










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.53 n.4 Stellenbosch 2017
http://dx.doi.org/10.15270/52-2-590
ARTICLES
The Grief and Trauma Project: a group work approach to restoring emotional and spiritual health to women in bereaved and traumatised indigent communities in the Western Cape, South Africa
Mrs Hilary McLeaI; Prof. Pat MayersII
IProject designer: 'The Warehouse', Registered NPO, Cape Town, Registered Social Worker in private practice
IIDivision of Nursing & Midwifery, Department of Health & Rehabilitation Sciences, Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
The extreme levels of grief and trauma experienced in resource-poor communities in South Africa are well documented. The concept of grief or trauma being experienced and managed as an isolated incident and access to psychological therapeutic support being available is assumed in much of Western literature. This study describes a response to the multiple grief and loss experiences of indigent South African communities, its continual nature and the paucity of help available. A group work approach to providing psychosocial and spiritual support was developed and implemented. Improved mental health, physical health and interpersonal relationship outcomes are described.
INTRODUCTION AND BACKGROUND
Many South African communities are exposed to multiple traumatic experiences, including ongoing community and domestic violence and family murders (Statistics South Africa, 2014; Kaminer, Du Plessis, Hardy & Benjamin, 2013; Weierstall, Hinsberger, Kaminer, Holtzhausen, Madikane & Elbert, 2013) In particular, historically disadvantaged and resource-poor communities in South Africa experience high levels of violence and trauma, fuelled by rapid urbanisation with associated infrastructural disparities (Atwoli, Stein, Williams, McLaughlin, Petukhova, Kessler & Koenen, 2013). The high level of murder, sexual assault and robbery is well documented (SAPS Official Crime Statistics 2012/2013). Half of the murder rate of 33:100,000 occurs in only 12.3% of police precincts, all of them low-income areas (Lancaster, 2015). South African women who live with high levels of crime and violence experience grief and trauma not as singular events, but as multiple continuous processes, in which trauma and stress is current, ongoing and anticipated, known as continuous traumatic stress (Statistics South Africa, 2014; Eagle & Kaminer, 2013; Straker, 2013). For many, the constant struggle for survival takes priority over grief in the event of a death in the family (Demmer, 2007; Gould, 2014).
The effects of trauma in South Africa are complex. In the South African Stress and Health (SASH) survey, Atwoli et al. (2013) reported that the lifetime and 12-month prevalence rates of PTSD were 2.3% and 0.7% respectively. Rosenblatt and Nkosi (2007) studied the year-long isolation and estrangement of widows from the entire community and the difficulties of this occurring in a transitional society; Rashe (2008) examined the coping mechanisms of women who experienced intimate partner violence with little recourse to help. Kaminer and Eagle (2010:155), writing on the levels of violence and trauma experienced particularly in indigent South African communities, point out the need for "local, contextually-specific understandings and interventions to emerge" and for researchers to understand "the intersection of continuous trauma and the structural violence of poverty which creates a particular challenge for South Africans." Violence, experienced personally or as a community, is transmitted through family systems and affects the ability to overcome situations (Benjamin & Crawford-Browne, 2010). The changing economic social and political context is also part of the experience of resource-poor violent communities (Kotzé, Els & Rajuili-Masilo, 2012; Drenth, Herbst & Strydom, 2010).
For most women in this situation, removal from the continuous traumatic events is impossible. Traditional forms of individual psychological and therapeutic support are unavailable to the majority of the population, given the numbers of social workers available, against the numbers requiring social work intervention in terms of the current legislation for vulnerable elderly, children and the disabled (Waters, 2013). Support for women in this position needs to be contextual, relevant and feasible. Religious rituals serve a specific purpose for women who have experienced trauma, but nothing further is offered by church, society or formal mental health structures after a death or traumatic event (Copeland-Linder, 2006).
LOSS AND GRIEF IN TRAUMATISED INDIVIDUALS AND COMMUNITIES
Most of the literature on this topic emanates from a Western worldview and assumes that a loss, grief or trauma is an individual experience which can be dealt with in isolation and regular life resumes after it has been appropriately addressed (Breen & O'Connor, 2007). The situation in indigent communities in South Africa does not allow for this separation of events, since trauma, loss and grief are often experienced communally.
Loss has been viewed as 'grief work' and theories have been developed which provide a particular understanding for satisfactory resolution of the loss (Parkes, 1996; Worden, 2003). Attachment theories have attempted to explain individual processes for coping with loss and to explain the wide differences exhibited (Bowlby, 2005; Wayment & Vierthaler, 2002; Field, 2006). These theories have been challenged (Wortman & Silver, 1989), as have theories relating to the connection with the dead, e.g. leaving the dead behind and reinvesting in new relationships has been countered with the view that the bonds between the deceased and the survivor continue but in a different form (Klass, 1999). Stroebe and Schut have argued that what occurs for the bereaved person is a fluctuation between loss and restoration-orientated processes as the person learns to adapt to the loss (Stroebe & Schut, 1999; Stroebe, 2001). A move to study 'resilience' and the constructs that make it possible for most people to cope marked a new direction in the understanding of loss and grief (Bonanno, 2004). This included the exploration of de-stigmatisation and understanding healthy responses to loss. Meaning-reconstruction theory, demonstrating that growth is possible as an outcome (using ongoing attachment, capacity to make sense of life, finding benefit in the experience, and reconstructing the experience) is a model that has emerged from more recent research in the field (Neimeyer & Anderson, 2002; Neimeyer, Baldwin & Gillies, 2006; Gillies & Neimeyer, 2006).
Breen and O'Connor (2007) argue there is a paradox in distinguishing 'normal' grief from complicated grief experiences. The is evident in the three major tensions that exist in the thanatological literature: the dominance of grief theories, the medicalisation of grief, and the effectiveness of grief interventions. The authors argue that there is a need to provide improved grief education for service providers, the bereaved, and the wider community, to conduct research that emphasises the context of grief and is relevant to service provision, and that current grief interventions require re-examination (Breen & O'Connor, 2007).
