










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.54 n.2 Stellenbosch 2018
http://dx.doi.org/10.15270/52-2-633
ARTICLES
Substance abuse and the workplace: a situation analysis
Breggie Smook; Marie Ubbink; Elma Ryke; Herman Strydom
Subject group of Social Work, North West University, Potchefstroom Campus, Potchefstroom, South Africa
ABSTRACT
Substance abuse among the employed in South Africa has increased in recent years with major economic consequences for employers. Specialist outpatient treatment programmes are available to employers, yet few employees are inducted into these programmes. A situation analysis was conducted to explore possible reasons for this state of affairs. This article provides an overview of workplace-related limiting factors in combating substance abuse and also covers the resources needed to deal with the problem of substance abuse in the workplace. The authors suggest collaboration between employers and outpatient treatment centres as a viable solution.
INTRODUCTION
This article is informed by a research study focusing on substance abuse among employed people in South Africa, which has increased in recent years, and the use of specialist outpatient treatment programmes for employees who abuse substances. The need for collaboration and networking between employers and outpatient treatment centres was also explored.
As one of the authors is a counsellor at an outpatient treatment centre, she became increasingly aware of the major negative impact of substance abuse on South Africa and more specifically on the employment sector. Considering that employers and outpatient treatment centres are both concerned with the problem of substance abuse in the workplace, the need for collaboration between these role players in dealing with the problem seemed self-evident. Yet data provided by the South African Community Epidemiology Network of Drug Use (SACENDU, 2012a) reveal a lower referral rate from employers than some other sources of referral of people with substance abuse problems for treatment nationwide. Accordingly, a qualitative research study was conducted to find possible reasons for this phenomenon and to determine possible solutions to the problem. A situation analysis was implemented to assess the issues concerning substance abuse and the workplace, and to explore the resources and capacities to deal with the problem. The need for collaboration and networking between employers and outpatient treatment centres was also explored. This article describes the results that emerged. The article concludes with recommendations to develop a networking programme for employers and outpatient treatment centres to deal collaboratively with substance abuse in the workplace.
PROBLEM STATEMENT
The growth in economic opportunities in South Africa since 1994 has led to an increase in the economically active population, and the United Nations Office on Drugs and Crime (UNODC, 2012) states that the concomitant increase in disposable income is largely responsible for an increase in substance consumption. Drug trafficking in South Africa has also increased exponentially since 1994 (UNODC, 2012), as has the number of people seeking treatment for drug and alcohol problems (McCann, Harker Burnhams, Albertyn & Bhoola, 2011).
Statistics on the prevalence of substance abuse indicate that South Africa is one of the top ten narcotic and alcohol abuse centres of the world (Anon, 2009). Alcohol remains the most commonly abused substance in South Africa, followed by cannabis (South Africa, 2010; South Africa, 2013a; Eberlein, 2010; McCann et al., 2011; SACENDU, 2012a). An increase in substance abuse among the employed is also reported (Grobler, Wárnich, Carrell, Elbert & Hatfield, 2006; McCann et al., 2011). The economic impact of substance abuse on employers is enormous and amounts to millions of rand annually in South Africa. Substance abuse among employees results in increased absenteeism, decreased productivity, accidents in the workplace, work errors, criminal activities at work and an increase in medical expenses, all of which translate into extensive economic losses every year (Eberlein, 2010; Grobler et al., 2006:; International centre for alcohol policies (ICAP), 2013; Parry & Bennetts, 1998). An estimated 60% of accidents in the workplace are related to substance abuse; criminal activities and theft at work treble as a result of substance abuse; and undetected substance abuse costs employers 25% of their annual wage bill (Dalton, Hoyle & Watts, 2006; McCann et al., 2011; Segal, Gerdes & Steiner, 2007).
Furthermore, the negative consequences of the link between substance abuse and HIV and AIDS have consistently been pointed out (South Africa, 2013a; McCann et al., 2011; Rose & Zweben, 2002; UNODC, 2012; UNODC, 2013:ix; Van Dyk, 2005). Given that companies are already encountering increased labour costs due to 37% HIV-related absenteeism (Barnett & Whiteside, 2006), the link with substance abuse places additional pressure on the business sector.
However, there are low identification and referral rates of substance abuse problems in the workplace (McCann et al., 2011: SACENDU, 2012a; 2012b). According to UNODC (2013), approximately one in six persons who need treatment for drug use disorders actually receive the treatment, while in Africa, only one in 18 problem drug users access treatment services, predominantly for cannabis use.
The aim of the research study was firstly to assess the phenomenon of substance abuse in the workplace, including the extent of collaboration between employers and outpatient treatment centres to deal with the problem and then to determine possible solutions to the problem.
A qualitative exploratory and descriptive design was adopted to gain insight into the problem of substance abuse in the workplace and to describe the findings. The systematic grounded theory approach was used to generate theory based on the viewpoints of participants regarding the problem of substance abuse in the workplace.
These research methods were used to answer the researched question: Will a networking programme between employers and out-patient treatment centres provide an alternative to address substance abuse in the workplace?
RESEARCH METHODS
The study was conducted in the Limpopo and Mpumalanga provinces as these provinces are clustered into one region for research and statistical purposes (SACENDU, 2012a). The focus was on outpatient treatment, as statistics (SACENDU, 2012b) reveal that most substance abuse clients in South Africa receive outpatient treatment.
The systematic grounded theory approach of Strauss and Corbin (Babbie, 2010; Creswell, 2013; Fouché & Schurink, 2011; Monette, Sullivan & De Jong, 2011) was used to generate theory based on the viewpoints of participants regarding the problem of substance abuse in the workplace.
A qualitative exploratory and descriptive design (Babbie, 2010; Fouché & De Vos, 2011; Neuman, 2006) was adopted to gain insight into the problem of substance abuse in the workplace and to describe the findings. Participants were selected by means of theoretical sampling (Babbie, 2010; Creswell, 2013; Fouché & Schurink, 2011; Strydom & Delport, 2011).
The two main "populations" in the study were the employment sector and outpatient treatment centres in the demarcated area. Participants from the employment sector included the employers and employees. Businesses within the proximity of outpatient treatment centres were selected because of cost-effectiveness considerations. Small, medium and macro businesses as defined by the National Small Business Act 102 of 1996 (Falkena, Abedian, Von Blottnitz, Coovadia, Davel, Madungandaba, Masilela & Rees, 2011) were involved. Occupational groups engaging in high-risk and safety-sensitive occupations (South Africa, 2013a, McCann et al., 2011; Pelser, 2011), such as public transport, security institutions and construction industries, were selected because of the significant life-threatening danger of these occupations to employees in the workplace and/or to the public. Employees involved as clients either for outpatient treatment or in aftercare were included in the sample. Four SANCA centres were targeted as they are the only registered outpatient treatment centres that provide substance abuse outpatient treatment in both the provinces mentioned. The staff members from the four outpatient treatment centres participated in the study on the basis of their specialist knowledge and experience in the field of substance abuse and their service delivery to the employment sector.
