










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSocial Work
versão On-line ISSN 2312-7198
versão impressa ISSN 0037-8054
Social work (Stellenbosch. Online) vol.53 no.4 Stellenbosch 2017
http://dx.doi.org/10.15270/52-2-596
ARTICLES
Conceptualising a proposed support strategy for sexually abused boys in middle childhood
Dr Helga SteynI; Dr Carlien van WykII; Prof Ansie KitchingIII
IPastoral counsellor, Centre for Child, Youth and Family Studies COMPRES, Faculty of Health Sciences
IICentre for Child, Youth and Family Studies COMPRES, Faculty of Health Sciences
IIIEducational Psychology School of Education Studies Faculty of Education Sciences North-West University, Potchefstroom, South Africa
ABSTRACT
Male child sexual abuse in middle childhood has serious effects with the increased risk of development of various mental illnesses and disorders, as well as extreme forms of emotional and behavioural problems. This study conceptualises a proposed support strategy for sexually abused boys in their middle childhood placed in a clinic school. The proposed support strategy involves three main facets, namely the strengthening of the sexually abused boy as an individual; sustaining a deep, trusting relationship; and the facilitation of a sustainable supportive context for these boys.
INTRODUCTION
Research on male child sexual abuse (hereafter referred to as MCSA) has shown that the incidence of sexual victimisation of males is significant. In an international context it is estimated that roughly 14% of males are sexually abused during childhood (Schraufnagel, Davis, George & Norris, 2010). Alaggia and Mishna (2014) mention a prevalence as high as 26% of men in community samples and up to 36% of men in clinical samples. In the South African context Mathews, Abrahams and Jewkes (2013) mention a community-based survey done in 2013 in urban Gauteng province in South Africa which reported a prevalence of 20,4% of MCSA before the age of 18. The true extent of MCSA, however, remains unknown because of continued low rates of disclosure (Easton, Saltzman & Willis, 2014; Schraufnagel et al., 2010). Current research is still limited to studies that focus on adult participants relating their retrospective accounts of child sexual abuse (hereafter referred to as CSA) in their childhood years (Easton et al., 2014; Fergusson, McLeod & Horwood, 2013; Jackson, Newall & Backett-Milburn, 2013).
The focus of this study is on MCSA victims in their middle childhood. It seems that MCSA in this developmental phase has serious effects with extreme forms of emotional and behavioural problems (Diamanduros, Cosentino, Tysinger & Tysinger, 2012; Gospodarevskaya, 2013; Mathews et al., 2013). It seems there is limited support available to MCSA victims amidst all the challenges. No support strategies at an international or national level could be located that focus specifically on support for MCSA victims.
In Gauteng there are two clinic schools with residential facilities (Department of Education South Africa, 2001). At an international level clinic schools are referred to as "residential care" (Quisenberry & Foltz, 2013), "institutional youth care" (De Swart, Van den Broek, Stams, Asscher, Van der Laan, Holsbrink-Engels & Van der Helm 2012) or "alternative schools" (Simonsen, Britton & Young, 2010; Simonsen & Sugai, 2013). For the purpose of this research the term "clinic schools" was used. Clinic schools form part of schools for Learners with Special Educational Needs (Department of Education South Africa, 2001) and seek to educate learners requiring high-intensity support in terms of behavioural and emotional difficulties (Casey, Reid, Trout, Duppong Hurley, Chmelka & Thompson, 2010; De Swart et al., 2012; Simonsen & Sugai, 2013). The behaviour of learners referred to these clinic schools is mainly characterised by rebelliousness, hyperactivity, disobedience and aggression (Thomas, 2010). The objective of a clinic school is to be a short-term and interim substitute educational setting for these learners (Lee & Barth, 2011; Lehr, Soon Tan & Ysseldyke, 2009). Their problem behaviour needs to be addressed in order for them to be integrated into the mainstream educational setting (Flick, 2011) and to equip them to return to a less restrictive environment as soon as possible (Ennis, Jolivette, Swoszowski & Johnson, 2012; Simonsen et al., 2010). Clinic schools can accommodate learners until they turn 12 (RE,1 2012). These learners with emotional and behavioural problems have difficulty in becoming integrated into the mainstream educational setting again (Casey et al., 2010; Flick, 2011).
According to RE (2014), the principal of one of these schools, there are also sexually abused boys placed in clinic schools. He believes that MCSA may add to the trauma of these learners, which may result in even more emotional and behavioural difficulties. Several authors (Quisenberry & Foltz, 2013; Soenen, D'Oosterlinck & Broekaert, 2014) confirm that many children placed in clinic schools have experienced abuse. For the purpose of this study the focus is specifically on MCSA victims placed in a clinic school.
According to social support theory, abused children who are effectively supported show higher adjustment levels compared to those abused individuals with low levels of support (Cyr, McDuff & Hébert, 2013; Sperry & Widom, 2013; Van Toledo & Seymor, 2013). Social support can give an individual the feeling of being loved and cared for. The individual can function as part of an interpersonal network (Wilson & Scarpa, 2013). Social support can be seen as a protective factor among individuals at risk (Arias & Johnson, 2013; Sperry & Widom, 2013), such as MCSA victims (Schönbucher, Maier, Mohler-Kuo, Schnyder & Landolt, 2014). Yet no research at national or at international level about support strategies for MCSA victims placed in a clinic school could be located. In view of the above-stated findings it seemed imperative to conceptualise a proposed support strategy for these MCSA victims. According to personal communications with some staff members of a clinic school (MvW, 2013; SS, 2012), the people involved with the MCSA victims lack the knowledge to support these MCSA victims effectively without such a support strategy. This lack of support in the specific context of a clinic school necessitated the conceptualisation of such a proposed support strategy. The clinic school is unique in the sense that social workers, psychologists, counsellors, teachers, and child and youth care workers (hereafter referred to as role players) are involved with these sexually abused boys on a daily basis. It could be of great value if these role players could work together in a coordinated effort as a collaborative team to support these MCSA victims. Phasha (2008) mentions that in South Africa the average Grade 4 learner spends 1,400 hours at school a year, while learners in a residential facility spend 6,700 hours at school in a year. Therefore these role players could have a high impact on these learners, because of the close and constant interaction between them. These role players can function as a collaborative team and sustain a supportive context for these boys.
This lack of a proposed support strategy for MCSA victims results in a continuation of the problem behaviour and a delay in integrating them into the mainstream educational setting again. If MCSA victims can be successfully supported during their period at the clinic school, some of their emotional and behavioural difficulties may also be addressed, and this may subsequently lead to their integration into the mainstream educational setting.
The proposed support strategy was conceptualised from a strengths perspective (Jones-Smith, 2011; Saleebey, 2012). The strengths perspective focuses on the MCSA victims' resources, potentials, resiliencies and capacities to address the effects of MCSA. In this study it is important to use the strengths and resources of the MCSA victim, as well as understand the context in which these boys are functioning. The weaknesses of the MCSA boy, such as the emotional and behavioural impact of the MCSA, will also be taken into account. Seen from the strengths perspective all individuals possess the potential and strengths that can be marshalled to improve quality of life as it builds on the individual's resources, possibilities, resiliencies and capacities for change and transformation (Jones-Smith, 2011; Sabalauskas, Ortolani & McCall, 2014; Saleebey, 2012). The research aim was to conceptualise qualitatively, by means of a qualitative interpretive design, a possible support strategy for sexually abused boys in their middle childhood who are placed in a clinic school in Gauteng.
Considering the above points, the research question addressed in this article is: How do professionals including social workers, psychologists, counsellors, teachers, and child and youth care workers conceptualise a support strategy for victims of MCSA in a clinic school?
METHODOLOGY
The research project consisted of three phases. During the first phase the experiences of MCSA of boys placed in a clinic school were explored and described in order to understand their support needs (Steyn, Van Wyk & Kitching, 2014). For this purpose seven participants were identified through purposive sampling in the two clinic schools in Gauteng; three in-depth interviews were conducted with each of these participants. These in-depth interviews were conducted at the two clinic schools and the duration of each interview was about 20-30 minutes.