Gender and multicultural aspects are critical factors in the variable outcomes of grieving populations (Berzoff, 2003; Gillies & Neimeyer, 2006; Rothaupt & Becker, 2007; Stroebe, 2008). Religious or spiritual beliefs in the afterlife and continued attachment influence the individual in his/her bereavement. The role of spirituality and religion for those facing a traumatic death are influences that are not well understood (Benore & Park, 2004; Chapple, Swift & Ziebland, 2011).
There is limited published literature on non-traditional therapeutic approaches to managing loss and grief in African communities. Studies conducted in indigent communities with respect to continuous traumatic stress, grief and loss have reported on their psychological and physical health impact on individuals and groups. The manner though which violence, whether personally experienced or as a community, is transmitted through family systems and the ways in which this can be interrupted has also been investigated (Hunt, Andrew & Weitz, 2007; Pereira, Andrew, Pednekar, Pai, Pelto & Patel, 2007; Marshall & Sutherland, 2008). Hunt et al. (2007) described a group method of managing grief, using the nine-cell bereavement tool. More recently, the concept of 'reasonable hope' has been used to investigate the use of tools that can be employed to move people from passivity to action and protection in dangerous or recurrently violent settings (Weingarten, 2003; Benjamin & Crawford-Browne, 2010; Weingarten; 2010).
The importance of cross-cultural practice and the indigenisation of African social work is receiving attention. Dialogue between cultural groups on principles, ethical norms and appropriate practice needs to inform interventions (Gray & Allegritti, 2003; Gray & Coates, 2010). Different cultures have different emphases, but all are reported as having a cultural, spiritual and community ritual base (Appel & Papaikonomou, 2013; Selepe & Edwards, 2008). The literature explores how these processes help with restoration and healing and meaning-making. Therapeutic procedures are used as opposed to crisis intervention and are considered as creative and proactive rather than medical and analytic (Hale, 1996; D'Souza, 2000; Nwoye, 2005; Selepe & Edwards, 2008).
In direct contrast to the Western model of support for individual grief, adhering to community-led customs is seen as more beneficial than operating as an individual (Rosenblatt & Nkosi 2007; Radzilani, 2010). It is important to consider different approaches to mourning, death and funeral practices, cultural rituals and influence of the ancestors and the necessity for the bereaved to appease them. These practices are considered essential for keeping communities stable and prosperous, and there are negative effects if these rituals and practices are not followed (Selepe & Edwards, 2008; Makhaba, Memela & Magojo, 2009; Keen, Murray & Payne, 2012).
In the South African context, the literature describing the management of loss and grief ranges from the Western individualistic, private and professionally managed to the descriptive and explanatory work of understanding of loss and grief that is embedded in a cultural, spiritual and community base and therefore collectively understood. Gray and Allegritti (2003) argue for inter-cultural dialogue on principles, norms and practices in varying cultures in reaction to the dominant Western approach to interventions found in the literature. Varying cultures are being examined for difference and similarities (Appel & Papaikonomou, 2013). The literature pertaining to resource-poor communities in urban and rural settings focuses on cultural rituals and community support (Setsiba, 2012; Yawa, 2010; Radzilani, 2010). An assumption of availability of adequate resources to support the bereaved person as an individual fails to take into account the context of complicated grief on conjugal bereavement of women in rural, indigent and marginalised communities (Opperman & Novello, 2006; Somhlaba & Wait, 2008) and low-income communities characterised by violence, death and continuous stress (Eagle, 2015).
Cross-cultural sensitivity is vital when working in a context where Western and traditional frameworks intersect (Nembahe, 1998). The contextual analysis of rural black women and depression and the assessment of needs and group strengths and weaknesses (Brown, Brody & Stoneman, 2000), as well as assessment of grief through culture and community (Kasiram & Partab, 2002) all form part of a new approach - the use of rigorous methodology within a group context and culture when dealing with loss and grief.
The traditions of various indigenous groups and the effects of the prescribed communally imposed rituals, especially with respect to the effect on women (who play the major role in the prescribed actions) and the role of the ancestors in understanding the communities' reactions to loss and grief were explored in a study of the Batswana population's experience of isolation as a result of stigmatisation of widowhood (Manyedi, Koen & Greeff, 2004). This study reported that witchcraft plays a large role in apportioning blame for distress and death. Continued trauma, deaths, illness and losses are considered a sign of ancestor displeasure and an explanation of further losses and distress (Manyedi et al., 2004; Ashforth, 2005).
Within South African communities the inter-relationships between loss, grief, trauma and traumatic stress are often concurrently experienced, given the high levels of communal and personal violence (Kaminer, et al., 2013; Statistics South Africa, 2014; South African Police Service, 2015). Kaminer and Eagle (2010:149) argue that there are significant limitations to exploring the impact of trauma with the use of "highly structured tools developed in contexts other than our own".
Theories of grief (Klass, 1999; Stroebe, 2001; Worden, 2003; Neimeyer et al., 2006) focus mainly on the individual in need of psychological support. The influence of context on the experience and manifestation of grief with reference to South Africa has been studied by Kasiram and Partab (2002) and Somhlaba and Wait (2009); however the focus has remained on individuals and their reactions to grief. Community counsellors experience trauma at the personal and vicarious level (Benjamin, 2011) that are related to the systemic on-going violence to which they are exposed, as well having to counsel persons affected by trauma and violence.
In the South African setting dual exposure to grief and trauma should not be considered as isolated events, which can be ameliorated with professional support, as this approach ignores the presence of continuous trauma and stress alongside the grief experienced. Continuous traumatic stress impacts on individuals and groups with changes in physical and psychological health.
THEORETICAL FRAMEWORK
The South African context is one in which high levels of violence disproportionally occur in resource-poor communities, in urban and peri-urban areas known as 'townships', the aftermath of the apartheid era (1948-1994). Indigenous African groups in the urban areas were forced to live in high-density townships with poor infrastructure and community resources. Lack of alternative accommodation at an affordable price prevents most people from moving to preferred alternative areas.
In this context of high exposure to violence and loss an emotional and psychological support mechanism for the resource poor was developed which took into account the shortage of professional social workers in the country (Waters, 2013; Dlamini & Sewpaul, 2015).