Data were collected by means of semi-structured interviews (Babbie, 2010; Greeff, 2011; Welman, Kruger & Mitchell, 2010) with the 29 representatives from the employment sector, 7 employees and focus group interviews with the 26 staff members from three of the four outpatient treatment centres in Mpumalanga. One centre withdrew from participating. The SANCA Polokwane treatment centre from Limpopo province was involved in the group orientation discussions; however, the centre experienced dire financial difficulties at the time and was compelled to withdraw from the research study. SANCA Polokwane was therefore not involved in the data-collection phase. The data collection took place between January 2012 and June 2012.
Data were systematically analysed through open, axial and selective coding (Braun & Clarke, 2006; Creswell, 2013; Fouché & Schurink, 2011; Monette et al., 2011). During the open coding stage, the data from the audio recordings, field notes and transcripts from the interviews were examined and re-examined in ascertaining the major themes. The data collected from the interviews were first broken down into codes and sub-codes. The data from the employment sector and outpatient treatment centres were dealt with separately, each with themes and sub-themes. These sets were then consolidated to create the main themes and sub-themes. Although 29 individual interviews were conducted, data saturation (Creswell, 2013; Fouché & Schurink, 2011) was reached after the data of 20 participants were analysed, which obviated the need for inclusion of the remaining nine. An independent analyst (co-coder) verified the data analysis and data saturation. Findings were verified by means of a member checking meeting (Botma, Greeff, Mulaudzi & Wright, 2010; Creswell, 2005; Ellingson, 2009) with participants from both populations with the purpose of sharing information on the research findings and engaging the participants in feedback. Feedback from the member checking meeting was integrated into the research findings on the related themes. The aim of the member checking process was to enhance the credibility of the data analysis (Botma et al., 2010; Creswell, 2005; Ellingson, 2009).
The authors considered and implemented several factors and strategies to ensure trustworthiness (Botma et al., 2010; Ellingson, 2009):
-
Truth value, through the use of reflexivity and member checking;
-
Applicability, through dense description, data saturation and the use of different sampling groups;
-
Gathering multiple viewpoints was necessary to avoid biases which could arise from the initial interpretations (Babbie, 2010);
-
Consistency, through the use of a systematic step-by-step audit trail and the assistance of a co-coder;
-
Impartiality, through continued involvement of the site coordinators, regular sessions with supervisors and an independent co-coder for feedback and reflecting purposes;
-
Authenticity, through the use of verbatim transcriptions, direct quotations and reporting the true feelings and experiences as conveyed by the participants.
The authors obtained permission to conduct the research from the SANCA Mpumalanga Management Board and the Mpumalanga Employers' Organisation Management Board. Informed written consent from all participants after completion of the orientation phase was also obtained. Participants were assured of the ethical conduct regarding confidentiality, which was also stipulated in the written consent. Coordinators from the outpatient treatment centres were also orientated on confidentiality matters during their induction programme. The interviewing protocol and role of the participants were thoroughly discussed with all participants. The participants gave permission for the use of audio tape recordings during the individual and focus group interviews. The authors obtained institutional permission to conduct the research.
RESULTS
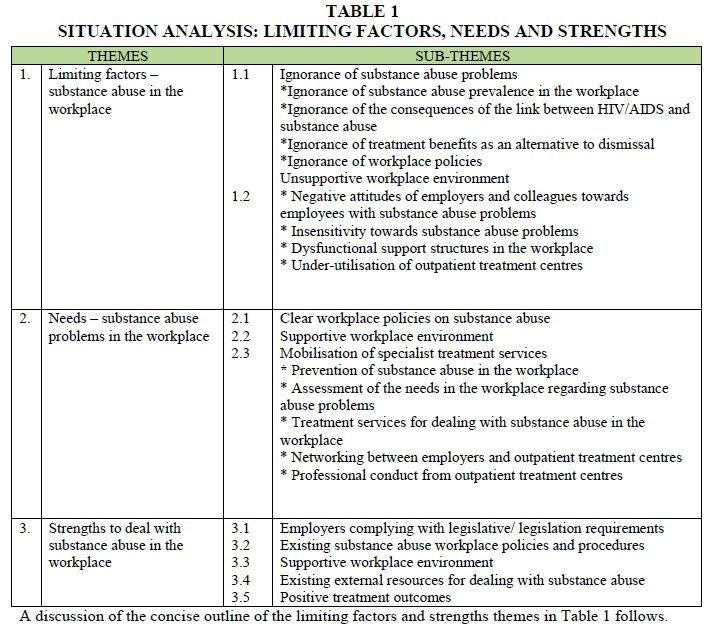
The data-analysis process produced three main themes: (i) limiting factors in addressing the problem of substance abuse in the workplace; (ii) needs identified in dealing with the problem; and (iii) strengths identified in support of the process of combating the problem in the workplace. We discuss each theme separately in relation to the identified sub-themes. We also indicate the relationship between the data that emerged from the empirical study and existing theoretical knowledge.
Table 1 is a concise representation of the situation analysis of the limiting factors and strengths.
Theme 1: Limiting factors - substance abuse in the workplace
The limiting factors to address substance abuse in the workplace are ignorance of substance abuse problems, ignorance of substance abuse prevalence in the workplace, ignorance of the consequences of the link between HIV/AIDS and substance abuse, ignorance of treatment benefits as an alternative to dismissal, ignorance of workplace policies.
Sub-theme 11: Ignorance of substance abuse problems
Ignorance of substance abuse prevalence in the workplace
Most of the participants reported that substance abuse problems existed in the workplace, that members of management seemed to consume the most alcohol and that some employers themselves experienced dependency problems. However, the extent of the problem was unknown and most of the employers were unaware of any needs regarding combating of substance abuse in their business. Only a few substance abuse cases were identified annually and referred for treatment. The employers expressed their views as follows: '"There is definitely a problem. I just don't know how big the problem is." "There are one or two substance abuse cases every year in the business." The viewpoint of a treatment centre on the reasons for the infrequent referrals was that "Employers don't refer. Employees don't come; they don't seek help from the employers. They are scared to tell the employers 'I'm having a problem with alcohol' because they are scared to lose their jobs. I guess it's a lack of knowledge, all around from the employee to the employer."
