










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.54 n.3 Stellenbosch 2018
http://dx.doi.org/10.15270/52-2-652
ARTICLE
The aftercare needs of Nyaope users: implications for aftercare and reintegration services
Sonto MahlanguI; Stephan GeyerII
IPostgraduate Student
IIDepartment of Social Work and Criminology, University of Pretoria, Pretoria, South Africa
ABSTRACT
Nyaope is a relatively new drug on the South African market and mostly (mis)used by youths. Without targeted intervention, this drug could negatively affect the wellbeing of the people involved. Aftercare and reintegration services are often downplayed, with little emphasis in both research and practice. This article reports on the aftercare needs of nyaope users from both the users' and the significant others' points of view in Hammanskraal (a South African township). A collective case study was implemented through semi-structured interviews with both nyaope users and significant others. Recommendations are offered to role players involved in aftercare and reintegration services.
INTRODUCTION
New drugs continuously enter the illicit drug market. Currently, in South Africa there is a relatively new drug on the market known as nyaope which is being mis(used) mostly by youths in the townships. "Nyaope is a cheap drug cocktail comprising heroin, marijuana and other elements like rat poison, cleaning detergents and even crushed pills used in the treatment of AIDS patients" (Ghosh, 2013:6). Abuse of drugs, such as nyaope, leads to road traffic accidents, suicide, violence and high-risk sexual behaviour. Failure to find a solution to drug abuse can lead to economic problems and handicap the social development of the country, and impede the bio-psychosocial wellbeing of the people involved (Moodley, Matjila & Moosa, 2012:6-7).
It is estimated that about 15% of South African youths are susceptible to drug abuse and that the exposure to the designer drug nyaope is very common and on the rise (Fernandes & Mokwena, 2016:153). As nyaope is one of the cheapest illicit drugs, it is widely available in South Africa and easily accessible to, among others, youths. For the second semester of 2016 the South African Community Epidemiology Network on Drug Use (SACENDU) released a report that suggests the use of nyaope continues to pose a problem, with as many as 9% of all patients in the Gauteng Province being admitted for nyaope use (Dada, Harker Burnhams, Erasmus, Parry, Bhana, Timol & Fourie, 2017:1). A study conducted at a secondary school in Atteridgeville by Moodley et al., (2012:6) estimated the prevalence of nyaope use was 2.9%. As a case in point, the Hammanskraal office (a township in South Africa north of the City of Tshwane) of the Department of Social Development (DSD) in the Gauteng Province admitted at least ten people addicted to nyaope to treatment centres on a monthly basis (Makhubela, 2015). As both authors reside in the Gauteng Province, and the fact that nyaope use emerged in townships of the Tshwane Metro during the early 2000s (Health24, 11/04/2014), Hammanskraal was selected as a township for the case study.
The Gauteng Department of Social Development's Annual Performance Plan (Department of Socisl Development, 2016:123) states that the number of service users who have accessed public in-patient treatment centres in the year 2016 was 1,436. Furthermore, it indicates that the number of people who received treatment for drug addiction and who participated in aftercare programmes was 9,563 in the Gauteng Province. The authors were interested in determining and ascertaining whether the aftercare needs of nyaope users are attended to in the aftercare programmes that are offered. The reality is that aftercare and reintegration services remain neglected both in South African practice and in research (cf. Swanepoel, Geyer & Crafford, 2016; Van der Westhuizen, Alpaslan & De Jager, 2013), especially in townships such as Hammanskraal. Aftercare is defined as "service delivery to enable service beneficiaries to regain self-reliance and optimal social functioning" (DSD, 2013b:30) as well as to sustain the gains attained in the initial treatment phase and to prevent relapses by offering support for participation in self- and mutual help and other programmes (Popovici, French & McKay, 2008:550). The ultimate goal of reintegration services is to strengthen ties between the user and the community, and to integrate the user into community life by helping him/her to assume normal social roles (Chui, 2016).
The percentage of people who misuse drugs is increasing in communities irrespective of the support that the communities provide and of what the different stakeholders and the DSD are doing to eradicate this social problem (Department of Social Development, 2013a:72). Consequently, Maluleke (2013:106) recommends that there should be more scientific enquiries on issues of aftercare and reintegration services among substance-dependent persons in South Africa. This underscores the fact that more research should be conducted on aftercare and reintegration services among people addicted to drugs.
The practice and research related to aftercare and reintegration services remain neglected (Van der Westhuizen, 2010:103), and, to the best of our knowledge, no previous South African study has explored the aftercare needs of nyaope users in a South African township from both the users' and the significant others' points of view. Therefore, the focus of this article is to address this research gap in knowledge and to report on the results of a study that aimed to explore and to describe the aftercare needs of nyaope users in Hammanskraal from the users' and the significant others' points of view. Recommendations with regard to aftercare and reintegration services will also be offered, as there are very few studies focusing on drug aftercare and reintegration services in Hammanskraal (Molefe, 2014).
BIO-PSYCHOSOCIAL MODEL
The theory that informed the study is the bio-psychosocial (BPS) model. The BPS model is based on the general systems theory that is applied in medicine and psychiatry, which holds that "all the three levels, biological, psychological and social processes, must be taken into account in every healthcare task" (Alvarez, Pagani & Meucci, 2012:174), because they are all integral and interactively involved in physical and psychological health and illness. The theory posits that substance abuse is the net result of complex interactions between a combination of biological, psychological, social and spiritual determinants (Dogar, 2007:11).
In the light of the BPS model, substance abuse treatment should adopt a holistic approach. It expands the role of the physician to coping with illness and searching for conditions that contribute to the patient's suffering (Fleisher & Feldman, 1999:1). Therefore, successful treatment is dependent upon comprehensive and accurate assessment and the matching of affected individuals to the most appropriate treatment (Alvarez et al., 2012:174). However, recovery may or may not require abstinence, depending upon the degree of severity and/or the type of syndrome. The above implies that a substance-use disorder could be treated like any other chronic illness, as it will require ongoing treatment. It could be suggested that all service providers in the field of addiction should work together towards finding solutions to a variety of serious problems. The adoption of the BPS model makes it possible for service providers to attend to the holistic needs of a nyaope user in the psychological, social, biological and spiritual domains.
It is equally important to note that each systemic level is interdependent with the others, and, theoretically, none has functional priority over the others (Alvarez et al., 2012:174). The treatment of nyaope addiction, and the aftercare and reintegration services, cannot focus on only one element; all the three levels - biological, psychological and social - should be taken into account. In addition, the recognition of spirituality plays an essential role in this BPS model with respect to a person's self-identity and self-direction (Morris, Johnson, Losier, Pierce & Sridhar, 2013:79), especially in the case of the young person recovering from nyaope addiction. In a study conducted by Galanter, Dermatis, Bunt, Williams, Trujillo and Steinke (2007:261) on the relevance of spirituality in social services, they found that a spiritual orientation plays a unique role in promoting an attitude that facilitates some service users' openness to change. Gabbard and Kay (2001:1957) think that a BPS model results in "combined treatment". Therefore, the authors of this article support the notion that nyaope users may do better with a combination of psychosocial-spiritual support and medical care (e.g. medication). Most importantly, assessment that is based on the BPS model requires that the service provider should be caring and have the communication skills necessary to develop rapport, elicit trust, offer continuity of care, provide ongoing accessibility, and learn about the living conditions of the patients and significant others (Fleisher & Feldman, 1999:4). The Framework for Social Welfare Services (Department of Social Development, 2013b) reflects the view of Fleisher and Feldman (1999), as it prescribes a continuum of care that includes aftercare and reintegration services. On the one hand, aftercare and reintegration services could sustain the gains of treatment, while on the other hand, neglecting them implies non-adherence of service providers to the required delivery framework.