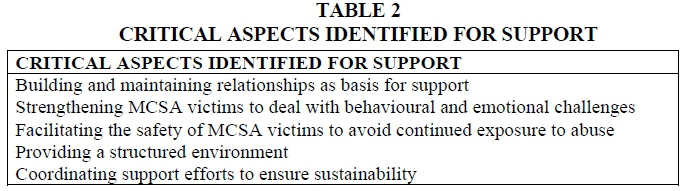
During the second phase the aim was to identify the critical aspects necessary to support sexually abused boys placed in a clinic school. Twenty-four participants were identified through purposive sampling; they included social workers, psychologists, counsellors, teachers, and child and youth care workers. Semi-structured individual interviews were conducted with each of these participants to identify the five critical aspects to support MCSA victims placed in a clinic school. These interviews lasted approximately 45-60 minutes each.
The aim of the third phase was to conceptualise a proposed support strategy for MCSA victims placed in a clinic school. A qualitative interpretive design (Schwartz-Shea & Yanow, 2012; St. George, 2010) was used, where two focus groups (Barbour, 2014; Flick, 2014; Wayne, 2013) were conducted with fourteen participants to assist with the conceptualising of a proposed support strategy for MCSA victims placed in a clinic school. The participants could give valuable insights based on their own practical experience. These focus groups lasted about 120 minutes each. The findings, as developed from the second phase of the study, were presented to these participants. Time was allowed to discuss the critical aspects in depth and how to transform these critical aspects into a support strategy. The participants reached consensus and the data were analysed.
All the findings obtained throughout the three phases were used to conceptualise a proposed support strategy. The conceptualising of a proposed support strategy for MCSA victims placed in a clinic school is described in this article.
Ethical considerations
The ethical aspects for Phases 1 and 2 were in place. The ethics committee of the North-West University, Potchefstroom Campus (Ethics number: NWU-00060-12-A1), Gauteng Department of Education and the two applicable district offices gave ethical approval for this study to be conducted. During Phase 3 it was ensured that no physical or emotional harm was done to the participants. This study was conducted with caution because of the sensitive nature of the issue of MCSA. Certain communication techniques were used (Greeff, 2011; Seidman, 2012) to facilitate the focus groups. Informed consent was obtained (Marzano, 2012; Reamer, 2013) from the participants. The procedures to be followed during the investigation were explained to all involved in this study in order to avoid any possible deception of the participants. All the participants were aware that participation was voluntary (Babbie, 2013) and anyone could withdraw from the study at any time. The participants were informed about the use of a digital recorder (Greeff, 2011) during the focus groups. The anonymity and confidentiality (Babbie, 2013; Reamer, 2013) of all participants were ensured. Identifying information was locked away in a file cabinet with restricted access and computerised data were protected by a password and encryption.
Data analysis
Thematic analysis was applied to analyse the data. The phases as recommended by Clarke and Braun (2013) were used to analyse the qualitative data. The researcher became familiar with all the raw data, transcribed all the data (Kowal & O'Connell, 2014) while reading through it (Bazeley, 2013) and assigned possible codes (Creswell, 2014; Flick, 2014; Harding, 2013) to the data. After this process possible themes were identified and the data that supported the codes were collated (Harding, 2013). The themes were reviewed, then defined and named (Bazeley, 2013). After this the information was written up to integrate the analytic narrative and the data extracts.
Trustworthiness
The criteria for excellent qualitative research were used to ensure trustworthiness during this study (Tracy, 2010). The criterion of a worthy topic (Tracy, 2010) was met, as the phenomenon of MCSA is very relevant and significant, because the occurrence of MCSA is a reality and research on MCSA is limited. Qualitative research needs to be conducted with rich rigor including sufficient data and time in the field (Barusch, Gringeri & George, 2011; Tracy, 2010). During Phase 3 data were obtained from two focus groups that included fourteen participants in total. This was a rich sample and data were collected rigorously until data saturation (Barusch Gringeri & George, 2011 Creswell, 2014) occurred. Peer reviews (Gringeri, Barusch & Cambron, 2013; Loh, 2013) were undertaken, where specific descriptions or themes were given to four participants to check for accuracy, comments and recommendations during follow-up interviews; this gave the participants the opportunity to comment on the findings and to assist with the interpretation of the data. Member checking (Creswell, 2014) was used, where possible themes were given to one participant to review. Credibility in based on dense description (Creswell, 2014; Tracy, 2010), concrete detail, triangulation or crystallisation (Creswell, 2014; Loh, 2013; Tracy, 2010) and member reflections (Creswell, 2014; Gringeri et al., 2013). A dense description (Creswell, 2014) of research methodology and a literature control were undertaken. The raw data and tentative interpretations of the data were discussed with four participants. The data were audited (Creswell, 2014; Gringeri et al., 2013) by a co-coder, while expert supervision was provided by a registered social worker and registered educational psychologist during the data-analysis process.
SUMMARY OF PHASES 1 AND 2
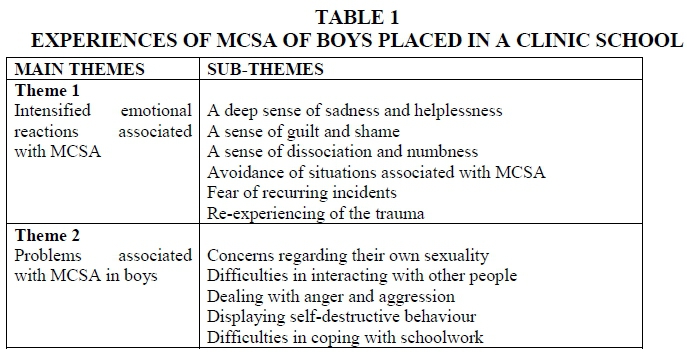
The following table provides a summary of the experiences of MCSA of boys placed in a clinic school that emerged from the in-depth interviews during Phase 1.
The following table shows the five critical aspects of support, identified during the second phase.
FINDINGS
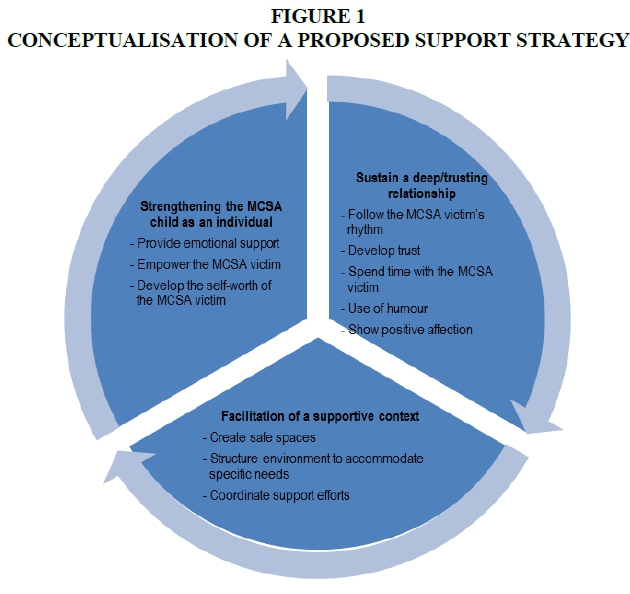
The proposed support strategy is based on the data retrieved from all three phases throughout this study and the literature overview. The proposed support strategy involves three main facets, namely strengthening the MCSA victim as an individual; sustaining a deep/trusting relationship with the MCSA victim; and facilitating a sustainable supportive context for these sexually abused boys.
The following figure provides a visual representation of the proposed support strategy.
The three main facets in the proposed support strategy (as illustrated in Figure 1) will be discussed. Relevant information from Phases 1 and 2 (as summarised in Tables 1 and 2) will be included in order to enrich the discussion.
