










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSocial Work
versão On-line ISSN 2312-7198
versão impressa ISSN 0037-8054
Social work (Stellenbosch. Online) vol.53 no.1 Stellenbosch 2017
http://dx.doi.org/10.15270/52-2-550
ARTICLES
"The man can use that power", "she got courage" and "inimba": discursive resources in counsellors' talk of intimate partner violence: implications for practice
Ms Annie FleischackI;.Prof Catriona Ida MacleodI ; Mr Werner BohmkeII
ICritical Studies in Sexualities and Reproduction, Rhodes University, Grahamstown. <afleischack@danville.co.za>
IIDepartment of Psychology, Rhodes University, Grahamstown, South Africa
ABSTRACT
Given the high rate of intimate partner violence (IPV), understanding how counsellors talk about IPV and their interventions is important. The authors conducted narrative interviews with eight counsellors from non-governmental organisations (NGOs) working with IPV. Using narrative-discursive methodology, this qualitative study paid attention to the discursive resources that the participants drew upon. Two broad clusters of discursive resources and one contradictory ('nurturing femininity') discourse emerged. The first cluster engenders a sense of helplessness in the face of overwhelming power relations; the second enables the counsellors to foresee positive outcomes for their counselling. Implications for counselling include emphasising enabling discourses, highlighting multiplicities of gender, and wider-scale interventions.
INTRODUCTION
South Africa is a violent society (Jewkes, Levin & Penn-Kekana, 2002), with violence often being used as a social resource to maintain, control and establish authority (Britton, 2006; Jewkes et al., 2002). Local research suggests that there is a high prevalence of intimate partner violence (IPV), a facet of this general violence (Joyner & Mash, 2011). Despite this, little research has been conducted on the understandings of, and social work and lay counselling interventions with regard to, IPV in the South African non-governmental organisation (NGO) context.
Various NGOs in South Africa have attempted to address IPV by providing services that aim to assist (mostly female) clients emotionally and logistically. It is acknowledged that NGOs play an important role in this regard through their counselling and empowerment programmes, legal support and shelter services (Britton, 2006; Kaldine, 2007). These facilities support and supplement state departments, in particular the Department of Social Development, in responding to IPV. NGOs in South Africa are often under-resourced and battle to provide services at the individual level, let alone to whole communities or families at a significant level (Rasool Bassadien & Hochfeld, 2005). It is, therefore, important for these counsellors to feel empowered in the counselling that they are able to provide, not only for the sake of the clients but also for the wellbeing of the counsellors themselves. In this paper we present results from a study of counsellors' narratives of their understanding of, and interventions concerning, IPV. These counsellors work in two NGOs, one located in an urban and another in a peri-urban area in the Eastern Cape province.
BACKGROUND
The prevalence of IPV: IPV is conceptualised in this study as sexual and physical violence within intimate partner relationships, with the understanding that these often go hand-in-hand with emotional and verbal abuse (Joyner et al., 2011) as well as economic abuse (Domestic Violence Act, No. 116 of 1998). South Africa has been identified as having one of the highest prevalence rates of IPV in the world (Britton, 2006; Joyner & Mash, 2011), with 19% of women experiencing a lifetime prevalence of victimisation (Seedat, Van Niekerk, Jewkes, Suffla & Ratele, 2009) and 27.5% of men reporting abusing their current or most recent partner (Gupta, Silverman, Hemenway, Acevedo-Garcia, Stein & Williams, 2008). IPV cuts across racial, education, employment and income-level lines (Modiba, Baliki, Mmalasa, Reineke & Nsiki, 2011).
The effects of IPV on women: Research has revealed many health and psychological consequences for women who experience IPV (Brownridge Taillieu, Tyler, Tiwari, Chan & Santos, 2011; Campbell, 2002). These include injuries, damage to the central nervous system, gastrointestinal symptoms and disorders, cardiac symptoms, gynaecological problems, depression, increased aggression, misuse of alcohol and drugs, and post-traumatic stress disorder. IPV during pregnancy, an aspect of IPV in general, is the second highest form of trauma during pregnancy, second only to motor vehicle accidents (Modiba et al., 2011). Studies from around the world reveal that IPV occurs in 2% to 13.5% of pregnancies (Devries, Kishor, Johnson, Stóckl, Bacchus, García-Moreno & Watts, 2010). In a study conducted in antenatal clinics in Gauteng province in SA, 41% of pregnant women who sought antenatal care were found to be victims of abuse (Modiba et al., 2011). These percentages are significant as IPV during pregnancy has damaging effects on both mother and child (Campbell, 2002; Jasinski, 2004).
Despite the high rate of IPV and its consequences, women face many barriers in reporting IPV, related to resource constraints and social issues. The resource-related barriers include the lack of availability of healthcare or service provision facilities in the first place (Mbokota & Moodley, 2004; Njuho & Davids, 2012), and lack of adequate assistance because of problematic interactions with the counsellors (Rasool Bassadien & Hockfeld, 2005). In terms of social issues, some women may not report abuse due to their conforming to conservative gender roles in which women defer to, rather than challenge, male authority, even when it includes violence (Jewkes et al., 2002).
IPV may thus be considered normal within relationships as a result of gender inequalities and women may blame themselves as a coping mechanism, or feel that their perpetrator did not harm them intentionally (Silverman, Raj & Clements, 2004). Women may also feel ashamed about reporting IPV because of the personal nature of the assault (Lewis, West, Bautista, Greenberg & Done-Perez, 2005), and may fear retaliation, or loss of the children (Hayden, 2010).
In some contexts, reporting IPV is discouraged as it is not considered socially acceptable to seek external help (Lee, Sanders Thompson & Mechanic, 2002). This may be a consequence of the social stigma that is attached to reporting violence, or to the cultural sanctioning of violence in some communities (Cokkinides, Coker, Sanderson, Addy & Bethea, 1999). Additionally, people may prefer to resolve issues of IPV by speaking to authorities or elders within their community (or a woman will speak to her mother-in-law) rather than seeking external support (Rasool et al., 2005). This is because the case has to be presented by the woman's family if it is to be heard in court, which is an unlikely occurrence (Rasool et al., 2005).
