










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.51 n.3 Stellenbosch 2015
http://dx.doi.org/51-3-457
ARTICLES
A critical ethic of care for the homeless applied to an organisation in Cape Town
Kathleen Jane Collins
Prof. Department of Social Work, University of Johannesburg, Johannesburg, South Africa
ABSTRACT
The situation faced by homeless people within South Africa is one complicated by numerous social, economic and political problems interacting to form a unique situation. The researcher volunteered within the church-based organisation U-turn, interacting with clients at a soup kitchen in Cape Town, South Africa. Using an ethnographic approach, the researcher was faced with dilemmas emerging from Tronto's (1993) "ethic of care". Discussing this organisation's mixed results at providing transformative care within this ethic and their own theoretical framework brings to light the merits of providing any service at all to clients who have very little else.
INTRODUCTION
Being homeless in South Africa is far more the consequence of a tragic failure of multiple systems than it is a question of individual vulnerabilities as is more common within first world societies (Schout, De Jongh & Zeelen, 2011; Van Laere & Withers, 2008). In the South African context the truly rock bottom end of poverty as depicted in the lives of the homeless exists at least partly because of the lingering echoes of the past apartheid system rather than because of mental illness, marginalisation or simply poverty (Cross, Seager, Erasmus, Ward & O'Donovan, 2010; Moyo, Patel & Ross, 2015). Moreover, there are unique factors in post-apartheid government policies that highlight the constituents of a growing economic inequality (Biko, 2013; Mohamed, 2011). The gap between the "haves" and the "have nots" is widening yearly, with South Africa surpassing Brazil in 2013 as having the highest Gini coefficient globally (Hoffman, 2013). This widening gap is making it far more difficult for those at the bottom to re-enter a society that is struggling to meet the needs of even the middle class (Biko, 2013; Mbeki, 2011).
Although political factors affect the situation of care of the homeless worldwide (Cross et al., 2010; Schout et al., 2011), in their attempt to redress past inequities, postapartheid policies have given rise to expectations of care, especially amongst black people as disadvantaged under apartheid, which have not been fulfilled (Jansen, 2009; Mbeki, 2011; Ramphele, 2008). As the democratic process transformed South African policies, it laid down a foundation of rights that has begun to foster a culture of prerogative which is potentially self-defeating for much of South Africa's poor. In their extreme form, expectations amount to societal attitudes of entitlement, making it difficult for clients of welfare services to feel personally empowered. An unemployment rate of 25%, involving 4.7 million people (Stats SA, 2013), corruption at all levels of government, wastage of public funds and unequal service delivery serves to push this entitlement into a deep-seated disillusionment with the available opportunities within South Africa (Biko, 2013; Gumede, 2012; Hoffman, 2013; Luiz, 2013; Marais, 2012; Ramphele, 2012; Wilson, 2010). This is a potentially debilitating temperament for the homeless, suggesting a life of meagre survival without hope of improvement. These most marginalised within society often suffer from "anomie", a feeling that life is pointless and experience a lack of belonging to a particular society (Schout et al., 2011), discouraging their response to care services within that society. Van Laere and Withers (2008) discern in international networks that not only the homeless but also their carers are the most marginalised groups in social service. In South Africa Cross et al. (2010) and Moyo et al. (2015) describe the difficulties of service providers as well as the gaps in social and economic policy in addressing the needs of the homeless.
Tronto (1993) argues that any ethic of care must be situated completely within a moral and political context. The uniquely South African context will, as this article indicates, impose its own effects on the provision of care to the homeless. This context provides both the moral imperative to provide care and, unfortunately, an economic and political environment that frustrates and debilitates one such organisation (U-turn) providing care. The article will examine arguments about whether or not it is better to provide inadequate care or rather no care at all, based on a critical discussion of the services delivered by U-turn in caring for the homeless in Cape Town, South Africa. How is Uturn transforming the lifestyle of the homeless people it seeks to serve? This question will be scrutinised within the context of the researcher's own experiences as a weekly volunteer from August 2011 to November 2013 and contextualised further with additional broader references to work with the homeless. Furthermore, the services that U-turn provides will be examined within the four attributes which Tronto developed in 1993, namely attentiveness, responsibility, competence and responsiveness. No attempt is made in the article to investigate the causes of homelessness in the clients at U-Turn, but rather it depicts the experience of care giving and receiving. The care provided by UTurn is presented in a structured programme consisting of three phases, which theoretically move the homeless from the street into a shelter, followed by employment and independent living off the street. On arrival in Phase 1 clients are registered on the computer and technologically monitored after this, providing a clear picture of their position in the programme. Effectiveness of the programme relies on the empowerment of the client and the programme assumes that clients wish to re-enter society in a functional way. However, care continues to be provided to those who do not move through the programme, under conditions which will be presented below.
METHODOLOGY
Ethnography is the most appropriate term for the methodology utilised in this research, referring to definitions by Babbie and Mouton (2001), Fine (2003) and Fouché (2011), which describe ethnography as the study of the behaviour of a group in the field, where the researcher typically enters the field as a participant-observer. The field itself also becomes a subject of study. In the continuum of four theoretical stances ranging from complete participant to complete observer in participant observation presented by Gold in 1958 and applied widely since then (Fine, 2003), the researcher in this case fills the second stance of "participant as observer", where she had duties as a volunteer at a soup kitchen of transporting and serving food, checking the register and interacting with clients while they ate and socialised (participant), and where she observed the setting, conducted informal interviews and kept a diary of the events and her reflections on them (observer). The body of literature on the homeless was consulted and the contents of the diary were classified deductively under Tronto's four attributes of an ethic of care.
SITUATING U-TURN WITHIN TRONTO'S ETHIC OF CARE
Cape Town's population is 3.7 million; vagrancy is estimated by the Department of Social Development (2013) at 7,000 people with night shelter and meals for fewer than 2,000. U-turn's programme consists of three phases: the first one reaches out with food, clothing and referral to shelter to those who are either homeless or strolling daily on the street; the second provides skills training and protected employment; and the third supports those who live and work independently. The organisation conveys a strong Christian message, employing only church-going individuals and preceding all its activities with a Bible reading, discussion and prayer. U-turn thus shapes the moral context of care through its Christian ethic. Disappointingly to a volunteer who espoused the three-phased structure, despite the organisation's best efforts to return their clients to norm-based sustainment in society, of the 944 clients whom they served in 2012, only 12 graduated from their programme (U-Turn Annual Report, 2012). The fact that so few of its clients re-entered society may be the result of a lack of available resources within the organisation, the wider economic environment, possible problems within the programme itself, and especially the unchanged volition of the clients themselves.