These findings are in line with the current literature on the discrepancy between the prevalence and referral rates of substance abuse cases. An estimated 5-35% of employees are dependent drinkers and approximately 7-20% probably have drug problems (Eberlein, 2010; Grobler et al., 2006; Hitzeroth & Kramer, 2010; McCann et al., 2011). A low identification rate of employees with substance abuse problems has been identified though (McCann et al., 2011). For instance, the South African Chamber of Mines revealed an estimated identification rate of 1% of substance abuse, which occurs mainly at hospitals where their employees have been referred for reasons other than problems related to substance abuse. Also, according to UNODC (2013), a limited number of people who need treatment for dependency actually receive it.
Ignorance of the consequences of the link between HIV and AIDS and substance abuse
Although many companies implement HIV-awareness programmes, most of the employers in the study were by and large unaware of the negative consequences of the link between substance abuse and HIV and AIDS. The following statement from an employee reflects the limited focus on substance abuse: "Very little is done to promote substance abuse awareness in our company ... the company mainly focuses on HIV-awareness campaigns." Literature sources consistently highlight the negative consequences of ignoring the link between substance abuse and HIV and AIDS (South Africa, 2013a; McCann et al., 2011; Rose & Zweden, 2002; UNODC, 2012; UNODC, 2013:ix; Van Dyk, 2005).
Ignorance of treatment benefits as an alternative to dismissal
Some of the employers reported that legislative requirements to consider rehabilitation in the event of substance abuse behaviour place considerable additional pressure on them. Dealing with substance abuse problems was considered time consuming and not a priority by most of the employers: production and profits were regarded as the main priority. It was evident that there was limited awareness of the benefits of treatment and counselling as alternatives to dismissal. Some employers were also misinformed about the legislative requirements regarding substance abuse incidents in the workplace: "The law says ... fire them ... fire them if they are drinking." A comment from a treatment centre: "By retrenching the employee with substance abuse problems, or having vague reasons to get rid of him, that will not help. We can rather network ways of how you can keep the employee so that you don't need to constantly re-employ and train new employees." Some of the interpretations of the legislative requirements to manage substance abuse in the workplace are in conflict with the requirements of the Labour Relations Act 66 of 1995 (South Africa, 1995). This Act stipulates that the employer has to provide opportunities for counselling and rehabilitation for substance abusers before dismissal is considered. The South African Labour Guide (South Africa, 2011) states that alcoholism and drug dependency are considered kinds of incapacities and not misconduct and that dismissal for unsatisfactory performance as a result of incapacity should be considered only after appropriate counselling and rehabilitation steps for employees have been implemented.
Ignorance of workplace policies
Some of the employees stated that policies on substance abuse in the workplace were unclear, while others reported that there were no workplace policies at all in this regard. Some workplace policies are masking the problem such as a policy of zero tolerance. A comment from a treatment centre: "So the employee will rather be absent from work than going to work and get caught under the influence and be fired. They stay away on the pretext that they 're sick." Grobler et al. (2006) and McCann et al. (2011) reiterate the importance of clear policies and procedures for dealing with substance abuse and dependency in the workplace. Various policies have been introduced in South Africa to deal with substance abuse, especially with regard to alcohol problems and, to a lesser extent, to the problem of illicit substances; however, only few drug-related policies have been implemented effectively (South Africa, 2013a).
Sub-theme 1.2: Unsupportive workplace environment
Negative attitudes of employers and colleagues towards employees with substance abuse problems
Negative attitudes of employers and colleagues towards employees with substance abuse problems included resistance to the problem of substance abuse; lack of interest in the problem; nonchalance regarding a possible solution to the problem; and, most ironically, even condoning substance abuse itself. The stigma attached to substance dependence was identified as a problem resulting in colleagues covering for or protecting each other, and/or employees concealing their own substance abuse problems. Conversely, some of the participants mentioned reverse stigmatisation and social endorsement of drinking: "7ou are excluded if you do not drink." The following comments illustrate some of the negative attitudes. An employer said: "The workplace is not a Rehab Centre. I need to make money." An employee in treatment said: "Others take the opportunity they have, the information they have to laugh at you and degrade you."
The following study (McCann et al., 2011) exemplifies the indifference towards substance abuse in the workplace. An American study of 1 300 railroad workers revealed a collective awareness of alcohol problems among the employees, yet few workers were willing to report cases of alcohol abuse. Over a period of a year 36% of the employees had seen co-workers drunk on duty; 15% had experienced co-workers who were too drunk or had too severe a hangover to work; and 60% said they had worked harder to cover for drunken co-workers. Only 14% of the co-workers were willing to report alcohol abusing colleagues if they caused serious damage, and 7% of the co-workers said that they would not report a colleague at all, even if someone was killed as a result.
Insensitivity towards substance abuse problems
A lack of sensitivity regarding relapse risk situations was identified; for example, some employees involved in a rehabilitation programme were expected to manage work functions where alcohol was served and they were actually expected to serve the alcoholic drinks. The employee participants perceived this as a sign of either ignorance or insensitivity. Encouraging substance use was also identified as a problem, for example, providing free alcoholic drinks at work functions and annual events, and holding regular Friday after-work social functions where liquor was available. A lack of encouragement and acknowledgement of employees' successes in treatment was also reported, leading to feelings of discouragement and demotivation. Employees said: "They say 'He's going to fail in the programme. He's going to go back and drink again.' Some are still encouraging me to join them in their drinking activities. You have to fight this thing alone."
Dysfunctional support structures in the workplace
A lack of confidence was expressed in the ability of employers to deal with the problem of substance abuse in the workplace. Some wellness assistance programmes in the workplace were not experienced as functional or supportive of employees in treatment. Employee Assistance Programmes (EAPs) were acknowledged as support structures, yet they were not perceived as professional treatment resources. The significance of sound workplace substance abuse management programmes is highlighted in the National Drug Master Plan (NDMP) (South Africa, 2013a). The importance of awareness among employers and employees about the benefits of a drug-free workplace (superior customer service, higher employee morale, increased productivity, reduced staffing costs and reduction in employee theft) is emphasised. However, according to the NDMP, South Africa lags behind international standards to manage employee substance abuse as part of occupational health, safety and risk management programmes. An appeal is made in the NDMP (2013-2017) for partnerships between the government and the public sector to implement comprehensive, ethical and sound workplace substance abuse programmes (South Africa, 2013a). Few businesses in the study had EAPs, with the exception of some of the macro businesses. Substance abuse problems were dealt with mainly by the employers or staff member(s) responsible for human resource management. Some of these staff members were not considered capable of dealing with the problem in the workplace or to motivate employees to join treatment programmes when necessary. Unwillingness on the part of employees to acknowledge substance abuse problems or become involved in treatment programmes was also mentioned. Corporate time frames for treatment often did not correlate with actual and realistic treatment time frames. It was also mentioned that employers were not always prepared to acknowledge relapses. An employer said: "I want value for my money. So the employee needs to be rehabilitated as soon as possible and sometimes the rehabilitation process is continuing time after time and still the person has not been rehabilitated." A comment from an employee in treatment: "Unfortunately now, for now, there is no one really who has an understanding of what this programme entails. I normally keep to myself, because, you know, you don't trust them, except a very few."
