










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.51 n.1 Stellenbosch 2015
http://dx.doi.org/51-1-428
ARTICLES
Beyond the bio-medical orthodoxies: Socio-economic and attitudinal impediments to exclusive breast feeding in rural Zimbabwe and possible roles of social workers and interventions to promote its uptake
Munyaradzi MuchachaI; Edmos MthetwaII
IPost Graduate Student, University of KwaZulu-Natal, Durban, South Africa
IIUniversity of Zimbabwe School of Social Work, Harare, Zimbabwe
ABSTRACT
Exclusive breastfeeding (EBF) which is one of the major remedies to infant and child mortality, is largely underutilised especially in rural Zimbabwe. EBF is a physiological process which transpires in a specific socio- economic milieu, to that end this paper labours to investigate the socio- economic factors militating against its uptake. Using the mixed methodology the paper reveals that issues such as poverty-gender inequalities, social and cultural beliefs are critical obstacles against EBF infant feeding practice. It is within the context of these socio-economic barriers this paper argues that social workers have a key role in facilitating EBF.
INTRODUCTION
The field of health is shifting from a disease model to a health model which acknowledges the influence of social factors in health outcomes (Bandura, 2004). This makes the profession of social work an indispensable profession in facilitating health promotion because of the inherent appreciation of social issues by the profession (IFSW, 2008). There is however a general propensity to side-line the profession when it comes to health care provision in Zimbabwe (Kaseke, 1991). Resultantly, most of the programmes spearheaded by the different players in the health sector tend to flop when it comes to acceptability by the communities within which they are implemented. It is from this understanding that this paper is intended to bring to the fore the role of social workers in the sustainment of health programmes in Zimbabwe utilising the case of Exclusive Breast Feeding (EBF).
The infant mortality rate in Zimbabwe stands at 97 deaths per 1,000; it is an acute problem and a threat to the realisation of the Millennium Development Goals, particularly goal number 4, which aims to reduce child mortality (Ministry of Health and Child Welfare, 2010). Paradoxically one of the chief interventions recommended in this social catastrophe (Moland, Paoli, Sellen, Esterik, Leshabari & Blystad, 2010) is free, accessible, sustainable and not far beyond the reach of many rural women, but is nevertheless being underutilised (Jenkins, Tavengwa, Chasekwa, Chatora, Taruberekera, Mushayi, Madzima & Mbuya, 2011).
A large body of evidence demonstrates the benefits of EBF as infant feeding practice for child survival, growth and development (Jenkins et al., 2011; Koyanagi, Humphrey & Moulton, 2009; Wieslaw & Frederica, 2011). This is premised on its high immunological, nutritional and hygienic value as compared to other liquids, solids and bottled infant milk formulas (World Health Organisation, 2003). Lack of EBF is associated with high incidences of diseases such as diarrhoea, pneumonia, bacterial meningitis, bacteraemia, respiratory tract infection, necrotising entercolitis and malnutrition (World Health Organisation, 2001). These ailments are in turn responsible for high morbidity and mortality as well as for poor school performance later, and impaired intellectual and social development (Jenkins et al., 2011; Jones, Steketee, Black, Bhutta, Morris & the Bellagio Child Survival Study Group, 2003; World Health Organisation, 2003).
EBF is defined by the World Health Organisation as "giving breast milk only to infants from 0-6 months and not feeding any food or liquid, not even water, with the exception of drops or syrups consisting of vitamins, mineral supplements or medicine only as recommended by the health workers" (World Health Organisation, 2001:28).
The 2003 Lancet series on child survival identified the promotion of EBF infant feeding practice during the first six months of life and continued breastfeeding for up to 12 months as the single most effective preventive public health intervention for reducing mortality among children aged five years and below (Jones et al., 2003). More recently, the 2008 Lancet series on maternal and child under-nutrition estimated that 1.06 million child deaths (ten percent of all mortality in children aged 5 years) are attributable to non-EBF in the first six months of life (Jenkins et al., 2011).
The Ministry of Health and Child Care in Zimbabwe recommends and promotes EBF as the most appropriate infant feeding practice for children from 0-6 months of age. Despite efforts by the Ministry to increase EBF uptake, its practice is still very low (Jenkins et al., 2011; Save the children, 2009). According to the National Nutrition Survey of 2010 the current national EBF stands at a low rate of five percent (Ministry of Health and Child Welfare, 2010). The Multiple Indicator Monitoring Survey of 2009 provides a higher national rate of 21%, with a higher proportion of 29% of infants in urban areas being exclusively breastfed compared to 26% in rural areas (UNICEF, 2009).
Breastfeeding is a complex process governed by psychological and physiological factors, which are in turn conditioned by a wide spectrum of environmental, socioeconomic and cultural circumstances (Jenkins et al., 2011; Save the children, 2009). It is against this background that this study investigates the socio-economic and attitudinal factors that militate against the uptake of EBF. Further to that the paper provide a niche and impetus for social workers response utilizing their "social expertise". The involvement of social workers in primary health care is justified and mandated by the International Federation of Social Workers (IFSW) statement on health which proposed Primary Health Care as the key social work tool to promote "Population Health" by tackling social determinants of health (IFSW, 2008).
