










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.53 n.1 Stellenbosch 2017
http://dx.doi.org/10.15270/52-2-545
ARTICLES
Exploring the views of health care service providers on life stressors and basic needs of HIV-positive mothers in rural areas of Lesotho
Ms Shoeshoe MofokengI; Prof Sulina GreenII
IPostgraduate student, University of Stellenbosch, Stellenbosch, South Africa
IIDepartment of Social Work, University of Stellenbosch, Stellenbosch, South Africa. sgreen@sun.ac.za
ABSTRACT
The human immunodeficiency virus (HIV) ranks as one of the deadliest viruses in the world. The second highest incidence of the virus has been recorded in Lesotho, where women and children are the most infected and affected. This article explores and describes views of health-care service providers on the life stressors experienced by HIV-positive mothers living in the rural areas of Lesotho and how their basic needs are met. Recommendations are made on how health-care service providers and the government can address the life stressors and basic needs of these mothers.
INTRODUCTION
People succumb to HIV and Aids on a regular basis. HIV and Aids is a disease that is killing people daily. It not only affects the health of sufferers, but also their psychosocial wellbeing and their economic situation. Lesotho is one of the poorest and least developed countries in the world. It has the second highest incidence of HIV, with 23.1% of its population recorded as being HIV positive, 340 000 of them being women (UNAIDS, 2014).
The availability of local support services is crucial to the provision of HIV and Aids care and prevention services for women (Castaneda, 2000:557). As there are fewer social, health and mental services in rural areas in general, women's access to the essential services may be restricted and existing services are more limited in scope than in urban areas.
There are a limited number of support services in the rural communities of Lesotho addressing life stressors and basic needs of HIV-positive mothers. One such support service, the Elizabeth Glassier Foundation (www.pedaids.org), provides free prevention of mother-to-child transmission (PMTP) services, comprehensive and family-centred HIV and Aids prevention, care and treatment services, community mobilisation for increased uptake and compliance with HIV and Aids services, and community healthcare workers who help with door-to-door visitation of patients to offer psychosocial support. There is also a mother-to-mothers organisation (www.m2m.org) that offers tracking of defaulters and psychosocial support groups on a monthly basis, which assists in dealing with life stressors that HIV-positive mothers face in their daily lives.
Castaneda (2000:560) reported that limited systematically derived information is available regarding the life stressors and basic needs of women who currently live with HIV and Aids in rural communities. Consequently the aim of this investigation was to explore the views of health-care service providers on the life stressors experienced by HIV-positive mothers and how their basic needs are met to determine how health-care service providers and government can provide social support to these mothers.
RESEARCH METHOD
Both quantitative and qualitative approaches were chosen to provide a framework from which the views of health care providers could be explored and described (De Vos, Strydom, Fouché & Delport, 2011). In addition, an exploratory and a descriptive research design were used in this investigation. An exploratory design was considered as appropriate for the study as it lends itself to acquiring insights into the nature of the life stressors and extent to which basic needs of HIV-positive mothers in the rural areas of Lesotho are met. A descriptive design was chosen to be used together with the exploratory design to offer an examination and explanation of the situation of these HIV-positive mothers (De Vos et al., 2011:95).
Through purposive sampling 30 participants who met the criteria for inclusion were recruited. Brink, Van der Walt and Van Rensburg (2012:141) state that it is justified that this type of sampling can be based on the judgment of the researcher regarding participants who are typical or representative of the characteristics and representative attributes of the study population. The criteria for selecting participants were that they should be doctors, nurses, social workers, counsellors or community health workers who fall within the catchment area of a selected hospital in Lesotho, should be rendering services to HIV-positive mothers, and should be able to participate in the study in English.
A semi-structured interview schedule guided interviews with the participants who were selected to participate in the study. After transcribing the interviews, themes were identified and a literature control was conducted as part of the data analysis so as to compare and contrast the data with existing literature (Creswell, 2003:30-31).
DISCUSSION OF THE FINDINGS
Profile of participants
Of the participants selected for the sample (n=30), nurses represented the highest number of 13 (44%), the second highest number of participants was seven (23.3%) community health workers, followed by six (20%) counsellors, three (10%) doctors and one (3%) social worker.