If women receive inadequate assistance when reporting IPV, or if there is a lack of service provision in the first place, women may develop strategies to cope with the IPV. Thus they would opt to remain in the relationship if they feel that they have no control over reducing or preventing their partner's violence towards them. Some women may remain in violent relationships because of fears that violence towards them may escalate if they make attempts to leave or because they fear retribution against their children (Rhodes & McKenzie, 1998).
IPV and counselling: Local and international research has shown that effective responses to IPV have many positive effects. These include women gaining confidence to leave a violent/abusive relationship as a result of being able to confide in counsellors or clinicians, and increased health and psychological wellbeing (Jewkes et al., 2002; Hatcher, Romito, Odero, Bukusi, Onon & Turan, 2013; Rhodes et al., 1998). Women who have access to, and utilise, the services of counselling centres are able to consider options for solving problems within the relationship, increase their emotional wellbeing and also develop an enhanced ability to physically remove themselves from the abuse (Iverson Stirman, Street, Gerber, Carpenter, Dichter, Bair-Merritt & Vogt, 2016; Rhodes et al., 1998).
However, counsellors and healthcare workers themselves may also be considered a barrier to reporting IPV. Even if women experiencing IPV are able to access service provision and healthcare, they may not receive the assistance that they need. Research into a Latino community in the USA revealed that counsellors sometimes did "not consider some potentially important personal barriers to reporting", such as the victim's shame, and were afraid to intervene on behalf of community members when dealing with IPV (Lewis et al., 2005:81). These barriers link to earlier work by Vogelman and Eagle (1991) which suggests that the victim may feel shame, for example, when reporting assault of a sexual nature. In terms of the South African healthcare sector, one of the main problems is the lack of acknowledgement of IPV altogether (Joyner & Mash, 2012). IPV is often not recognised by primary healthcare providers and, when it has been diagnosed, the treatment has often been badly coordinated, fragmented, has missed important aspects and has lacked continuity (Joyner et al., 2012). This may be a result of the lack of appropriate or sufficient training that healthcare providers receive globally (Watts & Mayhew, 2004) and locally (Mash, Fairall, Adejayan, Ikpefan, Kumari, Mathee, Okun & Yogolelo, 2012).
Various models of conducting counselling in relation to IPV have been suggested in the literature. For example, Miller, Veltkamp, Lane, Bilyeu and Elzie, (2002) present care pathway guidelines for IPV counselling. These guidelines delineate specific timelines in which assessment and intervention occur, how decision-making should be addressed, what clinical services should be considered and how interactions amongst counsellors should be managed. Mwau (2000) suggests using feminist principles in counselling: validating women's feelings, helping them explore options, educating them about the dynamics of IPV, acknowledging their strengths, and helping them cope with guilt or shame.
Research on the experiences of IPV counselling has been used to refine recommendations for the counselling encounter. For example, McHattie (2011) used the critical incident technique to investigate what women who had undergone counselling for IPV found helped or hindered the healing process. Three themes emerged: safety and trust; empowerment; and issues relating to shame. Safety and trust in the counselling relationship meant that the women felt comfortable enough to share their stories. Participants also identified the importance of empowerment, specifically having their agency supported, being able to accomplish certain tasks, having access to information and learning skills. Acceptance and validation were seen as assisting in overcoming the shame associated with IPV.
The discursive approach to understanding IPV counselling: In this particular study we take a discursive approach to understanding IPV counselling, focusing specifically on the discourses drawn on by counsellors in their talk about IPV and their interventions regarding IPV. 'Discourses', or 'discursive resources' are conceptualised as "practices which systematically form the objects of which they speak" (Foucault, 1972:49). That is, they are "broad patterns of talk - systems of statements - that are taken up in particular speeches and conversations" (Terre Blanche, Durrheim & Kelly, 2006:328) and are "the organised and regulated, as well as the regulating and constituting, functions of language" (Bove, 1990, in Jackson & Mazzei, 2012:50). Young and Collin (2004:379) suggest that discourses "are not single, unitary or bounded perspectives, but fairly fluid frames, that enable us to hold thoughts, discussion and action together in a way that is meaningful for a particular purpose at a particular time."
Discursive resources construct the object about which they talk, but also allow spaces for particular kinds of human subject (Parker, 1992). This is linked to the concept of subject positioning (see also Davies & Harré, 1990): the ways in which we situate ourselves and others when we speak about them (Gavey, 2011). Different discourses have different implications for what can be considered knowledge, and this in turn allows us a level of possibility for acting on the world (Burr, 2003). Discourses are simultaneously constitutive of, and constituted by, social practices. It is for this reason that we are interested in the discursive resources that counsellors draw on in their talk about IPV, as these will have implications in terms of how they proceed with the actual counselling encounter.
METHOD
In this qualitative study we sought to answer the following questions: How do counsellors in NGO contexts talk about their understandings of, and practices in response to, IPV? What discursive resources and subject positions do the counsellors draw upon in their narratives?
Data were collected through interviews with counsellors from two NGOs, one in an urban and the other in a peri-urban area in the Eastern Cape. We chose to collect data from two different sites for diversity. Both NGOs serve clients from lower socioeconomic circumstances. The services provided by the NGOs include women's empowerment; individual, couple and family counselling; working with the police and magistrate's court to process protection orders, maintenance and divorce orders; and referrals to safe houses.
Eight counsellors across the two sites (six at the urban site and two at the peri-urban site), all of whom are women, participated in the study. These were a sample of the population of counsellors at the NGOs who were willing and able to participate. All are experienced in counselling clients who have experienced IPV. One had university-level counselling qualifications and the seven others were lay counsellors who were qualified via in-house training. Both sites utilise a client-centred, solution-focused approach in which the clients choose their way forward from a variety of options presented by the counsellors. Some counsellors had been abused by their partners and could be viewed as 'wounded healers' and thus it appeared that they had an empathetic investment in their clients' wellbeing.