EBF is an infant's lifesaving interventions that falls into broader maternal child health primary health care interventions. The World Health Organization (1978) defines primary health care as an essential health care based on practical, scientifically sound and socially acceptable methods and technology made universally accessible to individuals and families in the community through their full participation and at a cost that the community and country can afford to maintain at every stage of their development in the spirit of self-reliance and self-determination. It forms an integral part both of the country's health system, of which it is the central function and main focus, and of the overall social and economic development of the community." (World Health Organisation, 1978).
THEORETICAL FRAMEWORK
The theoretical standpoint presented by Ajzen, which is the theory of planned behaviour, based on the research by Fishbein and Ajzen (1975), provided the conceptual framework for this study. The theory focuses on understanding people' s behaviour and its determinants, including the psychological and socio-economic determinants. The theory of planned behaviour for human action is guided by three factors:
- Behavioural beliefs, which are beliefs about probable outcomes of behaviour and the evaluations of those outcomes;
- Normative beliefs, which are beliefs about the normative expectations of others and motivation to comply with those expectations;
- Control beliefs, which are beliefs about the presence of factors that may aid or hinder performance of behaviour and the perceived power of those factors (Ajzen, 2006).
Each of these beliefs produces certain attitudes or perceptions. Behavioural beliefs create a particular attitude regarding behaviour, while normative beliefs lead to perceived subjective norms, and control beliefs produce perceived behavioural control. Attitude toward behaviour, perceived subjective norms and perceived behavioural control contribute towards the intention to perform an action (Ajzen, 2006). If understanding behaviour is the primary objective, then the factors determining the intention to perform that behaviour must be specified (Fishbein & Ajzen, 1975). For the purpose of this study, it refers to the factors that predict the actions and intention to breastfeed. The theory of planned behaviour explains the relationship between the intention to breastfeed, and the factors that affect a women's decision regarding breastfeeding. Attitudes, surrounding circumstances, subjective norms and perceived behavioural control all influence the intention to perform a certain behaviour, which in turn predicts the likelihood of a particular behaviour taking place.
The theory of planned behaviour not only provided the framework for this study, but it also served as a guide to identify the influence of significant others in determining behavioural change and the adoption of new health behaviours. Jenkins et al. (2011) note that older women and in-laws are perceived by mothers as good advisers, because of their knowledge of existing social norms and in this sense they influence the mother's infant feeding choices. This can be explained by the theory of planned behaviour that attitudes are determined by the society's perception of the desirability of one's action (Fishbein & Ajzen, 1975).
Perceived behavioural control refers to one's belief as to the ease and likelihood of success in performing certain behaviours (Ajzen, 2006). If mothers believe that EBF is difficult, constraining, not very helpful and socially unacceptable, they will typically not choose to breastfeed exclusively. Hindering socio-economic factors may also make the mother reach the conclusion that practising EBF is challenging and she may not start or continue practising it.
Subjective norms are the perceived social pressure to perform or not perform certain behaviours such as breastfeeding (Ajzen, 2006). Some of this pressure is overt and some is covert. Overt pressure can take many forms such as advice, attitudes, policies, laws and educational material. Covert pressure is very subtle and includes being in an environment where a particular infant feeding practice is dominant. In a Zimbabwean rural setup there are cultural expectations of women which govern their behaviour (Gelfand, 1985). Breastfeeding is one such behaviour that is influenced by subjective norms. Women who are raised and live in segments of society in which children are not exclusively breastfed are not likely to breastfeed. Gelfand (1985) asserts that, in rural Zimbabwe, the infant feeding practices were largely influenced by the existing social norms which were inculcated mostly by in-laws and grandmothers.
METHODOLOGY
The principal objective of the study was to ascertain the socio-economic and attitudinal barriers to EBF uptake among rural women in Zimbabwe and the major research question was: What are the socio-economic and attitudinal factors that militate against the uptake of EBF in rural Zimbabwe? The concurrent nested model of a mixed research methodology was employed and was identified by its use of one data-collection phase, during which both quantitative and qualitative data were collected simultaneously (Creswell, 2009). The study was carried out in Mataga Ward, Mberengwa District Midlands's province in Zimbabwe at Mataga Rural Health Centre.
The primary target group (the respondents) were mothers who had infants from 0-6 months accessing maternal and health services at Mataga Rural Health Centre during the data-collection month. The secondary target group was the Mataga Rural Health Centre health workers (nurses and village health workers), who these served as key informants and are referred to as such throughout this study. Availability sampling method was utilised to select 20 (100%) mothers to take part in the study, while health workers (two nurses and two village health workers) were selected through a purposive sampling technique. Village health workers are community-based volunteers who facilitate community based health practices. Ethical considerations such as voluntary and informed participation, debriefing, and confidentiality and anonymity were observed. The study was given ethical approval by the University of Zimbabwe School of Social Work Ethics Committee.