RESEARCH QUESTIONS AND GOAL
The research questions that guided the study on which this article is based were:
-
Based on the views of nyaope users, what are the aftercare needs of nyaope users in the Hammanskraal community?
-
Based on the views of significant others, what are the aftercare needs of nyaope users in the Hammanskraal community?
The goal of the study was to explore and describe the aftercare needs of nyaope users from both the users' and the significant others' points of view in Hammanskraal.
RESEARCH METHODS
The study adopted a qualitative approach as the focus was on the perceptions of nyaope users and significant others about aftercare needs and the concomitant aftercare and reintegration services, not on the meaning that the researchers bring to the research (Creswell, 2009:47). Applied research was the most suitable approach for this study. Merriam (2009:3) states that applied research is undertaken to improve the quality of practice of a particular discipline - in this study the aftercare and reintegration services of nyaope users. A case study, as the research design, is particularly useful when there is a need to obtain in-depth knowledge of an issue or phenomenon within its context (Padgett, 2017:35). The collective case study was deemed the most appropriate design to attain the goal of the study, because it enabled the researchers to combine/compare data obtained from the users and the significant others (Yin, 2003:42).
The study population included the nyaope users in the Hammanskraal community as well as significant others. Hammanskraal is a township about 40 km north of the South African capital city of Pretoria (Nxumalo & Gare, 2015:6). The inhabitants are African Black people, since Hammanskraal was formerly a black township in the homeland of Bophuthatswana. Poverty and unemployment are widespread. A large proportion of the Hammanskraal population lives in informal settlements.
The sampling for this study took place in two phases. Firstly, the South African National Council on Alcoholism and Drug Dependence (SANCA) Hammanskraal was approached and they used purposive sampling to identify the nyaope users who had relapsed and their significant others (partner, husband, wife, niece, nephew, brother, sister, parent/caregiver to the nyaope user). To be considered for inclusion in the study, the nyaope user and the significant other were not required to be direct matches. The study explored the views of nyaope users and significant others who were not necessarily related to each other.
Secondly, only the people who volunteered their participation (i.e. volunteer sampling) following recruitment via SANCA were interviewed by the first author. Data were collected to the point of data saturation, when six nyaope users and six significant others were interviewed. For the purpose of this research semi-structured interviews were utilised as a data-collection method with two distinct interview schedules (Bernard, 2000:191). The interviews for the study were audio recorded. Thematic analysis was conducted according to the process proposed by Clarke and Braun (2013:121-123). Credibility, transferability and confirmability were tested in establishing the trustworthiness of the study (Lietz & Zayas, 2010). More specifically, peer debriefing was used to ensure trustworthiness. The authors had discussions with a colleague who had a general understanding of the nature of the study to review perceptions, insights and analyses. The authors also analysed the data from the transcriptions (i.e. observer triangulation). The outcome of the analyses was confirmed for accuracy through member checking. In addition, the data obtained from both the users and the significant others were compared to identify similarities and differences in opinion (i.e. data triangulation) (Lietz & Zayas, 2010:198; Oliver-Hoyo & Allen, 2006:43).
Ethical clearance was obtained from the Research Ethics Committee of the university (Ref no.: GW20151129HS) and SANCA (Hammanskraal) granted permission for the study.
RESEARCH FINDINGS AND DISCUSSION
The findings are outlined in two sections, namely the biographical profile of the nyaope users and significant others, and the themes and sub-themes. After that the triangulated data are presented.
Findings: Nyaope users
Biographical profile
The biographical information of the nyaope users revealed that all of the participants were male. The majority were Sepedi speaking. All participants had some high school education, with the majority of them completing Grade 12. Moreover, the majority of the participants were not in formal employment at the time of the study. Furthermore, all the participants relapsed after an initial treatment and they mostly received their treatment at a government/public treatment centre. Most participants were already being treated for the second time.
Themes and sub-themes
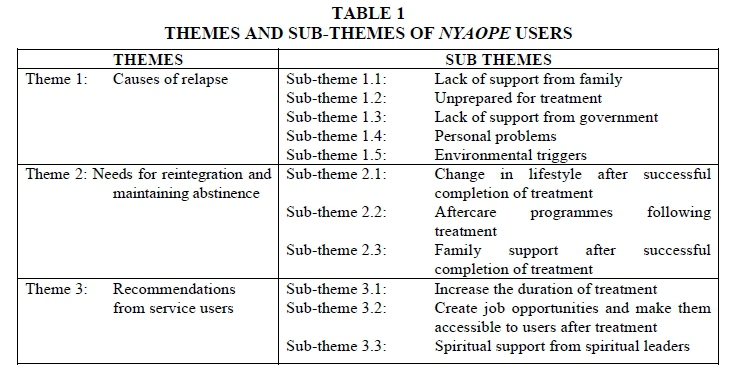
Table 1 outlines the data of the nyaope users in thematic form.
Theme 1: Causes of relapse
The causes of relapse were identified as being lack of support from family, lack of support from the government, personal problems and environmental triggers.
Sub-theme 1.1: Lack of support from family
It was identified that family members do not support the user after treatment. Relationships within the family are also negatively affected by the stress associated with the user's substance abuse (Groenewald & Bhana, 2016:647). This is because family members are often victims of crime, they lose hope in the user and they endure pain associated with the user being addicted to nyaope. Some of the participants' views are encapsulated in the quotations below:
"My last relapse was caused by ... [the] lack of support from my family."
"We need support, lot of support from our parents."
This finding highlights the importance of getting the family members of the person addicted to drugs to take part in preparatory groups prior to treatment and in groups after treatment. These groups could assist in addressing unresolved feelings experienced by the user. This statement concurs with the finding of Van der Westhuizen, Alpaslan and De Jager (2011:364) that the benefits of family involvement in aftercare are associated with better treatment compliance and outcomes. Hence, it is indicated that there is a need to make the treatment centres aware that families need to be involved during the treatment process of the addicted individual, so that it becomes easy for the families to continue supporting the individual after he or she has completed the rehabilitation process (Mzolo, 2015:2).
Sub-theme 1.2: Unprepared for treatment
Closely linked to the previous sub-theme was the finding that the nyaope users were in disagreement with their family members and often felt betrayed as they sensed they were coerced into going for treatment. Some participants expressed themselves as follows:
"I was not ready in my heart. It is like I was forced to quit nyaope. I was still very much in love with it before I was taken to a treatment centre."
"I was really addicted; it did not come from me to get rehabilitated."