Life stressors experienced by mothers living with HIV in the rural areas of Lesotho
Edwards (1995:817) found that life stressors may be generalised as critical issues that people perceive as exceeding their personal and environmental resources to manage them. Life stressors include difficult social and environmental transitions, traumatic life events and any other life issues that disturb the existing fit between personal and environmental resources. HIV is one of the most serious critical life issues that a person can experience in that it affects not only the physical wellbeing but also the resources of its host. This is the biggest challenge for HIV-positive mothers in the rural areas.
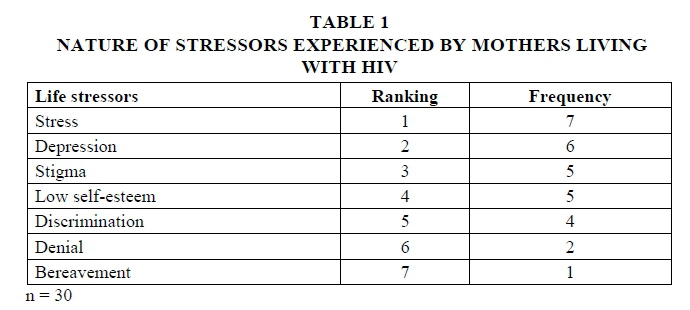
Consequently the nature of the life stressors associated with HIV experienced by these mothers was investigated. The rankings, from 1 to 7, were calculated on the basis of the frequency with which the stressors were selected by the participants. The rankings are presented in the table below and are discussed separately in order of the rank in the following sections.
Stress
Stress is the habitual or continuous response to a life stressor and is characterised by troubled emotional or physiological states, or both. Prolonged stress, together with a lack of effective coping skills and personal vulnerability, can lead to physiological, emotional or social dysfunction (Edwards, 1995:817). Being HIV positive causes emotional stress in mothers and they question where and how they were infected, and whether the community will accept them. The intake of antiretroviral medication requires a lifetime commitment as well as a solid support system; otherwise the chances of defaulting are high.
As shown in Table 1, health-care service providers identified stress as the strongest life stressor that HIV-positive mothers experience. These findings correspond with the view of Van Dyk (2008:274) that some people experience acute stress disorder after an HIVpositive diagnosis, or after the death of a significant other. An acute stress disorder is an anxiety disorder that develops in response to an extreme psychological or physical trauma.
When a mother experiences such feelings, she needs a strong support system to help her identity the signs and help her cope with the stress. Stress can also cause fear of disclosing HIV status and accessing treatment.
Depression
Ownyby, Jacobs, Waldrop-Valverde and Gould (2010:73) observed that depression is among the most common neuropsychiatric disorders that affect persons with HIV infection. It has a dramatic effect on patients' quality of life. In spite of its implications, it is likely that depression is under-recognised and under-treated in patients with HIV infection. Depression has a significant impact on the course and outcome of HIV infection through its effects on patients' adherence to medication regimens and via psycho-neuro-immunological mechanisms.
It is worth noting that Tsai, Bangsberg, Frongillo, Hunt, Moore, Martin and Weiser (2012) maintain that depression is recognised as a strong predictor of non-compliance with medical treatment plans. Furthermore, depression is associated with deteriorating HIV outcomes, including immunological decline, progression to Aids, and Aids-related mortality.
A fifth (n=6) of the participants reported that depression was the greatest life stressor experienced by mothers living with HIV. This is in line with the finding by Gleitman, Reisberg and Gross (2007:614) that depression centres on feelings of sadness, hopelessness and broad apathy about life. In addition, Ross and Deverell (2004:54) describe depression as anger turned inward towards oneself, citing an example that people may feel anger towards themselves for not having prevented the illness.
As also observed by Tsai et al. (2012:1), depression is common among people living with HIV and Aids in the United States and treatment is important clinically. If depression is not treated satisfactorily, deteriorating HIV-related outcomes may result. They add that several cross-sectional studies have described an association between food security and depression amongst people living with HIV. This relates to Maslow's theory which holds that, when the needs on the lowest tier are not met (physiological needs), it is difficult to meet higher needs (Louw & Edwards, 1997).
There is an urgent need for health-care providers to recognise and treat depression in their patients or to refer their patients to mental-health specialists for diagnosis and treatment when necessary. This requires trained and qualified professionals; with the support services offered in Lesotho, where psychosocial support is mainly supplied by other HIV-positive mothers or community health workers who have been informally trained, it may be very difficult to identify a client who is depressed or even refer her to the necessary support service for help.