The study received ethical clearance from the university's Psychology Department and permission to conduct the research from the two sites was obtained. Participants were assured that the interviewers would not ask them directly personal questions. Informed consent was obtained from each participant, including their permission to audio-tape the interviews. Pseudonyms are used for the participants, and the location and names of the NGOs kept non-specific.
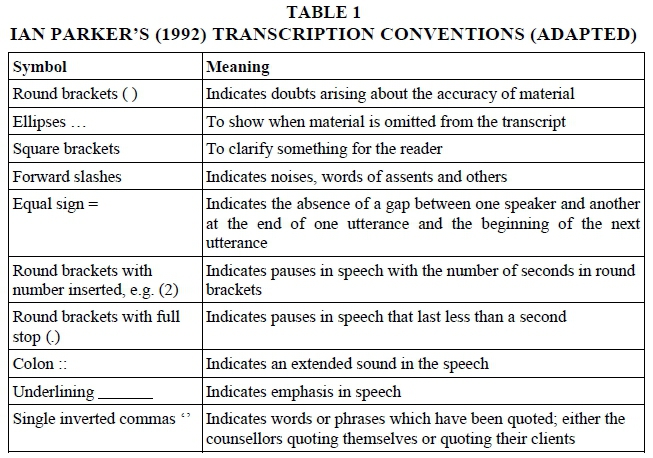
Data were collected through a series of three interviews, using Wengrafs (2001) Lightly-Structured Interview Schedule. The first author and a co-researcher conducted the interviews. The co-researcher took notes during the interviews, focusing on the topics that arose in the counsellors' narratives. In the initial session counsellors were asked to narrate their understandings of, and experiences in conducting counselling with respect to, IPV during pregnancy. The two researchers then constructed interview questions based on topics that arose in their narratives, which were asked in session 2, which took place 15 minutes after session 1. Session 3 was conducted two months later, once the data had been transcribed using Parker's (1992) transcription convention methods (see Table 1 below) and a preliminary analysis had been conducted in order to determine which topics in the narratives would be suitable sources for follow-up questions.
The data were transcribed and then analysed using elements of Taylor and Littleton's (2006) narrative-discursive method to examine the discursive resources being drawn on in counsellors' narratives. Taylor and Littleton's (2006) analytical approach allows the researcher to focus on how an interviewee's narrative is situated in a particular time and place: meanings that exist in the "wider discursive environment" (Taylor & Littleton, 2006:23). It is this environment and how it shapes people's talk - "who that world makes and constrains them to be" (Taylor & Littleton, 2006:23) - and the subject positioned enabled by that talk which interests us in this paper.
The data were coded using the using the first iterative analytical task laid out by Taylor et al. (2006). This entailed looking for common elements that occur across several interviews as well as at different times within one interview and which point to particular discursive resources.
RESEARCH FINDINGS
Six discursive resources emerged from the counsellors' narratives. Five of these clustered broadly into two over-arching themes: discourses that engendered a sense of helplessness and those that allowed the counsellors to foresee positive outcomes for their counselling. In the first theme victimhood in the face of social power relations is emphasised. Discursive resources in this cluster are: 'patriarchal masculinity', 'traditional African culture' and 'female victimhood'. In the second theme women's agency is emphasised as well as an environment conducive to change. Discursive resources in this cluster are: 'female survivorhood' and 'human rights'. The 'nurturing femininity' discursive resource, which stood alone, depicts women in a positive light as carers of children and partners, but suggests that this is responsible for women not leaving IPV relationships when they should. These discursive resources will be highlighted with extracts from the narratives below.
Cluster of discursive resources: engendering helplessness
In this cluster of discursive resources, counsellors refer to gendered and cultural power relations that render their work difficult and that serve to keep the status quo concerning IPV. These discursive resources are the 'patriarchal masculinity' discourse, the 'traditional African culture' discourse and the 'female victimhood' discourse. Each is discussed below.
'Patriarchal masculinity'
Within the discursive resource of 'patriarchal masculinity' the counsellors positioned men as heads of households. In this role the men are depicted as the financial providers whilst women, according to the counsellors, are financially dependent on men. These ideas reproduce notable tenets of hegemonic constructions of masculinity (Brownridge et al., 2011; Connell, 2002; Hof & Richters, 1999, Vogelman et al., 1991). In this light men may also often perceive that they can control those whom they finance, as noted in Extract 1, linked to Extract 2 below:
Extract 1:
Shelly (P11): some of [the] women are staying with ... their husbands =/mmm/= because they don't have the sustainability of finance
Extract 2:
Duvi (P5): most cases you see it's the power =/mmm/= that made men to be abusive =/mmm/= they think that . they own this woman =/yes/= they own the children =/mmm/= they own everything (.) so no one (.) can change their mind set =/mmm/= if they want some things to happen this way (.) it must go that way (.)
As can be seen in the above extracts from Shelly's and Duvi's interviews, counsellors indicate that when women stay with their partners for financial stability, this limits the possibility for women's agency and predisposes them to the risk of violence and abuse as they may find it difficult to leave the IPV relationship. This phenomenon also relates to Connell's work on gender relations where she suggests that men often feel that women are "their property - to discard if they wish and to kill if need be" and to treat as they will (Connell, 2002:2).