The framework for the development of the intervention was that of 'reasonable hope' (Weingarten, 2010). Reasonable hope provides the therapist and client "with a way of thinking about hope that makes it more accessible even in the grimmest circumstances" (Weingarten, 2010:8). Reasonable hope looks not for the perfect solution, but for what may be good enough and thus initiates the process of change. Small actions are not trivial as they have ripple effects and set in motion a move towards action and creativity as opposed to passivity and helplessness. Five characteristics of reasonable hope are described: it is "relational; consists of a practice; maintains that the future is open, uncertain, and open to being influenced; seeks goals and pathways to them; and accommodates doubt, contradictions, and despair" (Weingarten, 2010:8).
Weingarten (2010) argues that a method of modelling change in a setting in which change was thought impossible is to harness the inherent knowledge of the people in their change process. The method of a group using their own experiences to engage with tools to bring personal and community change was developed. Weingarten's approach helps a participant to identify the smallest possible actual step that can be taken with respect to a change in thinking or behaviour. The smallest action taken can facilitate hope in a fear-filled person. The steps of this approach are outlined below.
-
Have a definite goal. Hope is about what is possible.
-
Reasonable hope is looking for the next smallest step you can take. Make a path to this goal that works. It can be small and ordinary.
-
We can feel despair and reasonable hope at the same time.
-
The brain can change. There is no need to remain in a negative situation.
-
Reasonable hope can best be expressed in a situation where you feel safe and calm.
-
Hope can grow in a community. People can do it together.
-
It is alright not to do everything that needs to be done. Make sure just ONE thing is done (Weingarten, 2010)
AIM AND OBJECTIVES
The aim of this study was to provide tools to restore emotional and spiritual health to women in bereaved and traumatised communities in the greater Cape Town area through a group intervention. The objectives for the study were that participants would:
-
No longer feel overwhelmed by their grief/trauma story;
-
Understand the physical, emotional and mental effects of grief/trauma;
-
Experience improved self-esteem, linked to their experience of survival;
-
Experience improved physical and emotional health;
-
Understand the concept of 'reasonable hope' and how it can help an individual to cope with trauma.
STUDY SETTING
The areas selected for the study were high-density poor socio-economic townships in Cape Town that include both formal and informal dwellings, which were located within 20 kilometres from the city centre. These areas are characterised by poor socio-economic conditions, unemployment and limited access to resources, and they experience high levels of interpersonal and communal violence, including gangsterism (Benjamin, 2011). The population of the selected townships is primarily of Xhosa origin, the second largest indigenous population group in the country and the dominant indigenous group in the study sites (Stats SA Mid-Year Estimates, 2016). The programme was offered at centrally located venues, in the main church halls, close to public transport hubs, which were accessed through church leaders who made their premises available at no cost.
POPULATION AND SAMPLE
Participants were recruited through information provided to church leaders, churches women's group meetings and their extended social networks. Snowball sampling was employed to ensure selection to the study of persons who had experience of the phenomenon. The inclusion criteria were women who had experienced ongoing trauma and loss, were willing and available to participate. Low literacy levels were not considered a barrier to participation. Participation was open to all.
Four groups were recruited from the local community. Fifty-seven women agreed to participate in the programme. Participants' average age was 45 and each had raised on average 3.8 children. Each group comprised between 8 to 15 women. Attendance at the groups was confidential and neither the church minister nor the women's group leader were informed as to who attended. No church leaders were invited to the groups to ensure privacy. Participants' names were not divulged to anyone outside of the group. They had the right to withdraw from the group at any stage without negative affect. Personal information was confidential and would not be used outside of the group experience. A contract of confidentiality between group members was an agreed part of the process.
GAINING ACCESS
As faith organisations and churches play an important part in the life of the communities from which the participants were drawn, recruitment of group participants was through eight church leaders who lived in their local communities. Leaders of political, social, cultural or other groupings were not considered for this initial study as sufficient numbers of participants were recruited through the churches and the church venues were familiar, safe and within walking distance of the participants' homes.
The church leaders gave the names of the church-based women's group leaders, who could facilitate the spread of the information to members who had experienced grief and trauma and who knew others with similar experiences. They were asked not to approach people directly to minimise coercion and bias. Women who were interested in participating were encouraged to attend and inform friends and neighbours about the groups. An introductory session was offered to explain the programme and give attendees an opportunity to invite others to join the group for the first formal session.
ETHICAL CONSIDERATIONS
Ethical approval for the study was granted by the Human Sciences Research Council (HSRC) 3/16/03/11. The principles of beneficence, non-maleficence, autonomy and justice were adhered to. Participation was voluntary and the right to withdraw without prejudice was explained. Interested persons attended session one, at which the programme was fully explained and questions answered. The purpose and the reason for the research were explained and all questions answered. Participants gave written informed consent on a form in the language of their choice. Participants' rights were protected during data collection. They were advised that they would be free to see the results of the research. Participants' rights were respected at all times.
Measures were put in place to protect participants from any harm and allow them to withdraw at any time during the programme. The need for record keeping was explained. Confidentiality and anonymity of participants was assured by keeping separate records for personal details and the use of numbers in place of names. Participants were informed of possible negative effects that could result from the research. Because the topic being investigated related to emotional events in participants' lives, they were offered access to professional support, if needed.
RESEARCH DESIGN AND METHOD
A three-phase process was employed:
-
design of the programme;
-
intervention (implementation of the programme - facilitation of the groups);
-
participant feedback of the programme.
Phase One: Design of the programme
The study utilised a pre-post-test intervention design. An initial literature review was conducted of the subject. The primary researcher spent time engaging with Xhosa culture, styles of worship, death rituals, funeral and bereavement support practices, responses to grief and trauma in the context of people's lives in resource-poor communities. A six-session programme was designed with a follow-up session after three months. Questionnaires were administered at three points: session one, session seven and the follow-up session eight. They were specifically chosen as they are a multiple-choice method, could be administered verbally and only a number had to be circled after each question was given verbally. This was to accommodate illiterate or semi-literate participants. The Associate Group Analysis (AGA) method (Kelly, 1985, Ryan, 2006) was used to evaluate the programme.
Data-collection tools
The workshop process used English as the language of delivery, but all information sheets and questionnaires were translated into Xhosa for those who preferred to communicate and write or read in their home language.