These quotations indicate that unless social workers implement strategies such as motivational interviewing (MI) to prepare nyaope users adequately for treatment and to manage their resistance to treatment in order to ultimately develop insight into their need for treatment, all inputs at the treatment centre could be futile (cf. Van Wormer & Davis, 2013:426-427). The potential conflict between the user and significant others should be dealt with constructively during treatment and aftercare services. Users could relapse because they do not accept that they are addicted to nyaope and therefore do not have a desire to abstain.
Sub-theme 1.3: Lack of support from government
Lack of support from the government was identified as another contributing factor to relapse. The users felt that there are no programmes, for example, offered by the DSD, that assist them in maintaining abstinence after treatment. The users noted lack of recreational activities and poor support from social workers after treatment. It was reported before that a lack of aftercare services is associated with relapse (McKay, 2001:9). The following statements are representative of the contributions of the participants regarding this aspect:
"The government can help me with programmes after rehab."
"The government can build us recreational facilities and sporting grounds. "
"I want a chance to attend group sessions and spend the whole six weeks at a [public] rehab."
The National Drug Master Plan 2013-2017 (NDMP) makes the point that demand reduction should focus on preventing the onset of drug usage and eliminate all conditions/factors that may tempt an individual to use substances (Department of Social Development, 2013a:62). Hence, the participants stressed the importance of having recreational activities in their communities, which they felt were lacking in the Hammanskraal community. This plight of nyaope users is underscored by the BPS model, which highlights that attention to addiction must include attention to the individual (with bio-psycho-social-spiritual characteristics) in relation to the surrounding environment (both natural and built) as essential components during aftercare services (Alvarez et al., 2012:174).
Sub-theme 1.4: Personal problems
Users are overwhelmed by challenges they face in their own lives, their families and the society they live in. The psychological aspect of the BPS model includes the thinking that leads to the use of the substance. These irrational or unhealthy thought processes may be associated with depression or anxiety, which in turn may encourage escape through drug use (Van Wormer & Davis, 2013:15-17). Users resort to smoking nyaope to cope with their problems and to ease their burdens. The identified problems include financial challenges and ambivalent romantic relationships. As a result of the pleasurable state of relaxation that comes after smoking the drug, users view the drug as a solution to their problems. The following statements are representative of the participants' views on this aspect:
"I had a girlfriend and we had problems, so a thought crossed my mind for me to go and see my old friends and took two puffs, then I got hooked again."
"I am a breadwinner, I do not have support for these type of things, somewhere I get stressed by all this."
The above finding concurs with the point that pre-clinical studies have found that exposure to stress, in addition to the drug itself, is a potent stimulus in reinstating drug-seeking behaviour among dependent people (Sinha, 2001:350). It could, therefore, be concluded that personal problems can be included as a cause of relapse after treatment. This was also confirmed in a study focusing on adolescents which found that substances are used in order to deal with socio-emotional challenges (Geyer, Le Roux & Hall, 2015:33).
Sub-theme 1.5: Environmental triggers
During the interviews the participants highlighted that they are influenced by their friends to take up their smoking habits again. Some are even discouraged from going to treatment, because they have witnessed their peers relapsing after treatment. As a consequence, there tends to be great frustration with going back to the same environment following treatment. These results concur with the findings of the research by Lebese, Ramukuela and Maputle (2014), where peer pressure was identified as a factor contributing to substance abuse. Some of the participants' views include the following:
"When I am there, my friends smoke ... And then I decided to join my friends and smoke."
"My relapse was caused by coming back to the same streets."
"When I am sitting alone at home, I become bored and broke; then I decided to go back to the streets and hustle."
The literature highlights that if the family fails to show acceptance of the user, the user will turn to other means in order to meet this need (Maree, 2013:76-77). The finding of this research confirms the above statement, namely that peer relationships play a role in substance abuse. It is thus important to take into equal consideration the social aspect as suggested by the BPS model during treatment and recognise that the users' social situation matters in the presentation of the addiction (Alvarez et al., 2012:174). Part of dealing with the social aspect, as suggested by the BPS model, could be adopting demand-reduction strategies as outlined in the NDMP. The NDMP stipulates that demand reduction is important and should focus on eliminating conditions/factors that could trigger substance use (Department of Social Development, 2013a:62). Based on the findings in this sub-theme, it appears that this particular strategy is not adequately implemented in the Hammanskraal community. Consequently, when the nyaope user returns to the same environment with the same peer networks, they are bound to experience triggers and cravings for the drug (Mzolo, 2015: 40).
Theme 2: Needs for reintegration and maintaining abstinence
Meeting the participants' need for reintegration into the community and need for support in maintaining abstinence was identified as entailing a change in lifestyle after successful completion of treatment; there was also a need for aftercare programmes following treatment and family support after successful completion of treatment.
Sub-theme 2.1: Change in lifestyle after successful completion of treatment Nyaope users need to change the type of lifestyle they were living before going for treatment and adopt a lifestyle more conducive to healthy living. This includes surrounding oneself with positive people and occupying oneself constructively. The above links to the Republic of South Africa (RSA), (1997:70), which specifies youths and substance abuse as priority areas requiring service delivery and emphasises the importance of strengthening family life and the role of effective family functioning in developing users' wellbeing. Some of the participants expressed the following views:
"It is staying positive and the fact that I have friends who call me to order when I am out of line."
"When I come back from [the] treatment centre, they can help me with programmes. If something does come up, they must let me know, something like plumbing and electrical opportunities."
Nelson (2012:128) mentions that it is important to maintain a balanced lifestyle. This might mean having a balance between work and family life, adequate sleep, healthy eating and regular exercising to be able to cope with everyday stressors. Service users should focus on maintaining a balanced lifestyle and be aware of their lifestyle becoming unbalanced (Nelson, 2012:128). The Cenaps model of relapse prevention stresses that total abstinence, as well as personality and lifestyle change, is essential for full recovery (Fisher & Harrison, 2013:120).
Sub-theme 2.2: Aftercare programmes following treatment
The users emphasised that if the government implemented adequate aftercare programmes, relapse after treatment could be prevented. The aftercare programmes they need must include therapeutic intervention from social workers after treatment. Another important element that was stressed was that a skills development centre should be available where participants could develop or enhance their skills. The views of the participants included the following:
"When I come back from the treatment centre, they can help me with programmes."
"All I want to add is that all they can do is to get me [application] forms or skills development centres."
The literature review signals that drug relapse is associated with inadequate aftercare services (McKay, 2001:213). Participants long for satisfactory aftercare programmes, as indicated in the views above. The Prevention of and Treatment for Substance Abuse Act 70 of 2008, Section 30(2), highlights the importance of prescribing integrated aftercare and reintegration services aimed at the successful reintegration of a service user into society, the workforce, and family and community life. Nonetheless, the findings of the study indicate that these aims have not yet been achieved and much remains to be done. A successful aftercare programme, based on a BPS model, will pay attention to the bio-psychosocial health of users and generate a continuum of services (Dogar, 2007:12).
Sub-theme 2.3: Family support after successful completion of treatment
Family support was highlighted as an important element that contributes positively to an individual's maintaining abstinence after treatment. This finding concurs with the views of Van der Westhuizen et al., (2011:364), specifically that family members can support one another, they can communicate openly and honestly and resolve conflict, and the family can change destructive behaviours, strengthen family bonds, and provide the drug user with emotional and practical support when the user is experiencing cravings. Family members need to be included and educated about giving support to a nyaope user. Participants' opinions include the following:
"You know if your family members stop judging you and support you, you also become strong emotionally."