Although EAPs are regarded as key in dealing with substance abuse and dependency in the workplace (Dalton, Hoyle & Watts, 2006; Grobler et al., 2006; McCann et al., 2011; Roman, 2002; Services SETA, 2003a) limiting factors in EAPs to identify employees with drinking problems have been pointed out. McCann et al. (2011) refer to possible reasons for this limitation, namely that most problem drinkers are not easily detected, reduced work performance often develops gradually and is not easily measurable, and the signs and symptoms of substance abuse problems are less visible among low-to-moderate drinkers than those of dependent drinkers. According to Roman (2002), successfully addressing the problem of substance abuse in the workplace requires training of EAP staff on the basics of substance abuse intervention. Grobler et al. (2006) maintain that training of EAP staff in the early identification of substance abuse problems, as well as in referrals for appropriate treatment at the earliest possible stage, will deliver better end results.
Under-utilisation of outpatient treatment centres
Most of the employers in the study were unaware of the external resources to address substance abuse problems in the workplace. The limited visibility of outpatient treatment centres, lack of feedback to employers on treatment progress, as well as the unsupportive workplace culture and negative attitudes were identified as possible reasons for the under-utilisation of specialist treatment resources.
Participants from the employment sector expressed the following views in respect of this sub-theme: "Our (employer's) knowledge of SANCA is extremely limited." Staff members from the treatment centres said: "The business people need our services, there's no doubt about that, for the sake of their productivity. But we haven't taken enough initiative. Our marketing strategies are not vigorous enough." Backer (2003) voices some serious concerns about any collaboration process. Much collaboration fails and there are are often inefficient mechanisms for bringing about change, especially if not properly planned and if sufficient resources are not available to ensure that interventions provide sustainable long-term outcomes. Some collaboration is entered into without first assessing whether collaboration is appropriate to address the problem. Participants may have unrealistic expectations regarding collaboration deliverables. Collaborations are often set up without proper attention to the establishment process and their sustainability requirements.
Theme 2: Needs to address substance abuse problems in the workplace
Most needs for combating substance abuse in the workplace were identified as limiting factors and related to workplace policies, the workplace environment in respect of substance abuse, and the mobilisation of specialist resources to assist employers in dealing with the problem.
Sub-theme 2.1: Clear workplace policies on substance abuse
A need was expressed for clear workplace policies and procedures on treatment issues such as payment of treatment fees, time off allowed from work for treatment sessions, support structures in the workplace to assist problem employees in the reintegration process, and constant monitoring and evaluation of the treatment progress. Participants considered benchmarking with different employers as an ideal opportunity to enhance workplace policies on substance abuse in the workplace. An employer's comments on benchmarking: "It will be interesting to benchmark with other companies on the empathy level - how far will your company support somebody with dependency problems? We need to share with each other best practices of how we are dealing with the problem. What about time off, or special leave, or maybe sick leave. In this way we can compare our own policies and procedures and maybe we are not so far behind, or maybe we need to change."
Sub-theme 2.2: Supportive workplace environment
An unsupportive workplace environment was earlier expressed as a major limiting factor. Questions were asked as to whether employers were truly concerned about the problem in the workplace. The employees expressed a strong need for a caring and sensitive environment for employees with substance abuse or dependency problems. A concerned workplace, a trustworthy and appropriately equipped management team to deal with the problem, consistent dissemination of information on the seriousness of the problem, and considering alternative solutions to the problem were regarded as evidence of a supportive workplace. A need was also expressed for encouragement of employees during the rehabilitation process, as well as for acknowledgement of successes. McCann et al. (2011) discuss the need to change the workplace environment if it in any way condones or encourages alcohol abuse and the recommend "treating the company" before attending to the problems of employees. "Treatment" of a company involves changing possible resistance to a substance abuse workplace policy; education of the entire workforce; assessment of the problem, as well as its causes; implementation of different solutions including disciplinary measures; and the involvement of external service providers such as social workers.
Sub-theme 2.3: Mobilisation of specialist treatment services Prevention of substance abuse in the workplace
This was identified as a key priority and this was reiterated at a member checking meeting. The key role of the employer was emphasised by a treatment centre: "I see the role of the employer as crucial in the patient's awakening that alcohol and drugs are bringing problems." Prevention is a priority measure to combat substance abuse with a significant shift from a supply-reduction approach to one of primary prevention in the new NDMP (South Africa, 2013a). Substance abuse prevention is described by McCann et al. (2011) as including activities aimed at preventing or delaying the onset of substance abuse problems with a subsequent increase in the treatment success rate. The workplace is the ideal environment to disseminate prevention messages on substance abuse (McCann et al., 2011). Raising awareness among employees of the impact of substance abuse on the workplace performance has been indicated as a successful measure to improve worker safety and increase productivity (Arkansas small business and technology development centre, 2011).
Assessment of the needs in the workplace regarding substance abuse
Assessment of needs on different levels was requested, that is, assessment of the extent of the problem of substance abuse in the workplace; employees' needs with regard to the problem and assessment of the capacities of employers to deal with the problem. The importance of individualised services to meet the needs of employers, as well as of employees was consistently mentioned. One employer reported: "You know, 90% of my workers are illiterate. You cannot just walk into the workplace and try to tell them about the negative consequences of substance abuse. You need to meet them in the field. You need to use visuals. They need to understand the message and how they could benefit. And they need to provide feedback on how they experienced your services."
Literature sources support the importance of assessment and emphasise that assessment is the key to effectively determine the nature of client needs in order to individualise services and provide essential information on resources and support systems (Andreasen & Kotler, 2008; Kirst-Ashman & Hull, 2009; Parker & Bradley, 2007; Segal, Gerdes & Steiner, 2007).