The BAI and the BDI-II questionnaires (multiple-choice self-report inventory) were selected for the study to ensure that the three sets of data could be used to measure the change in anxiety and depression following the programme (Dozois & Covin, 2004). The validated isiXhosa version of the tools was used, thus English and IsiXhosa versions were made available to participants, and they could complete the questionnaires in the language of their choice. Questions were verbally delivered in both languages to ensure that low-literate or illiterate participants were fully included in the process and could (with assistance from another group participant) complete the questionnaires. This support of the participants of each other was not directed in any way by the facilitator, but arose spontaneously from members of the group. The results were used to guide the workshop facilitator as to the levels of anxiety and trauma in participants, in how to manage any extreme emotion in the participants. As the researcher had no prior knowledge of the participants' mental states, findings from the questionnaires served to alert her to any significant stresses in participants in order to refer such persons for professional counselling, if this was considered necessary.
Phase Two: Intervention
After ethical approval had been obtained from the Human Sciences Research Council (HSRC) for between six and eight group workshop sessions, a pilot study was conducted during 2010 with two groups to test the workshop programme. Adaptions were made to the personal information sheet to include not only the number of children born to a participant, but how many children had actually been raised by the participant, as this inclusive parenting of needy family members was found to be a common occurrence in the target areas. To facilitate completion of the workshop programme, an extra session was included to accommodate participants who may have had difficulty in attending because of factors such as community protests over lack of services or unhappiness with governments provision of resources (a percentage of which may possibly turn violent) and attending the workshop session would be physically unsafe. This provision was required on two separate occasions over the life of the groups for the reasons outlined.
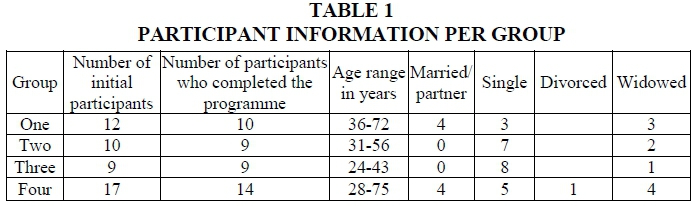
Four groups were conducted; one in each of the townships of Nyanga, Sweet Home Farm, Khayelitsha and Philippi within the City of Cape Town metropole during 2011 and 2012. Each group programme was run over seven sessions, facilitated by the first author. Participant information for each group programme is indicated in Table 1.
It should be noted that in each group several participants circled more than one option under the heading marital status, thus marital status information may not be accurate.
The seven-session programme (Table 2) commenced with an initial introductory session. During this session women were encouraged to inform others about the programme in order to encourage attendance by others. This session was followed by six weekly three-hour sessions. Each session comprised of a scripture reading, prayer, a verbal expression of a feeling experienced, and a range of skills to manage the context they find themselves in (see Table 2). Exercises to enable participants to openly speak of emotional states were included in each session. Exercises were designed so that women could work in pairs and this encouraged active participation. Light refreshments were provided in each session.
In session six the concept of 'reasonable hope' was introduced. Each participant chose one self-selected task to work on during the intervening period based on the reasonable hope concept. A seventh and final session was conducted twelve weeks after session six. The average length of time of a group's existence was 19 weeks.
In session six the 'reasonable hope' exercise was explained for the participants to work on during the three-month break. This required each participant to choose a personal hope: for themselves, some other person or situation they had not expressed before, which they could imagine seeing come to fruition in the intervening 3 months till the group reconvened.
In session seven the feedback regarding change experienced through the reasonable hope exercise was recorded. Each participant was provided with the feedback from the BAI and BDI-II questionnaires (the final questionnaire was scored during the session) if requested. A score for anxiety and depression was obtained for each participant. The questionnaire scores were not included in the evaluation. The scores were used to alert the facilitator to potential distress in a participant, which might require referral to formal counselling. Of the 57 participants, only two needed further professional counselling. This was offered and each had an individual session with the field researcher, who is a registered professional social worker.
Phase Three: Evaluation of the programme
The evaluation of the programme was undertaken between three and ten months after completion of the workshops, to determine the effect that the workshops had on participants and to establish whether changes need to be made to future workshops. The focus of the evaluation was on the impact of the workshops on the grief and trauma in participants' lives.
Of the 59 participants in the four workshop groups, 41 had contactable cell phone numbers to be invited to the evaluation session. Thirteen participants from the communities of Nyanga, Khayelitsha and Philippi in the Cape Town Metropole attended the evaluation session. There were no attendees from the Sweet Home Farm group as there were difficulties making contact with them, as cell phones were the main means of communication and are also often stolen. Three of the participants had secured employment in the intervening period and were therefore unavailable. Participants' travel costs were reimbursed and refreshments were provided at the end of the session. Participants were placed in the same groups they had been in for the workshop sessions. A person fluent in isiXhosa and English, unknown to the participants, facilitated each group. The evaluation session (held in both languages according to the choice of the participants) consisted of two parts: the first section utilised a short questionnaire comprising six questions which required a written answer, and in the second section each participant was asked to give verbal examples of the change they had experienced as a result of the workshop.
The six evaluation questions, available in English and isiXhosa (Table 3), were designed using the Associative Group Analysis (AGA) method (Kelly, 1985; Grenard, 2003). The method uses continuous free word association and measures perceptions, attitudes and beliefs without directly asking participants to identify these characteristics (Grenard, 2003). This method was used to determine the effect of the programme on the psychological disposition of the participants. The method can be used without reference to either levels of formal education or language fluency or literacy fluency. It is a scientific unstructured method helping to identify subjective perceptions and dominant characteristics of members of different cultural groups. It specifically accommodates varying levels of ability, differing home languages, language and literacy skill levels and educational qualifications. It was chosen specifically to address this cross-section of South African society, represented in the community from which the participants were drawn (Snyman, Pressentin & Clarke, 2015).
Participants were asked to write down as many words as they could think of. In AGA the analysis requires that a weighted score is given to each response in the order they were written down. Although this method assumes a level of literacy, the questions were all given verbally as well as in written form and there was no time limit given for the responses. It was assumed that as only one-word answers were required this would not be a deterrent to the less literate. The use of AGA (though developed for a north European context) was considered positive in its ability to measure responses from a wide educational spectrum as it caters for this feature of South African society. Although some participants answered using multiple words, one-word replies were found to be sufficient for the scoring method. The written responses were recorded without correction of any kind as they were received.
