










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.53 n.2 Stellenbosch 2017
http://dx.doi.org/10.15270/52-2-565
ARTICLES
Resilience amongst children living with HIV: Voices of foster parents residing in Bhambayi, Kwazulu-Natal, South Africa
Paida GomoI; Tanusha RanigaII; Siphiwe MotloungIII
IMs Paida Gomo, social work practitioner
IISchool of Social Work and Community Development, University of KwaZulu-Natal, Durban, South Africa. Ranigat@ukzn.ac.za
IIISchool of Social Work and Community Development, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
The resilience of children living with HIV and placed in foster care has been overlooked by the World Health Organisation, UNAIDS and UNICEF. Using qualitative methodology, this study explored the resilience of children living with HIV from the perspective of foster parents residing in a community in KwaZulu-Natal, South Africa. Using resilience theory, this paper presents three key themes, namely resilience and its link to disclosure, the need for care complements the need for cash, and family and community support systems. This paper makes suggestions for harnessing the undeniable contributions made by foster parents in enhancing the resilience of children living with HIV.
INTRODUCTION
There is empirical evidence that foster families have provided much care to, and enabled the resilience of, children living with HIV in their homes (Bali, 2003; De Jager, 2011; Freeman & Nkomo, 2006). South Africa has an unenviable estimated 3.7 million children who are orphaned, about half of whom have lost one or both parents to AIDS (World Health Organisation, 2013). Consequently the rapid expansion of foster care placements started in 2003 and the National Department of Social Development encouraged family members who were caring for orphaned children to apply for foster care grants (Raniga & Simpson, 2011). Foster care has become a viable option for alternative care for children living with HIV and in 2014 the South African Social Security Agency (SASSA) data revealed that 430 357 children were placed in court-ordered foster care and that 80 per cent of these children were placed with their extended family (SASSA, 2013).
Meintjes and Hall (2012) stated that it is important to take note that unjust and discriminatory apartheid policies resulted in high levels of social dislocation, sexual abuse, neglect and extreme marginalisation of children living with HIV. The Eastern Cape, KwaZulu-Natal, Limpopo and Mpumalanga are the four provinces in South Africa that had the highest number of orphaned children who were placed in foster care (Meintjes & Hall, 2012). The province of KwaZulu-Natal in particular had the highest number of children placed in foster care (SOCPEN, 2013). Foundational legislation such as the White Paper on Social Welfare (1997), the Children's Act 38 of 2005 as well as the National Development Plan Vision 2030 prioritise family and community-based care over institutional care. In addition, Meintjies and Hall (2012) add that the high HIV prevalence rates and the high mortality rates amongst parents has left many children orphaned in the province of KwaZulu-Natal. These researchers argue further that figures could be higher as those who are in informal foster care and not in receipt of the state foster care grant are excluded from these statistics (Meintjes & Hall, 2012).
In the post-1994 era it is important to take note that the economic and political crisis in South Africa has resulted in high poverty and unemployment rates, compounded by the breakdown of social and health infrastructures (Madhaven, 2004). There is also general acceptance that kinship and non-kinship families are severely constrained financially to absorb orphans, especially those children who are living with HIV. This paper provides researched evidence of the perspectives of foster parents to deepen understanding of the factors that contributed to resilience of children living with HIV and placed in foster care, as well as to understand the risk factors that may affect resilience of children living with HIV and placed in foster care. As such, the research questions guiding this study were:
-
What are the factors that contribute to resilience of children who are placed in foster care and living with HIV in Bhambayi?
-
What are the risk factors that may adversely affect resilience of children who were placed in foster care and living with HIV in Bhambayi?
RESILIENCE AND CHILDREN LIVING WITH HIV
For the purposes of this study, the authors adopted Ungar's (2008:218) definition of resilient people as as those who manage "to navigate their way to health-sustaining resources, including opportunities to experience feelings of well-being and conditions of the individual's family, community and culture to provide these health resources in culturally meaningful ways after one's exposure to significant adversity, whether psychological, environmental or both".
We argue that foster parent families tend to adapt positively and are able to cope with children who are living with HIV in their care based on their genuine love and care for the children, with the help of the state social grant support and socio-cultural resources, thus making the family unity stronger to cope during times of adversity. This conceptualisation of resilience appears to have synergy with other theories such as the strengths-based approach, asset-based community development and bonding social capital in that the focus is on promoting people's strengths and networks to overcome risk rather than eliminating risk (Zimmerman, 2013).