"We need support, a lot of support from our parents."
Families and parental factors contribute towards building the capacity of the substance-dependent persons to overcome any challenges ahead of them (Maluleke, 2013:86). Equally, a family should be viewed as an integral part of aftercare services, considering the facts that the addiction occurred in the family, that the family could have participated in and perpetuated the addiction, and that the addiction caused harm to the family. The BPS model posits that it is of the utmost importance that a medical doctor is able to extend health care beyond the patient to include the family and community (Dogar, 2007:11). Therefore, family therapy is of paramount importance for families with a person addicted to nyaope in treatment centres, as families could also learn coping mechanisms and how to support their loved ones (Mzolo, 2015:15)
Theme 3: Recommendations from service users
Nyaope users are well aware of the high relapse rate after treatment. They expressed their views on what they think should be done at treatment centres and after discharge. They recommended that the duration of treatment should increase, job opportunities should be created and be accessible to them after treatment, and that they receive support from spiritual leaders during and after treatment.
Sub-theme 3.1: Increase the duration of treatment
There is no doubt that the short duration of the treatment is frustrating many nyaope users. The six weeks allocated at the government treatment centres are considered insufficient in their view. The majority of the participants accessed their treatment at a government treatment centre and they felt that, given the extent of their addiction, it takes a bit longer for the drug to be successfully eliminated from their systems. There was a strong belief that if the duration of the treatment is increased from six weeks to six months or more, positive results could ensue. The following statements are representative of the views of the participants on this aspect:
"I am not satisfied with the duration of the treatment."
"The treatment period was too short. I needed more than six weeks, I was an addict."
Considering the increase in the demand for treatment, an adequate treatment period and ongoing aftercare services are vitally important in preventing relapse and ensuring the maintenance of recovery (Van der Westhuizen & De Jager, 2009:77). As mentioned by the authors, an adequate treatment period is essential; the users feel that the current duration of treatment is inadequate. Research has shown unequivocally that good outcomes are contingent on adequate treatment duration (National Institute of Drug Abuse [NIDA] 2012 in Swanepoel, 2014:65).
Sub-theme 3.2: Create job opportunities and make them accessible to users after treatment
Unemployment has dire consequences for families and communities who are plagued by nyaope use (Mokwena & Morojele, 2014:380). Creating employment opportunities for users who have successfully completed treatment is considered to be among the possible solutions. Nonetheless, taking nyaope users to an aftercare programme that is inclusive of skills development could make job opportunities accessible to the users as well. The participants expressed their views as follows:
"They must help me with employment and school, tertiary education."
"I must place my focus in school and find a job for me to keep busy ..."
"When you are working, you can concentrate on your job, there is a slight possibility that you can go back to drugs."
Participants are aware of the fact that employment opportunities would keep them away from the streets and their habits of using drugs; hence, poverty is understood as a contributory factor to nyaope use (Mokwena & Fernandes, 2014:43). It is emphasised that strong collaboration between community structures and government departments is needed to address the challenges posed by the negative social environment, which would include addressing the unemployment rate in predominantly black communities (Mokwena & Morojele, 2014:381). With the latest unemployment rate at 27.7% (the highest since 2008), nyaope users could be demotivated to sustain their abstinence, because opportunities of securing employment, especially for Black African youths, remain slim (Peyper, 2017).
Sub-theme 3.3: Spiritual support from spiritual leaders
Nyaope users felt that they need spiritual support at the treatment centre and after they have been discharged from the centre. They believe that the restoration of their relationship with a Higher Power will give them the courage and peace that will assist them in maintaining abstinence. They indicated that spiritual support should be incorporated as part of the healing process at the treatment centre and continued into aftercare. The following statements are representative of the views of the participants regarding this aspect:
"Now I wish that God can help me become a better person ... I can become a better person and start attending church and community meetings."
"That place needs God because people get admitted and then relapse."
The positive outcome of one's spirituality was determined in a study by Mason, Deane, Kelly and Crowe (2009:1934). They highlighted that greater spirituality is associated with self-sustained abstinence. Furthermore, Mason etal., (2009:1935) found that over 80% of participants in their sample considered that spirituality would be helpful in the maintenance of recovery, in completing the treatment programme and in preventing a relapse. According to the BPS model, the spiritual aspect is a key component of overcoming addiction. Spirituality is crucial in recovery, because it is related to one's sense of meaning and interconnectedness (Van Wormer & Davis, 2008:12).
Findings: Significant others
Biographical profile
The biographical profile of the significant others reveals that the majority of participants were those who acted as mother figures to the nyaope users. The nyaope users received treatment mostly at government treatment centres and relapsed after initial treatment. The participants' ages ranged between 40 to 71 years, and all identified themselves as African Black. They were from the Sepedi, isiZulu, Tshivenda and Xitsonga tribes.
Themes and subthemes
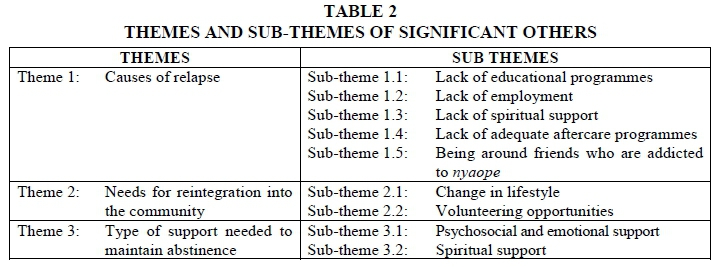
Table 2 presents an overview of the themes and sub-themes related to significant others.
Theme 1: Causes of relapse
The participants identified the causes of relapse of the nyaope users as the lack of educational programmes, lack of employment, lack of spiritual support, lack of adequate aftercare programmes and being around friends who are addicted to nyaope.
Sub-theme 1.1: Lack of educational programmes
The participants stressed that lack of educational programmes in communities contributes to relapse. The significant others referred to vocational training facilities and educational programmes that nyaope users could attend after treatment. They also stressed that it is important that these opportunities must be accessible, meaning that nyaope users should be able to attend free of charge. Some of the participants' views are quoted below:
"It is by taking him to school."
"I thought that they received some kind of life skills training for them to forget about nyaope and that environment."
"What can be done is that he must get a school, I don't know if there is a school or college that he can go to for free."
The Prevention of and Treatment for Substance Abuse Act 70 of 2008 notes that treatment could focus on education as one of the strategies that could equip individuals with additional skills to maintain their treatment gains and sobriety, and avoid relapse. However, based on this finding it seems that this strategy has not yet materialised. As Makhubela (2015) states, policies take time to be implemented in practice. It has been highlighted before that educational facilities are the best tool that could be provided to communities to help in the fight against substance abuse (Lebese et al., 2014:341).
