










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.79 n.1 Johannesburg Feb. 2024
http://dx.doi.org/10.17159/sadj.v79i01.16603
RESEARCH
Self-reported experience of Outreach activities amongst undergraduate Oral Health students at a University in South Africa
C KrugerI; NR NkambuleII; A BhayaIII
IOral Hygienist/Lecturer. MSc Dentistry. Department of Community Dentistry, Faculty of Health Science, University of Pretoria, Pretoria, Gauteng, South Africa. Email: candida.kruger@up.ac.za. ORCID 0000-0001-9448-4138
IICommunity Dentistry Specialist / Senior Lecturer. MChD (Community Dentistry). Department of Community Dentistry, Faculty of Health Science, University of Pretoria, Pretoria, Gauteng, South Africa. Email: zodwa.nkambule@up.ac.za. ORCID 0000-0003-2524-6413
IIIHead of Department. Department of Community Dentistry, Faculty of Health Science, University of Pretoria, Pretoria, Gauteng, South Africa Email: ahmed.bhayat@up.ac.za ORCID 0000-0002-8103-1233
ABSTRACT
INTRODUCTION: Outreach activities (OAs) are structured learning experiences, combining intentional learning goals with services to underserved communities. Oral health students participated on the Phelophepa Train (PT) and school-based programmes (SBPs) as part of their OAs.
AIM AND OBJECTIVES: To evaluate the self-reported experiences of OA amongst undergraduate oral health students.
DESIGN: Cross-sectional which included final year dental (N=62) and oral hygiene students (N= 13) registered in 2019.
METHODS: Information was obtained using a modified, self-administered questionnaire which included the number and type of procedures performed; work-related limitations, personal work benefits, academic development and civic responsibility
RESULTS: The response rate was 93% (N=65) and students performed more procedures on the train compared to the SBP. Most common procedures undertaken by dental students were screening (64%) and restorations (56%) for oral hygiene students it was screenings (92%) and examinations, Assure sealants and screenings 39% on the train and 31% at SBPs. The most common challenges on both the train and SBPs were inadequate materials (74%) and (41%), poor infection control (15%) and (41% and defective equipment (31%) and (38%) respectively.
CONCLUSION: Although students performed a variety of clinical services they reported to have faced a number of challenges. The majority of students reported that OAs exposed them to the needs of the communities and encouraged them to improve their independence and accountability towards patients
Key words: Outreach activities, oral health students, dental services, self and social development, academic, civic responsibility.
INTRODUCTION
Outreach activities (OAs) is defined as structured learning experiences combining intentional learning goals for students with service to the community. (1, 2) The three main objectives of an outreach program are to improve learning, promoting civic engagement, and strengthening communities through addressing their societal needs. Although teaching and training of dental professional follows the traditional teacher-centred method of instruction in which teachers deliver and students receive lessons, OAs activities enhance students learning and prepare them to serve communities. Since the introduction of these activities into the undergraduate dental program, it has shown to educate students, to meet the health care needs of their patients and gain a holistic understanding on the provision of dental care to patients in need. (3, 4) Students who participated in OAs, reported to have gained additional experience of specific clinical procedures, increase in confidence and awareness of career opportunities. (5, 6) These activities have shown to play a vital role in exposing students to community issues such as the barriers to accessing dental care, their civic responsibility to communities, academic development and self-confidence when providing dental care to underserved populations. (7)
Final year dental undergraduate students enrolled in the Bachelor of Dentistry (BChD) and Bachelor of Oral Hygiene (BOH) programmes at the School of Dentistry, University of Pretoria participated in OAs as recommended by the Health Professions Council of South Africa (HPCSA) as part of service learning and teaching. (8) These activities take place under supervision of qualified dentists and oral hygienists via two platforms, local school-based programmes (SBP) in close proximity to the dental school and via the Phelophepa Train (PT). The SBPs include clinical and preventative procedures; the oral hygiene (OH) students perform mostly preventative procedures, whilst dental students perform dental restorations and attend to the relief of pain and sepsis. These procedures often take place in environments different to their current training facility but which could be expected in their eventual working environment.