Tronto's (1993) definition of care posits that care ought to hold a central role within human life and is fundamentally a practice rather than a set of rules or principles. This centrality aligns with the Christian belief held by the organisation that one must care for those in need. The care that they provide is for many of the staff an everyday practice. U-Turn's Phase 1 client-side operation is the presentation of the meals, clothing and engagement with clients on the street with the aim of getting them into shelters. It is in Phase 1 that the researcher was engaged as a volunteer. For one staff member, Johnny,1 this is his vocation and a large part of his identity. In his past he himself was on the street and his upliftment by the Christian faith drives his motivation to persevere with the seemingly futile situation his clients find themselves in. The practice of an ethic of care requires both particular acts of care as well as a habit 'to care' that informs the carer's moral life (Tronto, 1993). Johnny is not the only person to have graduated from the programme and now working at U-turn, but one of a handful such clients. This may indicate the programme's success and the internalisation of the organisation's values. It also highlights, however, the restricted success that clients have in re-entering society, as the total number engaged overshadows the small number who graduate each year from Phase 2, to be discussed below.
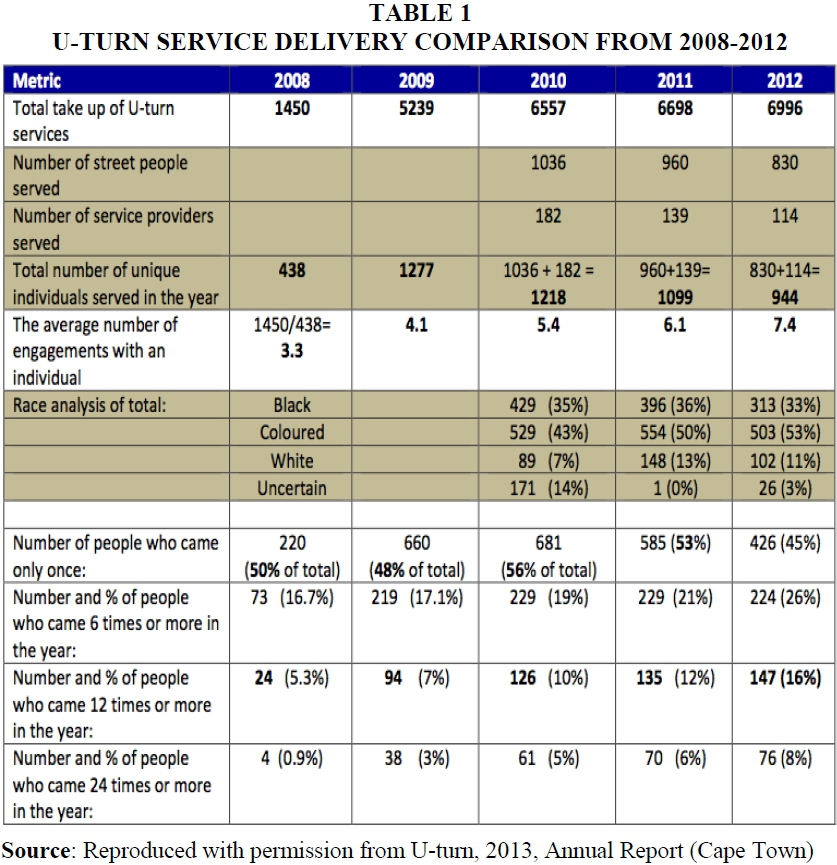
During provision of care, a caregiver will typically face a range of moral dilemmas. The moral qualities of care are more ambiguous than carefully defined precepts, as the practice of care is both complex and evolving (Tronto, 1993). The table below is taken from U-turn's Annual Report (2013). It shows the total number of clients served from 2008 to 2012, the racial makeup of clients and the percentages of clients who return frequently, setting some uncertainties in its interpretation.
Table 1 indicates the use of care that U-turn provides in Phase 1. With increasing service delivery since records were formalised in 2008, in 2012 client numbers decreased and the largest proportion, 45% of 944 clients, came only once. This percentage is apparently unaffected by U-turn as no behavioural change is indicated by their attendance alone. Given that only 12 of 944 moved from Phase 1 to Phase 2, the question is raised whether care should be provided if it allows for the stagnation of the client (the pragmatic view), the other view (which would be Tronto's) being that removing care could lead to further hardship for the clients. One possibility is that the programme does not appeal enough for clients to return; another possibility is that given that the meals and clothing services are run using a voucher system received mainly by donation, a limited number of vouchers may be in circulation, requiring an increase in community awareness and support. A third possibility is that basic needs are being met by another source of income, which could be employment, however temporary.2 The communication loop in Phase 1 is too limited to provide information that would answer these questions.
Tronto's (1993) study of care as a political ethic is regarded as classic. Although she has written more current work, the original definition and philosophy continue to be relevant and are applied in critical analyses around the world (Barnes, 2012, Bozalek & Hooyman, 2013; SSPARC, University of Brighton, 2012; ESOCSCI (New Zealand), 2012). The provision of U-turn's services will be discussed further within the framework of Tronto's ethic of care in the sections below. As the categories overlap and interlink in this framework, there will be some repetition in the article.
Care, according to Tronto (1993), is a process that is divisible into distinct four phases namely caring about (paying attention), taking care of (assuming responsibility), care giving (the physical act of caring) and care receiving (the reaction to care provided). This links to her four sub-elements; (1) attentiveness, which is the proclivity to become aware of need, (2) responsibility, the carer's willingness to respond and assume responsibility for care, (3) competence, having the skill and resources necessary to provide good quality care, (4) responsiveness, which refers to the response of the object of care to that care and how the care-giver incorporates this within their care process to steer clear of potential abuse. Bozalek and Hooyman (2013:3), discuss this the views of care in this framework "as a moral, social and political practice and disposition necessary for human survival, and regards humans as relational and interdependent, thus placing the necessity of care in everyday life as a central focus."