It is widely acknowledged in the literature that persons who are resilient demonstrate three core characteristics: a sense of self-esteem, self-efficacy and ability to solve problems. Self-esteem is explained by Cherry (2014:14) as "a person's overall sense of self-worth or personal value". It is important to note that children living with HIV and living in foster care face the double jeopardy of coping with their HIV status and having their perceptions of the world greatly influenced by how their peers, family members and social service professionals hold about persons living with HIV. Self-efficacy is explained by Bandura (2006:307) as "a person's beliefs about their capabilities to produce designated levels of performance that exercise influence over events that affect their lives". It was important to acknowledge that their past family backgrounds as well as their current foster family experiences were important factors to consider in understanding the children's resilience. One does need to be mindful that this does not imply that foster families are expected to adapt and fit into the status quo and to structural systems that are beyond their control. But for the children in this study the potential for personal and relational transformation can be forged out of adversity.
Masten (2001) distinguished three types of resiliency outcomes: positive outcomes despite high-risk environments, competent functioning in the face of acute or chronic life stresses, and recovery from trauma. This typology has been useful as it suggests that resilience is more than an absence of one's internal locus of control and, instead, embraces the strengths, assets and competencies of all family members in the household. Therefore when conducting the interview and focus group session with the foster parents, it was important for the authors to be conscious of the personal characteristics of the child, the family cohesion and availability of external support systems that contributed to the resilience of the child living with HIV. This study addressed an empirical gap in the literature by providing foster parents caring for children living with HIV from one predominantly informal settlement, North of Durban in KwaZulu-Natal, South Africa with the opportunity to dialogue and provide insight into their coping and resilient experiences.
RESEARCH METHODOLOGY
The research setting
Bhambayi is a mixed formal/informal settlement located in the Inanda region, 35 km north of the Durban city centre. While the majority of residents have lived in the area for more than 30 years, the past decade has seen an influx of people from the Eastern Cape and neighbouring African countries such as Mozambique, Zimbabwe, Congo and more recently also from Somalia. This in-migration has contributed to deeper levels of poverty and unemployment in the community. Residents' access to basic services such as water, sanitation and electricity has improved in the past five years. The Inanda Department of Social Development social workers visit the community weekly and the Provincial Department of Health operates a mobile clinic weekly on a Monday. There are many community-based organisations that provide early childhood educare services to toddlers and pre-school children, and the Siyazama support group provides psycho-social services to the elderly in the community. The Department of Social Work, UKZN students and academics have for the past 18 years provided social work services to residents in Bhambayi. The majority of the residents in Bhambayi speak isiZulu.
Design
A qualitative methodology underpinned this study, which utilised a descriptive design to guide the research process. Terre Blanche, Durrheim and Painter (2006) state that this design enables researchers to produce subjective data that are rich descriptions produced by the participants. This approach afforded foster parents the opportunity to speak authoritatively about resilience amongst children living with HIV in Bhambayi, KwaZulu-Natal.
Selecting the participants
As applicable to qualitative methodology, the researchers employed non-probability, purposive sampling to select the foster parents of children living with HIV from the community. The researchers networked with the Bhambayi Settlement Project, which operates under the auspices of the Inanda Department of Social Development office in order to access the intake register of those families who were affected by HIV and AIDS and were receiving psycho-social and material support from this Project. A letter detailing the research purpose and process was given to the Site Facilitator and several meetings were held with the Site Facilitator for the purposes of identification of participants from the Project's case records. As stated by Marlow (2011), convenience sampling comprises selecting the participants from a context where they are easily available and accessible. The criteria for inclusion of foster parents in the sample for the study were as follows:
-
Children were placed in foster care as per the South African Children Act 38 of 2005 for at least two years;
-
the children were diagnosed with HIV;
-
the foster parents were in receipt of at least one state social grant; and
-
the foster families were recipients of psycho-social and material services provided by the Bhambayi Settlement Project.
Terre Blanche et al. (2006) maintain that a specified sample size cannot be pre-determined at the outset of the data-collection process; instead the sample will be complete when the information collected becomes saturated or repetitive. Bearing this in mind, the researchers obtained the details of 14 foster parents from the case registers and then made contact with them by means of individual interviews. The study received ethical approval from the UKZN Research Ethics Committee in June 2015 and ethical issues such as confidentiality, recording and reporting of the data were discussed and clarified (Marlow, 2011). The researchers took into consideration Walker's (2012) assertion that data saturation is reached when adequate information is obtained from the participants and no new information is obtained to answer the research questions. As such, the final sample consisted of 14 foster parents and permission was sought from the children to interview the foster parents.
