. & MAJ, M., Bipolar Disorder: Clinical and neurobiological foundations. West Sussex: Wiley-Blackwell. [ Links ]
COLOM, F. & VIETA, E. 2006. Psychoeducation manual for bipolar disorder. New York: Cambridge University Press. [ Links ]
DORE, G. & ROMANS, S.E. 2001. Impact of bipolar affective disorder on family and partners. Journal of Affective Disorders, 67: 147-158. [ Links ]
FOUCHÉ, C.B. & SCHURINK, W. 2011. Qualitative research designs. In: AS. DE VOS (ED.), STRYDOM, H, FOUCHÉ, C.B. & DELPORT, C.S.L. Research at grass roots for the social sciences and human science professions. 4th ed. Pretoria: Van Schaik Publishers. [ Links ]
GOOSSENS, P.J.J., VAN WIJNGAARDEN, Β., KNOPPERT-VAN DER KLEIN, E.A.M. & VAN ACHTERBERG, T. 2008. Family caregiving in bipolar disorder: Caregiver consequences, caregiver coping styles, and caregiver distress. International Journal of Social Psychiatry, 54 (4): 303 - 316. [ Links ]
GREEFF, M. 2005. Information collection: interviewing. In: A.S. DE VOS, (ed), STRYDOM, H, FOUCHE, C.B. & DELPORT, C.S.L. Research at grass roots for the social sciences and human science professions. 3rd ed. Pretoria: Van Schaik Publishers. [ Links ]
HATFIELD, A.B. 1987a. Social support and family coping. In: HATFIELD, A.B. & LEFLEY, HP. Families of the mentally ill. New York: The Guilford Press. [ Links ]
HATFŒLD, A.B. 1987b. Families as caregivers: A historical perspective. In HATFIELD, A.B. & LEFLEY, HP. Families of the mentally ill. New York: The Guilford Press. [ Links ]
HAYDEN, EP. & NÜRNBERGER, J.I. 2006. Genetics of bipolar disorder. In: EL-MALLAKH, RS. & GHAEMI, S.N., Bipolar depression: A comprehensive guide. Washington, DC: American Psychiatric Publishing, Inc. [ Links ]
KECK, P.E., MCELROY, S.L. & HAWKINS, J.M. 2010. Acute mania. In: YATHAM, L.N. & MAJ, M., Bipolar disorder: Clinical and neurobiological foundations. West Sussex: Wiley-Blackwell. [ Links ]
KILBOURNE, A.M., GOODRICH, D.E. & BAUER, M.S. 2010. Collaborative care for bipolar disorder. In: Yatham, L.N. & Maj, M., Bipolar disorder: Clinical and neurobiological foundations. West Sussex: Wiley-Blackwell. [ Links ]
LAM, D., DONALDSON, C, BROWN, Y. & MALLIARIS, Y. 2005. Burden and marital and sexual satisfaction in the partners of bipolar patients. Bipolar Disorders, 7: 431-440. [ Links ]
LAST, CG. 2009. When someone you love is bipolar: Help and support for you and your partner. New York: The Guilford Press. [ Links ]
LEFLEY, H.P. 1987. Culture and mental illness: the family role. In: HATFIELD, A.B. & LEFLEY, HP. Families of the mentally ill. New York: The Guilford Press. [ Links ]
MCELROY, EM. 1987. The beat of a different drummer. In: HATFIELD, A.B. & LEFLEY, HP. Families of the mentally ill. New York: The Guilford Press. [ Links ]
MICHALAK, EE., MURRAY, G, YOUNG, AH. & LAM, R.W. 2010. Quality of life impairment in bipolar disorder. In: RITSNER, M.S. & AW AD, AG., Quality of life impairment in schizophrenia, mood and anxiety disorders - new perspectives on research and treatment. Amsterdam: Springer. [ Links ]
MIKLOWITZ, D.J. 2011.The bipolar disorder survival guide: What you and your family need to know. 2nd ed. New York: Guilford Press. [ Links ]
MIKLOWITZ, DJ & GOLDSTEIN, M.J. 1997 Bipolar disorder: A family-focused treatment approach. New York: Guilford Press. [ Links ]
MOND1MORE, FM. 2006. Bipolar: A guide for patients and families. Maryland: The Johns Hopkins University Press. [ Links ]