Tronto's framework is particularly well suited in the South African context as it takes into account cultural variation with its wide-ranging categories. U-turn's clients come from many walks of life and across all four major racial groups within South Africa (UTurn Annual Report, 2012). A comprehensive definition of care allows for the analysis of the effects of macro processes of political and economic disadvantage as well as linking this to the micro context of a client' s life (Barnes, 2012; Bozalek & Hooyman, 2013). Such a perception legitimises the sharing of power with local authorities and community leaders, arguing against the accretion of power amongst the currently powerful such as the state or regional authorities, thereby increasing the value of care activities (Tronto, 1993). The local contact also mitigates the estrangement from care based in more remote macro structures that Schout et al. (2011) write about, which leads to care avoidance in clients and care paralysis in service providers in Europe. Sanchez (2010) concluded that in South Africa people closer to the level of those being cared for are more likely, and perhaps better able, to provide that care appropriately. U-turn's service is run from a disused electricity power station donated by the local authority, which is in the process of upgrading the building structure and facilities to better support the service. Thus a local non-governmental care service leads to a local governmental response to improve the local community facilities and creating lasting value. This is in contrast to the national government, which has halted its financial support via the national lottery grant (U-Turn Annual Report, 2012). Time and again we see examples of a lack of support or policy change on a national level that adversely affects nongovernment organisations such as U-turn. (Gumede, 2012; Luiz, 2013; Marais, 2012; Ramphele, 2012; Wilson, 2010).
ATTENTIVENESS TO LOCAL NEEDS
Attending to the needs of those in society requires an awareness of the need, and who has needs (Tronto, 1993). Tronto (1993) argues that this is crucial for genuine human interaction. The organisational mission of U-turn is to uplift street people by direct intervention at basic need level.
Neoliberalism and privileged irresponsibility
The homeless, within a pervasive neoliberalism, fall victim to the belief that the growth of wealth within a country will trickle down and eventually uplift those at the bottom of the societal pyramid. Economists and social workers alike criticise this as too idealistic and macro-focused (Biko, 2013; Gray & Lombard, 2008; Patel, 2005; Pillay, 2013; Sewpaul, 2005). In similar vein, Tronto (1993) coined the phrase "privileged irresponsibility" describing how the most advantaged within society purchase caring services, thus delegating care-giving work, and ultimately avoiding the responsibility for the adequacy of hands-on care. There is an ignorance that prevails which makes it difficult for a person of means to even be aware of the needs of the less fortunate. In South Africa, although adults and children beg prominently in affluent neighbourhoods, their position is generally considered their own responsibility and not the result of any need that might be fulfilled by a caring society (Galvao, 2012). This point is examined further under the heading of responsibility below.
Privileged irresponsibility affords those with means the opportunity to ignore the hardships that they do not face as well as avoiding giving care directly (Tronto, 1993). This speaks to the attentiveness of the general public and their being closed to the needs of others, particularly their long-term needs. The "care" that homeless people receive on the street is not sustained; it is often simply a hand-out of small change, a means possibly for people to alleviate their own personal guilt at having so much more than the beggar in front of them. Galvao (2012), Schultz and Buys (2011) in common with Cape Town's civic policy (Department of Social Development, 2013), consider that these types of actions create an enabling environment that keeps people on the streets. U-turn strives to counteract this situation in their philosophy, as well as specifically through implementation of their voucher system.
U-turn also receives donations in the form of food and clothing from local shops and schools. U-turn vouchers are available to the general public and individuals can provide them to the beggars who appear on the streets of Cape Town, thereby steering them into a monitored organisation, which a once-off hand-out does not do. These donations are the result of U-turn raising awareness of the needs of their clients, increasing the attentiveness of the wider community and highlighting their responsibility to care.
Assisting clients' re-entry into modern society
U-turn has set out to welcome clients in off the street, provide a warm meal, clothing, interim medical attention and, if possible, referral to stable accommodation or shelter. Following this, the aim is to assist in the client's re-entry into society through various levels of employment and the development of clients' information technology, interpersonal and management skills in a structured training programme.
RESPONSIBILITY TO PROVIDE CARE
"We might assume a responsibility because we recognise that there is no other way that the need will be met except by our meeting it" (Tronto, 1993:132). Webster (2010:228) explains that the high rates of unemployment and poverty are not "personal trouble" but a public issue. The public accountability for the upliftment of the poor and previously disadvantaged population of South Africa is underlined in a multi-dimensional overview of governance by Plaatjies (2013). This does not contradict the belief that a local authority and community are better poised to assist those in need.
The following two sections will highlight the differences in support from local and national governments in caring for the homeless.
Contrasting local and national governments
U-turn is situated within the City of Cape Town, located in the Western Cape, one of the nine provinces in South Africa. Local government here does take on the responsibility to provide care in partnership with U-turn. For example, there is the Graffiti Clean-up Project, aimed at removing graffiti from city property and public infrastructure in one of the sub-councils in the city. This mutually beneficial partnership uses U-turn clients and provides them with a "sheltered employment" opportunity (Wilson, n.d.). The same is true for the usage of a restored power station, which was donated by a local authority.
There are 22 shelters in Cape Town, with beds for 2000 people (U-turn database, 2013). There are also six new emergency shelters for assessing needs and reference to specialists in cases of mental illness. This move reaffirms the City's commitment to "ensuring Cape Town is a caring and inclusive city" (Pollack, 2012:1). Conversely, it is often the case that policy makers regard visible homelessness as a negative and a hindrance to economic growth (Cross et al., 2010). Local government has been accused of trying to clean the streets in the hope of attracting economic investment by having poverty-free central business districts simply by removing spaces for and traces of vagrancy (Cross et al., 2010; Galvao, 2012). Additionally the City has created its own voucher programme called Give Responsibly, which utilises many of the same NGO partners as U-turn, instead of partnering with U-turn and supporting a programme already in motion (giveresponsibly.co.za, accessed 24 June 2013). This may nevertheless prove to benefit the organisation in the long term with growing awareness of using vouchers as an as an alternative to cash-based hand-outs. It remains to be seen, however if their clients, like clients of other service providers, will benefit from increased competition.
In contrast to the actions of the local government of Cape Town which support U-turn indirectly with aligned programmes and directly through the provision of a venue to provide care, the national government has reduced support by removing the allocation of Lotto grant money to the organisation, which accounts for 60% of the loss incurred by the organisation in 2012. Additionally, a recent policy change of provincial hospitals affected their patients by shifting focus from dental care to broader HIV programmes. The latter, although an understandable change in view of the wider scale of HIV incidence, still has an impact on the lives of the homeless within Cape Town as illustrated in my journal extract from 6th March 2013 (below).
