










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.79 n.1 Johannesburg Feb. 2024
http://dx.doi.org/10.17159/sadj.v79i01.18042
RADIOLOGY CORNER
MAXILLOFACIAL RADIOLOGY
Double type III dens invaginatus
C SmitI; GD BuchananII; Z YakoobIII; MY GamieldienIV; L RobinsonV
IBChD, MSc (Maxillofacial Radiology) ORCID: 0000-0003-4047-6356
IIBChD, PDD (Endodontics), MSc (Dentistry), PhD (Anatomy) ORCID: 0000-0003-2957-166X
IIIBChD, PDD & MSc (Maxillofacial Radiology), PG Dip General Management (GIBS UP) ORCID: 0000-0003-1966-5574
IVBChD, PGDipDent (Oral Surgery), MSc (Anatomy) ORCID: 0000-0001-5334-7989
VBChD, PDD (Maxillofacial Radiology), PDD (Forensic Odontology), MChD (Oral Path), FC Path (SA) Oral Path ORCID: 0000-0002-0549-7824
CASE
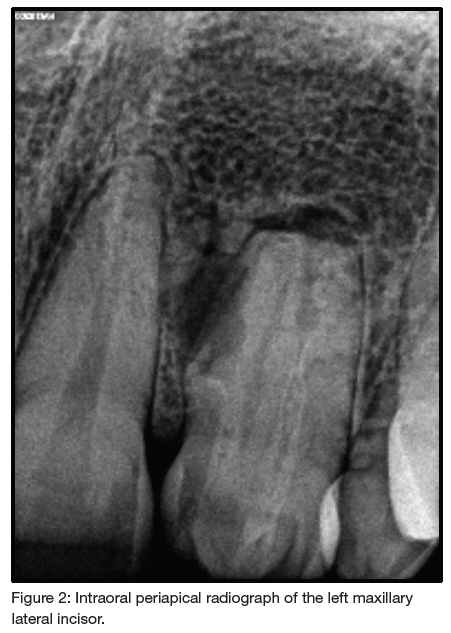
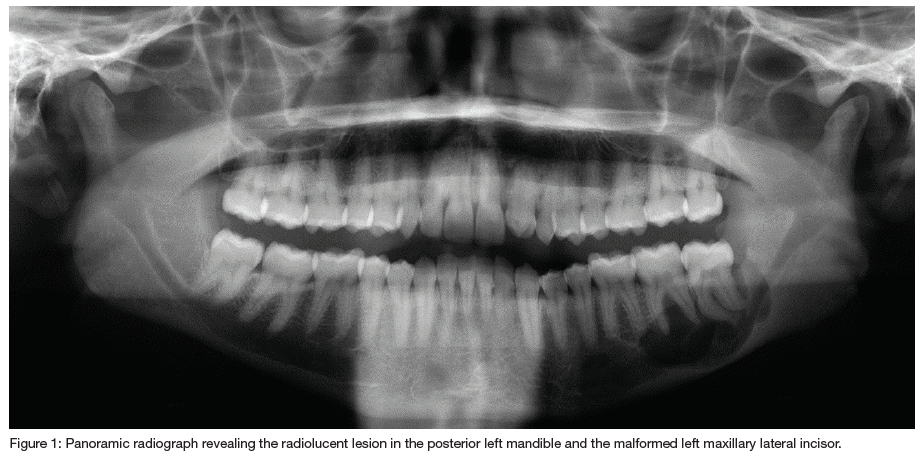
A 27-year-old male patient presented with a six-month history of swelling involving the left posterior mandible. The patient's medical history revealed no co-morbidities and the dental history was non-contributory. Extra-orally, there was a localised hard bony swelling involving the left posterior mandible. Intra-oral examination revealed a full complement of teeth with the left maxillary lateral incisor crown appearing malformed and a retained left maxillary deciduous canine. A panoramic radiograph revealed a well-defined, multilocular radiolucency with scalloped inferior borders in the left posterior mandible associated with the first to third molars (Figure 1). On further examination, a periapical was taken and revealed that the left maxillary lateral incisor appeared malformed with a periapical radiolucency (Figure 2). The periapical radiograph confirmed the presence of a double dens invaginatus on the mesial and distal aspects. The patient was referred for an incisional biopsy of the lesion in the left posterior mandible, which was subsequently diagnosed as an inflamed odontogenic keratocyst and managed accordingly.
