










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSocial Work
On-line version ISSN 2312-7198
Print version ISSN 0037-8054
Social work (Stellenbosch. Online) vol.50 n.3 Stellenbosch 2014
http://dx.doi.org/10.15270/50-2-407
ARTICLES
http://dx.doi.org/10.15270/50-2-407
Assessment of pain and suffering in child abuse and homicide victims: Suggestions for social work practice
René AlbertynI; Nico NortjéII
IDepartment of Paediatric Surgery, Red Cross Children's Hospital, The University of Cape Town, Rondebosch, South Africa
IIDepartment Dietetics, University of the Western Cape, Bellville, South Africa
ABSTRACT
Child abuse and homicide are on the increase worldwide. Often the burden falls upon social workers to argue the case of victims without being able to quantify the pain the children have suffered. A case study approach was used in which a High Court case was utilised as base to describe the proposed methodology to assess the level of pain, post-mortem, a victim could have gone through. The application was a four-step methodology constructed by using paediatric pain assessment. This study found that there is a need for the development of post-mortem pain scales to aid social workers.
The skin and bones tell a story which the child is either too young or too frightened to tell. Johnson, Cameron and Camps
INTRODUCTION
The maltreatment of children is a global problem. Estimates on the incidence of the problem are mostly inaccurate as are many cases of abuse and homicide, particularly in poor and developing countries, which are largely under-reported or even unreported (World Health Organisation, 2010), since a significant proportion of child abuse and homicide cases are attributed to incidents (such as burns, injuries, falls, drowning) in which the abuse has been deliberately inflicted by those close to the child. UNICEF (2009) estimates that almost 300 million children worldwide are subjected to violence, exploitation and/or abuse. A recent report by UNICEF states that "South Africa's levels of violence against children are among the highest in the world. Tens of thousands of children are victims of abuse, neglect and exploitation every year - and offenders often go unpunished" (UNICEF, 2012:1).
Far more revealing are the statistics from South Africa (a developing country with 50 million people (Statistics South Africa, 2011)), where instances of child homicide are estimated to be double those in most underdeveloped countries (Abrahams, Jewkes, Martin & Lombard, 2013:562). Latest child homicide statistics revealed that three children a day are murdered in South Africa, and that the overall paediatric homicide rate in the country is 5.5 per 100 000 children (Mathews, Abrahams, Jewkes, Martin & Lombard, 2012:1).
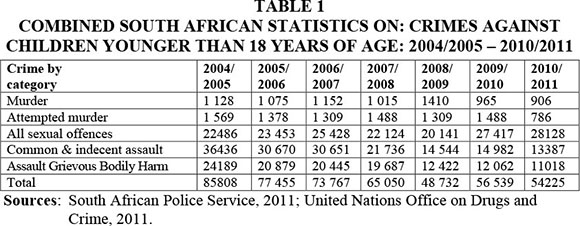
Statistics released by the South African Police Child Protection Unit indicate that 23 664 cases of child abuse alone were reported 1994, 35 838 cases in 1996 and 23 231 cases of deliberate child neglect in 1998 (Pierce & Bozalek, 2004:820). In addition, the number of child homicides increased by more than 22% during 2006-2008 (South African Police Service, 2011). Approximately 63 906 cases of crime against children younger than 18 years of age were recorded during 2007-2008, of which 1 410 were murder and 1 488 attempted murder (South African Police Service, 2011).
