










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSocial Work
versão On-line ISSN 2312-7198
versão impressa ISSN 0037-8054
Social work (Stellenbosch. Online) vol.54 no.2 Stellenbosch 2018
http://dx.doi.org/10.15270/52-2-635
ARTICLES
Surviving a laryngectomy: the views of post-operative cancer patients and their families
Hendriëtte Steyn; Sulina Green
Department of Social Work, Stellenbosch University, Stellenbosch, South Africa
ABSTRACT
Major advances in cancer detection and treatment options have now afforded cancer patients the prospect of a longer life. This places various demands upon patients, families and social workers in the field of oncology. A combination of quantitative and qualitative research approaches was used to explore the survivorship experiences of patients and families who presented with an advanced stage of larynx cancer, where a total laryngectomy was indicated, implying removal of the entire larynx. Findings of the study reveal that patients and families mobilise both inner strengths and social support to adapt to inevitable physical changes that follow a laryngectomy.
"You have to become used to it [laryngectomy experience] yourself. You first keep to yourself as you do not want others to know what is wrong. Later on you re-integrate and as you become used to it you totally come back again"
INTRODUCTION
The desire and need to survive can be seen as a central characteristic shared by all human beings (Rom, Miller & Peluso, 2009:27). This study focuses on the survivorship experiences of patients (and their families) who presented with an advanced stage of larynx cancer where a total laryngectomy was indicated, implying removal of the entire larynx (Casper & Colton, 1998:1).
BACKGROUND
The most common risk factors for cancer of the head and neck region include the use of tobacco and alcohol, but Woodard, Oplatek and Petruzzelli (2007:526) warned that anyone can be at risk of such a cancer. The literature indicates that male smokers between the ages of 45 and 75 years are generally more vulnerable to cancer of the larynx (Casper & Colton, 1998:7; Ross, 2000:13). Owing to the fact that this disease mostly occurs in late middle age, it can be typified as a disease of the elderly (Deshmane, Parikh, Pinni, Parikh & Rao, 1995:121; Renner, 1995:216; Ross, 2000:14). Besides substance abuse, other social factors such as low socio-economic status, low levels of education, a generally poor social network and poor coping skills are also detected among patients presenting with cancer of the head and neck region (Cady, 2002:347; Eadie & Doyle, 2005:120).
Following surgery, patients have to breathe through a permanent tracheostoma (Graham, 2004:126), which now provides the only airway to the lungs (Ross, 2000:15). These patients no longer inhale through the nose and pharynx, and exhale from the lungs to the nose and mouth. For normal speakers, pulmonary air supports both life and speech, but for the laryngectomy patient, life breathing and speech breathing are distinctly separate activities (King, Marshall & Gunderson, 1971:113).
Consequences and challenges of cancer and treatment
Hoffman's (1989:85) observation that "survivors" entire lives, not just their cells, are affected by their cancer diagnosis" emphasised the comprehensive impact of cancer and its treatment on cancer survivors. In line with this, Haylock, Mitchell, Cox, Temple and Curtiss (2007:62) held the opinion that, following a diagnosis of cancer, patients may have to deal with a "new normal" life instead of their previous "old normal" life. Especially in the case of laryngectomy patients and their families, many of these survivors have great difficulty in adjusting to the physical and lifestyle changes following surgery (Johnson, Casper & Lesswing, 1979:1813).
Survivorship
The National Coalition for Cancer Survivorship (NCCS) defines survivorship as "the journey that a person takes from the moment of diagnosis onward". On this journey survivors have to pass "through a common progression of events", which can be perceived as a unique experience (Miller, Merry & Miller, 2008:369). A wide variety of authors in the literature were in agreement in defining the beginning and endpoint of survivorship as extending from the time of diagnosis onward through the rest of the cancer patient's life (Griffin-Sobel, 2005:509; Haylock, 2006:16; Kaplan, 2008:989; Quigley, 1989:63; Rowland, 2008:362).
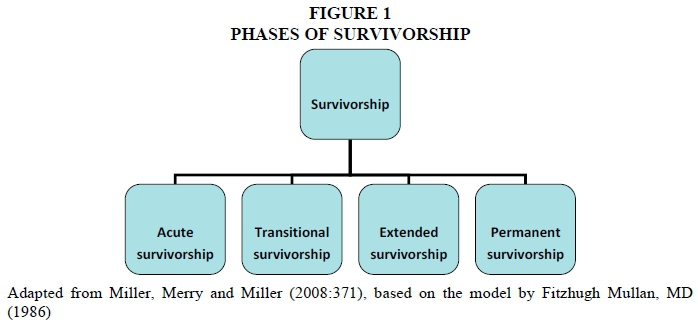
In describing the progression through this cancer journey, Miller et al. (2008:369-374) referred to Fitzhugh Mullan's (1986) proposed "seasons of survivorship", categorised as "acute", "extended" and "permanent survivorship". Miller et al. (2008:369, 372) added the season of "transitional survivorship" between "acute" and "extended survivorship", meaning the transition from active treatment to careful observation, which includes the emotional, social and medical adaptations that may occur. These phases of survivorship are illustrated in Figure 1.
For the laryngectomy patient, acute survivorship starts at the stage of diagnosis, followed by medical treatment, such as surgery (laryngectomy) and post-operative radiotherapy (if indicated). During the transitional phase of their survivorship journey, laryngectomy patients have to adjust to the comprehensive effects of surgery and have to attend follow-up visits at the clinic. The extended phase of their survivorship journey alludes to their post-operative rehabilitation by recovering from treatment and their ability to cope with these effects. Eventually, survivors will be challenged with their re-entry into society, which represents the permanent survivorship phase of their survivorship journey.
Increased life expectancy
Because of the advances in screening and detection of cancer, improved medical treatment options and better supportive care, cancer patients have an increased life expectancy (Alfano & Rowland, 2006:432; Rowland, 2008:361). This phenomenon of prolonged survivorship tends to challenge laryngectomy patients, their families and multidisciplinary team members in various ways. First, patients have to cope, throughout their increased life expectancy, with the comprehensive physical, social and psychological impact of cancer and its treatment.
Second, extended survivorship affects the family system as a whole. Patients are now dependent on and exposed to their family and other support systems for a longer period of time. Families may experience difficulty in dealing with this demand as they are not always equipped to handle the side-effects of the operation (Blanchard, 1982:240). Consequently, Feuerstein (2007:5) included families in an attempt to explain survivorship. Families of cancer survivors can also be referred to as "secondary survivors", as they too often face long-term consequences of the patient's survivorship (Haylock, 2006:16; Kaplan, 2008:989; Rowland, 2008:362). For this reason families of patients are included in research when exploring and describing the experiences of laryngectomy patients.