Data collection and analysis
An interview schedule composed of open-ended and closed questions was used to collect data from mothers, while an interview guide composed of open-ended questions was utilised to collect data from the health workers (nurses and village health workers). Quantitative data were analysed using the Statistical Package for Social Scientists, while qualitative data were analysed through content-coding procedures based on a set of predetermined themes of interest.
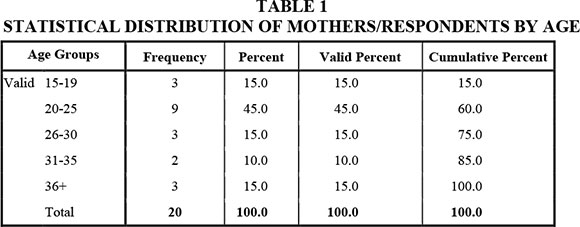
Table 1 shows the age distribution of mothers who participated in the study. Out of the 20 (100%) mothers interviewed, nine (45%, the largest proportion of mothers) were from the 20-25 age range; three (15%) respondents were within the 15-19 age range, while age groups 26-30 and 36+ had three respondents each. Two (10%) respondents belonged to the 31-35 age group. The high rate of mothers in the 20-25 age group confirms the findings of the Zimbabwe Demographic Health Survey of 2011, which reported a high fertility rate among women from the age of 20-25 (Zimbabwe National Statistical Agency, 2011).
LEVEL OF EDUCATION OF THE RESPONDENTS AND EBF PRACTICE
A large proportion of respondents (13, 65%) managed to reach primary level. Seven (35%) mothers managed to reach secondary level. The primary school attendance rate in this study tallies with the findings of the Multiple Indicator Monitoring Survey of 2009, which recorded a 99% primary education net attendance of the girl child in Zimbabwe (Gandure, 2009). Fourteen respondents only managed to complete the primary level of education. Seven had reached secondary school level. Five of the seven mothers (71%) who had secondary education managed to practise EBF. Eleven (55%) mothers who had no primary education did not exclusively breast feed. Only two (14%) respondents with primary education managed to practise EBF.
The above results show a higher prevalence of EBF among respondents with secondary education (71%) than with primary education (14%). The influence of education on the uptake of EBF was also recognised by all the nurses (key informants), who registered a high prevalence among mothers who have secondary education. Implicit in these results is that educating a girl child is likely to promote and sustain positive health behaviour in traditional communities.
Women in Zimbabwe have limited access to the means of production, hence their income and economic status is low (Gandure, 2009). As illustrated by Figure 1 above, there were very few women who earned more than $50 per month in Mataga. Among the 20 (100%) mothers who were interviewed, five (25%) had an income estimate of $5, four (20%) earned an estimate of $20, four (20%) earned an estimate of $50, three (15%) earned $100,while only two (10%) mothers earned more than $200.

These findings correspond with UNICEF (2009) findings that many women in rural areas are living far below the poverty line. Another influencing factor is that agricultural activities, which are the main source of livelihood in rural areas, have been hampered by vagaries of weather. According to the Multiple Indicator Monitoring Survey of 2009, wealth quintile or income influences the uptake of EBF (UNICEF, 2009).
EMPLOYMENT STATUS OF MOTHERS AND THE FATHERS.
This study found that unemployment is rife. Eighteen (90%) mothers and 13 (65%) fathers reported that they are not employed. Two (10%) mothers reported that they were self-employed. This confirms UNICEF (2009) findings of high unemployment rates among rural women in Zimbabwe. On a comparative note related to Figures 2 and 3, the unemployment rate was higher among the mothers than fathers by a margin of 24%. Ascertaining employment status is imperative in analysing the income and wealth quintiles of the family and its implications on EBF uptake.
EXCLUSIVE BREAST FEEDING RATES AMONG THE 20 MOTHERS IN MATAGA WARD
EBF rates in Zimbabwe are low especially in rural areas, as noted by the Multiple Indicator Monitoring Survey of 2009 (UNICEF, 2009). Six (30%) respondents confirmed that they were practising EBF. Fourteen (70%) respondents reported that they were not practicing EBF. This study noted a 30% EBF in Mataga Ward. The Mataga Ward EBF rate confirms national results of 29%, as there is only 1% difference from the Multiple Indicator Monitoring Survey findings (UNICEF, 2009).
KNOWLEDGE AND UNDERSTANDING ABOUT EXCLUSIVE BREAST FEEDING AMONG RESPONDENTS AND IMPLICATIONS FOR UPTAKE
The respondents exhibited extensive knowledge and understanding of the meaning of EBF. Fifteen (70%) mothers provided very satisfactory responses. Five (25%) mothers showed satisfactory knowledge of EBF. The study noted not much significant correlation between this knowledge of the meaning of EBF and actual practice. Out of the 14 (70%) of the mothers who exhibited extensive knowledge of EBF, only five (25%) managed to practise EBF. This state of affairs is a clear pointer to the fact that knowledge of EBF does not translate into its active uptake. These results can elucidated by the theory of planned behaviour that knowledge alone is not sufficient to change behaviour, but that attitudes, subjective norms and perceived behavioural control regarding behaviour all influence the intention to perform certain behaviours (Ajzen, 2006). Jenkins et al. (2011) note that older women and in-laws are perceived by mothers as good advisers, because of their knowledge of existing social norms and in this sense they influence the mother's infant feeding choices. This can be explained by the theory of planned behaviour that attitudes are determined by the society's perception of the desirability of one's action (Fishbein & Ajzen, 1975).