Data-collection methods
Data were collected from the 14 foster parents by means of one semi-structured interview and one focus group session. The advantage of the interview was that both the researchers had well established relationships in the community and this prolonged engagement enhanced the trustworthiness of the data (Marlow, 2011). The interview schedule and the focus group guide comprised mainly open-ended questions which were aligned to the underlying objectives of the study. Trustworthiness was further ensured by tape-recording the interview and focus group session as well as by peer debriefing as both researchers met weekly to discuss the transcripts of the data (Marlow, 2011). Additionally, the use of triangulation of two data-collection sources (interview and focus group) contributed to authenticate research findings and increased the trustworthiness of the study (Terre Blanche et al., 2006).
A major challenge experienced was that some of the interviews took more than a day to complete as the researchers had to allow the respondents' time to recover from their emotional state, because some questions were sensitive and related to the children's experiences of living with HIV. The findings from this study cannot be generalised to households across the country, but pertain mainly to the experiences of a group of African foster parents who were caring for children infected with HIV in a predominantly informal settlement in one province in South Africa. Data were distilled by categorising the rich narratives of the foster parents into relevant themes and bearing in mind a number of key assumptions and theoretical frames of reference, outlined below.
The resilience and coping strategies of children living in foster care may be overlooked when planning treatment, care and support services in spite of intentions by international and national policy makers to do so, because of a powerful and complicated socio-economic community context. This assumption has relevance for social work practitioners as it is important to acknowledge that despite this sub-group of children suffering from a significant traumatic health condition and foster parents caring for the children in a context of high poverty and extreme deprivation, the ability to rise above such adversity and respond with resilience to these risks formed the backdrop for this study (Truffino, 2010). Masten, Best and Garmezy (1990) point out that studies on children's resilience illustrated three variables that operate as protective factors. These factors encompass intrapersonal qualities of the children, the family's characteristics and the broader socio-cultural context (Schoon & Parsons, 2002). Theron, Theron and Malindi (2013) state from their qualitative study undertaken in a rural South African community on the views of Basotho youth that there is lack of understanding of resilience within an African context. This study was an attempt to address this empirical gap and to understand the resilience factors of children living with HIV who were placed in foster care and residing in an impoverished community in KwaZulu-Natal, South Africa.
Three important themes emerged from the data analysis which form the central premise of the results and discussion below: resilience and the link to disclosure, the need for care complements the need for cash, and family and community support systems. In the interpretation of the findings the researchers were mindful that understanding the foster parents' roles as caregivers necessitates an understanding of the complex interplay of socio-economic forces that profoundly impact on the children's resilience and how they cope in their lives (Theron & Malindi, 2010).
DISCUSSION OF RESULTS
The findings presented emerged from the analysis of 14 individual semi-structured interviews and one focus group session conducted with foster parents caring for children living with HIV as well as from field notes and meetings between researchers on the analysed data. The discussion on the findings will be presented in two sections:
-
A biographical profile of foster parents and their relationship to the child living with HIV;
-
A discussion of three inter-connected themes, namely resilience and the link to disclosure, the need for care complements the need for cash, and family and community support systems.