NATIONAL INSTITUTE OF MENTAL HEALTH USA.GOV (NIMH). 2010. Booklet on bipolar disorder. [Online] Available: http://www.nimh.nih.gov/publicat/bipolar.cfm. (Accessed 2012/02/02). [ Links ]
NIEUWENHUIS, J. 2007a. Qualitative research designs and data gathering techniques. In: K. MAREE (Ed.). First steps in research. Pretoria: Van Schaik Publishers. [ Links ]
NIEUWENHUIS, J. 2007b. Analysing qualitative data. In: K. MAREE (ed) First steps in research. Pretoria: Van Schaik Publishers. [ Links ]
OGILVIE, A.D., MORANT, N. & GOODWIN, G.M. 2005. The burden on informal caregivers of people with bipolar disorder. Bipolar Disorders, 7: 25-32. [ Links ]
OSTACHER, M.J., NIERENBERG, A.A., LOSIFESCU, D.V., EIDELMAN, P., LUND, H.G., AMETRANO, RM., KACYNSKI, R., CALABRESE, J., MIKLOWITZ, D.J., SACHS, GS. & PERLICK, D.A. 2008. Correlates of subjective and objective burden among caregivers of patients with bipolar disorder. Acta Psychiatrica Scandinavica, 118: 49-56. [ Links ]
PARKER, G. & KETTER, TA. 2010. Management of bipolar II disorder. In: YATHAM, L.N. & MAJ, M., Bipolar disorder: Clinical and neurobiological foundations. West Sussex: Wiley -Blackwell. [ Links ]
PERLICK, DA., ROSENHECK, RA., CLARKFN, J.F., MACIEJEWSKI, PK, SIREY, J., STRUENTNG, E. & LINK, B.G. 2004. Impact of family burden and affective response on clinical outcome among patients with bipolar disorder. Psychiatric Services, 55 (9): 1029-1035. [ Links ]
SCHURPNK, W., FOUCHÉ, C.B. & DE VOS, A.S. 2011. Qualitative data analysis and interpretation. In: AS. DE VOS, (ed) STRYDOM, H, FOUCHÉ, C.B. & DELPORT, C.S.L. Research at grass roots for the social sciences and human science professions. 4th ed. Pretoria: Van Schaik Publishers. [ Links ]
SMITH, H. 2007. Social interventions. In: BAUMANN, SE., Primary health care psychiatry: A practical guide for southern Africa. Cape Town: Juta. [ Links ]
STRYDOM, H. 2011. Ethical aspects of research in the social sciences and human service professions. In: A S. DE VOS (ed) STRYDOM, H, FOUCHÉ, C.B. & DELPORT, C.S.L. Research at grass roots for the social sciences and human science professions. 4th ed. Pretoria: Van Schaik Publishers. [ Links ]
SURDUT, A.B. 1998. Social Interventions. In: BAUMANN, S. E. Psychiatry and primary health care: A practical guide for health care workers in Southern Africa. Cape Town: Juta & Co, Ltd. [ Links ]
TAYLOR, E. H. 2006. Atlas of bipolar disorders. United Kingdom: Thomson Publishing Services. [ Links ]
TERKELSEN, KG. 1987a. The meaning of mental Illness to the family. In: HATFIELD, A.B. & LEFLEY, HP. Families of the mentally ill. New York: Guilford Press [ Links ]
TERKELSEN, K.G. 1987b. The evolution of family responses to mental illness through time. In: HATFIELD, A.B. & LEFLEY, HP. Families of the mentally ill. New York: Guilford Press. [ Links ]
VAN DER VOORT, T.Y.G., GOOSSENS, P.J.J. & VAN DER Β DL, J.J. 2007. Burden, coping and needs for support of caregivers for patients with a bipolar disorder: A systematic review. Journal of Psychiatric and Mental Health Nursing, 14: 679-687 [ Links ]
VIETA, E. 2009. Managing bipolar disorder in clinical practice. 2nded. London: Current Medicine Group Ltd. [ Links ]
WEBBER, M. 2010. The evidence base for psychosocial mental health practice. In: WEBBER, M. & NATHAN, J. Reflective practice in mental health: Advanced psychosocial practice with children, adolescents and adults. London: Jessica Kingsley Publishers. [ Links ]


{kind=link}
{kind=link}