Strengthening the MCSA victim as an individual
According to the strengths perspective, all individuals possess the potential and strengths that can be marshalled to improve quality of life and build on the individual's resources, possibilities, resiliencies and capacities for change and transformation (Gray, 2011; Jones-Smith, 2011; Saleebey, 2012). According to Eloff, Ebersöhn and Viljoen (2007), there needs to be greater knowledge about the assets, resources and capacities of vulnerable children. These authors are of the opinion that such information can assist in the construction of a more rounded, comprehensive and accurate understanding of these children and that such an understanding will enable interventions that will maximise wellbeing by taking the totality of each child's existence into account. This can in turn enhance resilience.
Resilience theory emphasises the phenomenon of maintaining wellbeing and coping well in the context of significant difficulty (Theron, Cameron, Didkowsky, Lau, Liebenberg & Ungar, 2011; Van Rensburg, Theron, Rothmann & Kitching, 2013). Several authors (Van Rensburg et al., 2013) have reported that South African youths draw on protective factors, such as the supportive resources of families, schools and communities, to adjust well to difficult life circumstances. According to Theron et al. (2011), individual traits and assets such as intelligence, temperament, a sense of humour and optimism can also serve as protective factors and can enhance resilience.
The MCSA victim as an individual experiences intensified emotional reactions (Jackson et al., 2013; Steyn et al., 2014) associated with MCSA, as well as problems associated with the MCSA (Steyn et al., 2014). It is therefore important that the conceptualising of a proposed support strategy for MCSA victims takes into account that this is an extremely vulnerable group of children. During the first phase of the study (Steyn et al., 2014) it became clear that MCSA victims experience a deep sense of sadness and helplessness (Alaggia & Mishna, 2014; Diamanduros et al., 2012; Gospodarevskaya, 2013), a sense of guilt and shame (Diamanduros et al., 2012; Dorahy & Clearwater, 2012), a sense of dissociation and numbness (Diamanduros et al., 2012; Dorahy & Clearwater, 2012), avoidance of situations associated with MCSA (Gospodarevskaya, 2013; Trask, Walsh & DiLillo, 2011), fear of recurring incidents (Alaggia & Mishna, 2014; Diamanduros et al., 2012) and of re-experiencing the trauma (Gospodarevskaya, 2013; Trask et al., 2011). The problems associated with the MCSA can range from concerns regarding the boy's own sexuality (Alaggia & Mishna, 2014; Parent & Bannon, 2012), difficulties in interacting with other people (Alaggia & Mishna, 2014; Kiselica & Novack, 2011:location 2810), dealing with anger and aggression (Gospodarevskaya, 2013; Parent & Bannon, 2012), displaying self-destructive behaviour (Alaggia & Millington, 2008; Parent & Bannon, 2012) to difficulties in coping with schoolwork (Frederick & Goddard, 2010; Parent & Bannon, 2012).
In light of the above discussion, different ways of strengthening the MCSA victim as an individual will be discussed next.
Provide emotional support
During Phase 2 participants mentioned the importance of the role players, who deal with this vulnerable group of boys, in providing emotional support to MCSA victims. This can be done by not triggering guilt feelings while working with these boys. There should also be a strategy in place to deal with these boys' anger and aggression.
In the second and third phase the importance of validating emotions and facilitating healthy expressions as a way to strengthen the MCSA victim as an individual was supported. Research literature (Alaggia & Mishna, 2014; Greene, Grasso & Ford, 2014) supports the use of validation of emotions. This can be done by means of an emotion chart on which the sexually abused boy can physically show on a chart how he is feeling at a particular moment. It is important first to focus on only four basic emotions: happy, angry, sad and scared. Otherwise the MCSA victim can feel overwhelmed by all the different emotions. Lierheimer and Stichter (2011), however, mention seven basic emotions to focus on: happy, sad, anger, fear, calm, disgust and surprise. Another way to allow the expression of emotions is by the role players validating and reflecting the boy's emotions, for example, "You look scared." According to Robinson (2011), this kind of validation of emotions helps the MCSA victim to gain insight into his own emotions and can assist him to accept his emotions. Participants mentioned that such an emotion chart should be used in the classroom, counselling room, residential facilities and at home. This will empower the MCSA victim to be able to express his emotions wherever he is at a particular moment. According to Kiselica and Englar-Carlson (2011:location 1930), the boy's emotional world can also be explored by using forms of artistic expression such as music, art or drama. Research literature (Cohen, Mannarino, Kliethermes & Murray, 2012; Reese, Horne, Bell & Wingfield, 2011:location 5173) supports the importance of allowing the sexually abused child to express his emotions in a non-threatening environment.
Empower the MCSA victim
It is also important to allow the MCSA victim as many choices as often as possible, as this will empower the boy to take back control of his life. Bastiaanssen, Delsing, Kroes, Engels and Veerman (2014) confirm these children need to develop the knowledge and skills to make their own decisions. Phasha (2008) mentions that sexually abused children can develop a sense of personal identity when role players pinpoint the child's strengths. It is important that all the role players are aware of and agree upon the strengths of a particular boy to enhance the empowering efforts based on the boy's strengths. Role players should exhibit high expectations of these boys. Reasonable goals could be set and the MCSA victim could be supported to make him confident about his own abilities. By fostering an environment that honours each boy's uniqueness, these MCSA victims are taught that they are valued, accepted and capable.
Another way to empower the MCSA victim is to make use of a safety plan. In the first and third phases the value of a safety plan for the MCSA victim as individual was mentioned. Such a safety plan can build the MCSA victim's personal safety skills, as well as helping him to access the available external resources (Barron & Topping, 2013; Cohen et al., 2012; Zeuthen & Hagelskjær, 2013). According to the data, a safety plan can reassure the sexually abused boy by teaching him to tell others when he feels afraid or to learn how to avoid potential abusers and dangerous situations (Kiselica & Novack, 2011:location 3043, 3090). This is particularly important for the MCSA victim who may never have experienced what it is to be safe from the sexual attention of others.
Develop the self-worth of the MCSA victim
During Phase 3 it became evident that a way to strengthen these MCSA victims is to develop sense of self-worth of the MCSA victim. The focus needs to be on the positive aspects of the boy's life and his strengths to counteract the stigmatisation of these boys. According to Sabalauskas et al. (2014), the strengths perspective enables the child to be inherently strong and resilient rather than feel flawed and in need of help. This can also build the self-worth of the MCSA victim as individual. CL (2013) added that negative self-concepts can be offset by positive experiences that the MCSA victims may experience in the relationship with the role players. Armstrong (2012) mentions the use of frequent specific and immediate praise to develop the self-worth of the child.
Sustain a deep/trusting relationship
Participants in all three phases of this study mentioned the importance of sustaining a deep/trusting relationship between the role players and the sexually abused boy. Research literature (Armstrong, 2012; Otten & Tuttle, 2011) confirms the importance of the relationship between the role player and the child. The role players will not be able to support the MCSA child effectively unless this relationship is deep (Handwerk, Huefner, Ringle, Howard, Soper, Almquist & Chmelka, 2008) and built on trust (Arias & Johnson, 2013; Cohen et al., 2012). The strengths perspective highlights that this relationship should be one where the role player believes in the boy as an individual (Jones-Smith, 2011; Sabalauskas et al., 2014). Ranahan (2013) concurs that there is no other form of intervention which is as immediate and grounded in the present as the relationship. This immediacy of the relationship allows the child to experiment with new ways of acting and experiencing as they are living their lives. Several authors (Sahay, 2013; Swanzen, 2011) mention the importance of giving love, care and support to the sexually abused child. Different ways of sustaining such a deep/trusting relationship will be discussed.