Some of the participants shared the view that women are expected to be submissive in marital relationships:
Extract 3:
Amandisa (P3): our culture [isiXhosa] =/mmm/ the man (1) is the (.) top of the:: house /okay/ . the man can . use that power (1) (on the woman here) /okay/...sihlonipha amadoda aye ayasi-user baya kuba esithi ngawo la lapha phezulu e-top)[we respect the men and they use us because they say that they are the ones at the top]
Extract 4:
Mrs X (P8): back in our culture (1) eh:: it was normal for a:: male to hit a woman /mmm/ and . there was nothing done by that [there was nothing done about it] and even = /mmm/= our traditional leaders would say, 'no (.) ... the man ... must discipline (.) his wife'/ =/mmm/= so I think that is what h::as promoted the violence
In Extracts 3 and 4, Amandisa and Mrs X draw on the discursive resource of 'traditional "African" culture' (see explanation below) to explain gender relations: that women should "respect the men" ("sihlonipha amadoda") and that it is expected that men should discipline their wives. They also draw on the discourse of 'patriarchal masculinity' by highlighting that men are the heads of the household and, as such, may use control and violence to maintain this position. That is, men ensure the subordination of women, often in the form of IPV (Connell, 1995). In relation to this, when hegemonic forms of masculinity come under threat, one way of addressing this is through violence in order to encourage the women to resort to being submissive (see Connell, 1995; Jewkes, 2009; Vogelman et al., 1991) as can be seen in the phrase "the man can ... use that power on the woman."
'Traditional African culture'
'Traditional African culture' featured relatively frequently as a discursive resource that the counsellors drew upon in their narratives. 'Traditional African culture' is seen as underpinning patriarchal masculinity, as noted in extracts above. Women are expected to respect men, which in the participants' rendition is used to make women subservient:
Extract 5:
R: (.) So the woman has to:: listen to the man?
Amandisa: (P4): Mmm mmm [yes] /mmm/ our culture /yes/ ... sihlonipha amadoda and amadoda azibheka ngathi zinkosi [we respect the men and men act like they are kings] big king /like the king ja /yeah/ if ufuna into yonke eh::funeka ucele u:: ul:: u:: ingathi ungumntana but ungumfazi wake uyabona [if you want anything you have to beg for it as though you were a child even though you are his wife]
The requirement of respect referred to by Amandisa here is seen as belittling of women: in "our culture" men are treated like kings and women have to beg the men if they need anything. An element of hegemonic masculinity is evident here: a "configuration of gender practice" which, through the operation of 'culture', ensures, or is assumed to ensure, the subordination of women by the dominance of men (Connell, 1995:77).
A number of other features that could contribute to trouble in the home were ascribed to 'culture', including men having affairs after the birth of a baby and the inability to talk about contraception. These are noted in Extracts 6 and 7 below:
Extract 6:
Leigh (P6): first of all:: as a... new mother /mmhmm/= you focus ... to the child /mmm/ ... (.) so... in the house there is a competition between ... the husband [and] the child . and also that . in our culture /mmhmm/ when you:: have:: a . new-born baby you must stay with the elders: . so:: the husband (.) get (eh) the chance to:: have ... another woman ... outside. the relationship
Extract 7:
Duvi (P5): mostly you see that in our culture /mmm/ (.) we don't talk about those things [contraception] =/mmm/= there are few people who do talk (.) they just . grow up (.) they just eh nantsika [what do you call it?] get ... pregnant =/mmm/= without planning =/okay/= mmm =
In Extract 6 Leigh notes that 'in our culture' women are expected to care for their newborn child. This time of separation during the breastfeeding period is known as ukwalisana, during which post-partum sex is not encouraged. During this period, which can be longer than a year, men may seek sexual satisfaction outside the marital relationship (Leclerc-Madlala, Simbayi & Cloete, 2009). In Extract 7 Duvi shares the view that it is "embarrassing" to talk about contraception in her culture. This may result in women becoming pregnant "without planning", an additional stress in the relationship. On the other hand, should a woman try to negotiate contraception use, research shows that she may be accused of challenging her partner's fidelity or he may accuse her of being unfaithful (Jewkes, 2009).
Traditional culture was also viewed as prohibiting people from seeking the advice of a counsellor, as noted in the following extract:
Extract 8:
Amanda (P7): with the cultural difference::s ... like in the Xhosa culture ... it's actually very infra dig2 (.) to go to a counsellor /mkay/ you are meant to sort it out yourself or ... to sort it out with your elders =/mmm: :/= um (.) if your elders can't sort it out you go to your priest and then =/okay/= and only then ... people go to a counsellor ... a lot of my clients ... by the time they come here they've done [been to] their elders and they've done [been to] the priest and now they're at [name of organisation]
In the extract above Amanda makes it quite clear that in 'traditional "African" culture', seeking the help of a counsellor is "infra dig" and should be considered the last resort in terms of conflict resolution. There is an order which should first be followed: firstly with one's partner, failing which, one should consult the elders, then a priest and only then a counsellor. This relates to the idea that elders are often consulted for advice as their opinions are considered important in African communities (Rasool et al., 2005).