It is important to note that very few nations have successfully eliminated homelessness, irrespective of the social safety nets in place. In fact, it is a growing problem in the European Union, USA, Canada, Japan and Australia. These are all first world, highly developed countries, with extensive social care and programmes to eradicate poverty, more richly resourced than South Africa is (Cross et al., 2010; Schout et al., 2011; Van Laere & Withers, 2008). In the South African context of unemployment and inequality described above, poverty features more substantially than the mental illness which is a significant factor in European homelessness (Schout et al., 2011; Seager & Tamasane, 2010; Van Laere & Withers, 2008).
The community, the organisation and the client
In contrast to the local government and organisations such as U-turn that are making an attempt at providing care to the homeless, the wider local community needs to be more involved. Privileged irresponsibility, discussed above, as posited by Tronto (1993), is prevalent, as well as the persistent opinion that blames the homeless for crime and drug use and for not trying. Tronto (1993) outlines what she calls a "disdain for care-receivers", the view that people that who needs are seen as being "needy", being less autonomous, less capable and thus as pitiful because they require help. Once they have become regarded this way, it becomes difficult for others to acknowledge their needs as actual needs. This presents as numbness to the plight of others, the public becoming inured to the needs of others. As such, the homeless become faceless, allowing a carelessness that comes from anonymity.
In the light of this, if U-turn and similar organisations do not act, then the needs of the homeless will not be addressed. This fact raises the issue of competence that will be discussed in following sections. If they were to cease an imperfect service, then that need would cease to be met at all, even if that service had been previously executed imperfectly. U-turn has assumed this responsibility, on the basis of the Christian ethic, as a faith-based organisation to care for the poor. U-turn originated from individuals working from within the church and then grew into a larger care organisation. The church has a biblically-based responsibility (83 references in the Old and New Testaments in the Bible) to care for the poor. The community supports the church and its endeavours through this ethic, and the church in turn holds itself responsible for the caring of the poor when this is possible within its resources, in this case by providing vouchers to be redeemed at U-turn. The organisation continually motivates individuals, companies and community institutions to care and to co-ordinate their donations into a usable service to benefit the homeless and those at risk of being homeless (U-Turn Annual Report, 2012).
Simultaneously, a client-centred treatment model was developed (Schultz & Buys, 2011), involving demonstration of input by the clients. Stated more plainly, nobody is helped at U-turn without his or her own tangible effort. To receive meals and clothing for example, there is payment by a voucher system in place; these vouchers may be donated, but can also be earned through work at the organisation. As such, the organisation encourages reciprocal responsibility, using a cycle of give and take to ideally transform the lives of clients. The following journal extract illustrates the centrality of the voucher system, the firmness of the rules within the setting and the clear expectation of moral behaviour from clients. In addition, this shows the intention to promote the internalisation of organisational values and the engendering of the client's responsibility, at least in part, for their own care.
6th June 2012:
Then a man came in late, gave a name for the register and stood around.
"Where is your voucher? " ask Johnny and Robert.
He says nothing.
''Then you must leave. "
Another client gives him a voucher.
"You must not do that, " says Johnny to the first client, "You must come in and say you do not have a voucher. Do not hope we will forget to ask and you can slink past."
Every client's progress is monitored via the use of a computer program (Salesforce Foundation, 2011) to track progress through the three phases of re-entry into the community. This program represents a form of internal accountability at the organisational level, allowing the organisation to evaluate its own effectiveness and the level of transformative care it is providing. This, however, is in stark contrast to the difficulties experienced when taking the register at particular locations, as shown in the journal extracts below:
13th June 2012:
As usual doing the register is vague because the people speak softly, do not tell me whether they have been there this week or not and take long to help me find their names.
20th June 2012
At the register, one man insisted he was John Black. "A pseudonym for a street person? " I ask.
"Yes because they abuse the facilities and get thrown out, " says Robert. "That is why it is so difficult to count the homeless; they are a migrant population, moving from service to service. "
By providing the service that it does, U-turn also shows responsibility towards the community. It is possible to suspend hostility when there is action to be taken and by becoming visible, especially through the promotion of its food and clothing vouchers; Uturn has provided intolerant members of the public an opportunity to steer the homeless away from the streets. A constructive outlet has also been given to the genuinely philanthropic individuals who intend to assist people in need but do not know how. Uturn has assumed a responsibility and this is to be commended, but subsequent to taking up this baton they have the responsibility to see it delivered and ensure their task is successful. Their ability to do this, however, is problematic for a number of reasons discussed in the following section.
POSSESSING THE COMPETENCE TO CARE EFFECTIVELY
In the care-giving phase the importance of competence arises as a moral question (Tronto, 1993). In terms of the scope of the homeless in their numbers, U-turn served 944 clients (Salesforce Foundation, 2011). The organisation cannot be expected to serve the full population of street people in Cape Town, estimated at 7,000 by the Social Development section of the Cape Town City Council in 2013. Structural changes at governmental policy level towards promoting job creation and housing would assist street people at a national level, but to reach a sufficient level for all would also be considered utopian (Naidoo, 2010). Even with the largest shelter in the Southern Hemisphere, U-turn is not able to give a place to all (Salesforce Foundation, 2011).
Internal competence of U-Turn
U-turn has 14 staff members in the organisation and four donation programmes. Professionally and experientially, the staff are well equipped for their positions. The reentry programmes have been designed in phases and are continuously monitored. Cooperation and co-ordination with the wider community take place actively. Research on the state of the art in entrepreneurial transformation of street people has been carried out and also implemented at U-turn (Schultz & Buys, 2011).
As the U-turn services grew, co-ordination with other local institutions was established, involving all the organisations serving the homeless in Cape Town. Monthly planning meetings are now held and the municipality has employed a full-time co-coordinator for street people, who has direct access to emergency help from formal systems of the police and hospitals as well as from the informal sector. This kind of community development exemplifies skills in neighbourhood work as typified by Henderson and Thomas (2001). Tronto (1993) argues similarly, as does Sanchez (2010), that members of the community who are closer to the level of those in need of care are potentially better able to provide that care.
The vast majority of clients simply arrive for a meal and then depart, seldom progressing along the organisation's desired trajectory. Of the 944 clients served in 2012, 45% came only once (U-Turn Annual Report, 2012). As such, U-turn is ultimately failing to deliver its ideal of transformative care. For those remaining in Phase 1, according to the empirical evidence, there is little or no internalisation of values of the organisation by the clients, no change in self-image nor an increase in religious beliefs. Almost half of clients simply move on after the first warm meal. The clients tend to have an external locus of control, focusing solely on their immediate survival needs: their next meal or where they will sleep - typically out in the cold, as Cape Town's shelters cannot accommodate all and also require co-operation from clients in terms of rules and behaviour, which is not always forthcoming.