Follow the MCSA victim's rhythm
It seemed that this is a very sensitive relationship because of the intensified emotional reactions (Jackson et al., 2013; Steyn et al., 2014) associated with MCSA, as was evident in the first phase. During Phase 1 participants mentioned their anxiety about engaging with people (Steyn et al., 2014). This anxiousness is also evinced in the research literature (Alaggia & Mishna, 2014; Gospodarevskaya, 2013). The vulnerability of the MCSA victims was evident in the first phase of the study (Steyn et al., 2014). Because of this vulnerability, it is therefore important to move slowly and carefully in this relationship with the sexually abused boy (Gil, 2011; Kiselica & Englar-Carlson, 2011:location 1863). In the third phase participants outlined this as a deep/trusting relationship where the MCSA victim as an individual needs to set the pace in the relationship (Alaggia & Mishna, 2014; Kiselica & Novack, 2011:location 2954). A participant mentioned that this establishment of the relationship with the MCSA victim is like a dance with him, in which the role player allows the MCSA victim to set the pace and give directions. The role players need to have patience in this relationship (Kiselica & Novack, 2011:location 3021, 3023), as it will be critically important to accept that each MCSA victim might have his own pace. It will therefore take time to establish and maintain a relationship with the MCSA victim (Kiselica & Novack, 2011).
Develop trust
A specific focus in this process of strengthening the relationship should be on the development of trust. During the second and third phase the participants mentioned that this growing relationship should be based on trust. However, the participants in Phase 1 mentioned their difficulty in trusting other people (Steyn et al., 2014). The importance of confidentiality to counter this feeling of mistrust was outlined. According to several authors (Cohen et al., 2012; Robinson, 2011; Stuart, 2013), the relationship between the MCSA victim and the role players provides the child with the experience of trusting another, which he can then take into other relationships. This experience of trust creates a positive internal working model of himself and his abilities within relationships, which means that he can go on to anticipate positive experiences of future relationships.
Spend time with the MCSA victim
On a more concrete level the strengthening of the relationship needs to include practical activities that will add to the strengthening of the relationship. According to data from the second and third phase, it was evident that the role players need to spend time and do activities with the boy in order to build this deep and trusting relationship. This is also supported by research literature (Barton, Gonzalez & Tomlinson, 2011; Solar, 2011). In the second phase participants mentioned the necessity of consistent contact between the role players and the MCSA victim to build the relationship.
Use of humour
Humour can also be included in this relationship. Suk-ching Chong and Leung (2012) support the use of humour. Humour can be a means to draw the attention away from the MCSA and to focus on sustaining this deep/trusting relationship. According to Kiselica and Englar-Carlson (2011:location 1839), humour is a vehicle to achieve intimacy and to reduce tension.
Show positive affection
The role players need to show positive affection, without touching the MCSA victim. According to the data, this positive affection can include spending time together, talking with each other and using humour. Touching is often associated with MCSA and so can harm the relationship with the MCSA victim. This touching can trigger intensified emotional reactions from the sexually abused boy (Kiselica & Novack, 2011:location 3025). Armstrong (2012) mentions that personally greeting the child can establish a positive rapport.
Facilitation of a supportive context for the MCSA victim
MCSA victims are very vulnerable, as already indicated. To ensure that these boys experience safety and care, a proposed support strategy should involve the facilitation of a supportive context for them (Ristuccia, 2013). According to social support theory (House, 1981), sexually abused children with adequate support adjust more easily after the abuse experience than those with low levels of support (Arias & Johnson, 2013; Cyr et al., 2013; Mathews et al., 2013). Several authors (Mathews et al., 2013; Sperry & Widom, 2013; Van Toledo & Seymor, 2013) are of the opinion that social support serves as a 'protective' factor against people's vulnerability because of the negative effects of stress on health. Such support is associated with networking, which provides social support and aims to reduce stress. Different ways to facilitate this supportive context will be discussed below.
Create safe spaces
The strengthening of the supportive context includes the creation of safe spaces, physical and emotional, as well as consistent supervision to the MCSA victim as individual. These safe spaces will enable the boys to learn to deal with guilt, anger, aggression and sexuality, as well as avoid re-experiencing the trauma associated with the MCSA. Sabalauskas et al. (2014) mention that these safe spaces can include instances where the role players focus on the thought processes that lead these MCSA victims to act out, rather than focusing on the acting out behaviour itself. From this exploration, role players can develop strategies with the boy, not for him, to enable the boys to shift their thinking to something more positive.
Throughout this study participants mentioned the MCSA victim's need to feel safe in all the different settings he is functioning in. Research literature (Bastiaanssen et al., 2014; Cohen et al., 2012; Ristuccia, 2013) confirm this need for safety. Several authors mention that safety can be advanced by providing supervision to these boys (Kenney, 2013; Rasmussen, 2013; Sahay, 2013; Soenen et al., 2014). According to Soenen, D'Oosterlinck and Broekaert (2013) as well as Wurtele (2012), most disruptive behaviour takes place at times and places where there is little if any supervision. The role players should take the following precautions to ensure the safety of these boys.
Data from the second and third phase of this study indicated that everything needs to be in place to ensure that the sexually abused boy is not exposed to any further sexual abuse (Cohen et al., 2012; Sahay, 2013). A way to accomplish this is to look into the room placements of these boys in the residential facilities. The ideal situation is to place these boys in single rooms. If this is not possible, however, not too many boys should be placed in one room and there should be safe spaces between the beds in a room to ensure that there can be no physical contact between the boys during the night. Boys of the same age and developmental stage should be placed together. It is also important to provide adequate monitoring, also during the night, to ensure the safety of all the boys. Wurtele (2012) suggests the use of surveillance cameras in strategic locations to advance supervision.
Participants from Phase 3 mentioned the unsupervised use of bathrooms during school time and at the residential facilities. It is important to ensure that these boys use the bathrooms only under proper supervision. Role players should structure their activities and lesson plans to have bathroom breaks regularly and therefore it would not be necessary for any boy to leave the classroom or residential facility group to use the bathroom without supervision. During break time and activity time the play area should be divided into different zones for the different age groups. This will minimise the chance of victimisation. Each area should have proper supervision.
Sometimes it might be necessary for the role players to intervene and remove the MCSA victim from a particular setting when the boy is becoming upset or restless. Then the role players can intervene in a positive manner. In these situations the role players can avoid confrontation and the escalation of behaviour by sending the boy on an errand, thereby giving him time to calm down. Several authors (Armstrong, 2012; Mundschenk, Miner & Nastally, 2011) confirm that this should be done before the behaviour escalates and the role player should make it a positive request. Participants in the second and third phase mentioned, however, that if the boy does not calm down and starts to show disruptive behaviour, there should be consistent and immediate consequences and the MCSA victim should take responsibility for his actions. According to Lewis, Romi and Roache (2012), the exclusion of a learner from a particular setting can be an effective means of dealing with, and immediate consequence of, disruptive behaviour. However, several authors (Greene, et al., 2014:ix; Otten & Tuttle, 2011) are of the opinion that exclusion may encourage negative attitudes towards school and teachers. This kind of suspension can actually reinforce the problem behaviour, because some of these learners do not want to be in the classroom. In some cases exclusion can decrease undesirable behaviour, but it does not teach a more appropriate behaviour response. The use of positive behaviour support (Armstrong, 2012; Sprague, Jolivette & Nelson, 2014), where positive and desired behaviour is reinforced, rather than using strategies of exclusionary discipline, can promote a more positive environment.
Structure environment to accommodate specific needs
The strengthening of a support network for MCSA victims also involves the setting of a highly structured environment by facilitating a routine. The facilitation of a routine creates security, consistency and predictability for the MCSA victim. This is supported by research (Bastiaanssen, Kroes, Nijhof, Delsing, Engels & Veerman, 2012; Boone, 2012; Quisenberry & Foltz, 2013; Suk-ching Chong & Leung, 2012). During the third phase the participants confirmed that in a structured and consistent environment, these MCSA victims feel safer, because they understand and know the guidelines and expectations. It is even better if this environment is consistent across all settings, such as at home, residential facility, class and counselling environment. It is important, however, to have a visual presentation (Otten & Tuttle, 2011) of a daily routine where all the boys can see it throughout the day. This visualisation can allow these boys to know exactly what activity will happen next and promote predictability.