'Female victimhood'
Many of the participants drew upon the discourse of 'female victimhood' in their narratives. This is noted in the extracts below:
Extract 9:
Shelly (P1): ... the phone rang and he took [picked] up the phone and answered it =/mmm/= in front of me ... I don't mind if ... he answers the phone =/yes/= but ... (1) maybe the person [on the other end of the line] was saying, (.) 'can you answer the phone in front of your wife?' ... because he said =/mmm/ (.) 'I don't care this is my phone, I can answer the phone anywhere . at any time' . and I was like, '. who is on the phone?' =/yes/= and I took the phone and broke it and (1) he beat me =/sjoe/= he beat me
Extract 10:
Nomsa (P2): in most cases . they [the women] cling because of . the financial /mmm/ . status because . in most cases . they are unemployed /mmm/ so they stay because they said, 'no he's the one who's supporting me and my children' /mmm/ sometimes they ... said no they still love: (.) the man ... the man still loves her though he is beating (.) her up =/mmm/= mmm sometimes =/sjoe/= it's [there are] cases like that
Extract 11:
Amandisa (P4): sometimes the:: wife wants ... money to buy (.) i-clothes for the children /mmm::/ sometimes the woman wants money to:: paid these fees /yes/= at school /mmm/ ja /okay mmm/ and then the . domestic [violence] starting from there =/mmm sure/ specially [if] the woman is not ... working /mmm/ the man is a [the] head of the house =/yes/ and using the power /mmm/ to beat up the woman /yes/ yes /mmm/= and then the woman suffering
We can see in the above three extracts that 'female victimhood' can occur for a variety of reasons, according to the participants. One of the explanations from Shelly is women challenging their partner's behaviour (Extract 9). In Extract 10 we see that women can become victims of their circumstances by being financially reliant on their partners and willing to experience the IPV in return for financial security for themselves and their children, as was noted earlier. Nomsa argues that the woman still views the man as loving her, even though he beats her. Another side of financial concerns underpinning victimhood is unpacked further by Amandisa in Extract 11, where women may ask for money to cover the cost of clothes and school fees and are beaten because their husbands cannot provide for them. Amandisa indicates that men then discipline the women for highlighting their lack of provision for their family. This is linked to a tenet of hegemonic forms of masculinity where women are positioned as inferior subjects as they are financially dependent on men (see also Brownridge et al, 2011; Connell, 2002; Hof & Richters, 1999; Vogelman et al., 1991), as mentioned earlier, and men may use IPV to maintain order in the house and discipline their wives (see Connell, 1995; Kim & Motsei, 2002). This, in turn, highlights unequal gendered power relations between the men and women as evinced in these extracts.
Cluster of discursive resources: enabling positive outcomes
Counsellors deployed two discursive resources that highlighted possibilities for change and for positive outcomes regarding IPV. In the first, 'female survivorhood', agency is emphasised, while in the second, the communitarian notion of human rights is invoked. Each is discussed below.
'Female survivorhood'
In contrast to a discourse of female victimhood, some of the counsellors drew upon the discourse of 'female survivorhood' in their narratives, as noted in Extracts 12, 13 and 14 below:
Extract 12:
Shelly (P1): I was like it's me really cause if I didn't ask (.) maybe there will [would be] no fight you know =/okay yes/ (.) /mmm/ . up to now but now he cannot do that to me now =/no/= he cannot do that =/mmm/ . never
Extract 13:
Nomsa (P2): she told herself that 'if I allow him beating me up ...he would never stop beating me up' ... she got courage ... she fought back (1) and ... then he stopped (.) that day he was never beat her up again
Extract 14:
Amanda (P7): we (.) ... kno::w (.) from experience and from ... theory from all different countries . that the most dangerous time for (.) for people is when they actually make a stand to do something different because /okay/ the (.) perpetrator ... relies on the victim remaining a victim
In Extracts 12 and 13 the participants talk of women (Shelly herself in Extract 12 and one of Nomsa's clients in Extract 13) removing themselves from IPV situations. That is, they attempted to "negotiat[e] . the seemingly powerless positions which [they] have been allowed" (Mills, 2004:84; see also Jackson & Mazzei, 2012) by fighting back against the inferior subject position (that of victim) in which their perpetrator was placing them. In this way the women are placed in the subject position of survivor. Jackson and Mazzei (2012:60) state that "a knowing subject ... is an acting subject." The participants draw on this notion by indicating that the woman was aware that the IPV that she was experiencing was a problem and she was able to fight back. In Extract 14 Amanda provides insight into how the dynamics between perpetrator and victim play out. She suggests that when a victim decides to act out against her situation (as noted in Extracts 12 and 13) it is "the most dangerous time for them." This is because they are breaking the cycle of the perpetrator subordinating them, potentially resulting in further IPV as a means to discipline the woman, which in turn reveals the broader issue of unequal gendered power relations.
It must be noted, however, that the fact that the women in these extracts (and many others in the narratives) came to see the counsellor in the first place also shows agency in that they are attempting to assertively gain more information to possibly remove themselves from the IPV relationship. The women are also in this way challenging the discourse of 'traditional African culture' in which it is considered a taboo to visit a counsellor. These extracts can also be seen as an example of a story of deliverance (see Haaken, 2010:84) as the women here are "plotting [their] escape."
'Human rights'
The discursive resource of 'human rights' was also drawn upon in various instances by the participants as a response to IPV: participants indicated that they spent a lot of time and energy "educating" their clients, and also those in their communities, about their rights. Action taken against the perpetrators was linked to police and legal systems in the form of, for example, maintenance, divorce and protection orders. Examples of this 'human rights' discourse can be seen in the extracts below:
Extract 15:
Mrs X (P8): 1) No =/mmm/= it's ... not that common [husbands beating wives to discipline them] because I think our women of . this generation =/mmm/= have realised that they've got the rights =/mmm/= and (.) they cannot be pushed around
Extract 16:
Leigh (P6): ... women /mmhmm/ (2) must stand up /mmm/ for their rights:: /mmm/ and break (.) the silence /yes/ (.) seek ... help /mmm (1) that's important/ ... because if they are:: (.) not stand up and speak out ... when you . live in a abusive relationship your health is infected [affected] /mmm/ (1) so it is everybody's business /yes/ women's rights and health are everybody's business
Extract 17:
Amandisa (P4): these days ... those women are open minds [open-minded] /mmm/= because [name of NGO] is there (.) to educate the women /yes/= about their human rights . all the stakeholders . tell about their human [rights] it's not [name of NGO] only ... to tell ... the community about their services
It can be seen in Extract 15 that participants see women standing up for their rights as playing a role in reducing IPV, as stated by Mrs X. This standing up for one's rights is noted as being encouraged by the participants, as seen in Extracts 16 and 17 from Leigh's and Amandisa's interviews, who claim that they respectively "educate" and "tell" the women about their rights and also spread this awareness and their services in the wider communities. Thus, in these extracts human rights are seen as empowering tools that help women overcome their victim status.