The majority of these cases will never be successfully resolved, as only 7% of child abuse cases heard in South African courts lead to conviction - which means that 93% of those accused in a court of law will walk free (Conradie, 2003:2). Most of the evidence in the prosecution of criminal cases of child abuse and homicide hinges on forensic and medical evidence that focuses on the injuries and damage sustained during the act of violence, or on the abuse during the traumatic event. However, little attention is paid to the suffering and pain endured by the victim of abuse and homicide during and after the act of violence. Unsubstantiated evidence is excluded in a court of law in most criminal cases. As a result, the circumstances surrounding the traumatic event as experienced by the victim (i.e. pain and suffering) will seldom be allowed as evidence in child homicide cases in a retrospective manner on behalf of the child who has died. The subjective nature of so-called hearsay evidence on pain and suffering probably precludes its inclusion. Nevertheless, the pain and suffering sustained during a traumatic event (i.e. motor vehicle accidents, neglect) play a major role in the determination of financial compensation in a court of law. In civil cases compensation is often based on a subjective analysis of projected pain and suffering in the future (Clarence, 1959:483). This raises several questions concerning pain and suffering sustained during acts of violence and homicide. The authors pose the question of whether pain and suffering should be included in the forensic and medical evidence in cases of child abuse and homicide. And if so, who would need to do this and would this be of any value as evidence in a court of law? Moreover, would the analysis be beyond reasonable doubt? Furthermore, would a post-mortem pain-measurement template answer the question?
For the purpose of this study both child homicide and abuse will be addressed, as social workers will deal with the spectrum of abuse. Often an act would start out as abuse and end up as homicide. The literature indicates that there are several reasons why children are killed: the child is unwanted; parental psychiatric illness; the parent wanted to relieve the victim of suffering; accidental homicide (child abuse and/or emotionally-based homicide); and spousal revenge. Younger children are more often the victims of child abuse or emotionally-based homicide; previous incidents of child abuse were found in 40% of homicide cases (Boudreaux, Lord & Jarvis, 2001:61,70).
GOAL OF THE STUDY
This article will explore the possibility of using a retrospective analysis of pain and suffering, conducted by social workers as part of the forensic evidence in the prosecution of child murder and abuse cases, and its application in the legal system. Once this has been established, the authors would propose that a template indicator be recommended by which pain can be categorised according to severity, taking individual factors (age, body type, etc.) into consideration, and post-mortem pain can be considered more explicitly in guilty verdicts for a more severe punishment. Social work policy in general has shifted over the past decade in South Africa, where cases of abuse have been seen as a primarily private affair in the past, but with the increase in child abuse and homicide cases recently, there has been a wider communal outcry which necessitates the social workers getting more involved and often having to testify in abuse and homicide cases (Mathews et al., 2012:4). The proposed change in the application in the legal system could hugely benefit social work practice in South Africa, whereby the social workers will be empowered with better tools to testify to the benefit of the child who can no longer speak for himself or herself.
METHOD
A case study methodology was used in which the case study became a strategy for doing the research, which involved an empirical investigation of a particular contemporary phenomenon within its real-life context, using multiple sources of evidence as presented below (Robson, 2011:136). Case studies are qualitative research strategies in their own right with their own design. Since the aim of qualitative studies is not to make any statistical generalisation on any population beyond the sample surveyed, no control group was included in the study. The reliability or consistency of the data analysis in qualitative research is an evolving process and can differ vastly from interpretation to interpretation (Nortje, 2014:180). What is of paramount importance to any qualitative study is the authenticity of the data, which refers to the idea that a fair, honest and balanced account of social life from the viewpoint of someone who lives it every day (Neuman, 2007:108) has been given.
In utilising this methodology, the context plays an important role, which is explained below, referring to a child abuse and homicide case that was tried in the Cape Town High Court.
Case: AH, a 3-year-old boy was admitted to the Red Cross Children's Hospital's Intensive Care Unit, after apparently having fallen from a bunk bed. He was unconscious on arrival in the Trauma Unit and was diagnosed as having a closed head injury and non-accidental injury (NAI). Diagnoses made at the time of admission include: multiple bruising (legs, torso), possible human bite on the (L) humerus, forehead hematoma, with surrounding bruising, pinch marks on the nipples, tramline bruises on the upper buttock area, bruising of the penis, and scratch marks on the scrotum and around the neck. The child was stabilised and transferred to the Paediatric Intensive Care Unit, where his condition deteriorated. He died 48 hours post-admission, after having been declared brain dead. As the clinical findings did not correlate with the history given by the parents, a post-mortem was requested by the state to investigate the possibility of non-accidental injury. For example, the father explained the cigarette burn lesions as having been "self-inflicted", indicating that the toddler had accidently burned himself.