This paper contends that although education, knowledge and behavior usually do not always tally, particularly in communities where cultural norms and belief systems tend to override individual choices, the extent to which knowledge modifies behavioral practices tends to be significant. For this reason, health education on exclusive breast feeding tends to be more effective especially to those with some educational background. Health education focuses on building individuals' capacities through educational, motivational, skill-building and consciousness-raising techniques. Healthy public policies provide the environmental supports that will encourage and enhance behaviour change. By influencing both individuals' capacities and providing environmental support, meaningful and sustained behavior change.
Mothers' attitude towards EBF
The mother's attitudes towards EBF were measured through enquiring whether the mothers felt that EBF alone was enough for their babies. Thirteen (65%) respondents pointed out that mother's milk alone was not enough for the baby and there is a need to give supplementary feeding. These 13 (65%) mothers did not practise EBF. Only one respondent, who was not practising EBF, mentioned that EBF was enough, but despite this she was not practicing it herself. Respondent number 5 was asked why she thinks that breastfeeding alone was not enough for the baby; she said in vernacular Shona that "Mwana anenge ane nzara nenyota saka anotoda porridge ne mvu " (the baby would be hungry and thirsty and would need porridge). The argument that the baby would be thirsty cannot be justified, because 88% of breastmilk is water and this is known to the mothers from the nurses (LINKAGES, 2004).
Traditional practices hindering EBF (nhova treatment)
The effects of tradition on human behavior are of paramount importance when it comes to the introduction of particular health practices as EBF. The power of tradition and of society over and above the individual even receives immense emphasis from architects of sociology such as Emile Durkheim. In his book: "Rules of sociological Method" Durkheim (1982) emphasizes the role of collectivity (social facts) in influencing human behavior. He argues thus: "Every type of social conformity carries with it a whole gamut of individual variations. It is nonetheless true that the sphere of permitted variations is limited. It is non-existent. Or very small as regards religious and moral phenomena, where deviations may easily become crimes" (Durkheim, 1982:47).
Zimbabwe tradition demands that traditional medicine be administered to babies to try and avert death caused by the condition that culminates in the subsiding of the fontanel in babies, mainly because of severe dehydration (a condition known as nhova in the vernacular). This practice is also common in Kenya, where infants are given various herbs to treat the condition known in Kenya as ndebele (Ministry of Health Kenya, 2009). Traditionally this condition is attributed to evil spells. Out of the 14 (70%) respondents not practicing EBF, 12 informed the study that they had treated nhova on their babies through administering different foods and medicines such as bark, juices, roots, herbs, cooking oil and wild fruit.
Once more, such traditional practices militate against the core tenets of EBF that prohibit the intake of any solids, let alone medicine unless prescribed by a qualified medical practitioner. To sustain EBF practice, it is necessary to keep in mind these traditional practices and safeguards that have tended to supersede modern medicine as guarantees of survival in resource-poor communities.
Pressure from in-laws
Significant others such as grandmothers, mothers-in-law and husbands influence the infant feeding practices adopted by mothers. Mothers-in-law were identified by respondents as key authority figures on the uptake of EBF. To this effect, 14 (70%) of respondents indicated that mothers-in-law are key decision makers with regard to infant feeding. In an African culture older persons are regarded as fountains of knowledge and younger persons tap knowledge from them. Most of the advice that came from the mothers-in-law discouraged EBF in favour of mixed infant feeding practices. The mother-in-law is usually powerful and influential in major decisions concerning the behaviour and conduct of her daughter-in-law. According to one respondent, the mother-in-law gave the infant porridge a day after delivery, arguing that the family tradition requires that the baby be fed on porridge the day she gets home from the hospital by its grandmother. On the same note, four respondents indicated that on leaving their babies with their grandmothers, they were automatically fed on porridge because of cultural norms and traditions.
It is worth noting that such a scenario is in no way peculiar to Zimbabwe, as it corresponds with findings in Malawi that the influence of the mother-in-law and husband was one of the greatest barriers to EBF in Malawi (Kerr, Berti & Chirwa, 2007).
Be that as it may, this state of affairs has its explanation in the theory of planned behaviour which envisages that people's behaviour is influenced by normative beliefs, which are beliefs about the normative expectations of others and the motivation to comply with those expectations (Ajzen, 2006).