Stigma
Stigma arises when a person is devalued because of a characteristic such as race, gender or illness. A major factor that distinguishes HIV and Aids from other chronic or terminal illnesses is stigma associated with the disease. This stigma results from a lack of knowledge about HIV and how it is transmitted (Skinner & Mfecane, 2004:159).
Five participants stated that stigma was one of the greatest life stressors experienced by the mothers living with HIV. This strongly supports the findings by Musingafi, Rugonge and Zebron (2012:105) that one of the reasons why stigma ranks so high is because some people with HIV stigmatise themselves. Consciously or not, some people with HIV think that their identity and worth have been damaged or spoiled because they have HIV. This is sometimes called "internalised stigma".
Bond, Chase and Aggleton (2002:353) conducted a study on stigma, HIV and Aids as well as the prevention of mother-to-child transmission in Zambia and found that, in the household and family setting, stigma manifested in the forms of verbal abuse, rejection, eviction and imposed restrictions on the person. People with HIV and Aids were subjected to blame, bitterness, anger, denial and the withdrawal of treatment and care, sometimes constituting blatant neglect.
Furthermore, the National Abandoned Infants Assistance Resource Centre (2012:9) found that stigma and discrimination contribute to infected women's vulnerability by inhibiting them from seeking help and support for their condition. The stigma around HIV and Aids can have a severe impact on those infected or affected by the virus. Prone to both stigma internalisation and stigma mismanagement, they are less likely to seek social support for fear of rejection and isolation. This inhibits discussion and acknowledgement of HIV as a major cause of illness and death, and prevents people from seeking counselling and obtaining medical and psychosocial care.
Social reactions to a disease evolve as new information about the disease becomes available, such as information on effective treatments. However, much of the HIV-related stigma is symbolic. A United States telephone survey of views of the general population comparing HIV and Aids stigma in 1991 and 1999, found that, although overt expressions of censure declined, one third of respondents in 1999 still expressed negative feelings towards HIV-positive people. Thus, despite changes in the treatment and perceptions around the epidemic, which should lead to decreasing stigmatisation, the negative effects of stigma continue to take a toll (Herek, Capitanio & Widaman, 2002:374).
Low self-esteem
According to Gordillo, Fekete, Platteau, Antoni, Schneiderman and Nostlinger (2009:28), self-esteem greatly determines the nature of interpersonal relationships, because individuals' feelings of self-worth have a bearing on both their beliefs and social behaviour. Low self-esteem may damage interpersonal relationships because it promotes a self-protective interpersonal style.
Five participants indicated that low self-esteem was the greatest life stressor experienced by mothers living with HIV. Self-esteem represents the extent to which one feels capable, significant, effective and worthy. It is the most important dimension of self-concept and is a major influence in human thinking and behaviour (Germain & Gitterman, 1996:17). The findings in this study reveal that, according to the participants, being HIV positive influences one's thinking and behaviour.
Discrimination
HIV and Aids-related discrimination remains one of the greatest stressors to people living with HIV infection or Aids. Discrimination concerns constitute but one reason why people do not have an HIV test or get their antiretroviral treatment, if they are infected (Van Dyk, 2008:131).
Four participants reported that discrimination was the greatest life stressor experienced by mothers living with HIV. It should be noted that, according to the National Abandoned Infants Assistance Resource Centre (2012:9), discrimination contributes to infected women's vulnerability by inhibiting them from seeking help and support. Disclosure is often avoided because women fear abandonment, rejection, discrimination, or upsetting family members.
Many HIV-infected individuals have voiced fears that disclosure would disrupt their current or future relationships, reputation or employment status (National Abandoned Infants Assistance Resource Centre, 2012:9).
Of importance for this investigation is that Baingana, Thomas and Comblain (2005:22) reported that stigma and discrimination can pose a challenge to professional intervention for a number of reasons. For example, in attempting to avoid discrimination, people may be less likely to adopt strategies to prevent the spreading of Aids infection such as condom use, revealing their status to sexual partners, and adherence to treatment regimens. Thus, in developing a support services programme for HIV-positive mothers, issues such as stigmatisation should always be taken into account.
Denial
Two participants said denial was the greatest life stressor experienced by mothers living with HIV.