Sub-theme 1.2: Lack of employment
South Africa's high youth unemployment rate has dire consequences for the country's economy. The high number of unemployed youths in South Africa leads to numerous social problems, such as substance abuse and crime (World Economic Forum, 2014:39). Likewise, this study identified unemployment to be contributing extensively to substance abuse. The participants mentioned that they want the government to assist in providing job opportunities to users after they completed treatment. The following statements are representative of the views of the participants regarding this aspect:
"He can be best supported by getting him a job when he comes back from the treatment centre."
"So if the government can have an aftercare programme, and create jobs, maybe these people might change."
The Drugs and Drug Trafficking Act 140 of 1992 states clearly that people must be equipped with additional skills to maintain abstinence and avoid relapse. Currently, the employment absorption rate for youths with matric is 50.3% (Peyper, 2017). Unemployment means that nyaope users experience extended periods of leisure time and they struggle to avoid boredom, hence they resort to smoking nyaope. However, in a study by Thothela, Van der Wath and Janse van Rensberg (2014:85), the availability of sporting facilities as a means of combating boredom, as well as a lack of stimulation and structure, provided little evidence that sporting schemes on their own are effective in reducing substance abuse.
Sub-theme 1.3: Lack of spiritual support
The participants indicated that nyaope users relapse because they lack spiritual support. Van Wormer and Davis (2008:11) identify this kind of support with reference to a biopsychosocial-spiritual model. The reason for the lack of spiritual support is that many nyaope users do not attend church once they become addicted. It is difficult for spiritual leaders/pastors of churches to reach out to them because they distance themselves from such institutions. The participants offered the following inputs:
"This family is affiliated with the Zion Christian Church but my son does no longer go to church."
"Every time he went out, I tried telling him that he must not go back to the same group of friends, he should go to church every Sunday. I tried my best."
Gossop (in Masombuka, 2013:94) is of the view that the early teachings of the Christian church strongly opposed and denounced the use of drugs. The practice of spirituality in one's daily routine could be significant in laying a solid foundation for a positive recovery cycle (Morris, et al., 2013:80). It is important to note that spirituality is crucial in recovery, because it is related to one's sense of meaning and interconnectedness (Van Wormer & Davis, 2008:12).
Sub-theme 1.4: Lack of adequate aftercare programmes
The participants mentioned that they witnessed the relapse of the nyaope users, because when they come back from treatment, they roam the same streets and go back to the same friends. If the government can introduce an aftercare programme that could keep the users occupied, the participants felt that the high relapse rate could be prevented. The participants shared the following:
"If there is an aftercare programme, he will be able to choose what he wants to do."
"If he can have something to keep him busy during the day, he can become clean."
"So if the government can have an aftercare programme and ask them what is it they want and create jobs, maybe these people might change."
The Prevention of and Treatment for Substance Abuse Act 70 of 2008 highlights the fact that substance users need to be linked to some form of aftercare and reintegrati on service. As it now stands, DSD social workers are expected to offer aftercare and reintegration groups for nyaope users who have completed the treatment programme. However, such groups are challenged by poor attendance of members (Makhubela, 2015). The statements of the significant others are an indication of the lack of an aftercare programme in the Hammanskraal community.
Sub-theme 1.5: Being around friends who are addicted to nyaope
The participants also highlighted the fact that friendships had an adverse effect on nyaope users' recovery process. This is because they misused substances with friends before going for treatment and this became a huge temptation in the process of recovery (Soeker, Matimba, Machingura, Msimango, Moswane & Tom, 2016:576). Furthermore, it has been said that there is a lot of negativity amongst friends who smoke nyaope about going for treatment. Some of the participants' views included the following:
"He had to ruin it when his friends were constantly dropping by to check on him."
". because when he comes from the treatment centre, he goes back to the same friends and does the same things they used to do."
When a substance-dependent individual has been through a rehabilitation process, and he/she returns to the same environment as before the process, relapse could be triggered (Larimer, Palmer & Marlatt, 1999:12). In another study the influence of friends and other associates was identified as an external locus of control that is always blamed for the initial taking of the drug or continued use of the drug (Mokwena & Fernandes, 2014:47). The consequences of nyaope addiction - for example, stealing valuable items from significant others to secure money to buy drugs, as well as the mentioned causes of relapse - often leads to desperation among the significant others to help the nyaope user to 'escape' from drug abuse. One significant other expressed the following opinion:
"It [treatment] must not be voluntary; it should be through a binding court order. The users will have rules that he needs to abide by, but if he goes voluntarily it will be easy for him to discharge himself."
Another mentioned:
"... he takes my dishes and sells them, more specifically electrical appliances ..."
Theme 2: Needs for reintegration into the community
The need for reintegration into the community was identified as important; users need a change in lifestyle, and make use of or be offered volunteering opportunities. Furthermore, during aftercare the nyaope users should regain the trust of the community and by not victimising their own community members (e.g. through theft of personal belongings).
Sub-theme 2.1: Change in lifestyle
The significant others indicated that for the users to be reintegrated back into the communities, a change in lifestyle is required. As mentioned earlier, drug abuse is associated with criminal activities. The significant others indicated that when nyaope users stop stealing from their community members, it will become easy for them to be trusted again. It is important that the substance-dependent persons assume new roles and responsibilities when they are reintegrated into the community (Maluleke, 2013:30). For example:
"He can be reintegrated back to the community if he changes his ways."
"His behaviour must change and he must get a job."
"They will see that he has changed when he is no longer roaming the streets and when he does what is expected of him."
The BPS model suggests that the role of the medical doctor should not be limited to help a nyaope user to cope with the drug abuse on a physical level, but should include assessing how the environment contributes to the user's struggle with addiction and hence broaden the professional service provided (Fleisher & Feldman, 1999:1). Change in lifestyle can be achieved by applying the BPS model whereby the nyaope user's recovery process will be inclusive of all aspects as outlined in the model. The BPS model suggests that a change in lifestyle could take place when the user has been dealt with holistically during treatment. This might mean developing a balance between work and family life, adopting pro-health habits, and learning to cope effectively with everyday stressors. According to the model, service users should focus on maintaining a balanced lifestyle and be aware when their lifestyle is becoming unbalanced (Nelson, 2012:128).
Sub-theme 2.2: Volunteering opportunities
It was indicated that the only thing that hinders users from being reintegrated into communities is lack of trust from community members. Users need to be given volunteering opportunities so that they can be able to regain the trust of community members. In this regard, volunteering opportunities are associated with creating community awareness of nyaope. Some of the participants' views included:
"If he can talk to the community, when he came back from treatment the first time, he went to schools and motivated learners."
"I want my child to be allowed to talk to other children in the community, tell them about the results [consequences] of nyaope."
As stated in the Prevention of and Treatment for Substance Abuse Act 70 of 2008, Section 30(2), service users should be allowed to share long-term sobriety experiences. Such experiences could be shared during awareness campaigns that are often run at local schools and the community at large. This could yield positive results for the users as it can help in rebuilding their lives and consolidating their reintegration into society (Gossop, Stewart & Marsdan, 2007:59).
Theme 3: Type of support needed to maintain abstinence
The significant others indicated that nyaope users require help in order for them to maintain abstinence. They highlighted the need for support on the psychosocial, emotional and spiritual levels.