Implicit in this scenario is that sometimes one's level of education in a rural environment becomes secondary to the expectations and dictates of culture and tradition. In such a situation it becomes important for any health-promotion strategy to be ingrained within the cultural expectations of the particular locality within which it is conducted. The impact of external influences on the mother's ability and resolve to embrace EBF. According to Durkheim, (1982), "there are ways of acting, thinking and feeling which possess the remarkable property of existing outside the consciousness of the individual. Not only are these types of behaviour and thinking external to the individual, but they are endued with a compelling and coercive power by virtue of which, whether he wishes it or not, they impose themselves upon him. Undoubtedly when I conform to them of my own free will, this coercion is not felt or felt hardly at all, since it is unnecessary. None the less it is intrinsically a characteristic of these facts; the proof of this is that it asserts itself as soon as I try to resist. If I attempt to violate the rules of law they react against me" (Durkheim, 1982:51).
Gender inequality
Power dynamics within the family were cited as a key factor exerting its influence with regard to the feeding of the babies. In an African rural milieu major decisions are made by the husbands as heads of the family. Eighteen (90%) respondents noted that they had a say on infant feeding. Indications are that 13 (65%) of the 18 fathers were against EBF, as they argued that the child should be given porridge because breast milk was not enough for the baby; that's why the baby was always crying. Another respondent informed the researcher that the husband is the one who bought peanut butter and margarine so that they could prepare porridge for the baby.
One respondent confirms having been confronted with what has tended to become the crucial question each time EBF is discussed in a traditional African setup, namely "Where on earth have you seen a baby surviving on breast milk alone?"
Implicit in such a scenario is that gender roles cut across all the facets of life, undermining even those aspects of human existence ordinarily thought to belong to the wife in a matrimonial relationship. This makes it essential for health-promotion practitioners to look at husbands as key stakeholders if such programmes as EBF are ever to be successful.
Limited income
Poverty and unemployment were cited as some of the impediments against EBF by many respondents. Respondents contend that they find it difficult to practise EBF given that inadequate food means low milk production.
This study observed that women in Zimbabwe have limited access to the means of production, hence their income and economic status are low. Among the 20 (100%) respondents interviewed, five (25%) had an income estimate of $5, four (20%) respondents earn an estimate of $20, four (20%) respondents earn an estimate of $50, three (15%) respondents earn $100, while only two (10%) respondents earn more than $200. Many women in rural areas live far below the poverty line (Gandure, 2009). Low amounts of milk from ill-fed and malnourished mothers have come as an unfortunate deterrent against EBF practice. To this end, the study noted a high prevalence of exclusive breastfeeding among mothers whose incomes are above $100; four (66%) of the six (100%) respondents practising EBF had an income above $100. Two respondents who were practising EBF had an income which is below $100. Fourteen (70%) respondents not practising EBF had incomes below $100. Two nurses and one village health worker informed the study that most mothers are failing to adhere to EBF because they are not producing enough milk generally as a result of hunger and starvation.
The above findings are in line with those from the Zimbabwe Vulnerability Assessment Committee, which found out that 39-45% of the people in Mberengwa were food insecure (Zimbabwe Vulnerability Assessment Committee, 2010).
The findings therefore draw the attention of all players in the promotion of EBF programmes to take poverty, unemployment and malnutrition seriously as obstacles against the achievement of set objectives. Informed by such a reality on the ground, the success of these programmes rests squarely on the adoption of a holistic approach to programming.
Role of social workers in promoting EBF: A discussion
Social Workers in primary health care utilises a plethora of interventions to meet the needs of their constituency varying from one on one/family casework and group work to community development work, health promotion activities and empowering community participation (IFSW, 2008). In line with this line of thought social workers have a cardinal role to play in the promotion of EBF. Social workers need to confront the prevailing barriers to EBF. These include low of education, retrogressive traditional practices, societal pressure, scarcity of food, as well as gender inequalities. The role of social workers will undoubtedly increase the uptake of EBF and in the long-term reduce fatalities associated with lack of EBF.
Social workers have a critical role in the implementation of maternal child health and other primary health care initiatives. Although in Zimbabwe social workers in hospital, clinics and private voluntary organisations are being involved in activities such as HIV and AIDs prevention, support for children and adults living with HIV and AIDs, epilepsy support, prevention and response, the field of EBF has always been a closely guarded area for people in the medical field. The area of maternal child health has largely been removed from the domains of social work, yet, the very definition of health is heavily loaded with socio-economic and psychological attributes (Kaseke, 1991).
Counselling of pregnant mothers, husbands and other family members
Counselling exhibit a special position in addressing barriers to EBF such as societal norms, peer pressure and traditional practices. Social workers are strategically empowered and well positioned to offer counselling to mothers during pregnancy and antenatal care periods when they visit the clinic. This can be through "Individual counselling" which entails one-on-one engagement, education or social support empowering the mother with key EBF messages and addressing challenges faced by the mothers (Shealy, Li, Benton-Davis & Grummer-Strawn, 2005). The individual counselling session should also seize the opportunity to demystify societal norms, myths and practices that stand in the way of EBF. Most importantly the session should build the esteem and confidence of the mother to practice EBF. Dhandapany, Bethou, Arunagirinathan and Ananthakrishnan (2008) in Pondicherry, India ascertained that most of the mothers who were antenatal counselled on breastfeeding initiated breastfeeding immediately after birth as compared to mothers who did not receive counselling.