A study conducted by Nam, Fielding, Avalos, Dickinson, Gaolathe and Geissler (2008) on the relationship of acceptance or denial of HIV status with antiretroviral treatment adherence among adult HIV patients in urban Botswana found that the key concept described by participants associated with good or excellent adherence was acceptance of their HIV status, whereas individuals experiencing adherence difficulties described aspects of denial.
As observed by Van Dyk (2007:220), disclosure can help people accept their HIV status and reduce the stress of coping on their own. It helps ease access to medical services, care and support, including access to antiretroviral therapy. Disclosure can help people protect themselves and others, especially if they happen to have accidents and blood is involved. It can also help reduce the stigma, discrimination and denial around HIV and promote responsibility, and it may encourage the person's loved ones to plan for the future.
Bereavement
Bereavement is an experience of pain and grief when a person loses someone or something of value, or if the loss of that person or thing is still anticipated (Mphale, Thlomola, Phatela, Rants'o & Nthane, 2010:108). Despite advances in HIV treatment and a reduction in Aids-related deaths, families will continue to lose loved ones to Aids. Bereaved women are particularly concerned about loss and coping issues related to their children, deceased partners or spouse, and family responsibilities (National Abandoned Infants Assistance Resource Centre, 2012:9).
One participant ranked bereavement as the greatest life stressor experienced by mothers living with HIV. According to Stroebe, Stroebe and Hansson (1999:34), the powerfully and deeply felt cravings for nurturance or security during the bereavement period can be transformed into needs for food, alcohol or sex.
According to AVERT (2012), despite the increased availability of antiretroviral medication, death is still a common outcome of HIV and Aids, and millions of children will lose one or both parents to the disease. When a mother's health is progressively deteriorating, it is important for her to plan for her children's future in terms of who will take care of them, whether that person is willing to take care of the children or whether resources would be available to take care of them.
Addressing the basic needs of HIV-positive mothers
Swartz, De la Rey, Duncan, Townsend and O'Neil (2011:238) recalled Maslow's (1970) theory that human motivation rests on a hierarchy of needs. Maslow maintained that once humans have fulfilled their basic needs, they can go on to meet more complex desires. Louw and Edwards (1997:446) proposed a contrasting approach to human motivation in allowing people to talk about the things that matter to them, and to systematically note what they say. This may proffer greater insights into human motivation. Maslow's hierarchy of needs, cited in Louw and Edwards (1997:449), are the following: physiological needs, safety needs, love and belonging needs, esteem and self-actualisation needs. This hierarchy of needs provided the conceptual framework for this investigation into the extent to which the basic needs of HIV-positive mothers are met according to the views of the participants.
Physiological needs
Physiological needs are about immediate survival, shelter, food and sleep. They are the primary and most basic needs for humans for daily survival (Poston, 2009:348) and are influenced generally by the cravings we have as human beings. If the body is deprived of oxygen, it will surely react in a certain way (Poston, 2009:349). An HIV-positive mother cannot take her antiretroviral medication as prescribed without first having a meal, as the body needs food to hold down the medicine for proper absorption.
Shelter as one of the physiological needs also plays a major role in providing a proper place for medication, where it will not be exposed to an environment that can negatively affect it, such as sun or fire, or where children cannot reach it. In the rural areas of Lesotho this may be a problem, especially where the whole family lives in a hut or one-roomed house which is used as a kitchen, bathroom and bedroom (Ministry of Health, 2013). A crowded poorly ventilated shelter may jeopardise the effectiveness of antiretroviral treatment and can contribute to the development of opportunistic infections such as tuberculosis or pneumonia and subsequent transmission to other members of the household.
Most participants stated that the mothers' psychological needs were not met because mothers "struggle to make ends meet" owing to a "lack of resources". Some, however, obtain assistance as the "government provides food supplements", which helps mothers to meet some of their needs.
Meeting physiological needs is affected by many different factors, such as "high unemployment rates and extreme poverty". According to Mbirimtengerenji (2007:616), unless and until poverty is reduced or alleviated, there will be little progress in either reducing transmission of the HIV virus or enhancing capacity to cope with its socioeconomic consequences. A multi-sectoral approach embracing a number of capacity-building programmes to combat the scourge is needed (Mbirimtengerenji, 2007:616).