The PT is regarded as a mobile hospital that provides primary healthcare services to underserved communities through various health specialities in the health sector where infrastructure does not allow. The PT follows a fixed route to different provinces in South Africa and offers medical and dental services. These services are rendered by undergraduate medical and dental students at a minimum cost to communities. The dental services include dental extractions, restorations, scaling and polishing's (S&Ps) and oral hygiene education (OHE).
SBPs take place at identified primary schools in close proximity of the institution of higher learning in a sponsored mobile unit. School children at these schools are screened for possible dental treatment in the beginning of each year. Class lists supplied by the schools are used to identify the school children and possible treatment needed. As part of their Public Oral Health module (POH), dental and oral hygiene students attend these schools two times per week on outreach. This takes place from February to October each year. Procedures that are performed are mostly preventative procedures. All materials, equipment and personal protective equipment (PPE) needed for procedures to be performed are taken from the institution of learning. Students have been involved in the SBPs and PT since 2015 but the impact of these activities has not been evaluated. This study was the first of its kind at a South African University to evaluate its impact on students. Whilst teaching and training of dental professionals is more teacher and patient centred, the inclusion of OAs in the curricula of the dental professional aims to prepare graduates to become independent, confident dental professionals experiencing real life authentic training and learning.
MATERIALS AND METHODS
A cross-sectional analytical study was conducted amongst all final year undergraduate dental (BChD V) (n=62) and oral hygiene (BOH III) (n=13) students registered at a South African University during the 2019 academic year. Therefore, a total of 70 students met the criteria and were included in the sample population. No sampling was required as all final year dental and OH students were invited to participate. A self-administered modified questionnaire consisting of both open and closed questions was used to obtain the necessary information. (9, 10) The questionnaire was anonymous and was assigned a unique serial number.
It consisted of five sections and 42 questions in total. The first section dealt with demographics, including age, race and gender.
The second and third sections dealt with the PT and SBPs respectively and included the types and numbers of clinical procedures performed, work related limitations, personal work benefits and traits of self and personal development. The number of procedures performed were classified into five categories (0, 1-5; 6-10; 11-15 and more than 16) and students were asked to choose which category best described the number of specific procedures performed. Based on the range of data we received and for statistical ease, it was decided to categorise the data into these categories.
The fourth and fifth section dealt with the academic development and civic responsibility of the students and included their academic curriculum, levels of theoretical learning, contribution to rendering dental services, motivation to contribute to social responsibility of underserved communities and responsibility and moral obligation to communities.
Data was captured on an Excel spreadsheet and then imported onto Statistical Package for the Social Sciences (SPSS) software version 27 and descriptive statistics for reporting the results.
Ethical clearance and permission to conduct the study was obtained from the University of Pretoria, Research Ethics Committee of the Faculty of Health Sciences (643/2019). All information was strictly confidential.
RESULTS
Of the 70 students who met the criteria, 65 (93%) signed the consent forms and were included in the study (response rate=93%). The mean age was 22.7yrs (±5.46) and 71% were females.
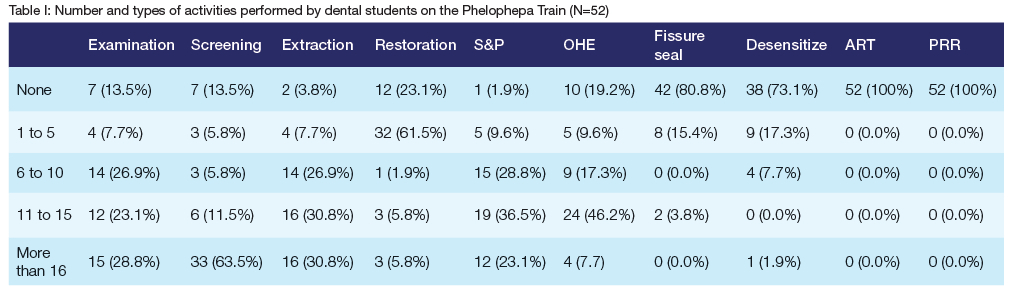
Number and type of activities performed by dental students on the PT
Almost two-thirds (64%) reported they screened more than 16 patients per day while 46% reported to have provided (OHE) to between 11 and 15 patients per day. Almost two-thirds (62%) performed one to five restorations per day and 37% reported to complete between 11 and 15 S&Ps per day. None reported to have performed Atraumatic Restorative Treatment (ART) or Preventive Resin Restorations (PRR) as shown in Table I.