In the second phase the participants mentioned that the daily routine should be structured properly with definite activities throughout the day. Participants from the first phase mentioned their struggle with less structured activities. This is also supported by several authors (Conley, 2013; Conn, Calais, Szilagyi, Baldwin & Jee, 2014; Nahgahgwon, Umbreit, Liaupsin & Turton, 2010). Bastiaanssen et al. (2012) add that these children should be stimulated to participate in activities. During the third phase it was suggested that in the classroom there should be activities, such as reading, computers and games, to keep the learners busy when their schoolwork is finished. Even at the residential facility the free time should be structured, like offering a choice between sport, reading, art, dancing, puzzles, computers or swimming.
Part of this routine also includes the physical structuring of these learners activities to create an organised and productive environment (Bastiaanssen et al., 2012; Mundschenk et al., 2011). It is important that they have a specific room and bed where they sleep every night, and have the same placement in the classroom and dining hall at the residential facility. This consistency will add to the facilitation of a support network. According to Simonsen, Fairbanks, Briesch, Myers and Sugai (2008), more structure promotes more appropriate behaviours.
The physical arrangement of these boys also impacts on their behaviour (Mundschenk et al., 2011; Simonsen et al., 2008). Data from the second and third phase implies that the physical space in which these boys are functioning should be designed to minimise crowding and distraction. Crowding can have a negative impact on behaviour. The simplest way to minimise crowding is to increase the amount of space in the different settings that these boys are in. If these boys feel crowded, they may experience challenges in self-regulating their behaviour. Role players should also be aware of things such as noise, lighting and temperature when designing the areas in which these boys should function. Simonsen et al. (2010) concur that crowding should be minimised.
The necessity of clear rules and boundaries for MCSA victims forms part of the supportive context for MCSA individuals. This is supported by several authors (Bastiaanssen et al., 2014; Boone, 2012; Curby, Rimm-Kaufman & Abry, 2013; Soenen et al., 2014; Vargas, 2013). During the third phase it was indicated that these rules and boundaries should be clear and easily understandable. They should be clear and behaviour specific (Reddy, Fabiano, Dudek & Hsu, 2013; Vargas, 2013) and should be concise, 10 words or fewer (Mundschenk et al., 2011). These rules should rather focus on what the boy should do than should not do. This will make for a more positive approach (Jolivette, Patterson, Swoszowski, McDaniel, Kennedy & Ennis, 2014; Mundschenk et al., 2011). Vagueness, repetition and complexity can muddle the boy's understanding and thus hamper compliance. Participants mentioned the importance of these rules and boundaries being consistent in all the different settings, and the consequences for not following these rules and boundaries should also be the same in the different settings, a view which is also supported by research literature (Conroy, Sutherland, Snyder & Marsh, 2008; Jolivette et al., 2014). Therefore in the context of a clinic school it is important that the different role players have regular meetings to discuss a specific boy's behaviour in order to implement the same rules, boundaries and consequences for not following these guidelines.
Coordinate support efforts
The use of a collaborative team could be very effective, as this draws on the special skills and knowledge of various role players (Kutash, Acri, Pollock, Armusewicz, Olin & Hoagwood, 2014; Zabel, Kaff & Teagarden, 2013). Bruns, Walker, Bernstein, Daleiden, Pullmann & Chorpita (2014) added that if systems work separately, they could be less effective in supporting the individual, as each system may maintain a separate plan for the child's care and prescribe multiple forms of support that are duplicated and/or uncoordinated. This fragmentation can undermine support efforts. In the proposed support strategy the collaborative team includes different role players. According to JvH (2012), this collaborative approach enables the different role players to apply the proposed support strategy in the different settings, such as at school, residential facility, home and counselling sessions in which these MCSA victims are functioning and thus optimise the level of support given to them. Therefore in the context of a clinic school it is important that the same strategy be applied in all the different settings.
These learners are living in a residential facility during the week with child and youth care workers. Their role can be described as professional parenting (Bastiaanssen et al., 2012; Bastiaanssen et al., 2014). These learners attend the clinic school, which is also on the same premises as the residential facility. The teachers are responsible for attending to the academic needs of these learners. There are also psychologists, social workers and counsellors who are responsible for the support and counselling of these learners (RE, 2014).
DISCUSSION
A proposed support strategy has been conceptualised that incorporates a focus on the development of the individual child who was an MCSA victim within a context of relationships that respect and acknowledge the child as a person as well as providing a safe environment. This attachment between the MCSA victim and the role players can serve as a protective factor (Bowlby, 2013) against the negative consequences of MCSA, where the boy can turn to the role player whenever protection or support is needed (Mikulincer & Shaver, 2007).
Although separated for the purpose of discussion, these elements of the proposed support strategy should be seen as interdependent and therefore part of a comprehensive support process that needs to be applied simultaneously and consistently by the role players in each of the systems in which these MCSA victims are functioning. This multilevel approach of support focuses on the child as an individual, as well as on the relationships in which the MCSA victims are involved and the different contexts in which they are functioning. These contexts can include home, school, residential facility and the counselling environment.
The proposed support strategy that applies these theoretical perspectives seems to indicate that the role players working with these boys do grasp the complexity of the challenges that these children face. Their assumed position is confirmed by the emphasis that they place on the need for communication between the role players. This is imperative to ensure the efficacy of the support. Therefore regular meetings are advised where feedback is given on how the MCSA victim is doing in the different settings, such as at home, school, residential facility and counselling environment. Sabalauskas et al. (2014) mention that, in adopting the strengths perspective, the role players discuss coping strategies and cognitive restructuring during these meetings rather than having a focus on consequences and restitution. Kutash et al. (2014) also stress the importance of communication in the collaborative team. Then all the role players will know what is happening in the boy's life and important information can be passed on from one setting to the others. These meetings must also allow for the adaptation of the proposed support strategy in order to streamline and coordinate it across the different settings for the particular boy. According to Molteni, Guldberg and Logan (2013), these meetings can also give the collaborative team a time and place to share ideas and good practice. The matter of confidentiality should be explicitly addressed, however, so that this information be treated with care in order for the MCSA victim to experience a trust relationship with the different role players.
The value of social support (Arias & Johnson, 2013; Sperry & Widom, 2013) to MCSA victims should be emphasised, as it can be seen as another protective factor against the negative impact of MCSA (Schönbucher et al., 2014). Support to MCSA victims is an ongoing process and therefore the application of these strategies will never come to an end. The role players need to take into account the complexity of support to MCSA victims, because of the vulnerability of these boys.
LIMITATIONS
Some limitations should be taken into consideration when interpreting the findings of this study. The first phase of the study explored the experiences of MCSA victims placed in a clinic school. The first limitation is that the findings are limited to a small sample of participants who are placed in a clinic school. Qualitative research can still be generalised when people in other contexts take note of this study and apply its findings that they can identify with in their different settings. A second limitation was the inclusion criteria, which stated that the boys had to disclose the MCSA at a previous stage or their parents had to give a clear indication of such abuse. Because of low disclosure rates among MCSA victims, it is possible that some potential participants were left out in this study. The third limitation was the sensitive nature of the research topic. Because of ethical considerations some sensitive questions could not be included in the study. The researcher who conducted the in-depth interviews also received expert supervision from a registered social worker and registered educational psychologist throughout the research project to ensure that she was competent and equipped to conduct this research.
In the second and third phases a limitation was the inclusion criteria which stated that the participants needed to have at least five years' experience of working with MCSA victims and/or clinic schools. The teachers and child and youth care workers in the clinic schools usually do not work for an extended period of time at a specific setting. Therefore quite a number of teachers and child and youth care workers working at the two clinic schools did not fit these criteria and therefore could not be included in this population. However, those participants who were included have a lot of experience of MCSA and/or clinic schools.