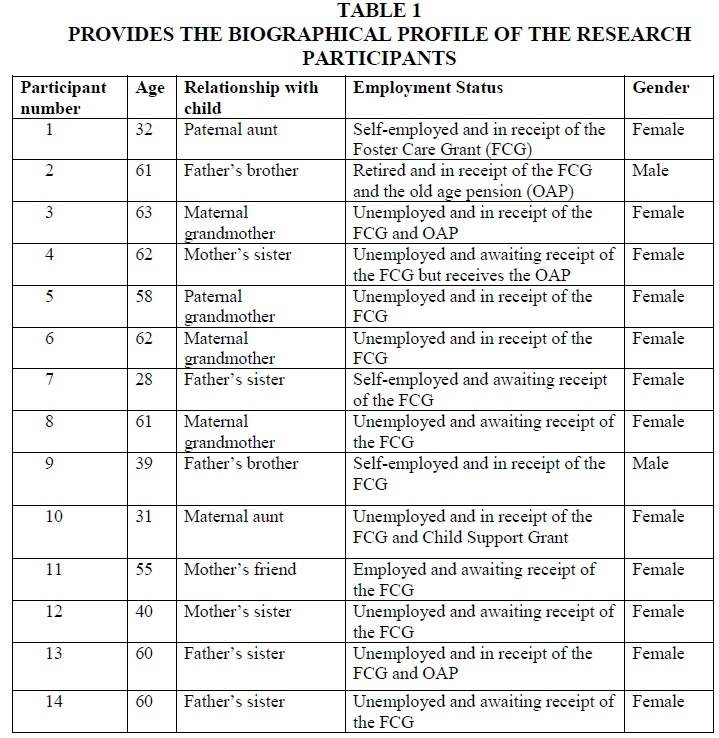
Three of the participants were aged 28 to 35 years, while two were between 36 and 40, two were over 50 and seven were over 60 (N=14). Table 1 also reveals that 12 of the foster parents were female and two were male. Consistent with qualitative research with elderly caregivers in rural Uganda undertaken by Ssengonzi (2009), gender inequalities are particularly acute in the era of HIV caregiving where older women take on parenting responsibilities at a time of their lives when their own physical strength and health are fragile and with consequences for their own personal finances. Raniga and Simpson (2010) and Akintola (2008) argue that in the post-apartheid era, the status of African women in South Africa has not changed as they make up the majority of foster parents who bear the brunt of caring for children infected with HIV at home. It is not surprising that 9 (64%) of the participants were unemployed, while one was employed, two were self-employed and one was retired. Eight of the participants were in receipt of the state foster care grant of R850 (US$65) at the time of the study and 7 had made the application to SASSA for the foster care grant and were awaiting the payment of the grant.
It is also important to note that one of the 14 foster parents was a non-kinship carer. She was a friend of the child's late mother. In South Africa kinship foster care has always been and continues to be a crucial safety net integrated in African family systems (Perumal & Kasiram, 2008). However, Perumal and Kasiram (2008) also warn that given the steady decline in traditional family living as a result of high levels of HIV and AIDS, poverty and unemployment in South Africa, the dominant view of family care being prioritised may not always be a feasible option. As a result, Perumal and Kasiram (2008) suggest that even though the dominant social construction of the family is significant in the life of a vulnerable child, there needs to be less emphasis on kinship care and more emphasis on significant others or non-kinship care to absorb children living with HIV. At the same time, Matthias and Zaal (2009) argue that having a community member volunteering to take care of an orphan gives hope to the ideology of adopting a developmental approach that promotes family and community-based care of children and that this is in accord with African values that states in isiZulu "umuntu ngumuntu ngabantu", which espouses the value of ubuntu and literally translates as "A person is a person because of others around him/her".
RESILIENCE AND THE LINK TO DISCLOSURE
All the respondents in this study were of the view that disclosing the diagnosis of HIV to a child residing in foster care is a controversial and emotionally charged issue (Wiener, Mellins, Marhefka & Battles, 2007). The literature identifies three main patterns of disclosure, namely full disclosure, non-disclosure and partial disclosure. Full disclosure entails open communication with the child by the primary caregiver about the potentially life-threatening illness of the child (Mavangira & Raniga, 2015). Non-disclosure means that there is no mention of HIV or any illness in the child's early years (Wiener et al., 2007). Partial disclosure is explained by Melvin (1999) as parents and/or the primary caregiver deliberately withholding significant information from the child about their illness for fear that such information may create distress for the child. The primary motive here is to protect the child's emotional wellbeing. Funck-Brentano (1995) argued that this partial disclosure can be termed illness deception. In this study some of the foster parents spoke about non-disclosure as they were of the view that the children placed in their care were not old enough to understand the HIV diagnosis and that it would traumatise them emotionally should they learn about their status. These foster parents believed that the non-disclosure protected the children and facilitated resilience in all areas of the child's life. Below are some comments shared by the foster parents.
"I feared to tell her because she had experienced her mother's death at first hand and how she suffered then being told that she has a virus that will kill her, would depress her or make her suicidal." (Participant 11)
"…this was in 2011; she was only 11 years so now I was so worried and disturbed because I thought that she was still very young to understand what the problem with her was." (Participant 14)
"I have a problem; I don't know how to tell him about his status. I am waiting for the child to grow up a little bit more maybe until when he has to go and get pills on his own." (Participant 7)
These responses also corroborate the findings of a study undertaken by Mahloko and Madiba (2012) with 90 caregivers who indicated that they had not disclosed the HIV diagnosis to children in their care as they believed that the children were too young to understand the HIV diagnosis. These foster parents were also of the view that this non-disclosure contributed to the children's resilience as they believed that by protecting the children from full disclosure of their HIV status the children were able to cope and were able to deal emotionally with treatment adherence and safety precautions.