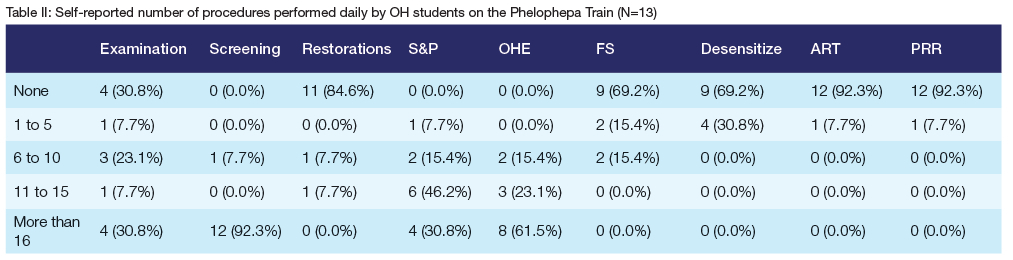
Number and type of activities performed by OH students on the PT
Almost half (46 %) reported that they performed between 11 and 15 S&Ps, 92% reported to have performed 16 or more screenings and 61% reported to have delivered 16 or more OHE sessions per day. Only 30% reported to complete Assure sealants (FS) and desensitizing procedures. (Table II)
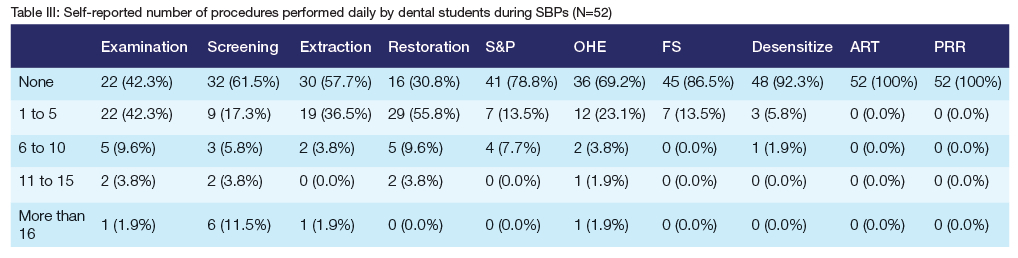
Number and type of activities performed by dental students on SBPS
Over half (56%) reported that they performed one to Ave restorations while 85% reported to have completed five or fewer examinations per day. Almost two-thirds (58%) reported not completing any extractions per day. None reported to have performed ART or PRRs in Table III.
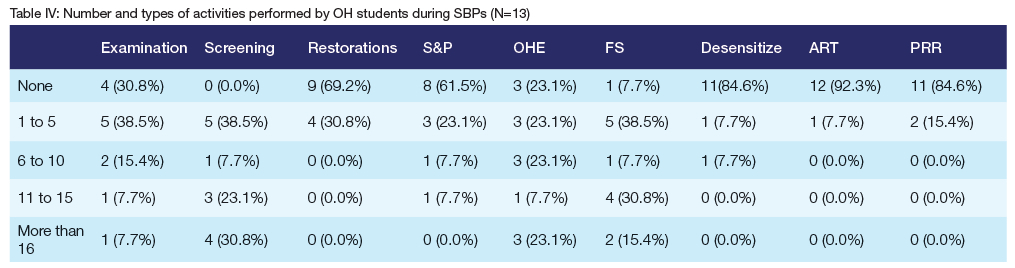
Number and type of activities performed by OH students during SBPs
Almost a third (31%) reported to have screened more than 16 patients while 31% reported to have placed between 11 and 15 FS per day. Almost a quarter (23%) performed one to five OHE sessions per day while 23% reported to complete between 1 and 5 S&Ps per day. Only less than 10% performed any ART while 15% reported to have placed PRRs as shown in Table IV.