Family history: Background information revealed that the mother and father of the child were not married at the time, that they were not living together, and that the child was primarily cared for by his mother. The relationship between the mother and father was described as volatile. AH attended a day-care facility, where it was noted that he was clumsy on his feet and that he tended to fall easily. He was otherwise normal in terms of developmental benchmarks and also speech development. Family and community members expressed their concern about the child's safety as abuse had been noted (he had been treated for cigarette burns to the face, ears, perineum, and facial bruising on a previous occasion). The child was removed from maternal care and placed in foster care, pending a child-abuse investigation. In violation of a previous court ruling, the mother allegedly removed the child from this placement and he died a few weeks later while in her care.
Post-mortem findings: A post-mortem was subsequently conducted. Findings corresponded largely with the initial diagnoses on admission. In addition, skin lesions (suspected to be cigarette burns) were noted in the following areas: three circular lesions on the (R) leg, one similar lesion on the dorsal aspect of the foot, one lesion on the left medial malleolus, four individual lesions under the eyes, in the ear and side of the head, three lesions on the cheek and one lesion in the posterior anal verge. One healed lesion was noted on the (L) upper arm. Post-mortem investigations also revealed severe abdominal trauma and peritonitis. The findings confirmed cigarette burns, soft tissue injuries, severe head trauma and blunt abdominal trauma. The case was handed to the police for further investigation.
Since there is no relevant measuring scale or data for the assessment and measurement of pain post-mortem, and since this has never been done in a court of law anywhere in the world, a four-step methodology based on a literature review (Baker & Wong, 1987:13; Coffman, Alvarez, Pyngolil, Petit, Hall & Smyth, 1997:224-225; Franck, Smith-Greenberg & Stevens, 2000:491; Herr, Coyne, Key, Manworden, McCaffery, Merkel, Pelosi-Kelly & Wild, 2006:47-48; Merkel & Malviya, 2000:409-410) was constructed, using paediatric pain assessment as a point of departure.
RESULTS
A four-step methodology which was developed will be described briefly below, with special reference to how it was adapted for the post-mortem evaluation of the aforementioned case.
1. A review of available medical information (and forensic reports in this case). This enables the social worker to determine the exposure to pain and suffering before and during the traumatic event. Assumptions on the pain and suffering endured by a child are usually based on the severity of the injury (second- to third-degree burns), the location of the injury (e.g. under the eyes, perineum, legs and ears) and number of injuries (13 fresh and 1 old lesion).
Injuries are often burn related and therefore it is useful in these cases to understand the epidemiology of non-accidental burn injuries, the patho-physiology of burns and a description of burn injuries in terms of depth and pain.
- Epidemiology and pattern of non-accidental burn injuries. The age at which children are most likely to sustain non-accidental burn injuries is 2-4 years of age, with boys being three times more at risk than girls (Greenbaum, Donne, Wilson & Dunn, 2005:631). Children with inflicted burn injuries are more likely to come from single-parent families and up to 96% of them are from low-income families (Peck, Priolo-Kapel, 2002:1015; Toon et al., 2011:99). In cases of non-accidental burn injuries, the pattern of injury (e.g. cigarette burns, liquid burns) is important as is the area burned (e.g. burns to the soles of the feet, genitalia, buttocks, face forehead, hands, chest and perineum) (Swerdin, Berkowitcz & Craft, 2002:378), which needs to be examined carefully (Ayoub & Pfeifer, 1979:910; Hight, Bakalar & Lloyd, 1979:519).