Competence restricted by environment
It is important to frame ethical questions of competence to take into account context (Tronto, 1993:134). The competence of this organisation is dependent on the competence of its network as a whole. The amount of shelter, food and clothing is dependent on availability and donation as shown in my journal extract below:
6th March 2013
"I distributed fruits - lots of apples, which our guys cannot eat due to the absence of teeth (my earlier approach to the Community Dentistry Department led to the reply that the state has prioritised HIV/Aids treatment and dentures are not available). I laughed with Robert; can we ask the schools not to provide apples but other soft fruit instead? " He does not reply.
At least part of the work hours required to service the clients at the soup kitchen are dependent on volunteers. Awareness and marketing only achieve so much within a community, which in turn leads back to the question of broader responsibility of the local community and larger society.
At U-turn clients live in places ranging from a prefabricated house (owned and paid for by someone else) through a tent pitched permanently in the nearby forest, to whatever sheltered position (under a bridge or a park bench) they can find in a public location, generally referred to as "the street". The difficulty in providing shelter is a significant reason for clients not progressing through the phases. As mentioned in an extract to follow, if clients do not find shelter, they do not progress through the programme.
11th June 2012:
''How can you sleep in the cold? " I ask for the umpteenth time.
"In Rondebosch [a neighbouring suburb, 4 km distant]. I find a place there."
"Is it under trees?" I ask. "Yes under trees."
Not the subway or bridge then. As they leave I say - sleep warm - thinking regretfully that I am always told to sleep well. Our clients are not even warm let alone well.
20th March 2013:
No one has jobs. We spoke about Straatwerk [an informal organisation that offers payment for cleaning streets on a daily basis]. "Sometimes they don't have jobs, " says Johnny. I am getting used to this feeling of offering nothing except food. There were several rounds of helpings for 11 people and they queued and I served until there was nothing left. The clients thanked me and I realise that I am also conveying respect to them.
A question often asked, by faithful churchgoers as well as other donors to the organisation centres on the likelihood of assistance perpetuating a problem. Conversely, if U-turn were not to feed the homeless, would they obtain jobs in order to survive? According to Stats SA (2013), the unemployment rate in South Africa is 25%, this number belies that fact that these workers are often more skilled, able-bodied and of sounder temperament than the homeless. Since the financial crisis of 2008 unemployment has risen globally, within the UK (7.8%), USA (9.7%) and EU (9.3%), and there are a number of these unemployed who are very unlikely to find employment, because of skill deficits, attitudinal problems and structural unemployment (Schout et al., 2011). These figures pertain to developed countries with less than 10% unemployment; as one can conclude with 1 in 4 unemployed, the situation in South Africa is far more extreme. This is further emphasised by the fact that even within low-unemployment, highly developed economies, homelessness remains a problem, such as in the European Union, USA, Canada, Japan and Australia (Cross et al., 2010; Van Laere & Withers, 2008), highlighting the macro-economic environment that U-turn must operate within.
Competence restricted by resources
U-turn's Phase 2, which stresses consistent employment, is fighting an uphill battle, giving some indication as to why there are large numbers of clients working within U-turn-managed projects themselves (U-Turn Annual Report, 2012). Sometimes care will be inadequate because the resources available to provide care are inadequate (Tronto, 1993). Because of changes in Phase 2 of the programme, specifically adjustments to their NuLife programme,3 capacity has been reduced. U-turn is now allowing clients to remain within NuLife as long as they need to, instead of ejecting them after six months. This change is better for the clients, as it allows them a higher chance of re-entry into society; however, it also reduces the number of clients that it is possible to cater for by slowing the throughput. Furthermore, up to 70% of clients have some form of drug dependence (Muizenberg Improvement District, 2009). Hence, the fact that U-turn has only 14 work rehabilitation places is another bottleneck that illustrates, at least partially, why only 12 clients graduated from the programme in 2012. Two thirds of graduating clients were still employed after six months, indicating the success possible if clients progress through the entire programme. However, while expansion is quite evidently needed, the organisation is at present running out of funding, operating at a loss that it cannot sustain over the longer term (U-Turn Annual Report, 2012).
In Phases 2 and 3 there is evidence of an improved self-image, incorporation of values and an appreciation for the work that U-turn has undertaken. This is partly evinced by the fact that many of the clients who graduate continue to work within the organisation. This in turn highlights both the difficulty of the external employment environment and the esteem in which graduating clients hold U-Turn. Johnny, as discussed above, is one such client who, after graduating, remained with the organisation, persevering through many difficult challenges faced by those living in the poorest areas of Cape Town to provide care. Johnny is doing this work on the basis of his belief and is immersed in the culture of the organisation. He is indeed appreciative not only of the researcher's contribution as a volunteer to U-turn, but also as a person helping him rather than improving client behaviour.
ADEQUACY OF CARE AS A MEASURE OF ITS SUCCESS
Tronto (1993) highlights the importance of continually questioning the delivery of care in order to make certain that caring work is done with competence, particularly if the adequacy of care given is a measure of its success (Tronto, 1993). It is not sufficient to simply provide care - it must also be well provided. Unpacking the suspicion that there is little possibility of clients progressing through the programme and that the organisation was simply providing food necessitates an analysis of that provision. The pattern of voucher redemption, however, is complex as the chart below indicates. Clients redeemed vouchers both in waves and in overall decreasing numbers in 2012.4 This in contrast to growing public awareness of this programme and others started by the city (Galvao, 2012). The Give Responsibly programme is competing both for a share of public awareness and their funding via the competing voucher systems. With the backing of the City and a system of easier redemption (possible at any Pick 'n Pay store around the city), this poses a threat to U-turn's own programme, threatening their basic service, provision of food, even further. Almost 30% of U-turn vouchers are not redeemed, possibly highlighting the difficulty in redeeming them at U-turn's only two locations of food provision in the suburbs of Cape Town. Furthermore, U-turn's voucher programme constituted the largest loss for the organisation: R125,000 in 2012. There is a positive observation in that 23 people were placed in shelters as a result of contact made from this programme.
U-turn may lack the competence to provide the transformative care it is seeking to provide, based on limited resources, a network that is over taxed by demand, and a lack of responsiveness to the situation. The organisation may also be providing the wrong kind of care, such as IT Training, and thus wasting resources. The Cape Town care situation is both difficult and complex, given the high unemployment, extreme inequality and the pervasive availability of low-cost highly addictive drugs, which explains the lower than anticipated performance. However, it may also be that the goal of transformative care is too lofty, given the inadequate resources and the poor economic situation. The low rate of exiting homelessness is well described in both the international and the local literature presented above. The commitment to provide care, regardless of the level, is something to be lauded. According to Tronto (1993), part of the responsibility of care giving is to provide an adequate level of care, as poorly provided care might itself be damaging. In this case, the provision to meet basic needs cannot be considered damaging, as there is no evidence that it disempowers client capacity. This condition relates to Tronto's next category.