Treatment services for dealing with substance abuse in the workplace
A need for information and awareness on the nature of treatment was expressed. The importance of early identification and intervention before dependency has developed was emphasised. The identification of substance abuse trends in the workplace was considered very important to enable employers to respond proactively and refer problem cases quickly. Employers preferred an outcome-based method of treatment and positive treatment results: "We need a clear before and after picture." "Iwant to see a difference." The supportive role of outpatient treatment centres was expressed by an employer: "SANCA will be my refuge. I will know that there's a plan B, a friend for the employer to phone."
Literature sources substantiate the findings that services should include empowerment of the workforce by means of education programmes to better results. Grobler et al. (2006) argue that the treatment success depends heavily on early diagnosis and early intervention. McCann et al. (2011) discuss the importance of education of key role players, as well as the workforce, on substance abuse in general. Eberlein (2010) suggests that 95% of successful rehabilitation depends on proper aftercare and the involvement of significant role players such as employers. Hitzeroth and Kramer (2010) and McCann et al. (2011) reiterate the importance of regular contacts with treatment counsellors and regard aftercare as an essential component of substance abuse treatment. To maintain sobriety and prevent relapse, a recovery plan, a reintegration plan, life style changes including improvements in health, social and legal status, stable marital relationships and support groups are necessary (South Africa, 2013b; Eberlein, 2010; Fisher & Harrison, 2009; Hitzeroth & Kramer, 2010; Van Wormer & Davis, 2008).
Networking between employers and outpatient treatment centres
Participants from the employment sector emphasised the importance of networking, awareness raising and the increased visibility of outpatient treatment centres. A comment from an employer on networking: "I think our company's knowledge about SANCA is extremely limited. I'm looking forward to meet with them and find out what they can offer and what their capacities are." The need for a team approach was highlighted. One of the employers described the importance of teamwork in the networking programme: "We are working in a circle. The circle must be a circle. We must be on the same line, otherwise the line will break. The circle will not be a circle anymore."
Pierson and Thomas (2010) describe networking as "the process of linking together individuals, groups and/or communities with common interests in order to spread information, knowledge, resource sharing, and mutual support." The assumption is that networking would increase capacities to solve social problems, meet organisational or individual challenges and promote a general aim. Dalton, Hoyle and Watts, (2006) refer to networking as a process by which moral support is gained and important information is gathered in areas outside of one's own expertise through the development of external and internal contacts. The purpose of networking is described by Kirst-Ashman and Hull (2009) as attempts by social workers to "strengthen or develop linkages among people, groups, or other organizations" in order to connect clients to resources. Thus, networking is considered a means to connect the employees experiencing substance abuse problems to a treatment resource, which in return holds benefits for the employer. According to Kirst-Ashman and Hull (2009), Long, Tice and Morrison (2006) and Weyers (2011), the social work profession has always been concerned with interagency networks, partnerships, service coordination and bringing about change in order to connect people and achieve a common goal, which would not be possible by working alone.
Professional conduct from outpatient treatment centres
The employers stressed the importance of professional conduct from outpatient treatment centres, though without mentioning reciprocal commitments on their part. They expected the treatment centres to respect employers' time, deliver quality services, honour commitments, focus on service delivery, provide regular feedback on the progress of treatments and ensure sustainable relationships between themselves and employers. Considering the importance of team work mentioned earlier, reciprocal professional conduct, respect and honouring of commitments are essential to ensure successful networking. Participants from the treatment centres commented on professional conduct: "The employer must also be consistent for what they're expecting. If they say our workshop starts at 10:00 ... sometimes half past eleven there's still nobody. When they want our services, they must be there. It must go both ways ... from us and from our partners. It's a two-way street." With regards to professional conduct, social workers are directed by the Code of Ethics of the SACSSP regarding the ethos of the profession, professional conduct and quality service delivery (SACSSP, 2012). Registered treatment centres are equally bound by the Code of Ethics of the SACSSP to adhere to professional conduct and quality service delivery. Reference is consistently made in literature sources to the core values of service, dignity and respect for the worth of the individual, importance of human relationships, integrity and competence (Greenfield, 2001; Long et al., 2006; Poulin & Contributors, 2000).
Theme 3: Strengths to deal with substance abuse in the workplace
During the situation analysis various strengths to deal with the problem of substance abuse in the workplace were acknowledged, although by only a few of the participants. These strengths included compliance with legislative requirements for counselling and treatment of substance abusers, the existence of workplace policies and procedures to address substance abuse, supportive workplace environment to deal with substance abuse problems, external resources to support the process of combating the problem more effectively and the existence of positive treatment outcomes. Such strengths align with an approach that builds on the strengths and resources of clients (Poulin & Contributors, 2000; Van Wormer & Davis, 2008). These strengths, ironically, were also identified by most of the participants as limiting factors and needs.
Sub-theme 3.1: Employers complying with legislation legislative requirements
Testimonials of employees indicated that at least some employers considered treatment before dismissal. Certain employers were willing to support problem employees, especially those who had credible and longstanding work records and those who were willing to cooperate in the treatment process. A comment from an employee: "When management sees that you have a substance abuse problem, they speak to you about being referred for help. They assist you to get help like they did for me; it's like a second chance before they consider dismissal."
Several South African pieces of legislation, i.e. the Occupational Health and Safety Act (85 of 1993), the Compensation for Occupational Injuries and Diseases Act (130 of 1993), Labour Relations Act (66 of 1995) and the Employment Equity Act (55 of 1998), stipulate that employers are obligated to allow for treatment and rehabilitation of employees with substance abuse and dependency problems resulting in poor work performance before dismissal is considered. Carroll and Buchholtz (2006) support the treatment of employees with substance abuse problems and state that it is "better to help troubled employees than to discipline or discharge them."
Sub-theme 3.2: Existing substance abuse workplace policies and procedures
Some of the participants mentioned the existence of workplace protocols and policies for problem identification, referral procedures, measures to assist employees with substance abuse problems and monitoring of the treatment progress. A comment from an employee in treatment: "Our Employee Wellness officer is situated almost 400 km from my local workplace. My case was promptly dealt with in the system, but I preferred to approach the local outpatient treatment centre because of private and practical reasons. My employer respected my request. The procedures were clear." Literature sources provide guidelines on substance abuse workplace policies and the function of such policies are clearly indicated (Albertyn & Bhoola, 2011; Grobler et al., 2006; Services SETA, 2003b).