Third, prolonged survivorship also affects the role of the social worker functioning as part of the multidisciplinary team in a hospital. Patients will remain in the hospital setting for a longer period while they attend the follow-up clinic, where they will receive aftercare and support services from the multidisciplinary team. Social workers should take note of Alfano and Rowland's (2006:439) observation that "treating cancer alone is no longer enough; we now must also focus on the goal of helping those living with and beyond a cancer diagnosis to lead full, productive, and meaningful lives". The literature (Casper & Colton, 1998:35, 50; Dhooper, 1985:220-225; Johnson et al, 1979:1816) emphasises the important role that social workers, as part of the team, have to play and the need for them to be equipped with interpersonal skills to adequately address these needs of patients. From the above it is evident that prolonged survivorship presents challenges for patients, their families and social workers.
To meet these demands patients and their families need professional guidance from social workers and multidisciplinary team members for a longer period after surgery (De Boer, Pruyn, Van den Borne, Knegt, Ryckman & Verwoerd, 1995:503). Consequently, the goal of this study was to gain a better understanding of the experience of post-operative laryngectomy patients and their families during the various survivorship phases in order to make recommendations to social workers dealing with survivorship issues in the field of oncology.
RESEARCH METHODOLOGY
A combination of qualitative and quantitative research approaches was used (Fouché & De Vos in De Vos et al., 2011:90, 92). As the qualitative approach aims to understand social life and the meaning people attach to everyday life (Fouché & Delport in De Vos et al., 2011:65), implementation of this approach contributed towards developing a better understanding of ways in which primary and secondary laryngectomy survivors make sense of their survivorship experience (Garbers, 1996:283). In the quantitative approach the aim is to objectively measure the social world (Fouché & Delport, in De Vos et al., 2011:64), while the researcher remains in the background without becoming involved in the events or "object of study" (Garbers, 1996:282).
In addition, a combination of both exploratory and descriptive designs was applied to meet the objectives of the study. The exploratory design was used to gain new insights into psychosocial factors which may affect the patient's and family's survivorship journey. The descriptive design focused on "how" and "why" questions revolving around the issue "What are the experiences of the laryngectomy patient and family while surviving a laryngectomy?" The researcher observed the laryngectomy experience of both primary and secondary survivors and then described the details of the situation to present a complete picture of the situation (Babbie & Mouton, 2001:80; Fouché & De Vos, 2011:96; Garbers, 1996:287).
Purposive sampling was applied as a type of a non-probability sampling technique to ensure that rich detail was obtained to ensure a maximum range of specific information (Strydom & Delport, in De Vos et al., 2011:392). Only patients who had undergone their operation not less than three months before, who attended follow-up visits at the hospital, and who had successfully acquired trachea-oesophageal speech were included in the study. Forty-five patients participated. To ensure triangulation (Delport & Fouché, in De Vos et al., 2011:442-443), a sample of 15 family members, representing one third of the patients who participated in the study, were interviewed to record their experiences of coping with a laryngectomee in the family.
Various and unique challenges were encountered in selecting the research sample, such as the lack of contact numbers to arrange for interviews on the same date as patients' medical appointment at the clinic; their speech ability on the day of their follow-up visit as it is dependent on their medical condition and/or the condition of their speech valve; transport arrangements, as well as their compliance.
Face-to-face interviews were conducted with laryngectomy patients to obtain research data through a semi-structured questionnaire (Babbie & Mouton, 2001:249; Greeff, in De Vos et al., 2011:351-353; Grinnell, 1993:268). An interview schedule was used for interviews with family members. The focus of both instruments was to explore the experiences of the participants. All interviews were audio-taped with the permission of the participants and transcribed by the researcher (Greeff, in De Vos et al., 2011:359). The narratives of participants were classified into themes and sub-themes and further divided into categories (Fouché & Bartley, in De Vos et al., 2011:249).
The study was conducted at a selected hospital in the Western Cape Province in South Africa. Permission was obtained from the Ethics Committee of the University of Stellenbosch and the hospital to ensure that the rights and interests of participants were protected (Strydom, in De Vos et al., 2011:129).
RESEARCH FINDINGS AND ANALYSIS
The following section will present an analysis and discussion of the findings of the views of patients and their families, in the form of tables, illustrated with various narratives.
Profile of participants
The age of patients (n=45) who were selected for the study varied between 42 and 79 years, with an average of 62 years. Both male and female patients were involved; however, more males (82.2%) than females (17.8%) participated. The majority of participants were married (55.6%) or lived with a partner (17.8%). Widowed participants constituted 13.3%, those never married 8.9% and divorced 4.4%. More than a third (35.6%) of patients had primary school or no (20.0%) education and more than three quarters (80%) of patients became pensioners (civil or social) following their surgery. Patients identified participating family members, mostly spouses and life partners (66.7%), as those people who were primarily exposed to their laryngectomy and its aftermath.
Experiences of post-operative cancer patients and families
The views of participants (patients and families) about their needs, experiences, reactions and coping during the various phases of survivorship are presented below.
The need for information during the acute phase
As patients' medical diagnosis and treatment represent the acute phase of the survivorship journey, the need for pre-operative information can be established as the starting point of their journey.
The need for information in general
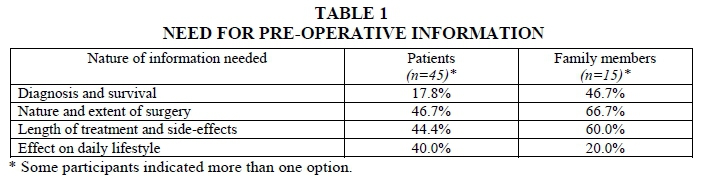
The majority (97.8%) of patients and family members expressed a need for general pre-operative information (Table 1).
-
Diagnosis and survival
Some (17.8%) patients required further information regarding their diagnosis. This included information about confirmation of, as well as causes of, the diagnosis ("I just wanted to know for sure whether I really had cancer"). Surprisingly, some patients related their diagnosis of larynx cancer to their previous social smoking habit. This view, which lists alcohol and tobacco as etiological factors commonly associated with a diagnosis of larynx cancer, is acknowledged by Cady (2002:347).
On a survival level, participants also wanted to know whether they could be cured ("I wanted to know whether and how I would be cured").
Of importance is that some (46.7%) family members also required further information with regards to the patient's diagnosis and survival. They experienced a lack of information as they had not been exposed to such a diagnosis in the past ("We did not have to deal with cancer in the past, we were very ignorant"). With regard to the survival of the patient, they also wondered about the success rate of the operation. It was Deimling, Bowman, Sterns, Wagner and Kahana (2006:307) who referred to diagnosis as a phase during which patients and families experience fear about the treatability of the disease, as well as prognosis and survival.
-
Nature and extent of surgery
With regards to the nature and extent of surgery, patients enquired about the availability of less invasive surgery and whether any alternative treatment options were available. In addition, patients were concerned about their post-operative physical appearance with specific reference to the tracheostoma. They questioned the need for the stoma ("... whether it was really necessary to make a hole in my throat") and its permanence. A family member also wanted to know how the operation would be done. This echoes research conducted by De Boer et al. (1995:507-508) regarding the rehabilitation outcome of long-term survivors treated for head and neck cancer, stating that the presence of the stoma constitutes the greater part of "damage" to laryngectomy patients' physical appearance.