RESPONSIVENESS TO CARE
"By its nature care is concerned with conditions of vulnerability and inequality. " (Tronto, 1993:134)
Responsiveness refers to the manner in which the care receiver responds to the care provided. To be in a position where one's autonomy and self-supporting capacity is questioned, and requiring of care, is to be in a position of vulnerability. There is a danger faced by people within this position that the caregiver may come to define the needs of the vulnerable. Tronto (1993) stated that responsiveness requires that the caregivers do not place themselves in another's position to understand, but rather to consider that position as the other describes it (Tronto, 1993). She warns further that the act of "taking care of" a need by implementing a solution without concern for the outcome or end result appears prevalent in bureaucracies (Tronto, 1993).
BALANCING THE NEEDS OF CARE GIVER AND CARE RECEIVER
On a macro level responsiveness becomes problematic and requires the averaging of data or inputs, thus becoming inflexible to the needs of individual clients on a micro level. This can be seen in the frustration expressed by a client in the following journal extract:
February 20th 2013:
"The thing is, " Albert says quietly to me, "Places like U-turn expect you to do what they want. No-one asks what you want. "
On the micro level, when providing care for an individual's specific needs, the solution required is often more tailored. Bozalek and Hooyman (2013) state that responsiveness should be considered in broader terms, such as asking how is the client responding to the care and how does this affect the quality of the care for both parties? There is a need to balance the needs of the care giver and the care receiver. This is particularly relevant in terms of the security of care givers, where U-turn must balance the needs of the care receiver with the wellbeing of the care givers. Care givers are frequently the target of violence when the homeless, accustomed to roaming the streets and searching for survival strategies, tend to disregard conventional norms and so verbally and physically abuse those in contact with them, as occurred several times during my period of participant-observation. Consequently, rules for punctuality and consideration of others are strictly upheld by caregiving organisations in the community. Galvao (2012) reports the case of two clients who attended the newly set up City of Cape Town assessment centre. Both clients were determined to leave addiction behind them, were successfully admitted to the city's programme and a rehabilitation programme, only to abandon these programmes because they found the rules too restrictive. At U-turn clients express their reluctance to comply with the rules of the shelters, but a fixed abode is a necessary condition for Phase 2. U-Turn's assumption is that their programme is acceptable and should be adhered to. It is possible that feelings of powerlessness increase the likelihood of resistance by clients to control by care givers, wanting to be able to effect decisions about their lives, even to their own detriment. Schout et al. (2011) discuss a situation in the Netherlands where care providers limit their efforts, based on the assumption that clients will be likely to ignore their instructions or miss appointments. The ideal situation of mutual effort is not present, nor the reciprocal responsibility discussed earlier. The desirable situation occurs where a care giver tentatively guides a client without being forceful, but still applying some visible guidance. This is a classic situation of motivation versus punishment; the latter simply does not work for members of society who shirk customary behaviours, while for the former it is a difficult option as the majority of clients have drug dependence, as evidenced by Seager and Tamasane's national estimate in 2010 and local reports by the Muizenberg Improvement District (2009), Galvao (2012) and Elim Night Shelter Organisation (2013). Responsiveness within care for the homeless is a dance with a reluctant partner, sometimes the caregivers must lead and other times they must follow. The decisions around this relates to attentiveness to responsiveness in each case.
QUANTIFYING RESPONSIVENESS AT U-TURN
In quantifying responsiveness at U-turn, figures produced by the organisation in 2012 reveal that of those who started the second phase of the rehabilitation programme, 70% complete the 6-month period. One hundred per cent of those who completed the programme found a job and 66% remain in employment for longer than 6 months (UTurn Annual Report, 2012).
Table 2 presents the racial population of U-Turn in relationship to data from the census surrounding typical factors associated with homelessness.
From the Cape Town 20115 census data extracted from Stats SA, the racial population percentages are Black (38.6%), Coloured (42.4%) and White (15.7%), which indicates that U-turn's client base (as a 13.5% sample of the homeless population of Cape Town) is largely representative of the city's population in terms of race. Given that the black population of South Africa is substantially poorer and the white population typically more affluent (Biko, 2013; Mbeki, 2011), there should be more black clients and fewer white clients, if poverty were to be taken as the primary factor. This raises questions about the arguments on the impact of poverty, previous disadvantage based on race and present policy on the homeless population. As the total number of clients has declined for three years and only 8% of clients come twice a month, there is an indication that basic needs are being met elsewhere. Where that is can only be a matter of speculation and is difficult to establish. Informal employment is not officially recorded and the homeless themselves do not readily provide information about their situation, as found in this research and in that of others such as Cross et al. (2010) and Moyo et al. (2015).
The ratio of specific U-turn client population groups to the unemployment percentage for each population group indicates there are more homeless people from the Coloured and White groups than simple unemployment or resulting poverty would suggest there should be. The deduction from these figures shows that higher unemployment and previous disadvantage as a result of racial policy do not sufficiently account for homelessness. Cross et al. (2010) support this by stating that homelessness is not simply a result of poverty, but of multiple systems of socio-economic factors.
When taking into account that, in contrast to the above self-expressed figures, an estimated 84% of U-turn's clients have some form of substance dependence (Elim Night Shelter Organisation, 2013) life sustenance becomes problematic. This substance dependence also suggests why so few clients graduate or why so many do not return. Even the present level of care is unsustainable, with the organisation running out of funds, recording a second consecutive operating loss and the exhaustion of past years' savings (U-Turn Annual Report, 2012). It is perhaps prudent for the organisation to scale down their operations in order to reliably provide a lower level of service. Is it then best for U-turn to reduce their scope and focus on rather mitigating suffering and providing for the most basic of needs, instead of attempting in vain to feed, clothe, house, educate and empower the most downtrodden and recalcitrant population in South Africa? This would require the stakeholders in the organisation to admit what may in fact undermine the current level of care, namely that they simply cannot sustain it nor effect a lasting change within the limits of their resources and context.