Group counselling is another intervention. It engrosses education or support sessions, discussions or classes in groups. Group counselling should target family members including the mother, in-laws, grandmothers and husbands. This forum is important as it reaches out to husbands, mothers in law and grandmothers who often don't get EBF information as they do not attend prenatal and antenatal services at the clinic. The group sessions should take the opportunity to foster positive male involvement not just with regard to EBF but cross cutting child care. Counselling has been found to be an effective intervention to increase the uptake of EBF in Ghana by Aidam, Perez-Escamilla and Lartey (2005).
Social marketing
Social marketing of EBF has been associated with increased uptake of EBF including in rural areas (Darmstadt, Bhutta, Cousens, Adam, Walker & De Bernis, 2005; Shealy et al., 2005). Social marketing has the strength that it reaches to diverse population groups and confronts societal barriers to EBF. Social marketing entails strategies such as community based promotions and advertising that support or encourage EBF and strengthen the perception of EBF and mainstream breast feeding as a normal, accepted activity (Andreason, 1995). Media campaigns are commonly presented to a wide audience and use public channels such as television, radio, printed materials, or outdoor advertising (Darmstadt et al., 2005) .Social marketing campaigns go beyond media campaigns in that they tend to be comprehensive, multifaceted approaches providing targeted, coordinated interventions to a variety of audiences, including consumers, their support systems, health care providers, the community, and the general public (Andreason, 1995; Darmstadt et al, 2005; Khoury, Bryant & Carothers (forthcoming); Shealy et al., 2005). Social marketing utilises conventional principles in commercial marketing foster healthy behaviors or support behavioral change (Andreason, 1995). It uses many different approaches simultaneously to effect synergistic change, which is particularly appropriate for EBF because of the interplay of many complex issues and barriers involved Khoury et al. (forthcoming) argue that a comprehensive social marketing approach including interventions to upsurge public awareness (through the media and other outlets) amplified rates of initiation and duration while also cultivating perceptions of community support for EBF. Jenkins et al. (2011) in rural Zimbabwe has established that social marketing of EBF through road shows was associated with increased EBF understanding and uptake. The understanding of social determinants of health places social workers at a unique position to champion social marketing that addresses barriers such as culture, social norms, and societal pressure.
Fostering peer support
The purpose of peer support is to encourage mutual and share support to pregnant women and those currently breastfeeding. Perceived social support has also been found to predict success in breastfeeding (Aidam et al., 2005). It entails social workers mobilising, training and ongoing support of volunteer peer mothers who have gone through the process to reach out to pregnant and breast feeding mothers. Peer support activities includes psychosocial support, encouragement, education about EBF that is what it constitutes and benefits, and help with solving problems (Shealy et al., 2005). Peer support enables sharing of experiences and how barriers such as the negative influence of the husband and mother in law and cultural practices can be addressed. Women's social networks are highly influential in their decision-making processes, they can be either barriers or points of encouragement for EBF (Shealy et al., 2005). Although the target audience is usually pregnant or breastfeeding women, it may include fathers and others who support the breastfeeding mother. As pointed out by (Darmstadt et al., 2005) peer support may represent a cost-effective, individually tailored approach and culturally competent way to promote and support breastfeeding for women of varying socioeconomic backgrounds, especially where professional EBF support is not widely available such as in rural areas. In a systematic review to evaluate interventions that promote breastfeeding initiation, Sirkorski, Renfrew, Pindoria & Wade (2003) found peer support programs to be effective in increasing the initiation and duration of breastfeeding.
Home visitations and health education
Home visitation is an important conduit of successful health education. It entails one-to-one house visits made by social workers to mothers who are pregnant and those breast feeding and their family members. Cardinal health messages such as the meaning of exclusive breast feeding, its advantages and the protective role of colostrum and prompt initiation of breast feeding after birth explained to the family. The mother and the family members such as the husband, mother in law and grandmothers are informed about disadvantages of prelacteal feeds and hazards of mixed feeding practices and effects of cultural practices such as the nhova (fontanel) treatment. A 2001 Cochrane review searched 20 controlled trials and found professes effective professional support increasing optimal breastfeeding (Sirkorski et al., 2003).
The cultural identity is a highly relevant factor because ethnicity and tradition that influences health practices. Thus, the social worker must be culturally sensitive and seek out culturally appropriate options encouraging an individual to change their practices with regard to infant feeding (Jenkins et al., 2011). Indeed, individuals may be unaware of ingredients that adversely affect the infant need information as to how they can adhere to EBF yet respecting important cultural and social traditions.
Advocacy
Social workers need to take a leadership role in promoting breastfeeding and in assisting communities to become EBF friendly and sensitive where breastfeeding mothers feel welcomed and supported.
Social workers need to advocate for the implementation of Baby-Friendly Initiative within hospitals and community health services. Research shows that facilities that implement baby-friendly practices have higher EBF rates (Shealy et al., 2005). Further to that they need to promote economic developments that will lead to better health practices among the general population including increased uptake of EBF. The paper noted earlier that due to limited income and hunger many mothers were not practicing EBF due to lack of milk. Social workers can help to promote health by advocating for the development of employment opportunities that will improve the socioeconomic status of all segments of society and thus their access to health and preventive services.