A contradictory discursive resource: 'nurturing femininity'
'Nurturing femininity' was a discourse which the participants drew upon very often in their narratives. Women being bound to their children through the metaphorical inimba (see Goboda-Madikizela, 2011), roughly translated as a connection to others through the umbilical cord, was revealed as an element of the discourse of 'nurturing femininity'. This discursive resource portrayed women in a positive light - as people who care not only for their children but also for men. Despite this, 'nurturing femininity' was seen in participants' talk as an element that may perpetuate IPV, as women are unwilling to leave their children or partner. This can be seen in Extracts 18 and 19 and extended in Extract 20 below:
Extract 18:
Shelly (P1): The woman:: (.) is having (.) that thing called ... umbilical cord =/mmm/= you know (.) a woman cannot just do things =/mkay/= ... in Xhosa we call it inimba... the man do not have that =/yes/= it's only women =/mmm/= that is why they taking time to act even if the woman ... is in an abusive situation (.) it [she] takes time to act =/mmm/= on it =/okay mmm/= it's because they have that inimba
Extract 19:
Shelly (P1): They [women] also think about the baby . they also think about the man =/mmm/= they also think about the people around them =/mmm/= she's not thinking about her only ... it's not easy to act as a ...woman =/mmm/= you take time to act ... it's because they are having that =/umbilical cord/. [yes] they are attached to everybody
Extract 20:
Lwando (P3): when we talk to women ... [we tell them that] (.) they should be aware of that =/mmm/= whatever they do ... they must not leave their children =/yes/= with the men =/sjoe /= because ... (.) women ... were born with (.) taking care (.) of their children [they are nurturers] =/mmm/= more than anyone
In Extract 18 Shelly suggests that women have an inimba, which lessens their agency when attempting to leave an IPV relationship. This is because they may need to "take time to act" as they have to consider those around them. Goboda-Madikizela (2011) suggests that the concept of inimba is used to describe the connection the mother has to her child (and others who are not related to her), which allows her to feel sympathy for them or to understand their feelings. Here Shelly extends the explanation of the inimba in Extract 19, where she claims that because women have an inimba, they are "attached to everybody": they are emotionally and physically linked to their children and emotionally to those around them. In Extract 20 Lwando adds to the idea of a woman's role by suggesting that mothers are born as nurturers. Thus, it is an innate, suggestively inescapable feature of womanhood and a role which should be fulfilled and respected despite the circumstances.
DISCUSSION
Our research shows that the discursive resources that the participants shared in their narratives concerning how they understood IPV, and how they intervene, clustered into two main themes: discursive resources that underpin a sense of helplessness in the light of social power relations, and discursive resources that engender a sense of agency and the possibility of positive outcomes. One discursive resource was contradictory in simultaneously portraying women in a positive light and perpetuating IPV. This was the stand-alone discourse of 'nurturing femininity', which helped to explain why women may stay in abusive relationships because of the physical and emotional attachments to their children (and partners).
The discourse of 'patriarchal masculinity' constructs men as violent, dominating, the head of the household and often the financial provider for the female partner/family, whilst women were mostly positioned as 'nurturers' and 'victims' of this violence. The discourse of 'traditional African culture' is drawn upon by the participants to show how unjust gendered power relations are entrenched culturally, as women are expected to respect men and be submissive in marital and sexual relationships. In addition, various 'cultural' practices such as ukwalisana, the taboo on talking about contraceptives and the taboo on seeking formal counselling contribute to women experiencing IPV and not receiving help. As a result of the cultural expectation of submissiveness, women may be unaware that the IPV that they are experiencing is a problem and thus may not seek help.
In relation to this, the participants deployed a discourse of female victimhood in relation to IPV. The discourse of 'female victimhood' manifested in a vari ety of ways, including counsellors' constructions of women as often having limited agency when it comes to leaving IPV relationships because of their financial dependence on their male partners. These discursive resources engender a sense of helplessness amongst the counsellors as the work that they do has to counter such entrenched patriarchal and cultural norms.
In some instances, however, the counsellors drew upon the discourse of 'female survivorhood', where women were positioned as survivors for having the strength to recognise that they are experiencing IPV and to leave these IPV relationships and the oppressive interactions that 'patriarchal masculinity' impose upon them. In this way participants depicted the women as resisting being a victim. Overall, the fact that women come for counselling in the first place also shows their defiance of the taboo of seeking a counsellor for help with IPV, within the discourse of 'traditional "African" culture', as opposed to seeking advice from elders, priests and traditional leaders within their community. The sense of agency and possibility in terms of counselling that the 'female survivor' discourse allows was buttressed with a discourse of 'human rights'. A 'human rights' discourse underpins many sexual and reproductive health laws and is a powerful tool that counsellors can draw on, both in their interactions with women who experience IPV and with communities.
The 'nurturing femininity' discourse depicts women in a positive light - they care for those around them, including their partner and children. However, this serves to act against them as they are therefore hesitant to leave an abusive relationship.
IMPLICATIONS OF THE FINDINGS FOR THE COUNSELLING PROCESS
The findings of this study show that the participants deploy contradictory discourses in talking about IPV and their interventions with regard to IPV: some discursive resources enable them to see positive outcomes for their counselling, and some engender a sense of helplessness in the face of overwhelming power relations. Helping counsellors to emphasise the positive discursive resources in their understandings of, and interventions concerning, IPV may assist them both in providing constructive counselling and in feeling positive themselves about the efficacy of their interventions.
While this would be of use, we argue that it is also insufficient. In addition to an emphasis on women's agency and human rights, counsellors should be supported in two ways: to nuance their understandings of masculinities and femininities, and to feel part of collective action that addresses the social dynamics within which IPV takes place.