Safety needs
Poston (2009:350) observes that safety needs are psychological in nature and are also determined by where an individual lives. A mother may feel the need to be protected from discrimination owing to her HIV-positive status; in the same way, she may also want to protect her children from any form of discrimination or harm. She also has the health of her children to worry about, especially of an infected child, for children with HIV are vulnerable to opportunistic and dangerous infections such as tuberculosis and pneumonia.
Safety needs are not only about a mother's children and her own status. They can also concern her daily life. Some women are afraid to ask their partners to use a condom, fearful of their reaction should they disclose their HIV status. Safe houses for mothers who may suffer abuse from their partners can help, while a counsellor is helping the family involved to solve disputes.
With regard to safety needs, some participants said HIV-positive mothers' needs were not met. The reasons for this included the fact that most mothers "live alone with their children" or "they are 'widows" and they run the "risk of being attacked' and were "abused by their spouse".
Love and belonging needs
Love and belonging needs are about acceptance, feeling safe and comfortable, and being supported, all of which usually contribute to long-term survival. Quality of life has been associated with the social support available to people living with HIV and to higher levels of life satisfaction (Roger, Migliardi & Mignone, 2012:488). A person needs support in order to accept his or her HIV status and live positively. In addition, support needs to be continuous for mothers to adhere to their medication programme, as this commitment will prolong life.
Roger et al. (2012:497) mention a study on social support conducted by Klepac, Pikla and Relja (2007) which suggested that quality of life is also influenced strongly by one's perceptions of social and family support. This study demonstrated that, regardless of other people's views, if an affected person perceived that social support was sufficient, improvements in individual resilience could be attained (Roger et al., 2012:497). Providing a link to community-based organisations that can promote social support for women living with HIV has clear implications for improved physical and emotional health.
As to love and belonging needs, most of the participants said these were sometimes met, usually by children because "they love unconditionally". Other participants, however, held the view that these needs were not met owing to lack of support because "spouses or husbands stay at their work places" and they are not around to provide "emotional support to their wives ". Mothers also suffered abuse such as "emotional abuse" because of being HIV positive. Important here is that Roger et al. (2012:488) maintained that love and belonging needs are about acceptance and feeling safe and comfortable. If mothers are abused and not comfortable, their love and belonging needs are not met.
Esteem
According to Germain and Gitterman (1996:17), self-esteem represents the extent to which one feels capable, significant, effective and worthy. It is the most important dimension of one's self-concept and has a major influence on thinking and behaviour.
Esteem has to do with recognition and achievement, setting goals and achieving them. Poston (2009:351) argues this is the highest platform in the category of basic needs. The process of growth, when addressing one's self-esteem, builds the bridge to one's awareness. The need for esteem is met when a person has established a certain level of status, recognition, fame, reputation and appreciation, to name just a few. These areas in a person's life take work to maintain.
A diagnosis of HIV often results in low self-esteem and may also have a negative impact on a person's reputation, for infection is usually associated with misbehaviour. A mother infected with HIV not only has to deal with society judging her, but also her own conscience and acceptance of her status. She may end up not respecting herself and even trying to make others accept her by stopping antiretroviral medication and claiming she was misdiagnosed and does not have HIV.
According to Gordillo et al. (2009:524), people living with HIV who are satisfied with the amount of support available to them tend to experience less psychological distress, a higher quality of life and greater self-esteem.
Disclosure seems to assist in meeting self-esteem needs, especially when the other lower human needs are met. According to participants, disclosure can help mothers to be "comfortable with their status". The participants reported that mothers' needs were not met because "they obey their husbands'" even in situations where they do not agree with them and this "brings about esteem" issues for the mothers when they "lack physical and emotional support". These findings correspond with Maslow's hierarchy of needs, which observed that it is difficult for upper-level needs to be met if lower-level needs are not met, as physical and emotional support reside on the lower levels of the hierarchy of needs.
Self-actualisation
Swartz et al. (2011:238) maintain that the self-actualisation need is the highest level of need to be achieved. It refers to the complete development of the self and becoming the best person one can be. Conditions necessary to satisfy this need include not being distracted by lower-level needs, being able to love and be loved, being free of self-imposed and societal constraints, and being able to recognise one's own strengths and weaknesses.
Where self-actualisation is concerned, being able to pinpoint how one truly feels about something is often a little more challenging to figure out, or it can be the determining factor for how well one is connected with one's self and abilities. For an HIV-positive person to reach self-actualisation means she has to fully accept her status, commit wholly to treatment, not be afraid to disclose, and be at the point to support others by offering her personal journey to self-actualisation as motive. For a mother to reach this stage support is needed so that she can later support others.