It was also evident from the focus group session that six of the 14 (42%) foster parents reported to have fully disclosed the HIV status to the child as the children frequently questioned the purpose of the medication that they were to take on a daily basis. These foster parents were of the view that full disclosure assisted with treatment adherence and positive psychological wellbeing and enhanced resilience of the children to cope with their HIV status. These are some of the comments made by the foster parents.
"I did not immediately tell the child that she was positive, I only told her after she had asked why she was taking the pills and I told her that her mum was positive and that is how she also contracted the virus through birth." (Participant 8)
"I would give the child some pills but she would go and throw them away then I noticed that her body was becoming weak and pale then I sat with the child and told her that she had to take her medication seriously because she was HIV positive." (Participant 2)
"I said to my child today: you found out that you are positive and the fact that your mother was sick, you contracted the virus from your mother. You should not be scared about being positive because I am also taking the pills." (Participant 5)
"She would throw away the pills so I just said to her, listen, if you stop taking these pills; it's going to affect your life. You are HIV positive and it is a virus that causes headaches and stomach pains." (Participant 3)
The responses above corroborate the results of a study undertaken by Kallem, Renner, Ghebremichael and Paintsil (2011) with 71 caregiver-child dyads from the Paediatric HIV/AIDS Care Program in Accra, Ghana. The children in this study were between the ages of eight to 14 years. The findings revealed that nearly 50% of the caregivers who had disclosed had stated that medication adherence was a driving force. The foster parents in this study were of the view that once full disclosure was made, the child was able to embrace their HIV status and this did result in improved treatment adherence and resilience to cope in their daily lives (Kallem et al., 2011).
The above findings illustrates the complex dilemmas faced by foster parents regarding disclosure of the HIV status to the child placed in their care. A qualitative study by Vreeman, Nyandiko, Ayaya, Walumbe, Marrero and Inui (2010) in Western Kenya revealed the same dilemma faced by caregivers of HIV-infected children. They perceived disclosure of the child's status as a positive move for older children as they would adhere to antiretroviral treatment and enhance the social support that they received. The same study however, also found that some respondents believed that disclosure was harmful to the child's emotional health and could possibly result in discrimination and stigmatisation for the family as a whole.
In this study the views shared by those foster parents who chose not to disclose to their children regarding their HIV status were of the view that this enhanced resilience within the child, as the child did not show any distress because they were not aware of their vulnerability and they did not have additional emotional baggage to worry about. It was also interesting, however, that those children who were told about their HIV positive status as illustrated in the sentiments shared above showed signs of distress and had their psychological balance disturbed. After having their HIV-positive status disclosed to them, the children still had to cope with the disclosure news as well as their arduous life circumstances. The foster parents deemed these children resilient because after the children knew about their HIV positive status, they continued to live their normal lives by taking part in social activities, pursing their academic work and even being motivated to live a positive and fulfilling life. This line of thought conforms to Ungar (2008) conceptualisation of resilience that when an individual manages to navigate their way to health-sustaining resources after one's exposure to significant adversity, intra-personal traits, family support and community influences are protective factors that these children use to cope with multiple agonies. The foster parents in this study also stated that material resources had helped the family unit to survive in harsh economic times. The theme below is a discussion on how the need for care complements the need for cash.
The need for care complements the need for cash
Child fostering has historically played a crucial role in African family life. However, in times of economic hardship, the contemporary debates have shifted to questioning the motive that foster parents have had in respect of the need for care versus the need for cash (Kasiram & Pillay, 2008; Madhaven, 2004). The foster parents in this study stated that benefiting from at least one state social grant was an important factor that contributed to the resilience of the children in their care.