It has also been noted that lack of education is associated with low EBF uptake among mothers. It is cardinal that social workers advocates for the education of women this has great value not just to EBF but many health outcomes.
CONCLUSION AND POSSIBLE INTERVENTIONS FOR ENCOURAGING EXCLUSIVE BREAST FEEDING PRACTICES
This study has revealed a number of impediments which often concurrently confront the mothers discouraging them from practicing EBF; these factors include low education levels, gender inequality, influence of mothers-in-law, the husband and other family members, traditional practices, low income and the mother's attitude. It is therefore important that efforts by the Ministry of Health and Child Care to upscale exclusive breastfeeding should be holistic so that they have an impact on all areas that determine the mothers' choice to practise EBF.
A number of recommendations can be made to increase the uptake of EBF in rural areas.
- The above-mentioned Ministry should ensure increased male involvement in health programmes that target families, as it was observed that male influence often presents a barrier to EBF uptake. Hence it is imperative that husbands accompany their wives to clinics, so that they may be educated on the recommended infant feeding practices. Facilitating male involvement also addresses gender inequalities not just in child care but in many other aspects of life.
- Community awareness on EBF should be scaled up and they should not only target mothers, but should be extended to members of the extended family such as grandmothers and mothers-in-law. This can be done through the utilisation of village meetings, church meetings and other community gatherings. Traditional leaders, church leaders and politicians should be included in the community awareness exercise as they are people of influence and people pay heed to their advice.
- Behaviour change awareness programmes targeting mothers and other community members should be initiated, seeking to change the attitudes of the mothers and community members towards EBF. These programmes should target perceptions such as that mother's milk alone is not enough for the baby. Behaviour change awareness can also address cultural beliefs that discourage exclusive breast feeding.
- The government needs to provide food to members of the community who are Hungary. Any food relief programme will impact positively on EBF practice. The study revealed that many mothers could not practise EBF because they were producing little milk because of a lack of food and starvation.
- It has also been noted that lack of education is associated with low EBF uptake among mothers. It is crucial that social workers advocate for the education of women, this has great value not just for EBF but has many other positive health outcomes.
- Village health workers need to be capacitated and conduct counselling sessions with mothers and family members to address barriers to EBF such as societal norms, peer pressure and traditional practices. This can be done through individual counselling, which entails one-on-one engagement, education or social support empowering the mother with key EBF messages and addressing challenges faced by the mothers .The individual counselling session should also seize the opportunity to demystify societal norms, myths and practices that hinder EBF. Most importantly, the session should build the esteem and confidence of the mothers to practice EBF. Group counselling is another intervention and it encompasses education or support sessions, discussions or classes in groups.
- This study was conducted on a small sample, but it points the way for future studies in this field. There is a need to do more and extensive research on the institutional capacity of the Ministry of Health and Child Welfare, as this study has not dwelt on the current efforts of the Ministry.
REFERENCES
ANDREASON, A. 1995. Marketing social change: changing behaviors to promote health, social development, and the environment. San Francisco, CA: Jossey-Bass Publishers. [ Links ]
AIDAM, B.A., PEREZ-ESCAMILLA, R. & LARTEY, A. 2005. Lactation counselling increases exclusive breast-feeding rates in Ghana. The Journal of Nutrition, 135(6):1691-1695. [ Links ]
AJZEN, I. 2006. Perceived behavioural control, self-efficacy, locus of control and the theory of planned behaviour. Journal of Applied Social Psychology, 32(4):665-683. [ Links ]
BANDURA, A. 2004. Health promotion by social cognitive means. Health Education & Behavior, 31(2):143-164. [ Links ]
CRESWELL, J.W. 2009. Qualitative, quantitative and mixed methods approaches (3rd ed). New York: Sage Publications. [ Links ]
DHANDAPANY, G., BETHOU, A., ARUNAGIRINATHAN, A. & ANANTHA-KRISHNAN, S. 2008. Antenatal counselling on breastfeeding - is it adequate? A descriptive study from Pondicherry, India. International Breastfeeding Journal, 3:3-5. [ Links ]
DARMSTADT, G.L., BHUTTA, Z.A., COUSENS, S., ADAM, T., WALKER, N. & DE BERNIS, L. 2005. Lancet Neonatal Survival Steering Team. Evidence-based, cost-effective interventions: how many new born babies can we save? Lancet, 365(9463):977-988. [ Links ]
DURKHEIM, É. 1982. 1858-1917. Rules of sociological method. New York: Free Press. [ Links ]
GANDURE. 2009. A situation analysis on the status of women's and children's rights in Zimbabwe, 2005-2010: A call for reducing disparities and improving equity. Harare: UNICEF Zimbabwe. [ Links ]
GELFAND, M. 1985. Growing up in Shona Society: from birth to marriage. Gweru: Mambo Press. [ Links ]
GREEN, C.P. 1999. Improving breastfeeding behaviours: evidence from two decades of intervention research. Published for the US Agency for International Development (USAID) by the LINKAGES Project. Academy for Educational Development, Washington, DC. [ Links ]
FISHBEIN, M. & AJZEN, I. 1975. Belief, attitude, intention and behaviour: an introduction to theory and research. Reading MA: Addison-Wesley. [ Links ]
INTERNATIONAL FEDERATION OF SOCIAL WORKERS (IFSW). 2008. IFSW Policy Statement on Health. [ Links ] [Online] Available: http://www.ifsw.org/p38000081.html.