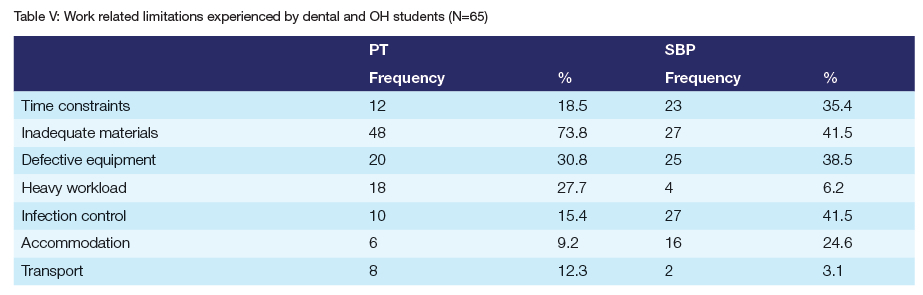
Work related limitations experienced by dental and OH students
The most common limitations reported were inadequate materials at the PT (74%) and SBPs (42%) respectively; defective equipment on PT (31%) and at SBPs (39%) and inadequate infection control measures (42%) at SBPs and (15%) on the PT. (Table V)
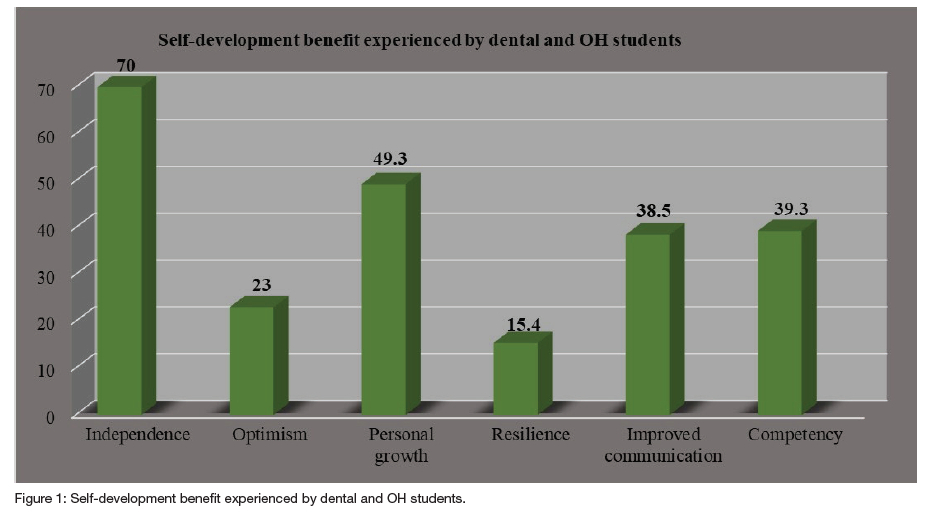
Self-development benefit experienced by dental and OH students
Almost all students (70%) reported that their self-development improved because of working independently on the OAs. Half (49.3%) of students reported that their self-development improved due to personal growth while 39.3% felt that their competency skills improved on the outreach. (Figure 1)
Academic development
Majority of students (91%) agreed that taking accountability for their own learning after participation in OAs and that involvement with other disciplines improved their awareness of OAs. The majority of students (86%) reported that their academic curriculum prepared them effectively to treat patients of diverse ethnicity on OAs and 82% reported that their applied theoretical leaning assisted them on OAs.
DISCUSSION
The response rate was 93% and this was similar to other studies that reported on the impact of dental outreach programs that had response rates between 90% and 97%. (7, 11, 12) The response rate could be due to the questionnaire being handed out to participants during a contact lecture session.
The participant's average age was 22 years with 71% being female. This is consistent with the demographics of dental and oral hygiene students as in the recent years, more females have been accepted to these professions. (13)
At both outreach sites students reported performing a number of different types of procedures. The most common procedures performed were screenings and OHE. The most common procedure performed by dental students were examinations and restorations. The high number of screenings could be due to the high number of patients that presented at these sites who needed to be treated. The demand for extractions and restorations were similar to another study, which reported that dental students completed mostly examinations, dental extractions and restorations (Bhayat et al., 2011).