Sub-theme 3.3: Supportive workplace environment
Internal support structures such as EAPs and health and safety divisions to assist employees with substance abuse problems were regarded as strengths in the workplace as was collaboration between employers and employees on problem identification and solutions. The encouragement of employees to sign up for treatment, support for them during the rehabilitation process, prompt follow-up of problem cases by management, an open and non-judgemental attitude towards employees with substance abuse problems, and support from colleagues in the reintegration process after treatment were also identified as essential strengths. Some comments from employees: "My immediate supervisor was exceptionally supportive and I had an intensive and in-depth 'fact-finding discussion' with him. The strong support from some of my colleagues and managers was maybe because I'm employed for 17 years with this company. And I have a credible work track record"; "Strict monitoring by management from the onset is extremely valuable and helps me not to relapse."
Sub-theme 3.4: Existing external resources for dealing with substance abuse
Existing external resources for dealing with substance abuse such as Alcoholics Anonymous (AA), Narcotics Anonymous (NA) and SANCA were acknowledged as valuable support structures for employees with substance abuse problems. The outpatient treatment centres involved in the study reported that they provide holistic, structured and evidence-based treatment programmes. This was substantiated by participants from the employment sector that had relationships with outpatient treatment centres and who gave due credit for their cultivation of positive relationships with employers. The importance of specialist substance abuse treatment and the utilisation of in- and outpatient treatment are acknowledged in various literature sources (South Africa, 2013a; Goodman, 2007; Grobler et al., 2006; Roman, 2002).
Sub-theme 3.5: Positive treatment outcomes
The credibility of outpatient treatment centres was acknowledged in employees' testimonies of success stories. Some of the employee participants reported that the treatment services were valuable and the counsellors knowledgeable and experienced. An employee's comments: "SANCA changed so many aspects in my life - the end results, the success stories are all evidence of the advantages of the treatment programmes." Goodman (2007), Miller and Weisner (2002), Slaymaker and Owen (2006) and Stevens and Smith (2005) mention various treatment benefits for the employment sector, i.e. reduced crime rates, an increase in employee efficiency, fewer incidents of disciplinary action on the job, and an increase in retaining employees in treatment. Goodman (2007) refers to a major research study on drug treatment in Britain, namely the National Treatment Outcome Research Study, which also revealed significant treatment benefits such as a reduction in crime rates and reconvictions. Eberlein (2010), Hitzeroth and Kramer (2010) and McCann et al. (2011) state that chances of a relapse are reduced when there are strong support systems such as the workplace, and sustainable aftercare programmes, including continuous contacts with treatment counsellors, and when clients personally implement major lifestyle changes.
DISCUSSION
With the grounded theory approach the data were systematically analysed (Braun & Clarke, 2006; Creswell, 2013; Fouché & Schurink, 2011). Failure to address substance abuse in the workplace was identified as the central phenomenon (axial coding). Three themes relating to the central phenomenon were identified, namely limiting factors, needs, and strengths to deal with the problem. Causal conditions influencing the central phenomenon, approaches (strategies) in response to the phenomenon and also consequences as a result of the approaches were identified. In the final stage of selective coding the interrelationship between the themes was drawn.
Regarding the first theme - factors limiting the successful resolution of substance abuse problems in the workplace - it became evident that ignorance of the problem of substance abuse in the workplace, an unsupportive workplace environment and the under-utilisation of outpatient treatment centres were causal conditions contributing to the core phenomenon. The gap in service delivery was exacerbated by dysfunctional support structures and some personnel not having the necessary skills. Approaches in response to the gap included ignoring the problem in the workplace, over-protection of colleagues, stigmatisation of the employees with substance abuse problems, concealing the problem, utilising unfeasible measures to address the problem, and preference to dismiss as opposed to treatment.
Consequences resulting from the causal conditions and approaches were limited or late identification of substance abuse problems, infrequent referrals for treatment, an increase in relapse risks, production losses due to increase in absenteeism, substance abuse-related accidents, sick leave, medical expenses and theft. Under-utilisation of outpatient treatment centres was identified as a consequence of the causal conditions and approaches to deal with the problem. It was therefore clear that the causal conditions, approaches and consequences all served to sustain the gap in service delivery.
The second theme revealed a close relationship between the limiting factors and the needs to deal with substance abuse in the workplace, i.e. the need for clear substance abuse workplace policies, a need for a supportive workplace environment, a need for specialist treatment services such as awareness and training programmes and, lastly, a need for networking between the employment sector and outpatient treatment centres. Mitigating the losses felt by both the employer and employee, therefore, required a rework of approach.
The third theme revealed strengths and existing resources to deal with the problem. Some employees reported positive experiences and identified strengths in the workplace such as adherence to legislative requirements for treatment of employees with substance abuse problems, existing and functional workplace policies and procedures, a supportive workplace environment, utilisation of specialist treatment services and positive treatment outcomes. Specialists and credible programmes aimed at providing services to the employment sector were available. The ecological approach provided the framework for the authors to assess both the problems and the needs, and identify the strengths within the macro environment. The interrelation between substance abuse problems, the impact of the problem on the workplace and utilisation of resources was evident.
RECOMMENDATIONS
We recommend a collaborative approach between employers, management, employees and outpatient treatment centres to address substance abuse in the workplace, as this would maximise the success rate and positive outcomes of the programme. As a means of collaboratively addressing the problem in the workplace with employers and outpatient treatment centres we propose a formal networking programme. This networking should include a clear purpose statement and procedures for proper assessment, planning, implementation, monitoring and evaluation of the programme. We lastly recommended that such a networking programme be tested within both the employment sector and outpatient treatment centres to evaluate its efficacy.
CONCLUSIONS
Ignorance of the scope of substance abuse in the workplace, indifference towards substance abuse problems, the stigmatisation of substance dependency, concealing of the problem and insensitivity regarding high-risk situations that may cause relapses all result in numerous employees with substance abuse problems either not being detected or attended to. Although legislative requirements stipulate that employers have to provide opportunities for treatment for substance abusers before dismissal, employers either experience these requirements as unnecessary demands, or they are misinformed about the requirements. Limited knowledge regarding the benefits of treatment as an alternative to disciplinary action was revealed.
Furthermore, many companies implement HIV-awareness programmes, but the enormous negative consequences of the link between substance use and HIV and AIDS are not addressed. This indicates a lack in knowledge and foresight to combat the problem of substance abuse in the workplace to counter the huge economic losses for the employer. In order to attend to the problem of substance abuse in the workplace, "treating" the workplace environment first needs attention. Considering that treatment success depends heavily on early diagnosis and early intervention, employers can contribute towards achieving better treatment results if prevention messages on substance abuse and problem solutions are continuously disseminated to employees. Education of key role players in the workplace on early identification, early intervention and treatment as disciplinary measure, as well as relapse prevention programmes, are means to empower the workforce in combating substance abuse in the workplace.