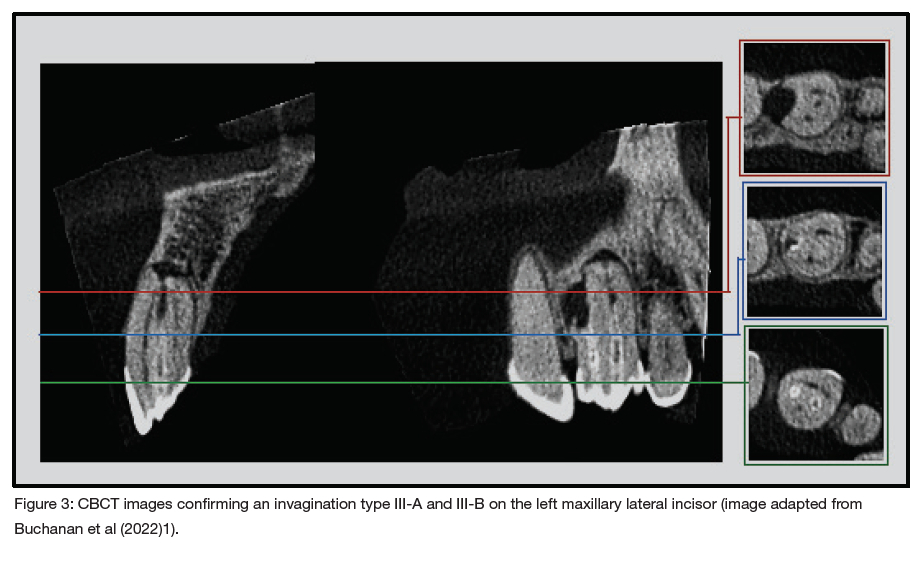
Concurrent referral for endodontic assessment of the left maxillary lateral incisor was made. The tooth had an exaggerated response to vitality testing and was diagnosed with irreversible pulpitis. A decision was made to perform a small field of view cone beam computed tomography (CBCT) scan (90KVp, 8mA and 12 seconds, voxel size 200pm) to better visualise the root canal morphology (Figure 3). The CBCT scan of the left maxillary lateral incisor confirmed two type III dens invaginatus and two canals. The mesial invagination was classified as a type III-A and the distal invagination as a type III-B. Additionally, c-shaped canals were noted both anteriorly and posteriorly. The distal invagination lost continuity with the enamel lining in the apical region. External root resorption was present at the apical and mesial aspects of the tooth with associated peri-invaginatus periodontitis.
INTERPRETATION
Dens invaginatus is a dental anomaly consisting of a coronal or radicular surface invagination.2-4 The prevalence of this dental anomaly varies according to the study population, but has been reported to be as high as 12%.5 A low prevalence of this anomaly was, however, reported in a black South African population.1 The affected teeth typically display an altered clinical appearance, with the morphology of the anomaly often varying in presentation.3 In most cases, the invagination is completely lined by enamel, although in some instances, this lining may be interrupted. The theorised pathogenesis involves two developmental errors in odontogenesis. First, an area of retarded growth is engulfed by the rest of the developing tooth germ.6 Second, the cells of the enamel organ proliferate and invaginate into the dental papilla.7 Coronal dens invaginatus, according to Oehlers3, can be classified according to the depth of surface invagination. Type I describes a surface invagination confined to the crown of a tooth, terminating coronally at the cemento-enamel junction (CEJ). In type II, the anomaly extends beyond the CEJ but is confined to the tooth structure, such that there is no communication with the periapical tissues. Micro-communications with the pulpal tissue may be possible. Type III describes a coronal surface invagination that can terminate in either the lateral periodontium (type III-A) or the periapical tissues (type III-B). Type III results in a direct communication, allowing a path for oral flora to the periodontium, leading to peri-invagination periodontitis.3 Pulpitis and pulp necrosis often develop due to the close proximity of the microorganism-harbouring defect and the pulp, through patent dental tubules.2
A study by Kirzioglu and Ceyhan found that type I dens invaginatus were present in 11.3% of the study population, whereas types II and III were only present in 0.7% and 0.8%, respectively. None of the type I cases displayed periapical pathoses, while the incidence increased in types II and III with 4% and 33%, respectively.5 Teeth demonstrating double dens invaginatus on a single tooth have also been reported, but these usually present with type I or II configurations.8-12 Four cases of a double dens invaginatus (type III with type II) have been reported in the literature, two of which were successfully treated with non-surgical endodontic therapy.13-16 A single tooth affected by a triple type II dens invaginatus has been reported, but subsequent radiographic features resemble a compound odontoma.
To the authors' knowledge, there has only been one report, apart from the current case, of a double type III dens invaginatus. This anomaly presented in a fused supernumerary tooth and a maxillary central incisor. Unfortunately, the authors did not report on the treatment of this tooth.17
Dens invaginatus have been treated with different modalities. Successful outcomes were influenced by the pulp vitality, complex anatomy of the invagination and the pulpal or periodontal communications. Treatment can range from fissure sealants, restorations and endodontic therapy to extractions. Treatment success tends to decline as the surface invagination becomes progressively deeper and more complex.18 A combination of surgical and non-surgical endodontic treatment of a type III invaginatus has also shown successful outcomes. Authors emphasise that non-surgical endodontic treatment should initially be performed, following which surgical treatment can be utilised if the non-surgical approach fails.19 In the current case, the double type III dens invaginatus was managed via non-surgical endodontic treatment.