- Patho-physiology of burns. The depth of a burn depends on the temperature and time of exposure. At 44° Celsius it will take 6-7 hours for full thickness destruction of the skin; at 60° Celsius it will take about 10 seconds; and at 70° Celsius it will take only 1 second to cause a third-degree burn. The critical temperature for clinically relevant tissue damage ranged from 50-55° Celsius (Hobbs, 1989:1302). Since cigarette burns are the most common occurrence of non-accidental injury burns, it is important to take cognisance of the impact. The burning tip of a normally manufactured cigarette is about 400° Celsius, but while dragging on the cigarette a temperature of between 600900° Celsius can be reached (Greenbaum et al., 2005:634). Typical deliberately inflicted cigarette burns are sharply defined as the expected size of the cigarette tip, round and "punched out". Such burn injuries require firm contact with the skin for a few seconds and cannot occur from accidental contact, which will produce a poorly defined lesion (Faller-Marquardt, Pollak & Schmidt, 2008:207). Cigarette burns are third-degree burns with lesions of between 4-10 mm across, resulting in a small circular or oval depigmented scar (Kos & Shwayder, 2006:315; Reed & Pomerantz, 2005:128; Sunderland, 2002:16). To cause scar formation, the glowing tip of the cigarette needs to be held to the skin for 2-3 seconds or longer (Faller-Marquardt et al., 2008:207). These burns are persistently painful.
- Burn injuries in terms of depth and pain. Burn injury pain is a source of immense suffering (Summer, Puntillo & Miaskowski, 2007:534). First-degree (or superficial) burns are normally caused by short exposure to the source of heat. Pain from these injuries can last for 2 to 4 days and they will heal within 5 to 10 days. Second-degree injuries are very painful and might present with erythema (redness of skin) and blisters. Pain is caused by the longer exposure to the heat source and the destruction of nerve ends in the dermis and epidermis. Third-degree burns are more destructive and, although they are initially painless, they cause painful itching as the wound starts to heal. The pain from cigarette burns develops quickly, with a prickling sensation followed by prolonged burning pain. Intense pain is slow to develop, but slower to subside and leaves the victim in pain for hours (Faller-Marquardt et al., 2008:201).
Based on this review, the child described above was exposed to unimaginable pain and suffering. The abuse was deliberate and premeditated, with the abuser fully aware of the nature of the actions.
2. Pre-trauma (and in this case post-traumatic) information. It is important to study what occurred before and after the trauma took place (Sirotnak, Grigsby & Krugman, 2004:265). This information is obtained from people who were either involved with the child or known to the child (i.e. friends, family members of the deceased and members of society). Such data include previous medical records, the usage of drugs (e.g. analgesics), pre-morbid personality, cognitive developmental level, ability to socialise, intellectual development, and the victim's ability to build relationships and trust (Hobbs, 1986:360; Hornor, 2005:6; Swerdin et al., 2007:373, Maguire, Moynihan, Mann, Potokar & Kemp, 2008:1078).
The "traumatic event" (the acts of violence that led to abuse and/or death) also needs be assessed (Greenbaum et al., 2005:632). The social worker ought to study the circumstance of the traumatic event (the final act of abuse or violence) that contributed to death (Johnson & Showers, 1985:208). He or she needs to determine whether the traumatic event was the sole cause of pain and suffering, and whether the event was significant enough to cause both emotional and physical pain and suffering, or whether the traumatic event was a significant but not the sole contributing factor to pain and suffering (Pollanen, 2005:119).
In the case under discussion, the toddler had a good relationship with his mother and her family. He was also well adjusted at school and able to socialise with his peers. Of concern was his observed clumsiness, but this was never investigated. However, the child's relationship with his biological father was poor. The cause of death in this case was attributed to a closed head injury - which could have caused pain. However, if the injuries documented prior to admission (i.e. soft tissue injuries, human bite, cigarette burns, bruises, welts), and those documented on admission (i.e. blunt abdominal trauma and head injuries) are brought into context, it can be concluded that there were significant levels of severe pain and suffering by the victim.