-
Length of treatment and side-effects
Of the 44.4% of participants who commented on their need for pre-operative information with regards to the length of treatment and side-effects of the operation, only one participant was concerned about the length of treatment. Almost half (42.2%) of the patients wanted more information on the effect the operation would have on their speech ability ("... how I would manage to talk again?"), while nine (60.0%) of the family members also needed more information in this regard.
-
Effects on daily life-style
The effect of the operation on daily activities such as eating, drinking and swallowing was the patients' main concern. They also wanted more information on the impact of the operation on their ability to work again and the continuation of pleasurable things like singing, joking and recreational activities ("I will be cut off ^from the things I loved to do ").
Surprisingly, only a few (20%) family members were concerned about the effect on daily activities; their greatest need was to know how to take care of the patient ("I wanted to know how I have to handle him"). Taking into account that survivors' life expectancy is increasing, Golant and Haskins (2008:420) found that family members will need to take care of patients for longer periods of time, with increasing pressure on them.
Pre-operative information offered by team members
Patients' experiences of the degree to which team members' explanations had helped them prior to their surgery varied as are reflected in Table 2.
-
Fully informed
The majority of participants (60.0%) reported that the team members' explanations of the operation fully prepared them for the process and found the way in which information was conveyed very helpful. They were satisfied that all their questions were answered, team members were not hesitant to answer questions and full explanations were provided. Another aspect which was important to them was that the various steps in this process were repeatedly and continuously explained ("The doctor did not only explain to me once, I think it was two or three times"). Because these steps were adhered to, patients felt secure and were always aware of what the doctors planned to do. In the end patients realised that, although the effect of the operation was permanent, a laryngectomy was the best option, because it had saved their lives and they were thankful for this ("After they informed me what they are going to do, Ifelt calm ").
-
Partially informed
Patients (35.6%) who indicated that they were only partially informed needed more information on the presence of the permanent tracheostoma, the effect of the operation on their speech, the impact on their daily activities, as well as about the physical consequences of the operation in general. They also felt uncertain about their eating and drinking ("They did not explain to me ... that I could eat although I had the pipe"), incidence of heartburn, how to manage a blocked stoma; how to deal with problems associated with the speech valve and more information on the length of their stay in hospital after surgery.
-
Not informed at all
A few (4.4%) participants who had a short interval between diagnosis and operation (43 days and 6 days respectively) felt that team members did not prepare them at all for the impact of the operation. The short time interval between diagnosis and surgery could have added to their level of stress at that stage (Chen, Tsai, Liu, Yu, Liao & Chang, 2009:478-9). Although Zeine and Larson (1999:59-60) emphasised the importance of adequate pre-operative counselling, a few (6.7%) participants reported that too much information could have resulted in their refusing the operation ("Maybe they thought it will frighten me"). Ross (2000:14) warned that patients and families may not be able to assimilate a great deal of information shortly before surgery, because their emotional state might affect their ability to "hear" or absorb this information (Zeine & Larson, 1999:59).
Emotional reactions to information received
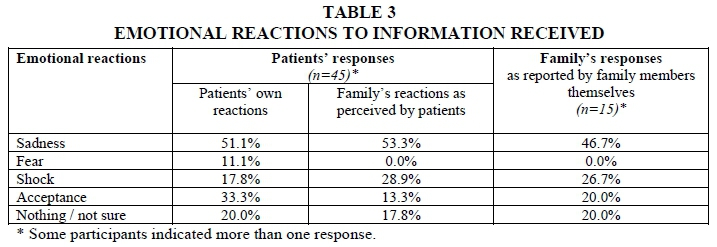
McQuellon and Hurt (1997:231) pointed out that a diagnosis and treatment of cancer is almost always an emotionally traumatic experience. This is especially true in the case of cancer of the head and neck area, because of its life-threatening nature and the threat of potential disfigurement and dysfunctioning. First, patients reported about their own emotional reaction at this time. They then described how they thought their families felt. Lastly, families described their emotional reactions at this stage. Patients and family members supplied a wide variety of responses to describe their feelings at the time of diagnosis and on being informed of the proposed surgery, as reflected in Table 3.
Emotional experiences of patients and families upon being informed of the diagnosis of cancer, varied from sadness, fear and shock to acceptance. Others could not classify their emotional reaction. Responses from patients and their families were largely similar, but an interesting finding was that families experienced shock to a greater extent than patients. Patients, on the other hand, experienced greater acceptance of information than family members did. This might be attributed to the fact that elderly survivors tend to be less affected by a diagnosis of cancer (Foster, Wright, Hill, Hopkinson & Roffe, 2009:243), since they might be accustomed to handling negative events in their lives and are not subject to the pressure of fulfilling multiple, competing roles as might be the case with younger survivors (Hara & Blum, 2009:47).
Physical readjustment during the transitional phase
During the transitional phase of their survivorship journey, patients and families have to deal with the reality of certain permanent physical changes (Miller et al., 2008:372).
Permanent physical changes most difficult to deal with
Almost half of the patients (44.4%) experienced extreme difficulty with their sensory functioning such as their inability to smell and taste. According to the literature (Lennie, Christman & Jadack, 2001:668, 673), a decreased ability to taste and smell is due to the olfactory process being destroyed during surgery. Loss of smell has far-reaching implications resulting in issues of safety, hygiene and a limited response to pleasurable odours. This was followed by extreme difficulties with post-operative speech (33.0%) and problems with eating and drinking (27.4%). Problems experienced with physical appearance (22.2%) and the permanent tracheostoma (21.2%) were of less importance. (Take into consideration that participants could supply more than one answer to each category).
About two-thirds (66.7%) of family members acknowledged that they found the adaptation to the patient's post-operative speech ability the most difficult physical change to adjust to, followed by the presence of the permanent tracheostoma (40%) ("The stoma because of all the mucus which exits through the stoma"). One family member (6.7%) referred to the fact that her husband reacted "like a child" as he did not want to be alone. In the words of the participant: "My husband cannot talk now. He is almost like a child ... he does not want to be alone, he does not want to be with people ... because he was always a man who could talk."
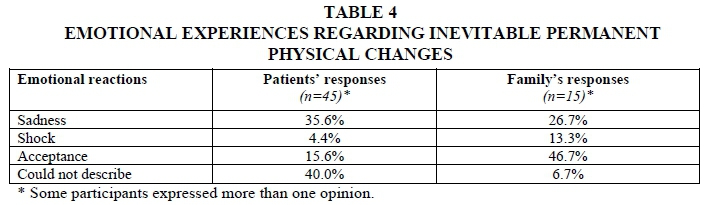
Emotional experiences regarding inevitable permanent physical changes
Patients' and families' emotional experiences when having to deal with inevitable permanent physical changes caused by the operation are presented in Table 4.From Table 4 it is clear that the majority of patients could not describe their emotional experiences and referred to the fact that they felt "different" or could not describe their feelings (40.0%), or they experienced sadness (35.6%). Most family members, on the other hand, accepted the permanent physical changes caused by the operation (46.7%).