The following are some comments shared by the foster parents
"He is my late daughter's son. The mother died when he was 3 years old and the father is not known, so I had to take care of him. I do not receive the FCG because the mother died without leaving any of the child's documents and I do not even know what to do about in. I just use my old age grant, God provides. You see she doesn't know any other mother except me the gogo (she laughs). I really desire that he has a future, my Lord and not just being a child without any direction." (Participant 4)
"You see I am old now. Look at the place we stay in. It is not ideal for a child living with HIV to be living in. When it rains, the water enters and spoils the clothes. I am all alone and what will happen to my son if I die? (There was a moment of silence because the participant was becoming emotional but she continued.) I have nothing to give him that he can continue to live a better life. The FCG helps to buy his clothes, food and school shoes." (Participant 3)
"Yes I get the foster care grant and it greatly helps with the uniforms for the child and his medication but I also have my worries about the child's future that have nothing to do with the money. Sometimes I just think about it and ask myself if he will find someone who will want to marry him with his status. I would want him to start a family one day but uuuum, I don't know." (Participant 9)
The voices of the foster parents reflect the genuine love and care that the foster parents expressed for their foster children. More so, the economic support received through the receipt of the state social grants helped to meet the material needs of the child such as nutritious food, school clothing and medication. The foster parents were also of the view that this material resource provided safety and stability for the child and helped the family stay hopeful and positive in times of adversity. The comments shared by the foster parents in this study corroborate the important finding by Hearle and Ruwanpura (2009) that even though many carers are living under materially deprived circumstances in KwaZulu-Natal, the beneficiaries of the foster care grant were not motivated by monetary incentives to care for orphaned children in the province and that children who were voluntarily fostered did not suffer any material and nutritional disadvantages. Madhaven (2004) suggests that the security that a child in foster care receives often reflects the nature of the relationship between foster and biological parents. The findings illustrated in Table 1 reveals that all the children shared kinship relations with the foster parents and this implies that there was a genuine love and care as well as interest in the child's wellbeing. The role of family and community networks was also explored as contributing factors to the resilience of children living with HIV. This theme is explored further below.
Family and community networks
During the focus group discussion the foster parents indicated that extended family, NGOs and other faith-based organisations played an important role in providing material assistance and psycho-social support to the children. These community support networks assisted the children to deal with unresolved grief and overcome psycho-social challenges. It is fortunate that Bhambayi has a number of government and community-based organisations that provide social work and health services to the residents of the community. Theron and Malindi (2010) explain that communities with strong social capital have a variety of strategies that avoid or minimise multiple or chronic risks for children and thus are able to improve the care and protection of children. Foster parents expressed how these community organisations helped to enhance the resilience of the children in their care.
"We have community care givers who do home visits to check on the wellbeing of the child. Sometimes the child feels that she is a bit mature to get help from them but she contacts them when she needs help." (Participant 9)
"This community has child and youth care workers who monitor the children's progress and they support a lot with home works and just advice to the children." (Participant 10)
"The lady from church also plays a motherly role figure, so it helps a lot with her self-esteem. In the community we also have youth care workers who help children living with HIV." (Participant 14)
Theron and Malindi (2010) add that resilience goes beyond self-efficacy and self-esteem, but rather entails a dynamic interaction with one's family and community systems. The majority of the participants spoke about being grateful for the various health and social service professionals who visited weekly to assist children in building relationships with other children in their local community and who provided psycho-social support for children. This finding corroborates the findings of a study undertaken in rural China with 195 HIV-infected children, who were also diagnosed with depression, that social networks and support systems in communities correlates with higher levels of resilience amongst children (Mo, Lau, Yu & Gu, 2014).
An interesting finding of this study was that one of the mechanisms used by the children to cope with psycho-social stresses was the reassurance that the children received from those foster parents who were also diagnosed with HIV. Participants 1, 9 and 12 stated that this played a major role in comforting the children and motivating them that they could also live a long and healthy life. Below are sentiments shared by these foster parents.
"I even told the child that I am also positive and taking pills but I have grown to be a gogo, so you can also grow to be a gogo." (Participant 12)
"I try to support the child by talking to her and reminding her that I am always there for her. I even tell the child that I am also positive and taking the pills." (Participant 1)
"I tell him that he is going to grow old and become very successful because he is a strong boy. I even tell him that he is the next Nelson Mandela and that he just needs to work hard, finish his school, because Mandela went to school and finished his school." (Participant 9)
This is significant as Truffino (2010) contends that the way in which the children living with HIV perceive their family caregiver impacts on their own resilience. In this sense the resilience of the children living with HIV and coping with AIDS-related stress is closely linked to the quality of care and perceptions of their foster parents (Madhaven, 2004). Many of the foster parents, however, mentioned the need for ongoing training and support services from social workers and health professionals to help them to deal with the psycho-social needs and demands of the children in their care. Attention must also be given to the economic demands of caregiving as this is a key contributing factor to the stresses and poor life satisfaction of family caregivers caring for persons with AIDS (Raniga & Motloung, 2013).
RECOMMENDATIONS AND CONCLUSION
Evidence from this study has revealed that foster parents continue to play a significant role in enhancing resilience amongst children living with HIV and placed in foster care. The key research question that guided the study was: How do children living with HIV and in dire poverty as well as who are placed in foster care develop resilience Inspired by resilience theory, this study highlighted that there were three main protective factors that the children used to cope despite living in a high-risk environment: intra-personal traits, family and community influences, and state social grants. Consistent with other empirical evidence, this confirms gaps in ongoing psycho-social and support networks required by foster parents caring for children living with HIV (Madhaven, 2004; Mavangira & Raniga, 2015).