3. Psychological and emotional reaction to the injuries. Stoddard (1982:1472) states that children exposed to prolonged and untreated pain show psychological reactions such as anxiety, fear, withdrawal and anger. Untreated and prolonged exposure to physical pain (as in abuse) can erode trust and destroy the mother-child bond, with serious long-term psychological consequences for the child (Slater & Bremner, 2011:619). At ages 2 to 3 children are predominantly dependent on the mother for support and protection (Newman & Newman, 2009:188) against harm and further abuse.
Child victims subjected to cigarette burns would try to guard the affected area from human touch and display severe avoidance tendencies - trying to avoid further exposure to the cause of pain. Abuse from cigarette burns can therefore not be accidental, but would imply that the child had been held down while being burned (Peck & Priolo-Kapel, 2002:1016).
The lack of parental protection in child cases (e.g. cigarette burns) will create psychological reactions such as anxiety as referred to by Toon et al. (2011:107).
4. Pain. Measurement in this context means the determination of a quantifiable pain score depicting the severity of the pain (Bonham, 1996:69; Reed & Pomerantz, 2005:122). Existing pain-measurement scales rely on the observation of the child's behaviour and the child's self-report (Henry & Foster, 2000:689; Martin-Hertz et al., 2003:32; Richardson & Mustard, 2009:924). The conclusions in abuse cases (concerning the victim's experience of pain) are usually based on the severity of tissue damage - i.e. whether they are first-, second- or third-degree burns, and the intensity of the heat source (Chroniere, 2003:598; Richardson & Mustard 2009).
In this case burn lesions were observed under the eyes, in the ears, on the hands and perineum of the child - all areas sensitive to pain. It was concluded that the child had been exposed to severe pain and suffering while being burned and afterwards, as the pain sustained from a cigarette burn would have lingered before subsiding. Of further importance is the fact that the tip of a burning cigarette would have had to be held to the skin for several seconds to sustain the level of skin lesions observed in the post-mortem photographs. The conclusion was made that the toddler had not only been physically and emotionally abused over a period of time, but also restrained and even tortured to death.
DISCUSSION AND CONCLUSION
Traditionally, the legal approach to pain and suffering has always centred on recovery and the awarding of damages for non-financial loss. Financial compensation became the less than perfect effort to compensate a victim for loss (Kulich, 1999:61; Kulich, Kreis, Fihman, Prescott, Pelletier, Bennett & Metha, 2001:119). While civil law recognises the role that pain plays in determining compensation for the victim, the same cannot be said about criminal law. The authors of this study ask whether pain and suffering endured during an act of violence carry enough weight to be included in criminal court proceedings, since pain relief is a basic human right and a medical obligation. Could the recognition of pain and acting on that pain and suffering be seen as the post-mortem "right of the victim of crime and violence"? Ought the suffering of victims of crime to be considered, even postmortem? Should social workers get involved in these cases to prevent other victims of abuse from ending up dead as well? These questions of obligation could also be reframed by asking who will speak out for the child victim of homicide.
Although the assessment of forensic pain (determining liability) in medicine is well documented and specifies the different roles (e.g. defendant, assessor or primary physician) and duties (e.g. objective unbiased reporting of scientific facts or clinical experience) of the pain clinician in his or her role as an independent expert witness (Muller & Saayman, 2003:40; Oates, 1993:571), no evidence of the intensity of pain and suffering endured by the paediatric homicide/abuse victim during the traumatic event has ever been regarded as aggravating circumstances in criminal trials. One reason might be that the subjective nature of pain could be used to argue against the implementation of a post-mortem pain-measurement scale in criminal prosecution, since the prevailing view is to ignore subjective experiences, or to consider them only to a limited degree.