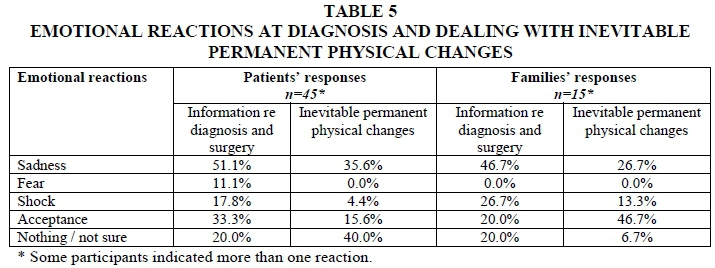
When comparing the emotional reactions of patients and families of survivors between the stages of being informed of the cancer diagnosis and having to adjust to inevitable permanent physical changes following surgery, interesting differences were found between the reactions of primary and secondary survivors. A summary of these responses is presented in Table 5.
Upon diagnosis of cancer, patients experienced feelings of sadness, but this changed to them saying that they "were not sure" of their feelings after surgery. They also experienced feelings of sadness, because they knew they had to face the reality of the inevitable permanent physical changes resulting from the operation. Family members experienced sadness when informed about the operation, but these feelings changed to acceptance when they realised that they had to deal with permanent physical changes in their relative.
The time lapse between the date of the patient's laryngectomy and date of interview with the family member varied between 10 and 138 months, with an average period of five years. Research conducted by De Boer et al. (1995:503) found that the greater the time that elapsed since treatment, the fewer the psychosocial problems associated with the condition. Since the patient's family is part of the ecological system within which the patient functions, this is also relevant to the family members involved (Germain & Gitterman, 1996:5-6).
Pre-operatively, it was more important for family members to have more information about the diagnosis and survival of the patient than it was for the patients themselves (table 5). It was more important for the family to know that the patient could be cured from cancer than to be emotionally affected by the inevitable permanent physical changes following the operation.
Coping and strengths during the extended phase
It is during the extended phase of survivorship that patients have to cope with emotions connected to physical changes caused by the operation, during treatment until completion and readjustment after the operation, and aftercare.
Coping with permanent physical changes caused by the operation
Most patients used both inner resources (inner strengths) and environmental resources (social support) in their attempt to cope with the physical changes, which illustrates the value of utilising both the strengths and the ecological perspectives (Germain & Gitterman, 1996:9-14; Saleebey, 2002:13-18).
Inner strength, as utilised by most (68.9%) participants, varied from having a fighting spirit ("...you have to fight back"), a willingness to adapt to changed circumstances, to the ability to come to terms with one's own limitations ("I realised that I will not be able to do the things I did before"). They also demonstrated a positive attitude of acceptance ("... to accept yourself the way you are now") and a deliberate decision to continue with life despite the operation ("Idecided ... I just have to continue with life"). These findings were in line with the principles of the strengths perspective as conceptualised by Saleebey (2002:13-18), namely to draw on one's inner strength, to see cancer as a challenge and an opportunity, to utilise the disease as an opportunity for growth and change, and to exhibit the ability to collaborate.
Although the role of social support was less important (15.6%), participants appreciated support from family, friends and people of the church while dealing with their physical changes. Environmental resources can also include a wider circle of relatives, friends and neighbours to provide the social support some may desperately need (Saleebey, 2002:17).
Coping with the end of active medical treatment
The majority of patients (71.1%) experienced a sense of gratitude that the medical treatment improved their physical condition ("I feel much better than before the operation") and that the hospital team supported them during the process. They were also thankful that they could re-enter their family cycle ("I was very thankful ... that I could go home and to be with my children'"), and could master post-operative speech ("...thankful that I could continue with my life"). Jefford, Karahalios, Pollard, Baravelli, Carey, Franklin, Aranda and Schofield (2008:30) and Hara and Blum (2009:40) found that families and friends will experience feelings of happiness upon completion of the patient's treatment as they can continue with their lives. Another reason for their gratitude was the financial benefit, as it implied that they did not have to spend money to travel to the hospital any longer (Hara & Blum, 2009:40). Patients may also experience a feeling of pride in managing to complete their prescribed medical treatment (Coughlin, 2008:61; Rowland, 2008:364).
Fear and uncertainty were reported by some (13.3%) patients, confirming findings by Haylock et al. (2007:62). Patients mainly experienced fear of social rejection, while the fear of recurrence of the cancer and uncertainty of leaving the safety and support of the hospital took second place:
"I was afraid to leave the hospital ... I turned back, I wanted to go back. I am afraid of being outside. I had an eternal fear for my acceptance ... because I did not have confidence in myself... while I was walking I thought, will my wife accept me the way I am?"
This fear and uncertainty are also mentioned in the literature (Jefford et al., 2008:21, 26), which notes that patients may experience anxiety about being separated from the healthcare system, while Rowland (2008:363-364) agrees that the transition from active treatment to recovery can be stressful.
A few (15.6%) patients experienced mixed feelings of happiness and sadness when they left the hospital system, which is in accordance with the findings of both Hoffman (1989:86) and Miller et al. (2008:372). In the current study, mixed feelings included feelings of thankfulness together with sadness ("A bit of sadness ... but also a bit of thankfulness ..."); shame ("...glad to be out of hospital, but actually I was ashamed of what the people will say") or feelings of discomfort ("I felt very satisfied ... a bit uncomfortable to be at home ").
The age of participants who experienced mixed feelings at the time of treatment completion was between 49 and 73 years, with five of them younger than 60 years. Survivors of the middle-age group might feel that they had more to lose than older survivors, since they might still be actively involved in multiple social roles (Cella, 1987:62; Hara & Blum, 2009:47).
Coping with post-operative readjustment
In coping with post-operative readjustment, patients indicated the most difficult adjustments they had to make, followed by their views on their family's most difficult adjustment. Family members themselves also commented on how they coped with the post-operative readjustment of the patient.
Patients' responses were in line with literature reviews (McQuellon & Hurt, 1997:233-234, referring to Pruyn et al. (1986)) on psychological aspects following head and neck cancer, and which reported that problems pertaining to speech, embarrassment about physical appearance and indications of psychological problems were the most difficult to adapt to.
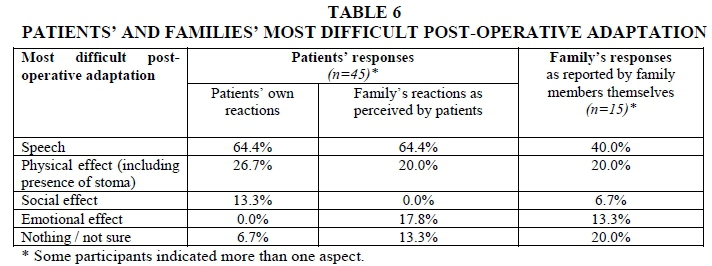
More than two thirds (64.4%) of patients and almost half (40.0%) of families reported that patients' speech was the most difficult to adapt to following surgery (Table 6). This finding is supported in the literature (Graham, 2004:127), stating that loss of speech and altered speech method is considered to be the most traumatic and challenging consequence of a laryngectomy. When participants (patients) were asked about their family's most difficult post-operative adjustment, some two thirds (64.4%) of participants indicated that family members found it difficult to adapt to their new way of communication and speech, corresponding well with their own experience.