Sub-theme 3.1: Psychosocial and emotional support
The participants highlighted the importance of psychosocial support for nyaope users. The majority indicated that psychotherapy should be offered pre- and post-treatment during group sessions. This finding is in line with the statement by Meyer (2005:292) that treatment of substance addiction should include preparation for treatment, treatment itself and also aftercare services to ensure that the dependent individuals develop skills to maintain sobriety. The participants understood emotional support to mean support from their significant others. Family involvement and support form part of aftercare and reintegration services (Maluleke, 2013:86). Some of the participants' views are:
"They can give him advice and coach him on life in general."
"These children need to attend group sessions after rehab."
"I want social workers to advise him, make him see that what he is doing is wrong."
"He needs to get support from us but he must be willing to get healed from addiction ways."
Social welfare services in general have the statutory obligation to provide aftercare and reintegration services to promote their clients' acquisition of housing, work or education after discharge. The service users should acquire personal support or treatment in order to 'escape' their substance dependency (Ekendahl, 2009:260). Additionally, family members should not enable the user to buy drugs by offering financial support. Furthermore, significant others could use language that demotivates users from using nyaope and encourage them to change their habits (Swarthout, 2016:150).
Sub-theme 3.2: Spiritual support
The participants also discussed the needs of the nyaope users for spiritual intervention in order to maintain sobriety. Spiritual support and the users' involvement in church activities and spiritual growth are vital elements and could help the users to abstain. Some of the participants' views are quoted below:
"Church can keep him busy, because he will be encouraged there."
"My son's behaviour needs God's intervention; I believe God will help him this time so that he remains clean from nyaope."
Another study indicated that when parents realise that their children's addiction is persisting despite talking to them, they tried to get religious help from faith-based organisations (Masombuka, 2013:93). This finding concurs with the finding of this research that the significant others regarded spiritual support as beneficial in maintaining the abstinence of nyaope users. Spiritual activities are a valuable factor contributing to successful completion of therapy (Morris et al., 2013:79).
In the next section the data obtained from nyaope users and significant others are triangulated (i.e. data triangulation). In the context of this qualitative study data triangulation should be interpreted as the collection of data from multiple sources, specifically different participants (i.e. nyaope users and significant others), to offer an exhaustive answer to the research questions and outlining the similarities and differences in the findings (Anney, 2014:277; Oliver-Hoyo & Allen. 2006:43).
Data triangulation
Similarities and differences between the findings pertaining to the nyaope users and significant others are discussed below.
Similarities of data from nyaope users and significant others
One similarity between the two groups of participants is that both were of the view that nyaope users do not get adequate support from the family and government to enable abstinence. The nyaope users identified triggers that caused them to relapse and highlighted the importance of involving family members to take part in preparatory groups that are held prior to treatment as well as in groups after treatment. Comprehensive intervention by the government will mean that an aftercare programme includes a life skills programme and therapeutic interventions are implemented after treatment. It was believed that nyaope users would be able to adapt to a new lifestyle provided that they undergo the skills programme. Both groups were of the view that employment opportunities that are accessible to the users after treatment could keep them busy and would be a constructive solution.
Another similarity that was identified was that the users need spiritual intervention in order for them to maintain abstinence. Some participants indicated that spiritual intervention should be implemented from the early stages of treatment, in the pre-sessions, during treatment at the centre and as part of the aftercare programme.
Furthermore, both groups indicated that nyaope users need to build trust among the community members. In regaining this trust, nyaope users need to be given volunteering opportunities after their treatment. In addition, the point was made that the users should stop stealing from community members in order for this trust to be rebuilt. It was also suggested that communities should be included in the recovery process of nyaope users.
Differences of data from nyaope users and from significant others
Users are overwhelmed by the challenges they face in their own lives, their families and in the communities they live in. Users resort to smoking nyaope to cope with their problems and to ease their burdens. The problems identified include financial challenges and spousal relationships. Moreover, nyaope users also indicated that they are often coerced into going for treatment. They stressed that it is crucial for the user to go to the treatment centre voluntarily. The seriousness and level of determination of the user to quit the drug will determine how positive the results will be. The users also felt strongly that the duration of treatment should be increased as the current period was considered too short and not successful. On the other hand, the significant others of the users indicated that they are hurt and frustrated by the users' addiction and therefore they end up coercing them to get the necessary help to quit the drug, even when they are not ready. One significant other felt that nyaope users should be admitted to a treatment centre through a binding court order as a way of preventing relapse, as stated in the Prevention of and Treatment for Substance Abuse Act 70 of 2008, Section 33.
CONCLUSIONS
Although the findings were derived from one township, attempts to ensure the trustworthiness of the study increase the potential of the conclusions and recommendations to be applicable to nyaope users in other townships of South Africa.
Addressing the identified causes of relapse could ensure long-term recovery of the users. The limited involvement of the whole family affects the users and the outcome of the treatment negatively. The users' willingness to undergo treatment could be beneficial in avoiding relapse. The practice of spirituality within one's daily routine is significant to solidifying a foundation for a positive recovery cycle. The effectiveness of aftercare programmes is jeopardised as a result of irregular or non-existent monitoring and evaluation practices and consequently the programmes are often poorly attended. Change in lifestyle entails dismantling old friendships that may trigger cravings and result in relapse.
The government's attempts to curb the scourge of substance abuse are inadequate in the community. Returning to the same environment after treatment is not conducive to assisting users to recover, as drugs are easily accessible. The unemployed youths are tempted to resort to drug abuse to deal with the boredom that comes with unemployment and lack of educational activities. It seems that vocational training and job opportunities ought to be prioritised by the government to help recovering addicts remain clean.
Nyaope users value the trust of the community and this could be used to develop an appropriate aftercare programme for users and to reintegrate them back into the community. It seems important that the substance-dependent person should assume new roles and responsibilities when they have been reintegrated into the community, so that they can regain the trust of community members. Among other things, changes in lifestyle, dismantling old friendships and stopping theft were identified as avenues to pursue building up trust.
The significant others of nyaope users have insights into the challenges of the users and therefore they were able to make recommendations with regards to what is required for nyaope users to abstain; these recommendations could inform aftercare and reintegration services.
RECOMMENDATIONS
Recommendations to relevant role players pertaining to the aftercare and reintegration needs of nyaope users are outlined below.
-
The Department of Sports and Recreation should create recreational activities that could keep youths occupied during the day.
-
The Department of Public Works should create employment opportunities and make them accessible to nyaope users following treatment - for example, linking them purposefully to the Expanded Public Works Programme.
-
The South African Police Services should work on reducing the quantity of drugs available on the streets of Hammanskraal; the suppliers of nyaope must be arrested and prosecuted.
-
The Department of Social Development should consider increasing the duration of treatment from six weeks to a more adequate period, for example, six months, because a high relapse rate is witnessed following the six-week period, perhaps because the treatment period is too short.
-
Education and awareness in communities on the impact of nyaope use should be a core element in the prevention of use and relapse, as the participants prioritised this.
-
Because nyaope users are shunned and shamed by community members, it is crucial for communities to be educated on reintegration services for nyaope users and the benefits of this in the recovery process.
-
Involvement of religious institutions should be strengthened. The role/impact of spirituality and religion should be investigated and be incorporated into aftercare and reintegration programmes.