The findings also highlight the importance of social work interventions that are required to manage disclosure to help foster parents to deal with the emotional turmoil presented by children living with HIV. In particular, this study corroborates the suggestion made by Mavangira and Raniga (2015) that user-friendly health services will enhance adherence to ARV treatment and promote ongoing supportive services for foster parents and the children living with HIV in their care. The following recommendations should be considered for implementation:
-
Strengthening partnerships between NGOs and the Department of Social Development social workers to establish support network forums for foster parents caring for children living with HIV in communities;
-
It is imperative that social workers lobby for funding to supplement the income received from the foster care grant;
-
Media campaigns to create public awareness and to de-stigmatise HIV will enhance the resilience of children living with HIV and placed in foster care.
This study represented a limited sample of 14 African foster parents caring for children living with HIV in one province in South Africa and does not represent a mix-race profile of foster families across different provinces in the country.
REFERENCES
AKINTOLA, O. 2008. Unpaid HIV/AIDS care in Southern Africa: forms, context, and implication. Feminist Economics, 14(4):117-148. [ Links ]
BALI, D.N. 2003. The role of informal carers for HIV/AIDS patients in high prevalence sub-Saharan African countries. Department of International Health, Liverpool School of Tropical Medicine, Liverpool, United Kingdom. (MA thesis) [ Links ]
BANDURA, A. 1994. Self-efficacy. In: RAMACHANDRAN, V.S. 1994. Encyclopedia of Human Behaviour. New York: Academic Press. [ Links ]
CHERRY, K. 2014. What is self-esteem? [Online] Available: http://psychology.about.com/od/sindex/f/what-is-self-esteem.htm. [Accessed: 18/06/2015]. [ Links ]
DE JAGER, E. 2011. Foster care of aids orphans: social workers' perspectives. Stellenbosch: University of Stellenbosch, South Africa. (MA Thesis) [ Links ]
DEPARTMENT OF SOCIAL DEVELOPMENT. 1997. White Paper for Social Welfare. Pretoria: Government Printers. [ Links ]
FREEMAN, M. & NKOMO, N. 2006. Guardian of orphans and vulnerable children. A survey of current and prospective care givers. Journal of AIDS Care, 18(4):302-310. [ Links ]
FUNCK-BRENTANO, I. 1995. Informing a child about his illness in HIV infection: words and meaning. Psychiatry Enfant, 38(1):109-139. [ Links ]
HEARLE, C. & RUWANPURA, K.N. 2009. Contentious care: foster care grants and the caregiver orphan relationship in KwaZulu-Natal Province, South Africa. Oxford Development Studies, 37(4):423-437. [ Links ]
HOSEGOOD, V., KIMOU, L., MADHAVAN, S., MATHAMBO, V. & WAKHWEYA, A. 2009. Strengthening families to support children affected by HIV and AIDS. AIDS Care, 21(1):3-12. [ Links ]
KALLEM, S., RENNER, L., GHEBREMICHAEL, M. & PAINTSIL, E. 2011. Prevalence and pattern of disclosure of HIV status in HIV-infected children in Ghana. AIDS Behavior, 15:1121-1127. [ Links ]
MADHAVEN, S. 2004. Fosterage patterns in the age of AIDS: continuity and change. Social Science & Medicine, 58:1443-1454. [ Links ]
MAHLOKO, J. & MADIBA, S. 2012. Disclosing HIV diagnosis to children in Odi district, South Africa: reasons for disclosure and non-disclosure. African Journal of Primary Health Care & Family Medicine, North America. [Online] Available: http://www.phcfm.org/index.php/phcfm/article/view/345/451. [Accessed: 22/12/2015]. [ Links ]
MARLOW, C. 2011. Research methods for generalist social work. Belmont, CA: Thomson Brooks/Cole. [ Links ]
MASTEN, A., BEST, K., & GARMEZY, N. 1990. Resilience and development: contributions from the study of children who overcome adversity. Development and Psychopathology, 2:425-444. [ Links ]
MASTEN, A.S. 2001. Ordinary magic: resilience processes in development. American Psychologists, 56(3):227-238. [ Links ]