Patients found it difficult to get used to their loss of voice ("The worst was not being able to talk") and the new way of speech production and communication ("To learn to talk was the most difficult"). Not being heard ("To express yourself in a situation where no one can hear you ") was another concern of patients, while they doubted the acceptance by others, as some people felt sorry for them or made fun of them ("...you never know how they are going to accept you"). Patients acknowledged that it must have been difficult for family members to get used to their loss of voice ("...as I cannot talk like before"); loss of self-expression ("I've lost my ability to laugh"), their new method of speech production ("... which process I have to go through so that I produce voice") and initial difficulty in understanding them.
Some (40.0%) family members found it difficult to adjust to the new technique of communication ("I learned not only to hear but to listen"), which in some cases even resulted in the patient's anger towards family members ("I could not understand him then he became angry"). This supports McQuellon and Hurt (1997:233-235), referring to Pruyn's study (1986), who found that patients felt frustrated for not being understood, not being able to make themselves heard in a noisy room and feeling inhibited about expressing themselves.
Coping with the hospital's expectations after treatment completion
As reflected in Table 7, the majority (75.6%) of the participants indicated that they knew exactly what to expect. A few (13.3%) participants indicated that they did not know exactly. A number (11.1%) of participants said that they did not know at all what was expected of them. More than half (60.0%) of family members, on the other hand, felt that they did not exactly know what was expected of them, whilst the other six (40.0%) felt that they knew fully what was expected of them.
-
Knew exactly
Those patients who fully knew what would be expected of them at home referred to their preparation in general ("I knew exactly as I received information on how to manage myself"), which they felt was helpful. Three quarters (75.6%) of patients were prepared on how to take care of the stoma and also what would be expected of them in terms of their new lifestyle ("I knew I had to give my full cooperation ... stop smoking ... alcohol and those things I have to leave"). They were motivated by their inner strength and a positive attitude and the need to be independent ("...not to be dependent on any person"). This links well with the strengths perspective conceptualised by Saleebey (2002:14), stating that every individual has certain strengths. They also found that religious faith helped them to feel prepared.
Family members felt prepared to care physically for the patient (stoma care; nasogastric tube feeding; general assistance at home; avoiding exposure to water), and to assist with their post-operative adaptation ("The doctors showed us very well how it will be, how he will adapt"). They emphasised the importance of this preparation even before the patient's discharge. Being able to visit the patient in hospital and to observe what was expected of them prepared them for their role as future caregiver.
-
Did not know exactly
Those who indicated that they did not know exactly what was expected from them in terms of aftercare did not ask for information or decided they would practise at home. These findings correspond with the literature (Cady, 2002:349) indicating that a shortened stay in hospital adds to patients' and families' pressure in performing post-operative self-care. One participant recommended the use of handouts and support groups in order to prepare patients for their aftercare.
-
Did not know at all
The few (11.1%) patients who indicated that they did not know at all what was expected from them when their treatment finished reported that they did not realise that the effect of the operation would be ongoing ("I thought that when the operation is over then everything is over"). They were ignorant as to what was expected from them in general and also in terms of their future employment. Cady (2002:349) emphasised that a shortened stay by patients in the safe environment of the hospital would result in increased pressure on patients to adjust to their laryngectomy experience in a relatively short time.
Family members also emphasised that there were both physical ("One night he coughed and then the valve came out... what do one do in such a case") and emotional effects ("I had to learn to deal with his different moods ") for which they were unprepared. These included the following: diet, stoma care, care of the Provox especially during an emergency, inability to scream or to sing (physical); mood swings, self-pity, self-centredness, anger (emotional). Taking into account the increased survivorship of cancer patients, informal caregivers could be expected to provide more complex care for a longer period of time, which may increase their levels of stress (Golant & Haskins, 2008:420). They often learned from experience (" We found out for ourselves what worked best for us") or learned from the patient himself how to provide care.
Psychosocial effects of laryngectomy and re-entry into society during the permanent phase
The final phase of survivorship as described by Miller et al. (2008:372) is the permanent phase. Participants were questioned about their experience of the psychosocial effects of the operation and their re-entry into society. Rowland (2008:364) mentioned that "being cancer-free does not mean being free of cancer", referring to the psychosocial and spiritual impact of the diagnosis of cancer.
Social effects and adjustment
A minority of patients acknowledged that the laryngectomy affected their social relationships negatively with regard to their employment and finances, as well as some friendships. A closer look at the social role fulfilment of participants will contribute towards a better understanding and interpretation of the findings of the study.
-
Social role fulfilment
Participants mostly referred to the physical effect of the operation ("I still do the same things which I did in the past") as opposed to their social role fulfilment. According to Cella (1987:62), the role of the survivor in the traditional nuclear family depends on the age of that survivor. Moreover, the psychosocial stages of development pose unique challenges and concerns for every survivor. The majority (60.0%) of patients who participated in the study were between 60 and 78 years of age, and were therefore representative of the elderly age group. Elderly survivors could be confronted with the inevitable loss of significant relationships. This may result in their turning to new peers or withdrawing from society at large for continued gratification. For the laryngectomy survivor, turning to new peers will be challenging as a result of the speech limitation.
Also of relevance are those representing the middle adulthood group, as some (40.0%) participants' ages varied between 42 and 59 years. According to Hara and Blum (2009:46), in this phase one fulfils multiple adult roles and responsibilities, particularly those involved in supporting a family. A cancer diagnosis at this time challenges one's ability to multitask effectively, which can undermine one's self-image as an adult in society.
-
Other family members
The majority of participants indicated that their relationship with other family members had improved. They felt that the support and acceptance of family members contributed positively to this improvement. The fact that more than one family member suffered from cancer also resulted in greater closeness between family members. Patients also commented that they contributed to this positive and improved relationship by letting go of previous social habits such as drinking and smoking ("They asked me to stop smoking but I did not stop ... now I've stopped. Now everyone likes me"). Cella (1987:62) referred to studies that suggested that close family ties can predict satisfactory adjustment to cancer, as the family usually "pulls together" to cope with the challenges.
-
Employment and financial situation
Patients experienced a decrease in their physical ability, which in some cases led to termination of employment. The number of pensioners increased from 26.7% to 80.0% after surgery. Surprisingly, some participants indicated that they learned to be more responsible (13.3%) with their finances, mainly owing to the fact that they stopped smoking and drinking.
-
Relationships with friends
There was no clear indication that the operation had a negative effect on relationships with friends. Some negative fall outs, however, occurred when friends continued with their bad social habits (15.6%) ("They all left me ... we do not travel the same road. In the past we drank a lot"); they had difficulty conversing ("Most of them stayed away because I could not talk") and friends felt sorry for them and mistakenly thought that speaking was uncomfortable ("They do not want me to talk a lot, they _feel sore on my behalf" ) for the patient. Some friends also found it difficult to adapt to the new way of communication (13.3%) or had the irrational fear that the patient might die unexpectedly whilst with them ("... they are afraid that I will die any moment"). Participants reported that after their speech ability improved, they were accepted again because it was difficult to see the patient in that condition. Some friends tend to exclude patients from social events ("They do not visit me, they cut me out").