Identical or thematic responses were then grouped together and their scores combined to give an overall ordered list of words. The weighting of responses facilitates comparison of the ranking of participant responses across the groups. Rather than using individual words as the trigger, evaluation questions were chosen to keep the focus of the responses on the participant's wellbeing before and after the workshops.
In the second part of the evaluation session participants were asked to give examples of the change they had experienced as a result of the workshop. Participants were asked the following questions, in order:
-
Can you give an example of something that has changed in your life because of the workshop / anything else?
-
When would you suggest to a friend or a neighbour that they attend the workshop? What would have happened to them for you to suggest it as a good idea?
-
What would you say to them about the workshop and why they should go?
The narrative responses were audio-recorded. They were then transcribed and translated into English from isiXhosa where necessary. These were checked by the translator and then verified by a second translator. The responses were then analysed by identifying key phrases in each narrative and grouping together similar responses.
The completed evaluation questions were collected for analysis. Any responses written in Xhosa were translated into English, and verified by a second translator. The responses to the evaluation questions were collated and each response weighted according to AGA methodology. Similar responses were then grouped together.
TRUSTWORTHINESS
Trustworthiness is established in qualitative studies through ensuring credibility, transferability, dependability and confirmability (Shenton, 2004). The primary researcher kept detailed field notes of the intervention and had regular feedback sessions with the research team of three mental health professionals. The researcher also ensured prolonged engagement with the participants. Triangulation of the data was accomplished with the collection of the evaluation questions and the verbal examples of the changes participants experienced as a result of the workshop. As required as part of the AGA methodology (Grenard, 2003), the second part of the workshop required participants to reflect on the effect that the workshops had on them and to consider under what circumstances they would recommend the workshops to someone else. As wide a range of participants as possible contributed to diversity and richness of the data (triangulation through data sources) and a comprehensive project report (Meldrum & Greathead, 2012) was compiled to facilitate auditability and transferability.
FINDINGS
Five anticipated outcomes were identified for the workshops, namely that the participants would:
-
No longer feel overwhelmed by their grief/trauma story;
-
Understand the physical, emotional and mental effects of grief/trauma;
-
Experience improved self-esteem, linked to their experience of survival;
-
Experience improved physical and emotional health;
-
Understand the concept of 'reasonable hope' and how it can help a person to cope with day-to-day living.
PARTICIPANTS' EVALUATION OF THE WORKSHOP
Participants reported changes in their lives as a result of their attendance. These were identified as the revival of hope from a hopeless position, improved relationships with others, and learning how to share their problems with others. Participants found the tools that the facilitator used as part of the process during the workshop sessions useful. The workshop had given the participants hope where they had none before, hope not just for the present but also for the future. Personal growth was for them an important outcome. In the second question participants were asked to consider their personal situations prior to participation in the workshop programme. Participants were suffering from isolation, needing to withdraw and feeling unable to share their feelings with anyone else. They also reflected on their emotional pain and difficulties with relationships and how the workshops had facilitated their ability to engage more positively in their relationships.
Participants were also asked to reflect on their current situation (Question 3). They reported that they no longer felt overwhelmed by their story and there was a sense of restoration experienced; they also reported an improvement in personal relationships and restoration of hope and they felt that they had learned how to support others. Suggestions for changes or improvement to the programme (Question 4) included that that sessions could be more frequent and venues should be more accessible, and there was a perceived need for the workshops to be offered to the wider community. The aspects of the workshop which was experienced as most helpful (Question 5) were the opportunities to share their stories with others and support for participants' prayer life/spiritual life. There were only positive comments about the workshops and a desire expressed for longer sessions, and changing the timing of the session so as to make them more accessible.
OUTCOMES OF THE PROJECT
Of particular interest was that not only did the project achieve the intended outcomes, but the evaluation reflected that the participants had benefited in other areas of their lives: they reported improvement in their close interpersonal relationships and in their spiritual lives, and a decrease in destructive behaviour patterns.
Improvement in participants' close interpersonal relationships
The most noticeable unintended outcome was that of improved relationships. A change in attitude was anticipated as a result of the intervention; however, the participants regarded this as one of the most important outcomes of their participation in the programme. Participants commented on how their relationships had changed:
"Before I came across this workshop, I used to fight a lot with my cousins but now I can sit down and talk things through with them and then we are able to forgive each other."
"Everyone talks as they please and (I) am not easily hurt now, (I) am now able to listen and work out how it happened before jumping to a conclusion."
Improved spiritual life
The spiritual element to the programme was found to be very helpful. Several participants spoke about how they had experienced an improvement in their own spiritual lives. The spiritual aspect of the programme (scriptures and prayer) were highly valued, as noted in the participant reflections:
"... the passages from scripture she used were of great help to me."
"The workshop has motivated me, particularly our prayer moments ... It helped a lot because every time we pray after prayer one can see a change in people's faces."
"I would definitely advise my neighbour to attend the workshop because we meet with other ladies. We pray and share with each other our problems. One never knows their neighbour's problems and how they live their lives. But here we are able to pray against challenges and by the time we live we know what each is going through and we cry with each other. I can invite my neighbour to attend to lessen her problems."
Changes in behaviour
Although behaviour change was an outcome that was anticipated, such behaviour is difficult to evaluate and was therefore not specifically included. The participants, however, particularly valued the effects of their learning on this aspect of their lives. "I do things differently now, and yes am doing my best". "The change in my life has been huge…" Changes identified included being able to share problems with others, not withdrawing or isolating one's self, improved communication with others. "I have made peace now with my family."
Of particular interest is the change in being able to manage anger and reduce aggression.
"After the workshop I was alright because before I used to be an angry person. But since the workshop I am not as angry, am now able to deal with things I was not able to deal with before."
BDI-II and BAI data
The sample size was too limited to determine any statistically significant change in the participants' wellbeing (Meldrum & Greathead, 2012). Although the participants reported an improvement in their daily lives, it was not possible to statistically associate this improvement with the workshop attendance.