In terms of the first of these, it is noted that the participants depicted men and women in a relatively binary fashion. The utilisation of the 'nurturing femininity' and 'patriarchal masculinity' discourses serves to essentialise men and women. Women are constructed as fulfilling domestic roles in the household and as being mothers (and victims and survivors of IPV) and men, as their counterparts, are constructed as largely adulterous, violent, dominating, heads of the household and financial providers. In this way the discursive resources do not allow the men and women much opportunity for taking up other subject positions. Researchers in South Africa have emphasised the multiplicities of masculinities and femininities (in South Africa) (see Breckenridge, 1998; Hearn, 1987; Kimmel, 1987, in Ratele, 2008). The exposure of counsellors to discourses that emphasise the multiplicities of masculinities and femininities and their up-take of these multiplicities in their understanding of IPV and in their interventions regarding IPV may assist in nuancing their interactions.
Secondly, the social dynamics to which participants refer are indeed embedded in the power relations that they and their clients face on a daily basis. Addressing these is also essential. There was generally little focus on mobilising large-scale collective responsibility for, and accountability with regard to, IPV in the counsellors' narratives besides awareness raising. It is thus important that wider-scale interventions and advocacy take place in order for the IPV to be more successfully and broadly addressed. These could include collective socially benevolent endeavours, such as joint income-generating projects or support for small or micro-businesses, leading to less financial reliance of women on men, which may break down power struggles. Other examples include social platforms where men and women are invited to discuss matters and learn about IPV from one another's perspectives, and media campaigns that address the gendered issues (e.g. perceived roles of men and women) that underpin IPV. This could lead to enlightenment and hopefully a deeper understanding of the gender power struggles, possibly leading to changed, more positive gender relationships.
REFERENCES
BRITTON, H. 2006. Organising against gender violence in South Africa. Journal of Southern African Studies, 32(1): 145-163. [ Links ]
BROWNRIDGE, D.A., TAILLIEU, T.L., TYLER, K.A., TIWARI, A., CHAN, K.L. & SANTOS, S.C. 2011. Pregnancy and intimate partner violence: risk factors, severity, and health effects. Violence Against Women, 17(7):858-881. [ Links ]
BURR, V. 2003. Social constructionism (2nd ed). London: Routledge. [ Links ]
CAMPBELL, J.C. 2002. Health consequences of intimate partner violence. The Lancet, 359:1331-1336. [ Links ]
COKKINIDES, V.E., COKER, A.L., SANDERSON, M., ADDY, C. & BETHEA, L. 1999. Physical violence during pregnancy: maternal complications and birth outcomes. Obstetrics and Gynaecology, 93:661-666. [ Links ]
CONNELL, R.W. 1995. Masculinities. Cambridge: Polity Press. [ Links ]
CONNELL, R.W. 2002. Gender. Massachusetts: Blackwell Publishing Inc. [ Links ]
DAVIES, B. & HARRE, R. 1990. Positioning: the discursive production of selves. Journal for the Theory of Social Behaviour, 20(1):44-63. [ Links ]
DEVRIES, K.M., KISHOR, S., JOHNSON, H., STÓCKL, H., BACCHUS, L.J., GARCÍA-MORENO, C. & WATTS, C. 2010. Intimate partner violence during pregnancy: analysis of prevalence qualitative material from 19 countries. Reproductive Health Matters, 18(36):158-170. [ Links ]
DOMESTIC VIOLENCE ACT, No. 116 1998. [Online] Available: www.justice.gov.za/legislation/acts/1998-116.pdf. [ Links ]
FOUCAULT, M. 1972. The archaeology of knowledge. London: Tavistock. [ Links ]
GAVEY, N. 2011. Feminist poststructuralism and discourse analysis revisited. Psychology of Women Quarterly, 35(1) 183-188. [ Links ]
GOBODA-MADIKIZELA, P. 2011. Intersubjectivity and embodiment: exploring the role of the maternal in the language of forgiveness and reconciliation. Signs, 36(3):541-551. [ Links ]
GUPTA, J., SILVERMAN, J.G., HEMENWAY, D., ACEVEDO-GARÇIA, D., STEIN, D.J. & WILLIAMS, D.R. 2008. Physical violence among intimate partners and related exposures to violence among South African men. Canadian Medical Association Journal, 179(6):535-541. [ Links ]
HAAKEN, J. 2010. Hard knocks: domestic violence and the psychology of storytelling. East Sussex: Routledge. [ Links ]
HATCHER, A.M., ROMITO, P., ODERO, M., BUKUSI, E.A., ONON, M. & TURAN, J.M. 2013. Social context and drivers of intimate partner violence in rural Kenya: implications for the health of pregnant women. Culture, Health & Sexuality: an International Journal for Research, Intervention and Care, (15)4:404-419. [ Links ]
HAYDEN, A. 2010. Why rock the boat? Non-reporting of intimate partner violence. Auckland: Auckland University of Technology. (D thesis) [ Links ]
HOF, C. & RICHTERS, A. 1999. Exploring intersections between teenage pregnancy and gender violence: lessons from Zimbabwe. Women's Health and Action Research Centre (WHARC), 3(1):51-65. [ Links ]
IVERSON, K.M., STIRMAN, S.W., STREET, A.E., GERBER, M.R., CARPENTER, S.L., DICHTER, M.E., BAIR-MERRITT, M. & VOGT, D. 2016. Female veterans' preferences for counseling related to intimate partner violence: informing patient-centered interventions. General Hospital Psychiatry, 40:33-38. [ Links ]
JACKSON, A.Y. & MAZZEI, L.A. 2012. Thinking with theory in qualitative research: viewing qualitative material across multiple perspectives. Oxford: Routledge. [ Links ]