-
Family members need to be empowered through life skills education in preparation for them to be part of the recovery process of the nyaope user.
-
Social workers need to attend capacity-building workshops that stress the importance of aftercare services to addicted persons and empower them with the necessary knowledge and skills to deliver appropriate aftercare and reintegration services.
-
Emotional support to nyaope users should be provided by both social workers and significant others.
-
As the main employer of social workers, the DSD should deliver a clear aftercare and reintegration programme and monitor it, as it should aim at teaching life skills and coping strategies to nyaope users.
-
Nyaope users emphasised that they relapsed because they were not prepared for treatment. Therefore, social workers should be trained and use motivational interviewing to prepare service users adequately for treatment in order to prevent relapses.
-
More referrals to a treatment centre should be done through Section 33 of the Prevention of and Treatment for Substance Abuse Act 70 of 2008, i.e. admission of involuntary service users to treatment centres to ensure that users complete the treatment period.
-
Awareness programmes should be strengthened in which nyaope users who have completed treatment could raise awareness at local schools.
-
More research needs to be conducted among all ethnic groups in order to reflect the demography of the diverse population of South Africa.
-
Future research needs to target female users in particular to obtain their perspectives as well.
-
Through intervention research, an effective aftercare and reintegration programme for nyaope users in the Gauteng province, and the rest of South Africa, could be developed and standardised.
Although the gold standard should be the prevention of all forms of drug abuse, the reality is that South African townships witness high levels of drug abuse, especially of the cheaper types of drugs such as nyaope. Consequently, many young people are addicted to nyaope and require treatment. It is incumbent on social workers to take the lead to ensure that through service delivery and building partnerships with all role players, nyaope users receive adequate and relevant aftercare and reintegration services so as to enable them to reach their full potential in life, become active citizens in society, and make a contribution towards their own wellbeing and the social development of the country.
REFERENCES
ALVAREZ, A.S., PAGANI, M. & MEUCCI, P. 2012. The clinical application of the biopsychosocial model in mental health a research critique. American Journal of Physical Medicine & Rehabilitation, 91(2):173-180. [ Links ]
ANNEY, V.N. 2014. Ensuring the quality of the findings of qualitative research: looking at trustworthiness criteria. Journal of Emerging Trends in Educational Research and Policy Studies, 5(2):272-281. [ Links ]
BERNARD, H.R. 2000. Social research methods: Qualitative and quantitative approaches. California: Sage Publications. [ Links ]
CHUI, W.R. 2016. Probation and community service orders: Understanding criminal justice in Hong Kong. [Online] Available: http://books.google.co.za/books?hl=en&. [Accessed: 30/08/2017]. [ Links ]
CLARKE, V. & BRAUN, V. 2013. Teaching thematic analysis: Overcoming challenges and developing strategies for effective learning. The Psychologist, 26(2):120-123. [ Links ]
CRESWELL, J.W. 2009. Research design: Qualitative, quantitative and mixed methods approaches. (3rd ed). London: Sage Publications. [ Links ]
DADA, S., HARKER BURNHAMS, N., ERASMUS, J., PARRY, C., BHANA, A., TIMOL, F. & FOURIE, D. 2017. Monitoring alcohol, tobacco and other drug use trends in South Africa: July -December 2016. South African Epidemiology Network on Drug Use (SACENDU), Research Brief, 20(1):1-19. [ Links ]
DEPARTMENT OF SOCIAL DEVELOPMENT. 2013a. National Drug Master Plan 2013-2017. [Online] Available: http://www.dsd.gov.za/index*2.php?.php=comdocman&task=docvie w&gid=414&itemid=3 [Accessed: 12/02/2014]. [ Links ]
DEPARTMENT OF SOCIAL DEVELOPMENT. 2013b. Framework for Social Welfare Services. Pretoria: Government Printer. [ Links ]
DEPARTMENT OF SOCIAL DEVELOPMENT. 2016. Department of Social Development Annual Performance Plan 2015-16. [Online] Available: http://www.socdev.gpg.gov.za/...final%20annual%20 perfomance%20report [Accessed: 11/10/2016]. [ Links ]
DOGAR, I.A. 2007. Biopsychosocial model. A.P.M.C, 1(1):11-13. [ Links ]
EKENDAHL, M. 2009. Alcohol abuse compulsory treatment and successive aftercare: A qualitative study of client perspectives. International Journal of Social Welfare, 18(1): 260-269. [ Links ]
FERNANDES, L. & MOKWENA, K.E., 2016. The role of locus of control in nyaope addiction treatment. South African Family Practice, 58(4):153-157. [ Links ]
FISHER, G.L. & HARRISON, T.C. 2013. Substance abuse: Information for school counsellors, social workers, therapists and counsellors. (5th ed). Boston: Pearson. [ Links ]
FLEISHER, D.R. & FELDMAN, E.J.1999. The biopsychosocial model of clinical practice in functional gastrointestinal disorders. In: HYMAN, P.E. (ed), Paediatric functional gastrointestinal disorders. New York: Academy Profession Information Services. [ Links ]
GABBARD, G.O. & KAY, J. 2001. The fate of integrated treatment: Whatever happened to the biopsychosocial psychiatrist? Am J Psychiatry, 158(12):1956-1963. [ Links ]
GALANTER, M., DERMATIS, H., BUNT, G., WILLIAMS, C., TRUJILLO, M. & STEINKE, P. 2007. Assessment of spirituality and its relevance to addiction treatment. Journal of Substance Abuse Treatment, 33(3):257-264. [ Links ]
GEYER, S., LE ROUX, L., & HALL, H. 2015. Exposure to substance use in the social environment: The experiences of adolescents in the Tshwane metropole. The Social Work Practitioner-Researcher, 27(3):322-343. [ Links ]
GHOSH, P. 2013. Nyaope: cheap drug cocktail ravaging black townships of South Africa. [Online] Available: http://www.16times.com/nyaope-cheap-drug-cocktail-review [Accessed: 24/10/2015]. [ Links ]
GOSSOP, M., STEWART, D. & MARSDAN, J. 2007. Attendance at narcotics anonymous meetings, frequency of attendance and substance use outcomes after residential treatment for drug dependence: A five year follow up study. Addiction, 103:119-125. [ Links ]
GROENEWALD, C.R. & BHANA, A. 2016. "It was bad to see my [child] doing this": Mothers' experiences of living with adolescents with substance abuse problems. International Journal of Mental Health Addiction, 14(5):646-661. [ Links ]
HEALTH24. 2014. Is nyaope South Africa's worst drug? [Online] Available: http://www.health24.com [Accessed: 04/09/2017]. [ Links ]