Emotional experiences upon loss of natural voice
In an attempt to describe how patients experienced the loss of natural voice, more than half of the patients (57.8%) experienced this loss as negative. Participants reported an overwhelming feeling of loss ("...you feel strange, I _ felt bad, for me it was difficult...") since they felt they were not heard ("It seems as if no one heard me when I talked"). People who teased them about their strange voice also affected them negatively ("...at times my voice sounded bass and then you got those who teased you...").
Some patients (40.0%) did not find the loss of voice as problematic, because they found new ways of compensating for their loss. Time as a healing factor ("...with time you accept it") links with the study by De Boer et al. (1995:503; 512-513), who observed that the greater the time that elapsed after treatment, the fewer the psychosocial problems patients experienced. Patients learned to focus on positive aspects such as their health and their gratitude for still having a voice. This finding is in line with the principles of the strengths perspective (Saleebey, 2002:14).
When the same question was presented to family members, they were mainly thankful (66.7%) for their relative's health, despite the loss of natural voice ("To me it was he had a voice. It did not matter to me how it sounded and how it came out"). Those for whom it initially was a negative experience (20.0%) also found that it changed to a positive experience. A few (13.3%) did not identify any problems in this regard.
Adjustment to society
The following categories of views were gained from patients and families on how they experienced their adjustment to society after medical treatment.
-
Easy
More than half (57.8%) of the patients indicated that they experienced their adjustment to society as easy. Aspects which helped them in their adjustment were successful mastery of speech ("It was very easy when I started to talk"); acceptance by others; support ("... my family was there for me"); their own attitude ("It was easy as it felt to me after the operation that I am still the same as I was before the operation") and their inner strength ("I will not that it let me down"). The finding correlates with a combination of the strengths and ecological perspectives, referring to external factors (speech; behaviour and support of other people) and internal factors (personal attitude; inner strength). When the same question was presented to family members, almost half of them (40.0%) indicated that it was not difficult for them as they continued with their lives as usual.
-
Difficult
Seventeen patients (37.8%) acknowledged that their post-operative adjustment was difficult. The two main areas of difficulty were their altered manner of communication ("Ifelt lonely because I could not communicate ") and dealing with other people's behaviour ('Some of them made a joke of me, others felt sorry for me ").
-
Not sure
Two patients (4.4%) were uncertain of how they viewed their adjustment to society following treatment.
Factors that made re-entry into society easier
Patients identified the factors that had helped to ease their re-entry into society.
-
Inner resources
Patients found that the role of self-acceptance ("Because I accepted myself who I am"); inner strength; appreciation of life and religious faith made their re-entry into society easier. These participants actively decided to continue with their lives. Family members also mobilised their inner resources in order to help them with their re-entry into society (" "I took it day by day"). In line with the strengths perspective, Saleebey (2002:14) stressed that, although disease may cause disruption, people have assets, resources, wisdom and knowledge that professionals sometimes are not aware of, which they utilise in order to master traumatic events such as cancer ("Idecided..."; "you have to tell yourself...; "my own will and positive thinking ").
-
External resources
With reference to external resources that eased their re-entry into society, participants first of all referred to the role of support from various sources. Other external resources which contributed to their easier adaptation were acquiring speech, the role of pre- and primary school children and grandchildren in their survivorship, as well as the role of recreational activities.
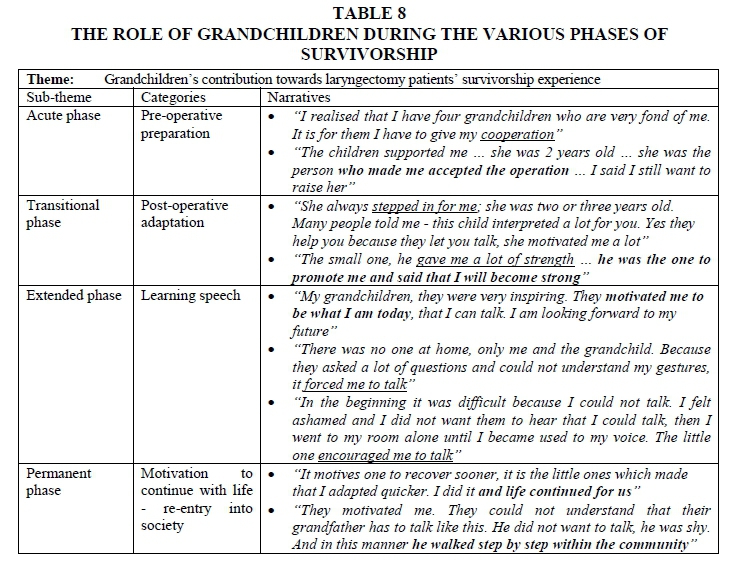
The role of pre- and primary school children and grandchildren in the rehabilitation of these patients was an unexpected and interesting finding which has not been reported in literature before. The age of these grandchildren ranged between a few months and three years of age.
Grandchildren's contribution during the phases of survivorship was acknowledged by participants and their narratives were divided into sub-themes and categories, presented in Table 8.
The valuable contribution that children and grandchildren made to assist patients throughout the various phases of their survivorship journey was illustrated by their narratives. This ties in well with the characteristics of the ecological perspective, referring to the interaction between the various systems within which one functions (Germain & Gitterman, 1996:5-6). This clearly illustrates Cella's (1987:62) observation that the family "pulls together" to cope with the challenges resulting from cancer.
Lessons learned during the survivorship journey
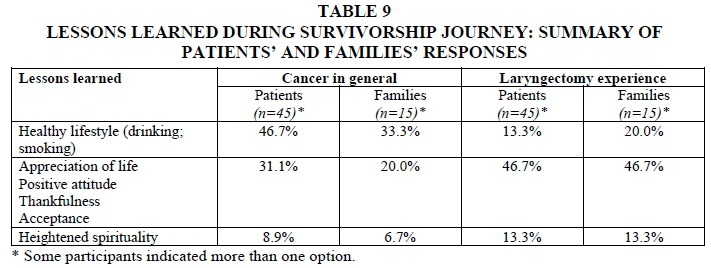
As stated in the literature (Surbone, Baider, Weitzman, Brames, Rittenberg & Johnson, 2010:257), the experience of survivorship is different for each cancer patient and is related to individual and societal variables. Lessons that were identified by patients and family members are presented in Table 9.
In general, patients (46.7%) mainly learnt to maintain a sober lifestyle by quitting previous social habits with regard to smoking and drinking as they realised that this contributed to their disease. From the laryngectomy experience they (46.7%) mainly learned to appreciate life and to maintain a positive attitude, which included thankfulness and acceptance of circumstances that cannot be changed. Family members, on the other hand, also learned from the patient's cancer experience about the importance of maintaining a healthy lifestyle (33.3%) and that cancer can be cured. The laryngectomy experience taught them to have a positive attitude and to appreciate life (46.7%). This behaviour is in line with the principles of the strengths perspective referring to inner strength as a source of coping when having to adapt to a challenge (Saleebey, 2002:14).