It should be noted, however, that parents' perceptions and inputs were not included, as a result of their limited availability for group or individual interviews. To compensate for this shortcoming the child and youth care workers, who serve as the learners' professional parents during the week, were included.
FINAL CONCLUSIONS
MCSA is a reality with extreme emotional and behavioural consequences for the sexually abused boy in middle childhood. These boys placed in a clinic school need support to deal with these consequences and to overcome some of the emotional and behavioural difficulties they are experiencing. In the unique context of a clinic school different role players can act as a collaborative and coordinated team to support these boys more effectively to enhance the process of integrating them into the mainstream educational system again as soon as possible.
A supportive space is created for MCSA victims through the proposed support strategy whereby support can be provided continuously. This integrated and coordinated approach will enable the role players who form part of a collaborative team to provide multilevel support. This ensures a simultaneous focus on the individual, relational and contextual levels in which these boys are functioning.
REFERENCES
ALAGGIA, R. & MILLINGTON, G. 2008. Male child sexual abuse: a phenomenology of betrayal. Clinical Social Work, 36:265-275. [ Links ]
ALAGGIA, R. & MISHNA, F. 2014. Self psychology and male child sexual abuse: healing relational betrayal. Clinical Social Work Journal, 42:41-48. [ Links ]
ARIAS, B. J. & JOHNSON, C.V. 2013. Voices of healing and recovery from childhood sexual abuse. Journal of Child Sexual Abuse, 22(7):822-841. [ Links ]
ARMSTRONG, T. 2012. Neurodiversity in the classroom: strength-based strategies to help students with special needs succeed in school and life. Alexandria: Association for Supervision & Curriculum Development. [ Links ]
BABBIE, E.R. 2013. The basics of social research (6th ed). Canada: Wadsworth Cengage Learning. [ Links ]
BARBOUR, R.S. 2014. Analysing focus groups. In: FLICK, U. (ed), The Sage handbook of qualitative data analysis. London: Sage Publications. [ Links ]
BARRON, I.G. & TOPPING, K.J. 2013. Exploratory evaluation of a school-based child sexual abuse prevention program. Journal of Child Sexual Abuse, 22:931-948. [ Links ]
BARTON, S., GONZALEZ, R. & TOMLINSON, P. 2011. Therapeutic residential care for children and young people: an attachment and trauma-informed model for practice. London: Jessica Kingsley. [ Links ]
BARUSCH, A., GRINGERI, C. & GEORGE, M. 2011. Rigor in qualitative social work research: a review of strategies used in published articles. Social Work Research, 35(1):11-19. [ Links ]
BASTIAANSSEN, I.L.W., DELSING, M.J.M.H., KROES, G., ENGELS, R.C.M.E. & VEERMAN, J.W. 2014. Group care worker interventions and child problem behavior in residential youth care: course and bidirectional associations. Children & Youth Services Review, 39:48-56. [ Links ]
BASTIAANSSEN, I.L.W., KROES, G., NIJHOF, K.S., DELSING, M.J.M.H., ENGELS, R.C.M.E. & VEERMAN, J.W. 2012. Measuring group care worker interventions in residential youth care. Child Youth Care Forum, 41:447-460. [ Links ]
BAZELEY, P. 2013. Qualitative data analysis: Practical strategies. London: Sage Publications. [ Links ]
BOONE, B. 2012. Basic training for residential childcare workers: a practical guide for improving service to children. Springfield: Charles C. Thomas. [ Links ]
BOWLBY, J. 2013. The making and breaking of affectional bonds. London: Routledge. [ Links ]
BRUNS, E.J., WALKER, J.S., BERNSTEIN, A., DALEIDEN, E., PULLMANN, M.D. & CHORPITA, B.F. 2014. Family voice with informed choice: coordinating wraparound with research-based treatment for children and adolescents. Journal of Clinical Child & Adolescent Psychology, 43(2):256-269. [ Links ]
CASEY, K.J., REID, R., TROUT, A.L., DUPPONG HURLEY, K., CHMELKA, M.B. & THOMPSON, R. 2010. The transition status of youth departing residential care. Child Youth Care Forum, 39:323-340. [ Links ]
CLARKE, V. & BRAUN, V. 2013. Teaching thematic analysis: overcoming challenges and developing strategies for effective learning. The Psychologist, 26(2), 120-123. [ Links ]
COHEN, J.A., MANNARINO, A.P., KLIETHERMES, M. & MURRAY, L.A. 2012. Trauma-focused CBT for youth with complex trauma. Child Abuse & Neglect, 36:528-541. [ Links ]
CONLEY, K. 2013. Healing the hurt child: Sean's story. Reclaiming Children and Youth, 22(2):44-50. [ Links ]
CONN, A., CALAIS, C., SZILAGYI, M., BALDWIN, C. & JEE, S.H. 2014. Youth in out-of-home care: relation of engagement in structured group activities with social and mental health measures. Children and Youth Services Review, 36:201-205. [ Links ]
CONROY, M.A., SUTHERLAND, K.S., SNYDER, A.L. & MARSH, S. 2008. Classwide interventions. Effective instruction makes a difference. Teaching Exceptional Children, 40(6):24-30. [ Links ]
CRESWELL, J.W. 2014. Research design: Qualitative, quantitative & mixed methods approaches (4th ed). London: Sage Publications. [ Links ]
CURBY, T.W., RIMM-KAUFMAN, S.E. & ABRY, T. 2013. Do emotional support and classroom organization earlier in the year set the stage for higher quality instruction? Journal of School Psychology, 51:557-569. [ Links ]
CYR, M., MCDUFF, P. & HÉBERT, M. 2013. Support and profiles of nonoffending mothers of sexually abused children. Journal of Child Sexual Abuse, 22:209-230. [ Links ]
DE SWART, J.J.W., VAN DEN BROEK, H., STAMS, G.J.J.M., ASSCHER, J.J., VAN DER LAAN, P.H., HOLSBRINK-ENGELS, G.A. & VAN DER HELM, G.H.P. 2012. The effectiveness of institutional youth care over the past three decades: a meta-analysis. Children and Youth Services Review, 34:1818-1824. [ Links ]
DEPARTMENT OF EDUCATION. 2001. Education white paper 6. Special needs education: Building an inclusive education and training system. [Online] Available: www.peopletoparliament.org.za [Accessed: 18/07/2013]. [ Links ]
DIAMANDUROS, T., COSENTINO, C.E., TYSINGER, P.D. & TYSINGER, J.A. 2012. Theoretical perspectives of male sexual abuse: conceptualization of a case study. Journal of Child Sexual Abuse, 21(2):131-154. [ Links ]
DORAHY, M.J. & CLEARWATER, K. 2012. Shame and guilt in men exposed to childhood sexual abuse: a qualitative investigation. Journal of Child Sexual Abuse, 21(2):155-175. [ Links ]
EASTON, S.D., SALTZMAN, L.Y. & WILLIS, D.G. 2014. "Would you tell under circumstances like that?": barrriers to disclosure of child sexual abuse for men. Psychology of Men & Masculinity, 15(4):460-469. [ Links ]
ELOFF, I., EBERSÖHN, L. & VILJOEN, J. 2007. Reconceptualising vulnerable children by acknowledging their assets. African Journal of AIDS Research, 6(1):79-86. [ Links ]
ENNIS, R.P., JOLIVETTE, K., SWOSZOWSKI, N.C. & JOHNSON, M.L. 2012. Secondary prevention efforts at a residential facility for students with emotional and behavioral disorders: function-based check-in, check-out. Residential Treatment for Children & Youth, 29:79-102. [ Links ]
FERGUSSON, D.M., MCLEOD., G.F.H. & HORWOOD, L.L. 2013. Childhood sexual abuse and adult developmental outcomes: findings from a 30-year longitudinal study in New Zealand. Child Abuse & Neglect, 37:664-674. [ Links ]