LARIMER, M.E., PALMER, R.S. & MARLATT, G.A. 1999. Relapse prevention: An overview of Marlatt's cognitive-behavioural model. Alcohol Research & Health, 23(2):151-160. [ Links ]
LEBESE, R.T., RAMAKUELA, N.J. & MAPUTLE, M.S. 2014. Perceptions of teenagers about substance abuse at Muyexe village, Mopani district of Limpopo Province, South Africa. African Journal for Physical, Health Education, Recreation and Dance, 1(2):329-347. [ Links ]
LIETZ, C.A. & ZAYAS, L.E. 2010. Evaluating qualitative research for social work practitioners. Advances in Social Work, 11(2):188-202. [ Links ]
MAKHUBELA, R.M. 2015. Interview with social worker, Department of Social Development. 17 March. Soshanguve. [ Links ]
MALULEKE, T.F. 2013. Perceptions of social workers regarding their role in aftercare and reintegration services with substance-dependent persons. Pretoria: University of Pretoria. (MSW Mini-Dissertation) [ Links ]
MAREE, A. 2013. Criminogenic risk factors for youth offenders. In: Bezuidenhout, C. (ed) Child and youth misbehaviour in South Africa: a holistic approach. (3rd ed). Pretoria: Van Schaik. [ Links ]
MASOMBUKA, J. 2013. Children's addiction to the drug "nyaope" in Soshanguve township: parents' experiences and support needs. Pretoria: University of South Africa. (MA Dissertation) [ Links ]
MASON, S.J., DEANE, F.P., KELLY, P.J. & CROWE, T.P. 2009. Pilot study: spirituality and religiosity. Substance Use & Misuse, 44(1):1926-1940. [ Links ]
McKAY, J.R. 2001. Effectiveness of continuing care interventions for substance abusers: Implications for the study of long-term treatment effects. Evaluation Review, 25(2):211-232. [ Links ]
MERRIAM, S.B. 2009. Qualitative research and evaluation methods. (3rd ed). Thousand Oaks, CA: Sage Publications. [ Links ]
MEYER, R. 2005. Towards a rational approach to substance abuse behaviour. CME: Your SA Journal of CPD, 23(6):290-293. [ Links ]
MOKWENA, K.E. & FERNANDES, L. 2014. Exploring the role of external locus of control in the use of nyaope: a qualitative enquiry. Botswana Journal of African Studies, 28(1):41-50. [ Links ]
MOKWENA, K. & MOROJELE, N. 2014. Unemployment and unfavourable social environment as contributory factors to nyaope use in three provinces of South Africa. African Journal for Physical, Health Education, Recreation and Dance, 1(2):374-384. [ Links ]
MOLEFE, J.M. 2014. Interview with social worker, Department of Social Development. 26 February. Themba. [ Links ]
MOODLEY, S.V., MATJILA, M., & MOOSA, M.Y.H. 2012. Epidemiology of substance use among secondary school learners in Atteridgeville, Gauteng. SAJP, 18(1):4-9. [ Links ]
MORRIS, D.N., JOHNSON, A., LOSIER, A., PIERCE, M. & SRIDHAR, V. 2013. Spirituality and substance abuse recovery. Occupational Therapy in Mental Health, 29(1):78-84. [ Links ]
MZOLO, M.P. 2015. Exploring family support for adolescents after rehabilitation for drug abuse. Pretoria: University of South Africa. (MA Dissertation) [ Links ]
NELSON, A. 2012. Social work with substance users. Los Angeles: Sage Publications. [ Links ]
NXUMALO, Z. & GARE, L. 2015. Community tourism in Hammanskraal (Gauteng). [Online] Available: http://www.gttp.org/wp-content/upload/2015/08/04/SAP [Accessed: 12/10/2016]. [ Links ]
OLIVER-HOYO, M. & ALLEN, D. 2006. The use of triangulation methods in qualitative educational research. Journal of College Science Teaching, 35(4):42-47. [ Links ]
PADGETT, D.K. 2017. Qualitative methods in social work research. (3rd ed). Thousand Oaks, CA: Sage Publications. [ Links ]
PEYPER, L. 2017. Only 4 in 10 people of working age have a job - report. [Online] Available: http://www.fin24.com/economy/only-4-in-10-people-of-working-age-have-a-job-report-20170821 [Accessed: 04/09/2017]. [ Links ]
POPOVICI, I., FRENCH, M.T. & McKAY, J.R. 2008. Economic evaluation of continuing care interventions in the treatment of substance abuse: Recommendations for future research. Evaluation Review, 32(6):547-568. [ Links ]
REPUBLIC OF SOUTH AFRICA (RSA). 1997. Ministry for Welfare and Population Development.1997. White Paper for Social Welfare. (Government notice 1108 of 1997, Government Gazette, 386 (18166)). Pretoria: Government Printer. [ Links ]
SINHA, R. 2001. How does stress increase risk of drug abuse and relapse? Psychopharmacology, 158(4):343-359. [ Links ]
SOEKER, S., MATIMBA, T., MACHINGURA, L., MSIMANGO, H., MOSWANE, B & TOM, S. 2016. The challenges that employees who abuse substances experience when returning to work after completion of employee assistance programme (EAP). IOS Press, 53(3):569-584. [ Links ]
SWANEPOEL, I. 2014. The causes of relapse amongst young African adults following in-patient treatment for drug abuse in the Gauteng Province. Pretoria: University of Pretoria. (MSW Mini-Dissertation) [ Links ]
SWANEPOEL, I., GEYER, S. & CRAFFORD, G. 2016. Risk factors for relapse among young African adults following in-patient treatment for drug abuse in the Gauteng Province. Social Work/Maatskaplike Werk, 52(3):414-438. [ Links ]
SWARTHOUT, J. 2016. Getting a loved one started in recovery: invitational intervention. [Online] Available: www.fireengineering.com [Accessed: 22/08/2016]. [ Links ]
THOTHELA, S., VAN DER WATH, A.E. & JANSE VAN RENSBERG, E.S. 2014. Factors contributing to relapse of mental health care users treated for substance induced psychotic disorder in a psychiatric hospital in Gauteng, South Africa. African Journal of Nursing and Midwifery, 16(1):15-88. [ Links ]
VAN DER WESTHIZEN, M.A. 2010. Aftercare to chemically addicted adolescents: Practice guidelines from a social work perspective. Pretoria: University of South Africa. (D Phil) [ Links ]
VAN DER WESTHUIZEN, M., ALPASLAN, A.H. & DE JAGER, M. 2013. Aftercare to chemically addicted adolescents: an exploration on their needs. Health SA Gesondheid, 18(1):1-11. [ Links ]
VAN DER WESTHUIZEN, M., ALPASLAN, A. & DE JAGER, M. 2011. Preventing relapses amongst chemically addicted adolescents: exploring the state of current services. Social Work/Maatskaplike Werk, 47(3):350-370. [ Links ]
VAN DER WESTHUIZEN, M. & DE JAGER, M. 2009. Relapsing after treatment: Exploring the experiences of chemically addicted adolescents. Social Work/Maatskaplike Werk, 45(1):76-90. [ Links ]
VAN WORMER, K. & DAVIS, D.R. 2013. Addiction treatment: A strengths perspective. (3rd ed). Belmont: Brooks/Cole, Cengage Learning. [ Links ]
WORLD ECONOMIC FORUM. 2014. The global competitiveness report 2014-2015. [Online] Available: www.weforum.org/gcr [Accessed: 09/11/2017]. [ Links ]
YIN, R.K. 2003. Case study research: Design and methods. (3rd ed). Thousand Oaks, CA. Sage Publications. [ Links ]


{kind=link}
{kind=link}