The development of clear substance abuse workplace policies has been recommended by both employers and employees. However, workplace policies should be a support structure in the workplace and not mask problems of substance abuse, as mentioned earlier. Benchmarking between different employers to share best practices regarding workplace policies is a viable means not only to develop workplace polices but also to streamline existing policies.
The importance of a team approach between the employers and outpatient treatment centres to deal with the problem in the workplace was consistently highlighted. Such a team approach, though, requires professional conduct and collaboration from both the employer and the outpatient treatment centre. The ecosystems approach provided the framework to indicate the interrelation between the problems, needs, strengths and resources, and the gaps in service delivery. The ultimate goal of the research study is to enhance the wellbeing of the employment sector and improve the social functioning of the workplace through a collaborative process (Segal, Gerdes & Steiner,, 2007).
REFERENCES
ALBERTYN, C. & BHOOLA, U. 2011. Proposed substance abuse policy and procedural agreement. In: McCANN, M., HARKER BURNHAMS, N.H., ALBERTYN, C. & BHOOLA, U (eds), Alcohol, drugs and employment (2nd ed). Claremont: Juta, 292-324. [ Links ]
ANDREASEN, A.R. & KOTLER, P. 2008. Strategic marketing for non-profit organizations (7th ed). Upper Saddle River: Merrill Prentice Hall. [ Links ]
ANON. 2009. The naked truth - statistics (SA & Global). [Online] Available: http://www.tnt.org.za/index.php/ption=com_content&view=article&id=21&Itemid=51 [Accessed: 15/03/2011]. [ Links ]
ARKANSAS SMALL BUSINESS AND TECHNOLOGY DEVELOPMENT CENTRE. 2011. Arkansas drug free workplace: facts and figures about drugs and alcohol in the workplace. [Online] Available: http://asbtdc.ualr.edu/drugfree/facts.asp [Accessed: 24/02/2011]. [ Links ]
BABBIE, E. 2010. The practice of social research (12th ed). Belmont: Wadsworth Cengage Learning. [ Links ]
BACKER, T.E. 2003. Evaluating community collaborations. New York: Springer. [ Links ]
BARNETT, T. & WHITESIDE, A. 2006. Aids in the twenty-first century: Disease and globalization (2nd ed). New York: Palgrave Macmillan. [ Links ]
BOTMA, Y., GREEFF, M., MULAUDZI, F.M. & WRIGHT, S.C.D. 2010. Research in health sciences. Cape Town: Pearson Education South Africa. [ Links ]
BRAUN, V. & CLARKE, V. 2006. Using thematic analysis in Psychology. Qualitative Research in Psychology, 3:77-101. [Online] Available: www.QualResearchPsych.com [Accessed: 30/05/2012]. [ Links ]
CARROLL, A.B. & BUCHHOLTZ, A.K. 2006. Business & society: Ethics and stakeholders management (6th ed). Mason: Thomson South-Western. [ Links ]
CRESWELL, J.W. 2005. Educational research: Planning, conducting, and evaluating quantitative and qualitative research (2nd ed). Upper Saddle River: Merrill Prentice Hall. [ Links ]
CRESWELL, J.W. 2013. Qualitative inquiry & research design: Choosing among five approaches (3rd ed). London: Sage Publications. [ Links ]
DALTON, M., HOYLE, D.G. & WATTS, M.W. 2006. Human relations (3rd ed). Mason: Thomson South-Western. [ Links ]
EBERLEIN, R. 2010. Lifestyle changes to beat addiction. Randburg: Knowres. [ Links ]
ELLINGSON, L.L. 2009. Engaging crystallization in qualitative research: An introduction. London: Sage Publications. [ Links ]
FALKENA, H., ABEDIAN, I., VON BLOTTNITZ, M., COOVADIA, C., DAVEL, G., MADUNGANDABA, J., MASILELA, E. & REES, S. 2011. SMEs' access to finance in South Africa: A supply-side regulatory review. [Online] Available: www.treasury.gov.za/publications/other [Accessed: 21/06/2011]. [ Links ]
FISHER, G.L. & HARRISON, T.C. 2009. Substance abuse: information for school counsellors, social workers, therapists, and counsellors (4th ed). Boston: Pearson Education. [ Links ]
FOUCHÉ, C.B. & DE VOS, A.S. 2011. Formal formulations. In: DE VOS, A.S., STRYDOM, H., FOUCHÉ, C.B. & DELPORT, C.S.L (eds), Research at grass roots: For the social sciences and human service professions (4th ed). Pretoria: Van Schaik Publishers, 89-100. [ Links ]
FOUCHÉ, C.B. & SCHURINK, W. 2011. Qualitative research designs. In: DE VOS, A.S., STRYDOM, H., FOUCHÉ, C.B. & DELPORT, C.S.L (eds). Research at grass roots: For the social sciences and human service professions (4th ed). Pretoria: Van Schaik Publishers, 307-327. [ Links ]
GOODMAN, A. 2007. Social work with drug and substance misusers: transforming social work practice. Wiltshire: Learning Matters. [ Links ]
GREEFF, M. 2011. Information collection: interviewing. In: DE VOS, A.S., STRYDOM, H., FOUCHÉ, C.B. & DELPORT, C.S.L (eds), Research at grass roots: For the social sciences and human service professions (4th ed). Pretoria: Van Schaik Publishers, 341-375. [ Links ]
GREENFIELD, J.M. 2001. The non-profit handbook: fundraising (3rd ed). New York: John Wiley & Sons. [ Links ]
GROBLER, P., WÁRNICH, S., CARRELL, M.R., ELBERT, N.F. & HATFIELD, R.D. 2006. Human resource management in South Africa (3rd ed). London: Thomson Learning. [ Links ]
HITZEROTH, V. & KRAMER, L. 2010. The end of addiction: A comprehensive South African guide. Cape Town: Human & Rousseau. [ Links ]
INTERNATIONAL CENTRE FOR ALCOHOL POLICIES (ICAP). 2013. Alcohol and the workplace. The ICAP Blue book: Practical guides for alcohol policy and prevention approaches. Module 22. [Online] Available: http://www.icap.org [Accessed: 10/01/2013]. [ Links ]