In qualifying the progress of clients we have to realise that a change in self-orientation is required for clients to think of themselves as settled people with the long-term plans involved in regular employment. Even those clients who are thrust into the streets without being responsible for the choice, as a result of retrenchment for example, once on the street, life orientation changes towards the addressing immediate situation and results in damage to behaviour through, for example, substance dependence. The conclusion is that service providers have not yet found a way to measure or describe a change in self-orientation; we have only found that time encourages stability - time with monitoring of a controlled routine and care (U-Turn Annual Report, 2012).
Initially I was a dissatisfied observer of the lack of client progress through the phases envisaged by the organisation; however, it soon became difficult to suggest change or critique clients' actions in the light of the odds they face, both internally with self-image and externally with community resources. As I have spent a longer time engaged with the situation, I have become more accepting of the futility at times present, while recognising a rhythm arising from the organisation's attentiveness and client responsiveness applied to care giving. My sense of rhythm could be described in terms of Tronto's notion of care becoming habitual. It is essential, though, as Tronto (1993) discusses, that the care provided be critically examined in order to judge its adequacy and ultimately its level of success. In overview, notwithstanding the unchanging nature in their living circumstances, the homeless people appreciate the care they receive and they welcome the food and the respect they are given. Clients of U-turn are vocal on this subject and regulars return often (See Table 1).
CONCLUSION
"Care as a practice involves more than simply good intentions." (Tronto, 1993:136)
Tronto (1993) argues that those who engage in the care process must continuously make difficult decisions. They must judge which needs are most important, what is the best way to meet these needs with their limited resources, while taking into account the responses of their care receivers. In U-turn's context judgment involves what services they provide, at what level and for how long, given the financial constraints they are facing. They must decide whether to slow expansion to reduce expenses, but at the same time then maintain the present bottleneck, one which is created by a lack of shelter, rehabilitation placements and internal work positions. The decision to increase capacity leads to the risk of having to raise more funds from a community in general not receptive to the needs of its clients.
U-turn's three-phased approach needs to be reconsidered in the light of the evolving situation at the lowest level of society, which constitutes their clients in or before Phase 1. Their approach of moving to higher level phases represents an ideal situation that is at odds with what is happening on a day-to-day basis. This disconnect is at a transformative level, leading to a waste of resources and a poor application of professional and volunteered skills. U-turn would benefit from a re-evaluation of the macro and micro situations within South Africa. At present there is at best a breakdown in their feedback cycle, preventing the adjustment of their programme to suit the emergent conditions. U-turn is a significantly technology-minded organisation utilising and implementing for other NGOs a cloud-based method of tracking clients and services delivered. This technology-based positioning, although presumably effective at a higher level within the organisation, or perhaps internationally in a predominantly first world setting, may blind the organisation to simpler measures that could assist with clients. As such, it requires the refocusing of resources on more sustainable measures closer to the level of clients such as manual labour, as a means to reduce costs and employ clients. Another option is for the organisation to utilise its technology focus to better engage with potential donors and employers through social media campaigns.
At worst it involves resigning themselves to the knowledge that there is little hope in assisting these clients beyond simply caring for their basic and immediate needs of survival. Possibly the knowledge on both ends is that there is nowhere for clients to go if the organisation succeeds in lifting them back into society. According to Tronto (1993), however, regardless of success or failure, the moral imperative to support and care for those in need remains. Given that an organisation like U-turn takes the responsibility to meet the needs of the homeless, there is the further responsibility, set by U-Turn's donors, that if care is to be provided, it should aim for an adequate level. The question then is what is an adequate level - one that prevents starvation and succumbing to the elements, but essentially perpetuates a life on the street? U-turn may be failing in their aim of providing transformative care in that there is a low number of clients graduating from their system, yet there is growing public awareness of the needs of the homeless (Galvao, 2012), as evinced by the discussions with community members and the introduction of similar programmes such as Give Responsibly. With this growing awareness comes the possibility that additional resources may become available. There is another view, based on the biblical responsibility to care for the poor, which accepts that some have found that their life on the streets is the best option for them and that the community is prepared to support this, foregoing a transformative objective. This version is consistent with Tronto's first moral attribute of attentiveness in caring. The question then shifts to whether U-turn will buckle under growing financial pressure or endure in the hope of a brighter future that may not be forthcoming? As a Christian faith-based organisation, they are more likely to take the second option. In their own words:
"In a way, our work is only just starting." (U-Turn Annual Report, 2013:13)
REFERENCES
BABBIE, E. & MOUTON, J. 2001. The practice of social research. Cape Town: Oxford University Press. [ Links ]
BARNES, M. 2012. Care in everyday life: an ethic of care in practice. Bristol: Policy Press. [ Links ]
BIKO, H. 2013. The great African society: a plan for a nation gone astray. Johannesburg: Jonathan Ball. [ Links ]
BOZALEK, V. & HOOYMAN, N.R. 2013. Ageing and intergenerational care: critical/political ethics of care and feminist gerontology perspectives. Agenda: Empowering Women for Gender Equity. doi. 10.1080/10130950.2012.755378. [ Links ]
CROSS, C., SEAGER, J., ERASMUS, J., WARD, C. & O'DONOVAN, M. 2010. Skeletons at the feast: a review of street homelessness in South Africa and other world regions. Development Southern Africa, 27(1):5-20. [ Links ]