DISCUSSION AND RECOMMENDATIONS
The goal of this study was to gain an understanding of the survivorship experience of post-operative laryngectomy patients and their families, starting from the moment of diagnosis onward. Findings of the study will be discussed according to the various phases of their survivorship journey.
-
During the acute phase, both patients and families experienced a need for information pre-operatively, although levels on which they required information differed to some extent. The majority of participants found the information they received prior to surgery to be adequate and helpful in their emotional, physical and social preparation for the operation, as well as for their post-operative adjustment. Emotional reactions to the received information as perceived by patients to a large extent correlated with their family's reactions and this was also confirmed by family members themselves. These emotional reactions mostly involved sadness, shock and acceptance.
-
In the transitional phase, patients and families differed with regards to their experience of the most difficult physical post-operative adaptation. While most patients found it difficult to describe their emotional reactions to these changes or they experienced sadness, the families responded with acceptance and thankfulness. Post-operative speech was the most difficult adaptation for both patients and families. To a lesser extent, physical aspects such as the presence of the stoma and limited physical ability presented another area of difficulty in their adaptation. Psychosocial_effects of the operation were experienced by both patients and families and these mainly involved the challenge of having to deal with the reactions of others.
-
Patients mobilised a combination of inner strengths and social support in order to adapt to the inevitable physical changes while facing the challenges of the extended phase of their survivorship journey. Various sources of social support were valuable for these patients' post-operative adaptation to these changes.
-
In the permanent phase of their survivorship journey, most patients found their re-entrance into society easy. They mobilised both internal and external resources to assist them in this regard. The diagnosis of cancer can be perceived as a teachable moment, and patients and families learned from their cancer experience to maintain a healthy lifestyle. With regard to the laryngectomy experience, they learned to be thankful for inherent blessings.
-
Cancer patients as primary survivors, as well as their families (secondary survivors) and social workers working in the field of oncology, are challenged by various survivorship issues. Based on findings of the study the following recommendations can be made when dealing with the phases of survivorship.
- During the acute phase of cancer survivorship, social workers should play a significant role in providing information to patients and families. The social worker is in an ideal position to offer support to both patients and families in order to take care of their emotional reactions at the stage of diagnosis.
- The transitional phase of survivorship will expect social workers to find innovative ways to encourage communication with patients and families who may find it difficult to express their emotional reactions to the inevitable permanent physical changes following surgery. This will be increasingly necessary as survivorship increases life expectancy and hence patients and families would have to deal with the effects of the operation for a longer period of time.
- Social workers should have the knowledge and insight into the most difficult post-operative adjustment patients and families will have to face, to assist them throughout the transitional phase of their survivorship journey.
- By applying the principles of the strengths and ecological perspectives, social workers should guide laryngectomy patients and families to work through the extended phase of their survivorship journey.
- In the permanent survivorship phase, social workers should enhance the mobilisation of both inner strength and external resources to facilitate the patients' re-entry into society. The role of pre- and primary school children or grandchildren should be emphasised, as this was found to be helpful with patients' post-operative adjustment.
- Social workers should look into ways to promote the cancer patient's experience of cancer as a teachable opportunity in order to promote a healthier and sober lifestyle.
Further research should focus on initiation of survivorship programmes for health care professionals to guide survivors to full utilisation of their own strengths as well as available community resources.
REFERENCES
ALFANO, C.M. & ROWLAND, J.H. 2006. Recovery issues in cancer survivorship: a new challenge for supportive care. Cancer Journal, 12(5):432-443. [ Links ]
BABBIE, E. & MOUTON, J. 2001. The practice of social research. (South African edition). Cape Town: Oxford University Press Southern Africa. [ Links ]
BLANCHARD, S.L. 1982. Current practices in the counseling of the laryngectomy patient. Journal of Communication Disorders, 15(3):233-241. [ Links ]
CADY, J. 2002. Laryngectomy: beyond loss of voice - caring for the patient as a whole. Clinical Journal of Oncology Nursing, 6(6):347-351. [ Links ]
CASPER, J.K. & COLTON, R.H. 1998. Clinical manual for laryngectomy and head/neck cancer rehabilitation (2nd ed). San Diego: Singular Publishing Group. [ Links ]
CELLA, D.F. 1987. Cancer survival: Psychosocial and public issues. Cancer Investigation, 5(1):59-67. [ Links ]
CHEN, S.C., TSAI, M.C., LIU, C.L., YU, W.P., LIAO, C.T. & CHANG, J.T.C. 2009. Support needs of patients with oral cancer and burden to their family caregivers. Cancer Nursing, 32(6):473-481. [ Links ]
COUGHLIN, S.S. 2008. Surviving cancer or other serious illness: a review of individual and community resources. CA: A Cancer Journal for Clinicians, 58(1):60-64. [ Links ]
DE BOER, M.F., PRUYN, J.F.A., VAN DEN BORNE, B., KNEGT, P.P., RYCKMAN, R.M. & VERWOERD, C.D.A. 1995. Rehabilitation outcomes of long-term survivors treated for head and neck cancer. Head & Neck, 17(6):503-515. [ Links ]
DEIMLING, G.T., BOWMAN, K.F., STERNS, S., WAGNER, L.J. & KAHANA, B. 2006. Cancer-related health worries and psychological distress among older adult, long-term cancer survivors. Psycho-Oncology, 15(4):306-320. [ Links ]
DELPORT, C.S.L. & FOUCHÉ, C.B. 2011. Mixed methods research. In: DE VOS, A.S., STRYDOM, H., FOUCHÉ, C.B. & DELPORT C.S.L. (eds). Research at grass roots:For the social sciences and human service professions (4 th ed). Pretoria: Van Schaik Publishers: 433-448. [ Links ]