With regard to self-actualisation needs, some participants held the view that these needs were sometimes met, because "the government provides free education and bursaries". Others, however, said mothers' self-actualisation needs were not met because it was "rare to find a mother whose needs are all met". It should be noted that, according to Johnson and Yanca (2007:13), unmet needs reflect an imbalance between the reciprocal response of the person and the environment. Sometimes needs are not met because of insufficient resources. The participants reported that mothers "do not have funds to cater for even their most basic needs'". According to Swartz et al. (2011:238) self-actualisation is a high level of need and refers to the complete development of the self and becoming the best person one can be. Conditions necessary to satisfy this need include not being distracted by lower-level needs. Considering the findings on the extent to which the lower-level needs of HIV-positive mothers are met, it would be very difficult for these mothers to reach self-actualisation.
IMPLICATIONS AND CONCLUSION
The findings of the study reveal that HIV-positive mothers in Lesotho are in distress. This is evident in the nature and range of life stressors they are experiencing and the limited extent to which their basic needs are addressed.
In order to promote their wellbeing, it is suggested that health-care service providers should inform HIV-positive mothers about existing social support structures such as door-to-door visitation services and support groups. In addition, social workers should use existing support groups for mothers to provide them with opportunities to assist each other in dealing with their life stressors and in addressing their basic needs. Where these groups do not exist, they should start such groups. This should, however, not be done in the customary facilities only, as some mothers cannot afford transport. Similarly, the need for government to expand social, health and mental services for HIV and Aids prevention, care and treatment in rural areas to address the life stressors and basic needs of these mothers is emphasised.
REFERENCES
AVERT. 2012. HIV & AIDS information. UK: AVERT. [Online] Available: www.avert.org [Accessed: 05/05/2014]. [ Links ]
BAINGANA, F., THOMAS, R. & COMBLAIN, C. 2005. HIV/AIDS and mental health. Washington DC: World Bank Human Development Network. [ Links ]
BELL, E., MTHEMBU, P., O'SULLIVAN, S. & MOODY, K. 2007. Sexual and reproductive health services and HIV testing: perspectives and experiences of women and men living with HIV and AIDS. Reproductive Health Matters, 15(29): 113-135. [ Links ]
BOND, V., CHASE, E. & AGGLETON, P. 2002. Stigma, HIV/AIDS and prevention of mother-to-child transmission in Zambia. Evaluation and program planning. London School of Hygiene and Tropical Medication Journal, 25(4):347-356. [ Links ]
BRINK, H., VAN DER WALT, C. & VAN RENSBURG, G. 2012. Fundamentals of research methodology for healthcare professionals (3rd ed). Cape Town: Juta & Company Ltd. [ Links ]
CASTANEDA, D. 2000. HIV/AIDS-related services for women and the rural community context. AIDS Care: Psychological and Socio-Medical Aspects of AIDS/HIV, 12:549-565. [ Links ]
CRESWELL, J.W. 2003. Research design: qualitative, quantitative and mixed method approaches. California: Sage publications. [ Links ]
DE VOS, A.S., STRYDOM, H., FOUCHE, C.B. & DELPORT, C.S.L. 2011. Research at grass roots: for the social science and human service professions (4th ed). Pretoria: JL van Schaik Publishers. [ Links ]
EDWARDS, R. 1995. Encyclopedia of Social Work. Washington DC: NASW Press. Elizabeth Glassier Foundation. [Online] Available: www.pedaids.org [Accessed: 05/05/2014]. [ Links ]
GERMAIN, C. & GITTERMAN, A. 1996. The life model of social work practice: advances in theory and practice. New York, N.Y.: Columbia University Press. [ Links ]