FLICK, G.L. 2011. Understanding and managing emotional and behavioural disorders in the classroom. Boston: Pearson. [ Links ]
FLICK, U. 2014. An introduction to qualitative research (5th ed). London: Sage Publications. [ Links ]
FREDERICK, J. & GODDARD, C. 2010. 'School was just a nightmare': childhood abuse and neglect and school experiences. Child and Family Social Work, 15:22-30. [ Links ]
GIL, E. 2011. Helping abused and traumatized children: integrating directive and nondirective approaches. New York: The Guilford Press. [ Links ]
GOSPODAREVSKAYA, E. 2013. Post-traumatic stress disorder and quality of life in sexually abused Australian children. Journal of Child Sexual Abuse, 22(3):277-296. [ Links ]
GRAY, M. 2011. Back to basics: A critique of the strengths perspective in social work. Families in Society: The Journal of Contemporary Social Services, 92(1):5-11. [ Links ]
GREEFF, M. 2011. Information collection interviewing. In: DE VOS, A.S., STRYDOM, H., FOUCHÈ, C.B. & DELPORT, C.S.L. (eds) Research at grass roots: For the social sciences and human service professions (4th ed). Pretoria: Van Schaik. [ Links ]
GREENE, C.A., GRASSO, D.J. & FORD, J.D. 2014. Emotion regulation in the wake of complex childhood trauma. In: PAT-HORENCZYK, R., BROM, D. & VOGEL, J,M. (eds) Helping children cope with trauma. Individual, family and community perspectives. London: Routledge. [ Links ]
GRINGERI, C., BARUSCH, A. & CAMHRON, C. 2013. Examining foundations of qualitative research: a review of social work dissertations, 2008-2010. Journal of Social Work Education, 49(1):760-773. [ Links ]
HANDWERK, M.L., HUEFNER, J.C., RINGLE, J.L., HOWARD, B.K., SOPER, S.H., ALMQUIST, J.K., CHMELKA, M.B. 2008. The role of therapeutic alliance in therapy outcomes for youth in residential care. Residential Treatment for Children & Youth, 25(2):145-164. [ Links ]
HARDING, J. 2013. Qualitative data analysis from start to finish. Los Angeles: Sage Publications. [ Links ]
HOUSE, J.S. 1981. Work stress and social support. Boston: Addison-Wesly Educational Publishers. [ Links ]
JACKSON, S., NEWALL, E. & BACKETT-MILBURN, K. 2013. Children's narratives of sexual abuse. Child and Family Social Work, 18(2):1-11. [ Links ]
JOLIVETTE, K., PATTERSON, D.P., SWOSZOWSKI, N.C., MCDANIEL, S.C., KENNEDY, C. & ENNIS, R.P. 2014. School-wide positive behavioural interventions and supports in a residential school for students with emotional and behavioral disorders: first years of implementation and maintenance follow-up focus groups. Residential Treatment for Children & Youth, 31(1):63-79. [ Links ]
JONES-SMITH, E. 2011. Spotlighting the strengths of every single student. California: Praeger. [ Links ]
KENNEY, W. 2013. Sexual misconduct in children: An intervention model that works in school and communities. Maryland: Rowman & Littlefield Education. [ Links ]
KISELICA, M.S. & ENGLAR-CARLSON, M. 2011. Establishing rapport with boys in individual counselling and psychotherapy: a male-friendly perspective. In: KISELICA, M.S., ENGLAR-CARLSON, M. & HORNE, A. (eds) Counselling troubled boys: A guidebook for professionals. [Online] Available: http://www.amazon.com [Accessed: 03/09/2013]. [ Links ]
KISELICA, M.S. & NOVACK, G. 2011. Promoting strength and recovery: counselling boys who have been sexually abused. In: KISELICA, M.S., ENGLAR-CARLSON, M. & HORNE, A. (eds) Counselling troubled boys: a guidebook for professionals. [Online] Available: http://www.amazon.com [Accessed: 03/09/2013]. [ Links ]
KOWAL, S. & O'CONNELL, D.G. 2014. Transcription as a crucial step of data analysis. In: FLICK, U. (ed.) The SAGE handbook of qualitative data analysis. London: Sage Publications. [ Links ]
KUTASH, K., ACRI, M., POLLOCK, M., ARMUSEWICZ, K., OLIN, S.S. & HOAGWOOD, K.E. 2014. Quality indicators for multidisciplinary team functioning in community-based children's mental health services. Administration & Policy in Mental Health & Mental Health Services Research, 41(1):55-68. [ Links ]
LEE, B.R. & BARTH, R.P. 2011. Defining group care programs: An index of reporting standards. Child Youth Care Forum, 40:253-266. [ Links ]
LEHR, C.A., SOON TAN, C. & YSSELDYKE, J. 2009. Alternative schools. A synthesis of state-level policy and research. Remedial and Special Education, 30(1):19-32. [ Links ]
LEWIS, R., ROMI, S. & ROACHE, J. 2012. Excluding students from classroom: Teacher techniques that promote student responsibility. Teaching and Teacher Education, 28:870-878. [ Links ]
LIERHEIMER, K. & STICHTER, J. 2011. Teaching facial expressions of emotion. Beyond Behaviour, 21(1):20-27. [ Links ]
LOH, J. 2013. Inquiry into issues of trustworthiness and quality in narrative studies: a perspective. Qualitative Report, 18(33):1-15. [ Links ]
MAIKOVICH-FONG, A.K. & JAFFEE, S.R. 2010. Sex differences in childhood sexual abuse characteristics and victims' emotional and behavioural problems: findings from a national sample of youth. Child Abuse & Neglect, 34(6):429-437. [ Links ]
MARZANO, M. 2012. Informed consent. In: GUBRIUM, J.F., HOLSTEIN, J., MARVASTI, A.B. & MCKINNEY, K.D. (eds) The SAGE handbook of interview research: the complexity of the craft (2nd ed). California: Sage Publications. [ Links ]
MATHEWS, S., ABRAHAMS, N. & JEWKES, R. 2013. Exploring mental health adjustment of children post sexual assault in South Africa. Journal of Child Sexual Abuse, 22:639-657. [ Links ]
MIKULINCER, M. & SHAVER, P.P. 2007. Attachment in adulthood: Structure, dynamics, and change. New York: Guilford Press. [ Links ]
MOLTENI, P., GULDBERG, K. & LOGAN, N. 2013. Autism and multidisciplinary teamwork through the SCERTS model. British Journal of Special Education, 40(3):137-145. [ Links ]
MUNDSCHENK, N.A., MINER, C.A. & NASTALLY, B.L. 2011. Effective classroom management: an air traffic control analogy. Intervention in School and Clinic, 47(2):98-103. [ Links ]
NAHGAHGWON, K.N., UMBREIT, J., LIAUPSIN, C.J. & TURTON, A.M. 2010. Function-based planning for young children at risk for emotional and behavioral disorders. Education and Treatment of Children, 33(4):537-559. [ Links ]
OTTEN, K. & TUTTLE, J. 2011. How to reach and teach children with challenging behaviour. San Francisco: John Wiley. [ Links ]
PARENT, S. & BANNON, J. 2012. Sexual abuse in sport: what about boys? Children and Youth Services Review, 34:354-359. [ Links ]
PHASHA, T.N. 2008. The role of the teacher in helping learners overcome the negative impact of child sexual abuse. A South African Perspective. School Psychology International, 29:303-327. [ Links ]
QUISENBERRY, C.M. & FOLTZ, R. 2013. Resilient youth in residential care. Residential Treatment for Children & Youth, 30:280-293. [ Links ]
RANAHAN, P. 2013. Being with: Child and youth care professionals' practice with suicidal adolescents. Relational Child and Youth Care Practice, 26(1):6-17. [ Links ]
RASMUSSEN, L.A. 2013. Young people who sexually abuse: a historical perspective and future directions. Journal of Child Sexual Abuse, 22:119-141. [ Links ]