KIRST-ASHMAN, K.K. & HULL, G.H. 2009. Generalist practice with organisations and communities (4th ed). Belmont: Brooks/Cole. [ Links ]
LONG, D.D., TICE, C.J. & MORRISON, J.D. 2006. Macro social work practice: A strengths perspective. Belmont: Thomson Brooks/Cole. [ Links ]
McCANN, M., HARKER BURNHAMS, N.H., ALBERTYN, C. & BHOOLA, U. (eds). 2011. Alcohol, drugs and employment (2nd ed). Claremont: Juta. [ Links ]
MILLER, W.R. & WEISNER, C.M. 2002. Changing substance abuse through health and social systems. New York: Kluwer Academic/Plenum. [ Links ]
MONETTE, D.R., SULLIVAN, T.J. & DeJONG, C.R. 2011. Applied social research: A tool for the human services (8th ed). Belmont: Thomson Brooks/Cole. [ Links ]
NEUMAN, W.L. 2006. Social research methods: qualitative and quantitative approaches (6th ed). Boston: Pearson Education. [ Links ]
PARKER, J. & BRADLEY, G. 2007. Social work practice: Assessment, planning, intervention and review (2nd ed). Glasgow: Bell & Bain. [ Links ]
PARRY, C.D.H. & BENNETTS, A.L. 1998. Alcohol policy and public health in South Africa. Cape Town: Oxford University Press. [ Links ]
PELSER, I. 2011. ETTEx Network: the future of drug testing (e-mail). 11 February 2011. [ Links ]
PIERSON, J. & THOMAS, M. 2010. Dictionary of Social Work. Berkshire: Open University Press. [ Links ]
POULIN, J. & CONTRIBUTORS. 2000. Collaborative social work: strengths-based generalist practice. Belmont: Thomson Brooks/Cole. [ Links ]
ROMAN, P.M. 2002. Missing work: The decline in infrastructure and support for workplace alcohol intervention in the United States, with implications for developments in other nations. In: MILLER, W.R. & WEISNER, C.M (eds). Changing substance abuse through health and social systems. New York: Kluwer Academic/Plenum. [ Links ]
ROSE, S.J. & ZWEBEN, A. 2002. Interrelationship of substance abuse and social problems. In: MILLER, W.R. & WEISNER, C.M (eds), Changing substance abuse through health and social systems. New York: Kluwer Academic/Plenum, 145-156. [ Links ]
South African Community Epidemiology Network of Drug Use (SACENDU). 2012a. Monitoring alcohol and drug abuse trends in South Africa (July 1996-June 2012). SACENDU research brief, 15(2). Tygerberg. [ Links ]
SACENDU (South African Community Epidemiology Network on Drug Use). 2012b. SACENDU report back meetings November 2012. Monitoring alcohol and drug trends: January-June 2012. Tygerberg. [ Links ]
SEGAL, E.A., GERDES, K.E. & STEINER, S. 2007. An introduction to the profession of social work: Becoming a change agent (2nd ed). Belmont: Thomson Brooks/Cole. [ Links ]
SERVICES SETA. 2003a. Toolkit: Employee assistance programmes and the law in South Africa. Parktown: s.n. [ Links ]
SERVICES SETA. 2003b. Toolkit: Managing substance abuse in the workplace. Parktown: s.n. [ Links ]
SLAYMAKER, V.J. & OWEN, P.L. 2006. Employed men and women substance abusers: job troubles and treatment outcomes. Journal of Substance Abuse Treatment, 31:347-354. [ Links ]
SOUTH AFRICA. 1993. Occupational Health and Safety Act 85 of 1993. [ Links ]
SOUTH AFRICA. 1993. The Compensation for Occupational Injuries and Diseases Act 130 of 1993. [ Links ]
SOUTH AFRICA. 1995. The Labour Relations Act 66 of 1995. [ Links ]
SOUTH AFRICA. 1998. The Employment Equity Act 55 of 1998. [ Links ]
SOUTH AFRICA. 2011. The South African Labour Guide. [Online] Available: http://www.labourguide.co.za/workplacediscipline/code-of-good-practicedismissal-general-461 [Accessed: 24/02/2011]. [ Links ]
SOUTH AFRICA. Department of Social Development. 2010. Central Drug Authority Annual Report 2010/11. Pretoria. [ Links ]
SOUTH AFRICA. Department of Social Development. 2013 a. National Drug Master Plan (NDMP) 2013-2017. Pretoria. [ Links ]
SOUTH AFRICA. Department of Social Development. 2013b. Reintegration and aftercare model for substance abuse services. Pretoria. [ Links ]
SOUTH AFRICAN COUNCIL for SOCIAL SERVICE PROFESSIONS (SACSSP). 2012. Policy guidelines for course of conduct, code of ethics and the rules for social workers (4th ed). Pretoria. [ Links ]
STEVENS, P. & SMITH, R.L. 2005. Substance abuse counselling: theory and practice (3rd ed). Upper Saddle River: Merrill Prentice Hall. [ Links ]
STRYDOM, H. & DELPORT, C.S.L. 2011. Sampling and pilot study in qualitative research. In: DE VOS, A.S., STRYDOM, H., FOUCHÉ, C.B. & DELPORT, C.S.L. (eds), Research at grass roots: For the social sciences and human service professions (4th ed). Pretoria: Van Schaik Publishers, 390396. [ Links ]
United Nations Office on Drugs and Crime (UNODC). 2012. World drug report. Vienna: United Nations Publication, Sales No. E. 12.XI. 1. [Online] Available: http://www.unodc.org/documents/data-and-analysis/WDR2012/WDR 2012. [Online] Available: web small.pdf [Accessed: 12/01/2013]. [ Links ]
United Nations Office on Drugs and Crime (UNODC). 2013. World drug report. Vienna: United Nations Publication, Sales No. E.13.XI.6. [Online] Available: http://www.unodc.org/secured/wdr/wdr2013 World_Drug_Report_2013.pdf [Accessed: 08/03/2013]. [ Links ]
VAN DYK, A. 2005. HIV/AIDS care & counselling: a multidisciplinary approach (3rd ed). Cape Town: Pearson Education. [ Links ]
VAN WORMER, K. & DAVIS, D.R. 2008. Addiction treatment: a strengths perspective. (2nd ed). Belmont: Brooks/Cole, Cengage Learning. [ Links ]
WEYERS, M.L. 2011. The theory and practice of community work: a Southern African perspective (2nd ed). Potchefstroom: Keurkopie. [ Links ]
WELMAN, C., KRUGER, F. & MITCHELL, B. 2010. Research methodology (3rd ed). Cape Town: Oxford University Press. [ Links ]


{kind=link}