GLEITMAN, H., REISBERG, D. & GROSS, J.J. 2007. Psychology (7th ed). New York: Norton. [ Links ]
GORDILLO, V., FEKETE, E., PLATTEAU, T., ANTONI, M.H., SCHNEIDERMAN, N. & NOSTLINGER, C. 2009. Emotional support and gender in people living with HIV: effects on psychological well-being. Journal of Behavioral Medicine, 32(6):523-531. [ Links ]
HEREK, G.M., CAPITANIO, J.P. & WIDAMAN, K.F. 2002. HIV-related stigma and knowledge in the United States: prevalence and trends, 1991-1999. American Journal of Public Health, 92(3)371-377. [ Links ]
JOHNSON, L. & YANCA, S. 2007. Social work practice: a generalist approach (9th ed). Boston: Allyn & Bacon. [ Links ]
LOUW, D.A. & EDWARDS, D.J.A. 1997. Psychology: an introduction for students in Southern Africa (2nd ed). Sandton: Heinemann Higher & Further Education (Pty) Ltd. [ Links ]
MBIRIMTENGERENJI, N.D. 2007. Is HIV/AIDS epidemic outcome of poverty in Sub-Saharan Africa? Croat Medical Journal, 48(5):605-617. [ Links ]
MINISTRY OF HEALTH, 2013. National Guidelines for the prevention of mother to child transmission of HIV. Maseru. Government of Lesotho. [ Links ]
MOTHERS TO MOTHERS. [Online] Available: www.m2m.org [Accessed: 05/05/2014]. [ Links ]
MPHALE, M., THLOMOLA, M.M., PHATELA, P., RANTS'O, J. & NTHANE, M.N. 2010. HIV and AIDS counselling and psychological support. Maseru: Ministry of Health and Social Welfare, Lesotho. [ Links ]
MUSINGAFI, M., RUGONGE, S. & ZEBRON, S. 2012. HIV and AIDS management: Handbook for social science students in Sub-Saharan Africa. Germany: LAP LAMBERT academic publishing GmbH & Co. KG and licensors. [ Links ]
NAM, S.L., FIELDING, K., AVALOS, A., DICKINSON, D., GAOLATHE, T. & GEISSLER, P.W. 2008. The relationship of acceptance or denial of HIV status to antiretroviral adherence among adult HIV patients in urban Botswana. Social Science & Medicine, 67(11):1934. [ Links ]
NATIONAL ABANDONED INFANTS ASSISTANCE RESOURCE CENTRE. 2012. Women and children with HIV/AIDS. National Abandoned Infants Assistance Resource Centre: U.C. Berkeley. [ Links ]
OWNYBY, R.L., JACOBS, R.J., WALDORP-VALVERDE, D. & GOULD, F. 2010. Depression care and prevalence in HIV-positive individuals. [Online] Available: https://doi.org/10.2147/NBHIV.S7296. [Accessed: 10/05/2014]. [ Links ]
POSTON B. 2009. An exercise in personal exploration: Maslow's hierarchy of needs. Everest College, Thornton: Association of Surgical Technologists. [ Links ]
ROGER, K., MIGLIARDI, P. & MIGNONE, J. 2012. HIV, social support and care among vulnerable women. Journal of Community Psychology, 40(5):487-500. [ Links ]
ROSS, E. & DEVERELL, A. 2004. Psychosocial issues in health, illness and disability: A reader for healthcare professionals. Pretoria: Van Schaik Publishers. [ Links ]
SKINNER, D. & MFECANE, S. 2004. Stigma, discrimination and the implications for people living with HIV/AIDS in South Africa. Social Aspects of HIV/AIDS, 1(3): 157-164. [ Links ]
STROEBE, M.S., STROEBE, W. & HANSSON, R.O. 1999. Handbook of Bereavement: theory, research, and intervention. USA: Cambridge University Press. [ Links ]
SWARTZ, L., DE LA REY, C., DUNCAN, N., TOWNSEND, L. & O'NEILL, V. 2011. Psychology: an introduction (3rd ed). Cape Town: Oxford University Press. [ Links ]
TSAI, A.C., BANGSBERG, D.R., FRONGILLO E.A., HUNT, P.W., MUZOORA C., MARTIN, J.N. & WEISER, S.D. 2012. Food insecurity, depression and the modifying role of social support among people living with HIV/AIDS in rural Uganda. Social Science and Medicine Journal, 74:2012-2019. [ Links ]
UNAIDS. 2014. UNAIDS Report on the Global AIDS Epidemic. Geneva: UNAIDS. [ Links ]
VAN DYK, A.C. 2007. HIV/AIDS care & counselling (3rd ed). Cape Town: Pearson Education, South Africa. [ Links ]
VAN DYK, A.C. 2008. HIV/AIDS care & counselling (4th ed). Cape Town: Pearson Education, South Africa. [ Links ]


{kind=link}