JENKINS, A.L, TAVENGWA, N.V, CHASEKWA, B., CHATORA, K., TARUBEREKA, N., MUSHAYI, W., MADZIMA, C. & MBUYA, N.M. 2011. Addressing social barriers and closing the gender knowledge gap: exposure to road shows is associated with more knowledge and more positive beliefs, attitudes and social norms regarding exclusive breastfeeding in rural Zimbabwe. Maternal and Child Nutrition, 8(4):459-470. [ Links ]
JONES, G., STEKETEE, R.W., BLACK, R.E., BHUTA, Z.A., MORRIS, S.S. & THE BELLAGIO CHILD SURVIVAL STUDY GROUP. 2003. How many child deaths can we prevent this year? The Lancet, 362(9377):65-71. [ Links ]
KASEKE, E. 1991. Social work practice in Zimbabwe. Journal of Social Development in Africa, 6:33-45. [ Links ]
KERR, R.B., BERTI, R.P, CHIRWA, M. 2007. Breastfeeding and mixed feeding practices in Malawi: Timing, reasons, decision makers, and child health consequence. Food and Nutrition Bulletin, 28(1). [ Links ]
KHOURY, A,J., BRYANT, C.A., CAROTHERS, C. The national loving support makes breastfeeding work campaign in Mississippi. Maternal Child Health Journal. Forthcoming. [ Links ]
KOYANAGI, A., HUMPHREY, J.H. & MOULTON, L.H. 2009. Effect of early exclusive breastfeeding on morbidity among infants born to HIV-negative mothers in Zimbabwe. American Journal of Clinical Nutrition, 89(5):1281-1282. [ Links ]
LINKAGES. 2004. Exclusive breastfeeding: the only water source young infants need, frequently asked questions. Academy for Educational Development. [ Links ] [Online] Available: www.linkagesproject.org.
MINISTRY OF HEALTH AND CHILD WELFARE. 2010. National Nutrition Survey. Harare: Ministry of Health and Child Welfare. [ Links ]
MINISTRY OF HEALTH KENYA. 2011. Rapid qualitative assessment: beliefs and attitudes around infant and young child feeding in Kenya. Ministry of Health Kenya. [ Links ]
MOLAND, K.M., PAOLI, M.M., SELLEN, W.D., ESTERIK, P., LESHABARI, S.C. & BLYSTAD, A. 2010. International Breastfeeding Journal, 5:10. [ Links ] [Online] Available: http://www.internationalbreastfeedingjournal.com/content/5/1/10. [Accessed: November 2013].
RITCHER, L. & GRIESEL, D. 1998. Breastfeeding and infant care in the context of HIV/AIDS, Psychology in Society, 24. [ Links ] [Online] Available: www.pins.org.za/pins24/pins24article05_Richter_Griesel.pdf. [Accessed: 21/08/2014].
SAVE THE CHILDREN. 2009. Infant feeding practices in Binga and Nyaminyami, Zimbabwe, in relation to HIV Report. Harare: Save the Children Zimbabwe. [ Links ]
SIRKORSKI, J., RENFREW, M.J., PINDORIA, S. & WADE, A. 2003. Support for breastfeeding mothers (Cochrane review). The Cochrane Library, Issue 3. Oxford: Update Software. [ Links ]
SHEALY, K.R., LI, R., BENTON-DAVIS, S. & GRUMMER-STRAWN, L.M. 2005. The CDC Guide to Breastfeeding Interventions. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. [ Links ]
SEARS, O.D., SHELLY, E.T. & LETTICIA, A.P. 2009. Social psychology. New York: Prince Hall. [ Links ]
UNICEF. 2009. Multiple Indicator Monitoring Survey 2009. Harare: UNICEF. [ Links ]
WIESLAW, J. & FREDERICA, P. 2011. Effect of exclusive breastfeeding on the development of children's cognitive function in the Krakow prospective birth cohort study. European Journal of Paediatrics, 28(4):372-377. [ Links ]
WORLD HEALTH ORGANISATION. 2001. The optimal duration of exclusive breast-feeding. A Systematic Review. Geneva: WHO. [ Links ]
WORLD HEALTH ORGANISATION. 2003. Global strategy for infant and young child feeding. Switzerland: WHO. [ Links ]
ZIMBABWE NATIONAL STATISTICAL AGENCY. 2011. Zimbabwe Demographic Health Survey 2010. Harare: Zimbabwe National Statistical Agency. [ Links ]
ZIMBABWE VULNERABILITY ASSESSMENT COMMITTEE. 2010. Rural Vulnerability Assessment. Harare: Government Printers. [ Links ]