DESHMANE, V.H., PARIKH, H.K., PINNI, S., PARIKH, D.M. & RAO, R.S. 1995. Laryngectomy: A quality of life assessment. Indian Journal of Cancer, 32(3):121-130. [ Links ]
DE VOS, A.S., STRYDOM, H., FOUCHÉ, C.B. & DELPORT, C.S.L. (eds). 2011. Research at grass roots: For the social sciences and human service professions (4th ed). Pretoria: Van Schaik Publishers. [ Links ]
DHOOPER, S.S. 1985. Social work with laryngectomees. Health & Social Work, 10(3):217-227. [ Links ]
EADIE, T.L. & DOYLE, P.C. 2005. Quality of life in male tracheoesophageal (TE) speakers. Journal of Rehabilitation Research and Development, 42(1):115-124. [ Links ]
FEUERSTEIN, M. 2007. Defining cancer survivorship. Journal of Cancer Survivorship, 1(1):5-7, 292. [ Links ]
FOSTER, C., WRIGHT, D., HILL, H., HOPKINSON, J. & ROFFE, L. 2009. Psychosocial implications of living 5 years or more following a cancer diagnosis: a systematic review of the research evidence. European Journal of Cancer Care, 18(3):223-247. [ Links ]
FOUCHÉ, C.B. & BARTLEY, A. 2011. Quantitative data analysis and interpretation. In: DE VOS, A.S., STRYDOM, H., FOUCHÉ C.B. & DELPORT C.S.L. (eds). Research at grass roots: For the social sciences and human service professions (4th ed). Pretoria: Van Schaik Publishers: 248-276. [ Links ]
FOUCHÉ, C.B. & DELPORT, C.S.L. 2011. Introduction to the research process. In: DE VOS, A.S., STRYDOM, H., FOUCHÉ C.B. & DELPORT C.S.L. (eds). Research at grass roots: For the social sciences and human service professions (4th ed). Pretoria: Van Schaik Publishers: 61-78. [ Links ]
FOUCHÉ, C.B. & DE VOS, A.S. 2011. Formal formulations. In: DE VOS, A.S., STRYDOM, H., FOUCHÉ C.B. & DELPORT C.S.L. (eds). Research at grass roots: For the social sciences and human service professions (4th ed). Pretoria: Van Schaik Publishers: 89-100. [ Links ]
GARBERS, J.G. (ed). 1996. Effective research in the human sciences: Research management for researchers, supervisors and master's and doctoral candidates. Pretoria: Van Schaik Publishers. [ Links ]
GERMAIN, C.B. & GITTERMAN, A. 1996. The life model of social work practice: advances in theory & practice (2nd ed). New York: Columbia University Press. [ Links ]
GOLANT, M. & HASKINS, N.V. 2008. "Other cancer survivors": The impact on family and caregivers. The Cancer Journal, 14(6):420-424. [ Links ]
GRAHAM, M.S. 2004. Alaryngeal speech rehabilitation in a group setting. Topics in Language Disorders, 24(2):125-136. [ Links ]
GREEFF, M. 2011. Information collection: Interviewing. In: DE VOS, A.S., STRYDOM, H., FOUCHE C.B. & DELPORT C.S.L. (eds). Research at grass roots For the social sciences and human service professions (4th ed. Pretoria: Van Schaik Publishers: 341-375. [ Links ]
GRIFFIN-SOBEL, J.P. 2005. Surviving cancer and cancer treatment. Clinical Journal of Oncology Nursing, 9(5):509. [ Links ]
GRINNELL, R.M. Jr. 1993. Social work research and evaluation (4th ed). Itasca, Illinois: FE Peacock Publishers, Inc. [ Links ]
HARA, R. & BLUM, D. 2009. Social well-being and cancer survivorship. Oncology (Williston Park), 23(2 Suppl Nurse Ed):40-50. [ Links ]
HAYLOCK, P.J. 2006. The shifting paradigm of cancer care. American Journal of Nursing, 106(3):16-19. [ Links ]
HAYLOCK, P.J., MITCHELL, S.A., COX, T., TEMPLE, S.V. & CURTISS, C.P. 2007. The cancer survivor's prescription for living. American Journal of Nursing, 107(4):59-70. [ Links ]
HOFFMAN, B. 1989. Current issues of cancer survivorship. Oncology (Williston Park), 3(7):85-88. [ Links ]
JEFFORD, M., KARAHALIOS, E., POLLARD, A., BARAVELLI, C., CAREY, M., FRANKLIN, J., ARANDA, S. & SCHOFIELD, P. 2008. Survivorship issues following treatment completion - results from focus groups with Australian cancer survivors and health professionals. Journal of Cancer Survivorship, 2(1):20-32. [ Links ]
JOHNSON, J.T., CASPER, J. & LESSWING, N.J. 1979. Toward the total rehabilitation of the alaryngeal patient. The Laryngoscope, 89(7):1813-1819. [ Links ]
KAPLAN, M. 2008. Cancer survivorship: Meeting psychosocial needs. Clinical Journal of Oncology Nursing, 12(6):989-992. [ Links ]
KING, P.S., MARSHALL, R.C. & GUNDERSON, H.E. 1971. Management of the older laryngectomee. Geriatrics, 26(4):112-118. [ Links ]
LENNIE, T.A., CHRISTMAN, S.K. & JADACK, R.A. 2001. Educational needs and altered eating habits following a total laryngectomy. Oncology Nursing Forum, 28(4):667-674. [ Links ]
McQUELLON, R.P. & HURT, G.J. 1997. The psychosocial impact of the diagnosis and treatment of laryngeal cancer. Otolaryngologic Clinics of North America, 30(2):231-241. [ Links ]
MILLER, K., MERRY, B. & MILLER, J. 2008. Seasons of survivorship revisited. The Cancer Journal, 14(6):369-374. [ Links ]
QUIGLEY, K.M. 1989. The adult cancer survivor: psychosocial consequences of cure. Seminars in Oncology Nursing, 5(1):63-69. [ Links ]
RENNER, M.J. 1995. Counselling laryngectomees and families. Seminars in Speech and Language, 16(3):215-220. [ Links ]
ROM, S.A., MILLER, L. & PELUSO, J. 2009. Playing the game: Psychological factors in surviving cancer. International Journal of Emergency Mental Health, 11(1):25-35. [ Links ]
ROSS, E. 2000. Psychosocial issues in laryngectomy. The Social Work Practitioner-Researcher, 12(1):13-23. [ Links ]
ROWLAND, J.H. 2008. What are cancer survivors telling us? Cancer Journal (Sudbury, Mass), 14(6):361-368. [ Links ]
SALEEBEY, D. 2002. The strengths perspective in social work practice (3 ed). Boston: Allyn and Bacon. [ Links ]
STRYDOM, H. 2011. Ethical aspects of research in the social sciences and human service professions. In: DE VOS, A.S., STRYDOM, H., FOUCHÉ, C.B. & DELPORT C.S.L. (eds). Research at grass roots: For the social sciences and human service professions (4th ed). Pretoria: Van Schaik Publishers: 113-130. [ Links ]
STRYDOM, H. & DELPORT, C.S.L. 2011. Sampling and pilot study in qualitative research. In: DE VOS, A.S. (ED), STRYDOM, H., FOUCHÉ, C.B. & DELPORT, C.S.L. 2011. Research at grass roots: For the social sciences and human service professions (4th ed). Pretoria: Van Schaik Publishers: 390-396. [ Links ]
SURBONE, A., BAIDER, L., WEITZMAN, T.S., BRAMES, M.J., RITTENBERG, C.N. & JOHNSON, J. 2010. Psychosocial care of patients and their families is integral to supportive care in cancer: MASCC position statement. Supportive Care in Cancer, 18(2):255-263. [ Links ]
WOODARD, T.D., OPLATEK, A. & PETRUZZELLI, G.J. 2007. Life after total laryngectomy: a measure of long-term survival, function, and quality of life. Archives of Otolaryngology - Head & Neck Surgery, 133(6):526-532. [ Links ]
ZEINE, L. & LARSON, M. 1999. Pre- and post-operative counseling for laryngectomees and their spouses: An update. Journal of Communication Disorders, 32(1):51-71. [ Links ]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}