In conclusion, careful radiographic evaluation can lead to the identification of these anomalies as they are most often asymptomatic in the early stages, and early detection can lead to preventative measures instead of complex endodontic treatments.
AUTHORS' DECLARATION
Funding
This research did not receiveanyspecificgrantfromfunding agencies in the public, commercialor not-for-profit sectors.
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethics approval
This study was approved by the University of Pretoria Ethics Committee (Reference no 76/2020). All procedures followed the ethical standards of the Helsinki Declaration of 1975, as revised in 2008.
REFERENCES
1. Buchanan GD, Gamieldien MY, Fabris-Rotelli I, van Schoor A, Uys A. Root and canal morphology of the permanent anterior dentition in a Black South African population using cone-beam computed tomography and two classification systems. J Oral Sci. 2022;64(3):22-0027 [ Links ]
2. Hunter KD, Brierley D. Pathology of the teeth: an update. Diagnostic Histopathol [Internet]. 2017;23(6):275-83. Available from: http://dx.doi.org/10.1016/j.mpdhp.2017.04.005 [ Links ]
3. Oéhlers FA. Dens invaginatus (dilated composite odontome). I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol. 1957;10:1204-18 [ Links ]
4. Bhatt AP, Dholakia HM. Radicular variety of double dens invaginatus. Oral Surgery, Oral Med Oral Pathol. 1975;39(2):284-7 [ Links ]
5. Kirziöglu Z, Ceyhan D. The prevalence of anterior teeth with dens invaginatus in the western mediterranean region of Turkey. Int Endod J. 2009;42(8):727-34 [ Links ]
6. Kronfeld R. Dens in dente. J Dent Res. 1934;14:49-65 [ Links ]
7. Swanson WF, McCarthy FM. Bilateral Dens in dente. J Dent Res. 1947;26:167-71 [ Links ]
8. Nu Nu Lwin H, Phyo Kyaw P, Wai Yan Myint Thu S. Coexistence of true talon cusp and double dens invaginatus in a singletooth: ararecase reportandreview of the literature. Clin Case Reports. 2017;5(12):2017-21 [ Links ]
9. Verma P, Sachdeva S, Mehta M, Goyal S. Bilateral double dens invaginatus in multituberculated maxillary central incisors with impacted supernumerary teeth: A rare case. J Indian Acad Oral Med Radiol. 2015;27(1):127 [ Links ]
10. Babu NSV, Rao K, Milind LS. Rare Case of Double Dens Invaginatus in a Supernumerary Tooth - An Unusual Case Report. 2014;1(5):48-50 [ Links ]
11. da Silva EJNL, Oliveira SG, Zaia AA. Management of a rare case of Class II double dens invaginatus in a maxillary lateral incisor. Dent Press Endod. 2014;4(2):79-82 [ Links ]
12. Zengin AZ, Sumer AP, Celenk P. Double dens invaginatus: report of three cases. Eur J Dent. 2009;3(1):67-70 [ Links ]
13. Koteeswaran, Vishnupriya Chandrasekaran, S Natanasabapathy V. Endodontic management of double dens invaginatus in maxillary central incisor. J Conserv Dent. 2018;21(5):574-7 [ Links ]
14. Ulmansky M, Hjørting-Hansen E, Praetorius F, Haque MF. Benign cementoblastoma. Oral Surgery, Oral Med Oral Pathol. 1994 Jan;77(1):48-55 [ Links ]
15. Vajrabhaya L ongthong. Nonsurgical endodontic treatment of a tooth with double dens in dente. J Endod. 1989;15(7):323-5 [ Links ]
16. Zoya A, Ali S, Alam S, Tewari RK, Mishra SK, Kumar A, et al. Double dens invaginatus with multiple canals in a maxillary central incisor: Retreatment and managing complications. J Endod [Internet]. 2015;41(11):1927-32. Available from: http://dx.doi.org/10.1016/j.joen.2015.08.017 [ Links ]
17 John H, Padmashree S, Jayalekshmy R. Cone Beam Computed Tomography Aided Diagnosis of Double Dens Invaginatus in a Fused Supernumerary Tooth and Maxillary Central Incisor : A Case Report. IJSS Case Reports. 2015;2(5):24-7 [ Links ]
18. Ridell K, Mejäre I, Matsson L. Dens invaginatus: A retrospective study of prophylactic invagination treatment. Int J Paediatr Dent. 2001;11(2):92-7. [ Links ]
19. Fregnani ER, Spinola LFB, Sönego JRO, Bueno CES, De Martin AS. Complex endodontic treatment of an immature type III dens invaginatus. A case report. Int Endod J. 2008;41(10):913-9 [ Links ]
 Correspondence:
Correspondence:
Name: Chané Smit
Email: chane.smit@up.ac.za


{kind=link}
{kind=link}