DISCUSSION
The evaluation of the Grief and Trauma project with women in resource-poor settings in townships around Cape Town showed that the programme achieved its aims. There was an overwhelmingly positive response in the women who joined the programme and who had no sense of control or hope for their futures. The power of the shared stories gives insight and a sense of managing their lives.
In a context of grief and trauma that the participants can do little to change, a group approach can provide a healing space for dealing with the emotional, psychological and physical reactions, for which there are limited, if any, formal therapeutic services. Group approaches are more cost effective in dealing with community trauma (Opperman & Novello, 2006; Kasiram & Partab, 2002).
The socio-economic conditions in which the participants live are such that any form of escape or relief is very limited, if not impossible. Physical and emotional reactions to trauma and loss are intertwined (Kaminer & Eagle, 2010; Pereira et al., 2007). This is a method of offering tools to healthily manage their lives in their particular context in a more positive manner. It employs context-specific tools aimed at the continuous grief and trauma after violence that is the South African experience in resource-poor communities (Benjamin & Crawford-Browne, 2010; Benjamin, 2011; Klass, 1999).
A literature review of social work in resource-poor communities found an absence of pre-emptive group-led responses to those living in a context of loss grief and trauma. Faced with overwhelming needs and legislative requirements as well as shortages of staff (Waters 2013; Dlamini & Sewpaul, 2015; Calitz, Roux & Strydom, 2014), social workers can only respond to crises and events within the demands of their job descriptions rather than pre-empt situations. This method of engaging with people in resource-poor communities offers social workers an alternative to time- and labour-intensive individual approaches.
A limitation of the study is that one cannot state with certainty that all the changes reported were directly related to attendance at the workshops. Several constraints affect attendance at such community workshops, including social, socio-political, economic and weather-related conditions. These contributed to the difficulty in arranging a suitable date and time for the evaluation event, thus there was an extended period between the group meetings and the evaluation. The custom of the majority of the participants to migrate to their ancestral family homes over a period spanning two months each year, when the summer school holidays and the Christmas and New Year national holidays coincide, lengthened the process. Despite this, the findings clearly demonstrated the impact the groups had on participants.
This study was limited to a specific context and comprised a single intervention over time. Findings cannot therefore be generalised. Further research should include replication of this workshop method with similar evaluation processes in different settings, with differing community groups. As most the participants were recruited through faith-based organisations, it cannot be assumed that their spiritual beliefs did not play a role and that the benefit of the workshop was due only to the intervention. Cross-cultural groups should also be run to evaluate the transferability of the approach.
CONCLUSION
For women whose daily existence is marked by recurring loss, grief and trauma, there is a need to create culturally acceptable interventions which facilitate coping skills and create the possibility of change. A group work approach with a structured supportive programme, experienced in the local setting which is safe and accessible, lends itself to changing of attitudes and ideas, and provides tools to manage their situation. This local setting for the group work event was deliberately aimed at engaging the participants in a shared experience as a community who would continue to live together after the workshop process concluded. The supportive network of family, friends and larger community in a context that is dangerous and re-traumatising is their main means of surviving. The power of the group was evident as it can generate a sense of safety and security to implement change in otherwise powerless individuals.
This approach to supporting persons who experience continuous trauma has the potential to reach a greater number of people who would not be able to obtain individual support and counselling. It has the potential for use by other members of the helping professions, such as the clergy and trained volunteer community counsellors.
ACKNOWLEDGEMENTS
Erica Greathead, 'Care for Kids' Programme Manager, The Warehouse Trust (NPO), Cape Town, South Africa.
Bev Meldrum, National Operations Manager, African Social Entrepreneurs Network, Cape Town, South Africa.
Gareth Mellon, Business analyst. The Warehouse Trust (NPO), Cape Town, South Africa.
REFERENCES
APPEL, D. & PAPAIKONOMOU, M. 2013. Narratives on death and bereavement from three South African cultures: an exploratory study. Journal of Psychology in Africa, 23 (3):453-458. [ Links ]
ASHFORTH, A. 2005. Witchcraft, violence, and democracy in South Africa. Chicago: University of Chicago Press. [ Links ]
ATWOLI, L., STEIN, D.J., WILLIAMS, D.R., MCLAUGHLIN, K.A., PETUKHOVA, M., KESSLER, R.C. & KOENEN, K.C. 2013. Trauma and posttraumatic stress disorder in South Africa: analysis from the South African Stress and Health Study. BMC Psychiatry, 13:1-12. [ Links ]
BENJAMIN, L. 2011. More than a drop in the ocean: breaking the cycle of violence. Cape Town: House of Colours. [ Links ]
BENJAMIN, L. & CRAWFORD-BROWNE, S. 2010. The psychological impact of continuous traumatic stress-limitations of existing diagnostic frameworks. Unpublished paper at a Continuous Traumatic Stress in South Africa Workshop: Department of Psychology, University of Cape Town. [ Links ]