DEPARTMENT OF SOCIAL DEVELOPMENT. 2013. Street people policy. Unpublished report. [ Links ]
ELIM NIGHT SHELTER ORGANISATION 2013. Interview with co-ordinator. ESOCSCI (New Zealand). 2012. [Online] Available: http://www.esocsci.org.nz/networks/care-ethics/. [ Links ]
FINE, G.A. 2003. Towards a peopled ethnography developing theory from group life. Ethnography, 4(1):41-60. [ Links ]
FOUCHÉ, C.B. 2011. Research strategies. In: DE VOS, A.S., STRYDOM, H., FOUCHÉ, C.B. & DELPORT, C.S.L. Research at grass roots: for the social sciences and human service professions. Pretoria: Van Schaik Publishers. [ Links ]
GALVAO, R. 2012. Homelessness. The Big Issue, 11 May - 01 June, 2012. [ Links ]
GOLD, R.L. 1958. Roles in sociological field observations. Social Forces, 36:217-223. [ Links ]
GRAY, M. & LOMBARD, A. 2008. The post-1994 transformation of social work in South Africa. International Journal of Social Welfare, (17): 133-145. [ Links ]
GUMEDE, W. 2012. Restless nation - making sense of troubled times. Cape Town: Umuzi. [ Links ]
HENDERSON, P. & THOMAS, D. 2001. Skills in neighbourhood work. London: Taylor and Francis. [ Links ]
HOFFMAN, P. 2013. Service delivery: constraints, corruption and cadres. In: PLAATJIES, D. (ed) Protecting the inheritance: governance & public accountability in democratic South Africa. Johannesburg: Jacana. [ Links ]
JANSEN, J. 2009. Knowledge in the blood: confronting race and the apartheid past. Cape Town: UCT Press. [ Links ]
LUIZ, J.M. 2013. Economic governance, markets and public accountability: a freedom constraint? In: PLAATJIES, D. (ed) Protecting the inheritance: governance & public accountability in democratic South Africa. Johannesburg: Jacana. [ Links ]
MacDONALD, R. 1997. Dangerous youth and the dangerous class. In: MacDONALD, R. (ed) Youth, the 'underclass' and social exclusion. London: Routledge. [ Links ]
MARAIS, D. 2012. The problem of having a home. [Online] Available: http://homeless.org.za/apps/wordpress/?page_id=1514 [Accessed: 24/05/2013]. [ Links ]
MBEKI, M. 2011. Introduction. In: MBEKI, M. (ed) Advocates for change: how to overcome Africa's challenges. Johannesburg: Picador Africa. [ Links ]
MOHAMED, S. 2011. Negative trends in the South African economy: how should these be overcome. In: MBEKI, M. (ed) Advocates for change: how to overcome Africa's challenges. Johannesburg: Picador Africa. [ Links ]
MOYO, U., PATEL, L. & ROSS, E. 2015. Homelessness and mental illness in Hillbrow, South Africa: a situation analysis. Social Work/Maatskaplike Werk, 51(1):1-21. [ Links ]
MUIZENBERG IMPROVEMENT DISTRICT. 2009. Street people. Unpublished report. [ Links ]
NAIDOO, V. 2010. Government responses to street homelessness in South Africa. Development Southern Africa, 27(1):129-140. [ Links ]
PATEL, L. 2005. Social welfare and social development in South Africa. Cape Town: Oxford University Press. [ Links ]
PILLAY, D. 2013. Ecology, economy and labour. In: DANIEL, J., NAIDOO, P., PILLAY, D. & SOUTHALL, R. (eds) New South African Review 3: the Second Phase - Tragedy or Farce? Johannesburg: Wits University Press. [ Links ]
PLAATJIES, D. (ed) 2013. Protecting the inheritance: governance & public accountability in democratic South Africa. Johannesburg: Jacana. [ Links ]
POLLACK, M. 2012. City opens three new assessment centres for the homeless. [Online] Available: http://www.capetown.gov.za/en/Pages/Cityopensthreenewassessmentcentresforthehomeless.aspx [Accessed: 12/08/2013]. [ Links ]
RAMLAGAN, S., PELTZER, K. & MATSEKE, G. 2010. Epidemiology of drug abuse treatment in South Africa. South African Journal of Psychiatry, 16(2):40-49. [ Links ]
RAMPHELE, M. 2008. Laying ghosts to rest: dilemmas of the transformation in South Africa. Cape Town: Tafelberg. [ Links ]
RAMPHELE, M. 2012. Conversations with my sons and daughters. Cape Town: UCT Press. [ Links ]
SALESFORCE FOUNDATION. 2011. U-Turn, harnessing the power of Salesforce CRM to help uplift street people in Africa. [Online] Available: http://homeless.org.za/apps/wordpress/?page_id=1839 [Accessed: 26/05/2013]. [ Links ]
SANCHEZ, D. 2010. Civil society responses to homelessness. Development Southern Africa, 27(1):101-110. [ Links ]
SCHOUT, G., DE JONG, D. & ZEELEN, J. 2011. Beyond care avoidance and care paralysis: theorizing public mental health care. Sociology. [Online] Available: http://soc.sagepub.com/content/45/4/665. [ Links ]
SCHULTZ, V. & BUYS, A. 2011. From dependency to dignity: the A2B entrepreneurial transformation movement. Pretoria: A2B Publishers. [ Links ]
SEAGER, J.R. & TAMASANE, T. 2010. Health and well-being of the homeless. Development Southern Africa, 27(1):63-83. [ Links ]
SEWPAUL, V. 2005. A structural social justice approach to family policy: a critique of the draft South African family policy. Social Work/Maatskaplike Werk, 41(4):310-322. [ Links ]
SSPARC, University of Brighton, 2012. [Online] Available: http://www.brighton.ac.uk/sass/research/conferences/critical-care.php. [ Links ]
STATS SA. 2013. Census Fact Sheet 2013. [Online] Available: http://www.statssa.gov.za/Census2013/Products.asp [Accessed: 19/05/2013]. [ Links ]
TRONTO, J. 1993. Moral boundaries: a political argument for an ethic of care. London: Taylor and Francis. [ Links ]
U-TURN ANNUAL REPORT. 2012. [Online] Available: http://homeless.org.za/apps/wordpress/wp-content/uploads/2013/02/2012-annual-report.pdf [Accessed: 29/04/2013]. [ Links ]
U-TURN ANNUAL REPORT. 2013. [Online] Available: http://homeless.org.za/apps/wordpress/wp-content/uploads/2014/02/2013-annual-report.pdf [Accessed: 01/02/2014]. U-TURN DATABASE. 2013. Unpublished report. [ Links ]
VAN LAERE, I. & WITHERS, J. 2008. Integrated care for homeless people. Sharing knowledge and experience in practice, education and research: results of the networking efforts to find homeless health workers. European Journal of Public Health, 18(1):5-6. [ Links ]
WEBSTER, E. 2010. There shall be work and security: Utopian thinking or a necessary condition for development and social cohesion? Transformation: Critical Perspectives on Southern Africa, 72/73:225-246. [ Links ]
WILSON, F. 2010. Dinosaurs, diamonds and democracy - a short, short history of South Africa. Cape Town: Random House Struik. [ Links ]
WILSON, R. n.d. The graffiti clean-up project in Cape Town. Unpublished report. [ Links ]
1 Names have been changed to preserve anonymity of respondents.
2 Some ad hoc work is available in the form of car guarding and street vendor assistance, particularly at special events.
3 Supported employment within U-turn's charity shops.
4 Data from December (114 vouchers redeemed) were excluded in order not to skew the results.
5 There is, however, a noticeably higher percentage of Coloureds and a lower percentage of Blacks and Whites in 2012. Comparisons have been made on both 2011 datasets.


{kind=link}
{kind=link}
{kind=link}