Furthermore, since the assessment and measurement of pain in living children are difficult, it is much more difficult in children who have died of unnatural causes - which is evident of the lack of existing post-mortem pain-measurement tools. However, it is possible to assess the pain (physical and emotional) endured during an act of violence retrospectively, and to report on that pain fairly accurately, as illustrated above. Validated measurement instruments are not yet available, but it is possible to develop such a methodology.
Thousands of children are victims of abuse, negligence and homicide (Pierce & Bozalek, 2004:820; Richter & Dawes, 2008:83), while acts of abuse, negligence and homicide are undoubtedly the cause of much pain and suffering. South African law acknowledges the retrospective and, in many cases, the prospective role of pain and suffering in civil cases (i.e. Road Accident Fund and Workman's Compensation) and in cases of negligence (inadequate treatment of pain or unintentional harm to another person) (Road Accident Fund Commission's Report, 2002). While South African law recognises the right of the victim to be heard, many childhood victims of abuse and homicide are unable to speak for themselves. These children have to rely on society, medical experts, social workers and prosecutors to speak for them. If this does not happen, they are denied their right to be heard. Moreover, they are denied their right to fair justice. If justice allows pain and suffering to be converted into monetary terms, surely these experiences should be allowed to be regarded as aggravating factors in criminal law. Posing the question as to whether the legal community might see the actual value of post-abuse and post-mortem pain assessments in legal matters, some might argue that there has been no need to include post-mortem pain measurement in homicide cases as up to now. However, the authors maintain that discussing pain and suffering in criminal cases would grant the victim "the right to be heard" to enable them to tell their stories and reveal the truth of how they suffered. In child homicide cases and cases of abuse involving inarticulate children's pain and suffering, the authors hereby argue that the findings should be included in the criminal investigation as aggravating evidence.
REFERENCES
AYOUB, C. & PFEIFER, D. 1979. Burns as a manifestation of child abuse and neglect. American Journal of Disabled Children, 133:910-914. [ Links ]
BAKER, M. & WONG, D.L. 1987. QUEST: a process of pain assessment in children. Orthopaedic Nursing; 6(1):1-22. [ Links ]
BONHAM, A. 1996. Managing procedural pain in children with burns: Part 1: assessment of pain in children. International Journal of Trauma Nursing, 2:68-73. [ Links ]
BOUDREAUX, M., LORD, W. & JARVIS, J. 2001. Behavioural perspectives on child homicide: the role of access, vulnerability and routine activities theory. Trauma, Violence and Abuse, 2(1):56-78. [ Links ]
CHRONIERE, M. 2003. Pain of burns. In: MELZACK, R. & WALL, P. (eds) Handbook of pain management. New York: Elsevier Ltd, 591-601. [ Links ]
CLARENCE, M. 1959. Liability for pain and suffering. Columbia Law Review, 59:476-486. [ Links ]
COFFMAN, S., ALVAREZ, Y., PYNGOLIL, M., PETIT, R., HALL, C. & SMYTH, M. 1997. Nursing assessment and management of pain in critically ill children. Heart Lung, 26:221-228. [ Links ]
CONRADIE, H. 2003. Are we failing to deliver in the best interest of the child? [Online] Available: Links ]crisa.org.za/fighting_crimes.pdf" target="_blank">http://www.crisa.org.za/fighting_crimes.pdf. [Accessed: 11/3/2012].