BENORE, E.R. & PARK, C.L. 2004. Death-specific religious beliefs and bereavement: belief in an afterlife and continued attachment. The International Journal for the Psychology of Religion, 14:1-22. [ Links ]
BERZOFF, J. 2003. Psychodynamic theories in grief and bereavement. Smith College Studies in Social Work, 73(3):273-298. [ Links ]
BONANNO, G. A. 2004. Loss, trauma, and human resilience: have we underestimated the human capacity to thrive after extremely aversive events? American Psychologist, 59:20. [ Links ]
BOWLBY, J. 2005. A secure base: clinical applications of attachment theory. London: Taylor & Francis. [ Links ]
BREEN, L.J. & O'CONNOR, M. 2007. The fundamental paradox in the grief literature: a critical reflection. OMEGA-Journal of Death and Dying, 55, 199-218. [ Links ]
BROWN, A.C., BRODY, G.H. & STONEMAN, Z. 2000. Rural Black women and depression: a contextual analysis. Journal of Marriage and Family, 62(1):187-198. [ Links ]
CALITZ, T. ROUX, A. & STRYDOM, H. 2014. Factors that affect social workers' job satisfaction, stress and burnout. Social Work/Maatskaplike Werk, 50(2):153-169. [ Links ]
CHAPPLE, A., SWIFT, C. & ZIEBLAND, S. 2011. The role of spirituality and religion for those bereaved due to a traumatic death. Mortality, 16:1-19. [ Links ]
COPELAND-LINDER, N. 2006. Stress among Black women in a South African township: the protective role of religion. Journal of Community Psychology, 34:577-599. http://dx.doi.org/10.1002/jcop.20116 [ Links ]
DEMMER, C. 2007. Grief is a luxury: AIDS-related loss among the poor in South Africa. Illness, Crisis and Loss, 15(1):39-51. [ Links ]
DLAMINI,T.T-I. & SEWPAUL,V. 2015. Rhetoric versus reality in social work practice: political, neoliberal and new managerial influences. Social Work/Maatskaplike Werk, 51(4):467-481. [ Links ]
DRENTH, C., HERBST, A.G. & STRYDOM, H. 2010. A complicated grief intervention model. Health SA Gesondheid, 15(1): Art. #415. Doi:10.4102/hsag.v15i1.415. [ Links ]
D'SOUZA, S. 2000. Poverty among widows of Kinshasa, Congo. Journal of Health Population and Nutrition, 18:79-84. [ Links ]
DOZOIS, D.J. & COVIN, R. 2004. The Beck Depression Inventory-II (BDI-II), Beck Hopelessness Scale (BHS), and Beck Scale for Suicide Ideation (BSS). In: HILSENROTH, M.J. & SEGAL, D.L. (eds.) Comprehensive handbook of psychological assessment. Hoboken: John Wiley & Sons Inc. [ Links ]
EAGLE, G. 2015. Crime, fear and continuous traumatic stress in South Africa: what place social cohesion? Psychology in Society, 49:83-98. [ Links ]
EAGLE, G. & KAMINER, D. 2013. Continuous traumatic stress: expanding the lexicon of traumatic stress. Peace and Conflict: Journal of Peace Psychology, 19(2):85-99. [ Links ]
FIELD, N.P. 2006. Unresolved grief and continuing bonds: an attachment perspective. Death Studies, 30:739-756. [ Links ]
GILLIES, J. & NEIMEYER, R.A. 2006. Loss, grief, and the search for significance: toward a model of meaning reconstruction in bereavement. Journal of Constructivist Psychology, 19:31-65. [ Links ]
GOULD, C. 2014. Why is crime and violence so high in South Africa? News24.com, 18 September 2014. [Online] Available: http://www.news24.com/Columnists/GuestColumn/Why-is-crime-and-violence-so-high-in-South-Africa-20140918. [ Links ]
GRAY, M. & ALLEGRITTI, I. 2003. Towards culturally sensitive social work practice: re-examining cross-cultural social work. Social Work/Maatskaplike Werk, 39 (4): 312-325. [ Links ]
GRAY, M. & COATES, J. 2010. Indigenization and knowledge development: extending the debate. International Social Work, 53(5):1-15. [ Links ]
GRENARD, J.L. 2003. Associative group analysis: a review of the method developed by Lorand B. Sazala, South Carolina: University of South Carolina. [ Links ]
HALE, F. 1996. Akan funeral practices in Samuel Asare Konadu's Ordained by the Oracle. Journal for the Study of Religion, 9:21-40. [ Links ]
HUNT, J., ANDREW, G. & WEITZ, P. 2007. Improving support for bereaved people within their communities: updating the nine-cell bereavement tool. Bereavement Care, 26:26-29. [ Links ]
KAMINER, D., DU PLESSIS, B., HARDY, A., & BENJAMIN, A. 2013. Exposure to violence across multiple sites among young South African adolescents. Peace and Conflict: Journal of Peace Psychology, 19(2), 112-124. [ Links ]
KAMINER, D. & EAGLE, G. 2010. Traumatic Stress in South Africa. Johannesburg: Witwatersrand University Press. [ Links ]
KASIRAM, M. & PARTAB, R. 2002. Grieving through culture and community: a South African perspective. Social Work/Maatskaplike Werk, 38:(1) 39-44. [ Links ]
KEEN, C., MURRAY, C. & PAYNE, S. 2012. Sensing the presence of the deceased: a narrative review. Mental Health, Religion & Culture, 16(4):384-402. [ Links ]
KELLY, R.M. 1985. The associative group analysis method and evaluation research. Evaluation Review, 9(1):35-50. doi:10.1177/0193841x8500900103. [ Links ]
KLASS, D. 1999. Developing a cross-cultural model of grief: the state of the field. OMEGA-Journal of Death and Dying, 39:153-178. [ Links ]
KOTZÉ, E., ELS, L., & RAJUILI-MASILO, N. 2012. "Women . . . mourn and men Carry on": African women storying mourning practices: a South African example. Death Studies, 36(8):742-766. [ Links ]
LANCASTER, L. 2015. Where murder happens in South Africa. Africa Check. [Online] Available: https://africacheck.org/2015/10/07/where-murder-happens-in-south-africa/. [ Links ]
MAKHABA, V.L., MEMELA, N.C., & MAGOJO, T.S. 2009. (Grieving a community event) "Akwehlanga Lungehlanga": African mourning rites and rituals and their psychological significance. In: MKHIZE, M (ed). Rhythms of an African Psychology. Pretoria: Van Schaik. [ Links ]
MANYEDI, M. E., KOEN, M. & GREEFF, M. 2004. Experiences of widowhood and beliefs about the mourning process of the Batswana people: research. Health SA Gesondheid, 8:69-87. [ Links ]
MARSHALL, R. & SUTHERLAND, P. 2008. The social relations of bereavement in the Caribbean. OMEGA-Journal of Death and Dying, 57:21-34. [ Links ]