JASINSKI, J.L. 2004. Pregnancy and domestic violence. A review of the literature. Trauma, Violence & Abuse, 5(1):47-64. [ Links ]
JEWKES, R., LEVIN, J. & PENN-KEKANA, L. 2002. Risk factors for domestic violence: findings from a South African cross-sectional study. Social Science & Medicine, 55(9):1603-1617. [ Links ]
JEWKES, R. 2009. HIV and women. In: ROHLEDER, P., SWARTZ, L., KALICHMAN, S.C. & SIMBAYI, L.C. (eds), HIV/AIDS in South Africa 25 years on: psychosocial perspectives. New York, NY: Springer. [ Links ]
JOYNER, K. & MASH, R.J. 2011. The value of intervening for intimate partner violence in South African primary care: project evaluation. BMJ Open, 1:1-9. [ Links ]
JOYNER, K. & MASH, R.J. 2012. A comprehensive model for intimate partner violence in South African primary care: action research. BMC Health Services Research, 12:399-408. [ Links ]
KALDINE, F. 2007. Violence against women and children. In: VISSER, M. (ed), Contextualising community psychology in South Africa. Pretoria: Van Schaik Publishers. [ Links ]
KIM, J. & MOTSEI, M. 2002. "Women enjoy punishment": Attitudes and experiences of gender-based violence among PHC nurses in rural South Africa. Social Science & Medicine, 54:1243-1254. [ Links ]
LECLERC-MADLALA, S., SIMBAYI, L.C. & CLOETE, A. 2009. The sociocultural aspects of HIV/AIDS in South Africa. In: ROHLEDER, P., SWARTZ, L., KALICHMAN, S.C. & SIMBAYI, L.C. (eds), HIV/AIDS in South Africa 25 years on: psychosocial perspectives. New York, NY: Springer. [ Links ]
LEE, R.K., SANDERS THOMPSON, V.L. & MECHANIC, M.B. 2002. Intimate partner violence and women of color: a call for innovations. Rural Health and Women of Color, 92(4):530-534. [ Links ]
LEWIS, M.J., WEST, B., BAUTISTA, L., GREENBERG, A.M. & DONE-PEREZ, I. 2005. Perceptions of service providers and community members on intimate partner violence within a Latino community. Health, Education & Behaviour, 32(1):69-83. [ Links ]
MASH, R.J., FAIRALL, L., ADEJAYAN, O., IKPEFAN, O., KUMARI, J., MATHEE, S., OKUN, R. & YOGOLELO, W. 2012. A morbidity survey of South African primary care. Plos One, 7(3):1-12. [ Links ]
MBOKOTA, M. & MOODLEY, J. 2004. Domestic violence - an antenatal survey at King Edward VIII Hospital, Durban. South African Journal of Obstetrics and Gynaecology, 10(2):46-48. [ Links ]
McHATTIE, L.J. 2011. What helps, what hinders when counselling women who have experienced intimate partner violence. Burnaby: Simon Fraser University. (D thesis) [ Links ]
MILLER, T.W., VELTKAMP, L.J., LANE, T., BILYEU, J. & ELZIE, N. 2002. Care pathway guidelines for assessment and counseling for domestic violence. The Family Journal, 10(1):41-48. [ Links ]
MILLS, S. 2004. Discourse: the new critical idiom (2nd ed). London: Routledge. [ Links ]
MODIBA, L.M., BALIKI, O., MMALASA, R., REINEKE, P. & NSIKI, C. 2011. Pilot survey of domestic abuse amongst pregnant women attending an antenatal clinic in a public hospital in Gauteng Province in South Africa. Midwifery, 27(6):872-879. [ Links ]
MWAU, A. 2000. Counselling victims of domestic violence in Kenya. In: TURSHEN, M. (ed), African women's health. Eritrea: Africa World Press. [ Links ]
NJUHO, P.M. & DAVIDS, A. 2012. Patterns of physical assaults and the state of healthcare systems in South African communities: findings from a 2008 population-based national survey. South African Journal of Psychology, 42(2):270-281. [ Links ]
PARKER, I. 1992. Discourse dynamics: critical analysis for social and individual psychology. London: Routledge. [ Links ]
RASOOL BASSADIEN, S. & HOCHFELD, T. 2005. Across the public/private boundary: contextualising domestic violence in South Africa. Agenda: Empowering Women for Gender Equity, 19(66)4-15. [ Links ]
RATELE, K. 2008. Analysing males in Africa: certain useful elements in considering ruling masculinities. African and Asian Studies, 7(4):515-536. [ Links ]
RHODES, N.R. & McKENZIE, E.B. 1998. Why do battered women stay?: three decades of research. Aggression and Violent Behaviour, 3(4):391-406. [ Links ]
SEEDAT, M., VAN NIEKERK, A., JEWKES, R., SUFFLA, S. & RATELE, K. 2009. Violence and injuries in South Africa: prioritising an agenda for prevention. The Lancet, 374(9694):1011-1022. [ Links ]
SILVERMAN, J.G., RAJ, A. & CLEMENTS, K. 2004. Dating violence and associated sexual risk and pregnancy among adolescent girls in the United States. Pediatrics, 114(2):220-225. [ Links ]
SYKES, J.B. (ed). 1982. The concise Oxford dictionary (7th ed), Oxford: Oxford University Press. [ Links ]
TAYLOR, S. & LITTLETON, K. 2006. Biographies in talk: a narrative-discursive research approach. Qualitative Sociology Review, 1(2):22-38. [ Links ]
TERRE BLANCHE, M., DURRHEIM, K. & KELLY, K. 2006. Research in practice: applied methods for the social sciences. (2nd ed). Cape Town: UCT Press. [ Links ]
VOGELMAN, L. & EAGLE, G. 1991. Overcoming endemic violence against women in South Africa. Social Justice, 18(1/2):209-229. [ Links ]
WATTS, C. & MAYHEW, S. 2004. Reproductive health services and intimate partner violence: shaping a pragmatic response in sub-Saharan Africa. International Family Planning Perspectives, 4(30):207-213. [ Links ]
WENGRAF, T. 2001. Qualitative research interviewing. London: Sage Publications. [ Links ]
YOUNG, R.A. & COLLIN, A. 2004. Introduction: constructivism and social constructionism in the career field. Journal of Vocational Behavior, 64(3):373-388. [ Links ]
1 KEY: P = Participant (the number indicates the order in which they were interviewed) R = Researcher
2 "Beneath one's dignity, unbecoming" (Sykes, 1982:514).