FALLER-MARQUARDT, M., POLLAK, S. & SCHMIDT, U. 2008. Cigarette burns in forensic medicine. Forensic Science International, 176(2-3):200-208. [ Links ]
FRANCK, L., SMITH-GREENBERG, C. & STEVENS, B. 2000. Pain assessment infants and children. Pediatric Clinics of North America, 47(3):487-512. [ Links ]
GREENBAUM, A., DONNE, J., WILSON, D. & DUNN, K. 2005. Intentional burn injury: an evidence based clinical and forensic review. Burns, 30(7):628-642. [ Links ]
HENRY, D.B. & FOSTER, R.L. 2000. Burn pain management in children. Pediatric Clinics of North America, 47(3):681-698. [ Links ]
HERR, K., COYNE, P., KEY, T., MANWORDEN, R., McCAFFERY, M., MERKEL, S., PELOSI-KELLY, J. & WILD, L. 2006. Pain assessment in the non verbal patient: position statement with clinical practice recommendations. Pain Management Nursing, 7(2):44-52. [ Links ]
HIGHT, D.W., BAKALAR, H. & LLOYD, J.R. 1979. Inflicted burns in children: recognition and treatment. JAMA, 242:517-520. [ Links ]
HOBBS, C.J. 1986. When are burns not accidental. Archives of Disease in Childhood, 61:357-361. [ Links ]
HOBBS, C.J. 1989. Burns and scalds. British Medical Journal, 298:1302-1305. [ Links ]
HORNOR, G. 2005. Physical abuse recognition and reporting. Journal of Pediatric Health Care, 19(1):4-11. [ Links ]
JOHNSON, C. & SHOWERS, J. 1985. Injury variables in child abuse. Child Abuse and Neglect, 9:207-215. [ Links ]
KOS, L. & SHWAYDER, T. 2006. Cutaneous manifestation of child abuse. Pediatric Dermatology, 23(4):311-320. [ Links ]
KULICH, R.J. 1999. Forensic assessment: ethical and clinical practice issues of the pain clinician. Current Review of Pain, 3:61-66. [ Links ]
KULICH, R.J., KRUIS, P.G., FIHMAN, S.M., PRESCOTT, J.C., PELLETIER, N.J., BENNETT, P. & METHA, N.R. 2001. Forensic issues in pain: review of current practice. Pain Practice, 1(2):119-135. [ Links ]
MAGUIRE, S., MOYNIHAN, S., MANN, M., POTOKAR, T. & KEMP, A.M. 2008. A systematic review of the features that indicate intentional scalds in children. Burns, 34:1072-1081. [ Links ]
MARTIN-HERTZ, S., PATTERSON, D., HONARI, S., GIBSON, J., GIBRAN, N. & HEIMBACH, D. 2003. Pediatric pain control practices in North American Burn Centers. Journal of Burn Care and Rehabilitation, 24(1):26-36. [ Links ]
MATHEWS, S., ABRAHAMS, N., JEWKES, R., MARTIN, L.S. & LOMBARD, C. 2013. The epidemiology of child homicides in South Africa. Bull World Health Org, 91:562-568. [ Links ]
MATHEWS, S., ABRAHAMS, N., JEWKES, R., MARTIN, L.J. & LOMBARD, C. 2012. Child homicide patterns in South Africa: is there a link to child abuse. South African Research Council - August 2012. [ Links ] [Online] Available: http://www.mrc.ac.za/policybriefs/childhomicide.pdf. [Accessed: 12/08/2013].