REAMER, F.G. 2013. Ethics in qualitative research. In: FORTUNE, A.E., REID, W.J. & MILLER, R.L. (eds) Qualitative research in social work (2nd ed). New York: Columbia University Press. [ Links ]
REDDY, L.A., FABIANO, G.A., DUDEK, C.M. & HSU, L. 2013. Instructional and behavior management practices implemented by elementary general education teachers. Journal of School Psychology, 51:683-700. [ Links ]
REESE, L.E., HORNE, A.M., BELL, C.D. & WINGFIELD, J.H. 2011. Counselling aggressive boys and adolescent males. In: KISELICA, M.S., ENGLAR-CARLSON, M. & HORNE, A. (eds) Counselling troubled boys: A guidebook for professionals. [Online] Available: http://www.amazon.com [Accessed: 03/09/2013]. [ Links ]
RISTUCCIA, J.M. 2013. Creating safe and supportive schools for students impacted by traumatic experiences. In: ROSSEN, E. & HULL, R. (eds) Supporting and educating traumatized students: A guide for school-based professionals. New York: Oxford University Press. [ Links ]
ROBINSON, S. 2011. What play therapists do within the therapeutic relationship of humanistic/non-directive play therapy. Pastoral Care in Education, 29(3):207-220. [ Links ]
SABALAUSKAS, K.L., ORTOLANI, C.L. & MCCALL, M.J. 2014. Moving from pathology to possibility: integrating strengths-based interventions in child welfare provision. Child Care in Practice, 20(1):120-134. [ Links ]
SAHAY, S. 2013. Making of victim a patient: Sexually abused children and the consequences of unprofessional help. Psychological Studies, 58(2):153-163. [ Links ]
SALEEBEY, D. 2012. The strengths perspective in social work practice (6th ed). New York: Pearson. [ Links ]
SCHÖNBUCHER, V., MAIER, T., MOHLER-KUO, M., SCHNYDER, U. & LANDOLT, M.A. 2014. Adolescent perspectives on social support received in the aftermath of sexual abuse: A qualitative study. Archives of Sexual Behavior, 43:571-586. [ Links ]
SCHRAUFNAGEL, T.J., DAVIS, K.C., GEORGE, W.H. & NORRIS, J. 2010. Childhood sexual abuse in males and subsequent risky sexual behavior: a potential alcohol-use pathway. Child Abuse & Neglect, 34(5):369-378. [ Links ]
SCHWARTZ-SHEA, P., & YANOW, D. 2012. Interpretive research design: Concepts and processes. New York: Routledge. [ Links ]
SEIDMAN, I. 2012. Interviewing as qualitative research: a guide for researchers in education and the social sciences (4th ed). New York: Teachers College. [ Links ]
SIMONSEN, B., BRITTON, L. & YOUNG, D. 2010. School-wide positive behavior support in an alternative school setting. Journal of Positive Behaviour Interventions, 12(3):180-191. [ Links ]
SIMONSEN, B., FAIRBANKS, S., BRIESCH, A., MYERS, D. & SUGAI, G. 2008. Evidence-based practices in classroom management: considerations for research to practice. Education and Treatment of Children, 31(3):351-380. [ Links ]
SIMONSEN, B. & SUGAI, G. 2013. PBIS in alternative education settings: positive support for youth with high-risk behaviour. Education and Treatment of Children, 36(3):3-14. [ Links ]
SOENEN, B., D'OOSTERLINCK, F. & BROEKAERT, E. 2013. The voice of troubled youth: children's and adolescents' ideas on helpful elements of care. Children and Youth Services Review, 35:1297-1304. [ Links ]
SOENEN, B., D'OOSTERLINCK, F. & BROEKAERT, E. 2014. Implementing evidence-supported methods in residential care and special education: a process-model. Children and Youth Services Review, 36:155-162. [ Links ]
SOLAR, E. 2011. Prove them wrong. Be there for secondary students with an emotional or behavioral disability. Teaching Exceptional Children, 44(1):40-45. [ Links ]
SPERRY, D.M. & WIDOM, C.S. 2013. Child abuse and neglect, social support, and psychopathology in adulthood: a prospective investigation. Child Abuse & Neglect, 37:415-425. [ Links ]
SPRAGUE, J.R., JOLIVETTE, K. & NELSON, M. 2014. Applying positive behavioural interventions and supports in alternative education programs and secure juvenile facilities. In: WALKER, H.M. & GRESHAM, F.M. (eds) Handbook of evidence-based practices for emotional and behavioural disorders: Applications in schools. New York: Guilford Press. [ Links ]
ST. GEORGE, S. 2010. Applied interpretation: a review of interpretive description by Sally Thorne. The Qualitative Report, 15(6), 1624-1628. [ Links ]
STEYN, H., VAN WYK, C. & KITCHING, A.E. 2014. Boys in middle childhood placed in a clinic school: experiences of sexual abuse. Child Abuse Research in South Africa, 15(1):15-28. [ Links ]
STUART, C. 2013. Helping young people cope. Relational Child & Youth Care Practice, 26(1):3-5. [ Links ]
SUK-CHING CHONG, S. & LEUNG, K. 2012. Challenges and management frameworks of residential schools for students with severe emotional and behavioural difficulties in Hong Kong. British Journal of Special Education, 39(1):30-38. [ Links ]
SWANZEN, R. 2011. Relational child and youth care involves emotional intelligence. Relational Child and Youth Care Practice, 24(1-2):72-81. [ Links ]
THERON, L., CAMERON, C.A., DIDKOWSKY, N., LAU, C., LIEBENBERG, L. & UNGAR, M. 2011. A ''day in the lives'' of four resilient youths: cultural roots of resilience. Youth Society, 43:799-818. [ Links ]
THOMAS, G. 2010. Redrawing the front line: A play therapy service for meeting the psychosocial needs of children and families in school. In: DREWES, A.A. & SCHAEFER, C.E. (eds) School-based play therapy (2nd ed). New Jersey: John Wiley. [ Links ]
TRACY, S.J. 2010. Qualitative quality: Eight "big-tent" criteria for excellent qualitative research. Qualitative Inquiry, 16(10):837-851. [ Links ]
TRASK, E.V., WALSH, K. & DILILLO, D. 2011. Treatment effects for common outcomes of child sexual abuse: a current meta-analysis. Aggression and Violent Behaviour, 16:6-19. [ Links ]
VAN RENSBURG, A., THERON, L., ROTHMANN, S. & KITCHING, A.E. 2013. The relationship between services and resilience: a study of Sesotho-speaking youths. The Social Work Practitioner-Researcher, 25(3):286-308. [ Links ]
VAN TOLEDO, A. & SEYMOUR, F. 2013. Interventions for caregivers of children who disclose sexual abuse: a review. Clinical Psychology Review, 33(6):722-781. [ Links ]
VARGAS, J.S. 2013. Behaviour analysis for effective teaching (2nd ed). New York: Routledge. [ Links ]
WAYNE, R.H. 2013. Focus group. In: FORTUNE, A.E., REID, W.J. & MILLER, R.L. (eds) Qualitative research in social work (2nd ed). New York: Columbia University Press. [ Links ]
WILSON, L.C. & SCARPA, A. 2013. Childhood abuse, perceived social support, and posttraumatic stress symptoms: a moderation model. Psychological Trauma: Theory, Research, Practice, and Policy, June 3:1-7. [ Links ]
WURTELE, S.K. 2012. Preventing the sexual exploitation of minors in youth-serving organizations. Children and Youth Services Review, 34:2442-2453. [ Links ]
ZABEL, R.H., KAFF, M. & TEAGARDEN, J. 2013. Promoting interdisciplinary practice: an interview with Steven R. Forness. Intervention in School and Clinic, 49(4):255-260. [ Links ]
ZEUTHEN, K. & HAGELSKJÆR, M. 2013. Prevention of child sexual abuse: analysis and discussion of the field. Journal of Child Sexual Abuse, 22:742-760. [ Links ]
1 In the case of personal communications, the initials of the persons were used to protect their identity.


{kind=link}