MATTHIAS, C. & ZAAL, N. 2009. The child in need of care and protection. In: BOEZAART, T. (ed), Child Law in South Africa. Cape Town: Juta Publishers. [ Links ]
MAVANGIRA, V. & RANIGA, T. 2015. Psycho-social experiences of perinatally HIV-infected adolescents residing in child and youth care centres in South Africa. Social Work/Maatskaplike Werk, 51(3):311-323. [ Links ]
MEINTJES, H. & HALL, K. 2012. Demography of South Africa's children. Child Gauge. Children's Institute. Cape Town: University of Cape Town, 82-85. [ Links ]
MELVIN, D. 1999. Psychological issues, challenges and achievements. Journal of HIV Therapy, 4(3):77-81. [ Links ]
MO, P.K.H., LAU, J.T.F., YU, X. & GU, J. 2014. The role of social support on resilience, posttraumatic growth, hopelessness and depression among children of HIV-infected parents in mainland China. AIDS Care, 26(12):1526-1533. [ Links ]
PERUMAL, N. & KASIRAM, N. 2008. Children's homes and foster care: challenging dominant discourses in South African Social Work practice. Social Work/Maatskaplike Werk, 44(2):159-169. [ Links ]
RANIGA, T. & SIMPSON, B. 2011. Poverty, HIV/AIDS and the old age pension: an analysis of older persons in Bhambayi, KwaZulu-Natal, South Africa. Development Southern Africa, 28(1):75-85. [ Links ]
RANIGA, T. & MOTLOUNG, S. 2013. The economic and psycho-social experiences and coping resources of family members caring for people living with AIDS in their homes in Bhambayi, KwaZulu-Natal, South Africa. Social Work/Maatskaplike Werk, 49(1):1-15. [ Links ]
SCHOON, I. & PARSONS, S. 2002. Competence in the face of adversity: the influence of early family environment and long-term consequences. Children and Society, 16(4):260-276. [ Links ]
SOUTH AFRICAN SOCIAL SECURITY AGENCY. 2013. SASSA Statistical Report. [Online] Available: http://www.sassa.gov.za/index.php/knowledge-centre/statistical-reports. [ Links ]
SSENGONZI, R. 2009. The impact of HIV/AIDS on the living arrangements and well-being of elderly caregivers in rural Uganda. AIDS Care, 21(3):309-314. [ Links ]
TERRE BLANCHE, M., DURRHEIM, K. & PAINTER, D. 2006. Research in practice: applied methods for social sciences. Cape Town: University of Cape Town Press. [ Links ]
THERON, L.C. & MALINDI, M.J. 2010. Resilient street youth: a qualitative South African study. Journal of Youth Studies, 13(6):717-736. [ Links ]
THERON, L.C., THERON, A.M.C. & MALINDI, M.J. 2013. Toward an African definition of resilience: a rural South African community's view of resilient Basotho Youth. Journal of Black Psychology, 39(1):63-87. [ Links ]
TRUFFINO, C.J. 2010. Resilience: an approach to the concept. Rev Psiquiatr Salud Ment (Barc), 3(4):145-151. [ Links ]
UNGAR, M. 2008. Resilience across cultures. British Journal of Social Work, 38:218-235. [ Links ]
UNGAR, M., BROWN, M., LIEBENBERG, L., OTHMAN, R., KWONG, W.M., ARMSTRONG, M. & GILGUN, J. 2007. Unique pathways to resilience across cultures. Adolescence, 42(166):287-310. [ Links ]
VREEMAN, R.C., NYANDIKO, W.M., AYAYA, S.O., WALUMBE, E.G., MARRERO, D.G. & INUI, T. 2010. The perceived impact of disclosure of pediatric HIV status on pediatric antiretroviral therapy adherence, child well-being and social relationships in a resource-limited setting. AIDS Patient Care, 24(10):639-649. [ Links ]
WALKER, J.L. 2012. The use of saturation in qualitative research. Canadian Journal of Cardiovascular Nursing, 22(2):37-46. [ Links ]
WIENER, L., MELLINS, C.A., MARHEFKA, S. & BATTLES, H.B. 2007. Disclosure of an HIV diagnosis to children: history, current research, and future directions. Journal of Development Behaviour Pediatric, 28:155-166. [ Links ]
WORLD HEALTH ORGANSIATION. 2013. Global HIV and AIDS Progress Report. Geneva: WHO Press. [ Links ]
ZIMMERMAN, M.A. 2013. Resiliency theory: a strengths-based approach to research and practice for adolescent health. Health, Education and Behaviour, 40(4):381-383. [ Links ]


{kind=link}