MERKEL, S. & MALVIYA, S. 2000. Pediatric pain, tools and assessment. Journal of Peri-Anesthesia Nursing, 15(6):408-414. [ Links ]
MULLER, K. & SAAYMAN, G. 2003. Forensic science in medicine: what every doctor in South Africa should know. South African Family Practice, 45(6):41-45. [ Links ]
NEUMAN, W.L. 2007. Basics of social research - qualitative and quantitative approaches (2nd ed). Boston: Pearson, 108-139. [ Links ]
NEWMAN, B.M. & NEWMAN, P.R. 2009. Life-span development: a psychosocial approach (11th ed). United Kingdom: Wadsworth. [ Links ]
NORTJE, N. 2014. Ethical tensions faced by dietetic students during fieldwork. South African Journal of Clinical Nutrition, 27(3):180. [ Links ]
OATES, R.K. 1993. Three do's and three don'ts for expert witnesses. Child Abuse and Neglect, 17:571-572. [ Links ]
PECK, M. & PRIOLO-KAPEL, D. 2002. Child abuse by burning: a review of the literature and an algorithm for medical investigations. Journal of Trauma, 53(10):1013-1022. [ Links ]
PIERCE, L. & BOZALEK, V. 2004. Child abuse in South Africa: an examination of how child abuse and neglect are defined. Child Abuse and Neglect, 28(8):817-832. [ Links ]
POLLANEN, M.S. 2005. Deciding the cause of death after autopsy - revisited. Journal of Clinical Forensic Medicine, 12:113-121. [ Links ]
REED, J. & POMERANTZ, W.J. 2005. Emergency management of paediatric burns. Pediatric Emergency Care, 21(2):118-129. [ Links ]
RICHARDSON, P. & MUSTARD, L. 2009. The management of pain in the burn unit. Burns, 35(7):921-936. [ Links ]
RICHTER, L.M. & DAWES, A. 2008. Child abuse in South Africa: rights and wrongs. Child Abuse Review, 17:79-93. [ Links ]
ROBSON, C. 2011. Real world research (3rd ed). New York: Wiley-Blackwell. [ Links ]
SIROTNAK, A.P., GRIGSBY, T. & KRUGMAN, D. 2004. Physical abuse of children. Pediatrics in Review, 25:264-277. [ Links ]
SLATER, A. & BREMNER, G. 2011. An introduction to developmental Psychology (2nd ed). London: Blackwell. [ Links ]
SOUTH AFRICAN POLICE SERVICE. 2011. Crime statistics. [ Links ] [Online] Available: http://www.saps.gov.za/statistics/reports/crimestats/2011/categories.htm [Accessed: 11/12/2013].
STATISTICS SOUTH AFRICA. 2011. South African Population July 2011. [ Links ] [Online] Available: http://www.statssa.gov.za/publications/P0302/P03022011.pdf [Accessed: 11/12/2013].
STODDARD, F.J. 1982. Coping with pain: a developmental approach to treatment of burned children. American Journal of Psychiatry, 139(6):736-741. [ Links ]
SUMMER, G., PUNTILLO, K. & MIASKOWSKI, C. 2007. Burn injury pain - the ongoing challenge. The Journal of Pain, 8(7):533-548. [ Links ]
SUNDERLAND, R. 2002. Child abuse: recognizing the injuries. Trauma, 4(1):11-16. [ Links ]
SWERDIN, A., BERKOWITCZ, G. & CRAFT, N. 2007. Cutaneous signs of child abuse. Journal of American Academic Dermatoly, 57:371-392. [ Links ]
TOON, M.H., MAYBAUER, D.M., ARCENEAUX, L.L., FRASER, J.F., MEYER, W., RUNGE, A. & MAYBAUER, M.O. 2011. Children with burn injury assessment of trauma, neglect, violence and abuse. Journal of Injury and Violence Research, 3(2):98-110. [ Links ]
UNICEF. 2012. Belief in "zero" campaign aims to end violence against children in South Africa. [ Links ] [Online] Available: http://www.unicef.org/infobycountry/southafrica62328.html. [Accessed: 11/12/2013].
UNICEF. 2009. Child protection from violence, exploitation and abuse. [ Links ] [Online] Available: http://www.unicef.org/media/media_45451.html. [Accessed: 11/12/2013].
UNITED NATIONS OFFICE ON DRUGS AND CRIME. 2011. Crime situation. [ Links ] [Online] Available: http://www.unodc.org/pdf/southafrica/country_profile_southafrica_8.pdf. [Accessed: 11/12/2013].
WORLD HEALTH ORGANISATION. 2010. Child maltreatment. [ Links ] [Online] Available: http://www.who.int/violence_injury_prevention/violence/child/en/. [Accessed: 11/12/2013].