MELDRUM, B. & GREATHEAD, E. 2012. Evaluation of the Grief and Trauma Project (unpublished report). Cape Town: The Warehouse. [ Links ]
NEIMEYER, R. & ANDERSON, A. 2002. Meaning reconstruction theory. In: THOMPSON, N. (ed.) Loss and Grief. New York: Palgrave. [ Links ]
NEIMEYER, R. A., BALDWIN, S. A. & GILLIES, J. 2006. Continuing bonds and reconstructing meaning: mitigating complications in bereavement. Death Studies, 30:715-738. [ Links ]
NEMBAHE, M. 1998. An investigation of mourning amongst urban Zulus in relation to Worden's model of mourning. Johannesburg: University of the Witwatersrand. (M.A.thesis). [ Links ]
NWOYE, A. 2005. Memory healing processes and community intervention in grief work in Africa. Australian and New Zealand Journal of Family Therapy, 26:147-154. [ Links ]
OPPERMAN, B. & NOVELLO, A. 2006. The generation of hypotheses with regard to the influence of context on complicated grief. South African Journal of Psychology, 36:374-390. [ Links ]
PARKES, C.M. 1996. Bereavement: studies of grief in adult life. London: Routledge. [ Links ]
PEREIRA, B., ANDREW, G., PEDNEKAR, S., PAI, R., PELTO, P. & PATEL, V. 2007. The explanatory models of depression in low income countries: listening to women in India. Journal of Affective Disorders, 102:209-218. [ Links ]
RADZILANI, M.S. 2010. Discourse analysis on performance of bereavement rituals in a Tshivenda speaking Community. An African Christian and traditional African perspectives. Pretoria: University of Pretoria. (D Phil thesis). [ Links ]
RASHE, R. Z. 2008. Family violence in African communities in the Western Cape: a theological-ethical assessment. Stellenbosch: Stellenbosch University. (M thesis). [ Links ]
ROSENBLATT, P.C. & NKOSI, B.C. 2007. South African Zulu widows in a time of poverty and social change. Death Studies, 31:67-85. [ Links ]
ROTHAUPT, J.W. & BECKER, K. 2007. A literature review of Western bereavement theory: from decathecting to continuing bonds. The Family Journal, 15:6-15. [ Links ]
RYAN, S. B. 2006. Using associative group analysis methodology to explore unrecognized cultural background knowledge in cross-cultural communication research. Yamagata University Annual Research Report. Yamataga: Yamagata University. [ Links ]
SELEPE, M., & EDWARDS, S. 2008. Grief counselling in African indigenous churches: a case of the Zion Apostolic Church in Venda. Indilinga African Journal of Indigenous Knowledge Systems, 7(1):1-6. [ Links ]
SETSIBA, T.S. 2012. Mourning rituals and practices in contemporary South African townships. Empangeni: University of Zululand. (PhD thesis). [ Links ]
SHENTON, A. 2004. Strategies for ensuring trustworthiness in qualitative research projects. Education for Information, 22:61-75. [ Links ]
SNYMAN, S., VON PRESSENTIN, K.B., & CLARKE, M. 2015. International classification of Functioning, Disability and Health: Catalyst for interprofessional education and collaborative practice. Journal of Interprofessional Care, 29(4): 313-319. [ Links ]
SOMHLABA, N.Z. & WAIT, J.W. 2008. Psychological adjustment to conjugal bereavement: do social networks aid coping following spousal death? OMEGA-Journal of Death and Dying, 57:341-366. [ Links ]
SOMHLABA, N.Z. & WAIT, J. W. 2009. Stress, coping styles, and spousal bereavement: exploring patterns of grieving among Black widowed spouses in rural South Africa. Journal of Loss and Trauma, 14:196-210. [ Links ]
SOUTH AFRICAN POLICE SERVICE. 2013. Crime statistics 2012/2013. SAPS Annual statistical report. Pretoria: South African Police Service. [ Links ]
SOUTH AFRICAN POLICE SERVICE. 2015. Crime Situation in South Africa. Pretoria: South African Police Service. [Online] Available: http://www.saps.gov.za/resource_centre/publications/statistics/crimestats/2015/crime_stats.php. [ Links ]
STATISTICS SOUTH AFRICA. 2016. Mid-Year Estimates 2016. [Online] Available:http://www.statssa.gov.za/?p=8176http://www.statssa.gov.za/?p=8176http://www.statssa.gov.za/?p=8176. [ Links ]
STATISTICS SOUTH AFRICA. 2014. Victims of Crime Survey 2013/14. [Online] Available: https://www.statssa.gov.za/publications/P0341/P03412013.pdf. [ Links ]
STRAKER, G. 2013. Continuous traumatic stress: personal reflections 25 years on. Peace and Conflict: Journal of Peace Psychology, 19:209-217. [ Links ]
STROEBE, M. & SCHUT, H. 1999. The dual process model of coping with bereavement: rationale and description. Death Studies, 23:197-224. [ Links ]
STROEBE, M. 2001. Bereavement research and theory: retrospective and prospective. American Behavioral Scientist, 44:854-865. [ Links ]
STROEBE, M. S. 2008. Handbook of bereavement research and practice: advances in theory and intervention. New York: American Psychological Association. [ Links ]
WATERS, M. 2013. SA has a 77% social worker shortage. Politicsweb. [Online] Available: www.politicsweb.co.za/party/sa-has-a-77-social-worker-shortage--mike-waters. [ Links ]
WAYMENT, H.A. & VIERTHALER, J. 2002. Attachment style and bereavement reactions. Journal of Loss and Trauma, 7:129-149. [ Links ]
WEIERSTALL, R., HINSBERGER, M., KAMINER, D., HOLTZHAUSEN, L., MADIKANE, S., & ELBERT, T. 2013. Appetitive aggression and adaptation to a violent environment among youth offenders. Journal of Peace Psychology, 19(2): 138-149. [ Links ]
WEINGARTEN, K. 2003. Common shock: witnessing violence every day: how we are harmed, how we can heal. New York: Dutton/Penguin Books. [ Links ]
WEINGARTEN, K. 2010. Reasonable hope: construct, clinical applications, and supports. Family Process, 49:5-25. [ Links ]
WORDEN, J.W. 2003. Grief counselling and grief therapy: a handbook for the mental health professional. New York: Springer Publishing. [ Links ]
WORTMAN, C.B. & SILVER, R.C. 1989. The myths of coping with loss. Journal of Consulting and Clinical Psychology, 57:349. [ Links ]
YAWA, S.N. 2010. A Psycho-analysis of Bereavement in Xhosa, Zulu, Tswana cultures. Pretoria: University of Pretoria. (M thesis). [ Links ]


{kind=link}
{kind=link}
{kind=link}