The high demand for extractions is possibly attributed to the high volume of patients in underserved communities with low socioeconomic status seeking relief from pain and sepsis. (14) This often results in decay extending into the pulp which limit the options and extractions are then the only means dealing with the disease. This is similar to the survey completed by South African Demographic and Health Survey (SADHS) (National Department of Health and ICF, 2019) in 2016 where respondents reported that the main reasons for them not seeking treatment was that treatment was too expensive; all services were not available and that sites were far to access the treatment. A similar study by Bhayat et al reported that the most common procedures performed at Primary Oral Health Care Facilities (POHCF's) in Gauteng were dental extractions, restorations and fissure sealants.(15) In addition, OH students reported to perform more FS at SBPs and this could be due to the fact that FS are placed mostly on school children while more S&Ps were performed on the PT which could be due to the adult population thatattended for °ervices and the possible lack of good oral hygiene aids like toothbrushes and toothpaste.
During SBPs, students had time to complete more procedures. This was possibly as a result that there were fewer patients that needed treatment; however, they completed more preventive procedures at the school. Possibly due to patients being young and more relaxed as opposed to the normal dental setting and had a better dental IQ by creating a space for patients to voice their choices. It could also be due to the fact that these children were screened and early caries was detected and prevented rather than waiting for patients to attend dental clinics after having pain and irreversible tooth damage and alleviate anxiety.
Possible reasons for the low performance of ART and PRRs were the severe state of caries that patients presented with which resulted in more invasive treatment options, a lack of radiographic equipment to diagnose the severity of the carious lesions and a possible lack of materials and equipment. As result students were forced to perform more extractions and restorations rather than conservative ART and PRR procedures.
The most common work-related limitation was inadequate materials which was similar to other studies. 14) Inadequate materials should not necessarily be perceived as not having enough materials to perform procedures. The possibility exists that students weren't exposed to similar materials used at their institution of higher education. Facilities and institutions are obligated to manage and improvise when materials are supplied due to inadequate budgets. (16)
Defective equipment was another work-related limitation and this was also reported by other authors. (11,14) The defective equipment could possibly be due to damaged equipment, old dental units not being maintained regularly, budget constraints forcing staff at the facilities not to replace defective equipment and modern hand pieces and equipment's non-availability.
More than half reported that infection control measures were insufficient. This compared to a similar study where 26% of students objected to infection control measures that were implemented at an outreach site. (10) In addition, possible cross infection contamination was of a concern to students, as the situation was different as to what they experienced at their clinical training institution.
More than two thirds (70%) of students felt that their confidence had greatly improved due to the increased independence and being allowed to make own decisions clinically which was similar to a previous study. (17) This could be as a result of them being allowed to formulate a clinical diagnosis independently, work in a multi-disciplinary team of professionals and work at rural sites and within communities which occur at OAs compared to the dental school environment. In the present study, 98% of students reported that their personal growth had improved. This could be due to the impact of OAs on academic development which could have made it easier for participants to understand the theory from lectures in a greater degree as reported by previous studies. (7)
Less than half (39%) reported that their competency skills improved compared and this was considerably lower to another study which reported that between 83-97% of students rated themselves as being more confident in preventive treatments. (18)
Outreach activities impact on the Academic development and Civic responsibility of students
Academic development
Almost all of the respondents (91%) strongly agreed that participating in OAs made them more accountable for their own learning and that involvement with other disciplines improved their awareness of OAs. This was considerably higher than other similar studies, which reported that between 51% and 74% of students who felt the same. (7 14) This could be due to them being exposed to various patient groups, ages, different cultures and socioeconomic background.
Experiential learning is constructing knowledge and meaning from real-life experience. In the context of medical education, the term is most commonly applied to experiences which have been included in a curriculum design to bring the learner into contact with others in a particular role and context. (19) Experience gained in authentic workplaces that are concurrently involved in education and delivering reallife services is the most important medium through which people learn to practice as healthcare professionals. Most of the students strongly agreed that their academic curriculum prepared them effectively to treat patients similar to other studies. (7, 11) As a result, when participants understand and apply theoretical concepts in real life situations, it improves the quality of services.
Civic responsibility
Almost all students reported that during and after participation of OAs they were more responsive to the needs of attended communities and they believed their motivation to treat underserved communities would contribute immensely to their social responsibility after qualifying as dental professionals. This was similar to studies which showed over 96% of students became more aware of the needs of communities, made them aware of their roles in the community and agreeing that they have a rebsponsibility to serve the community. (7, 11, 14, 20, 21)
Students experienced an 88% responsibility and moral obligation to the community and the people after participation. This was similar to other studies which reported that over 99% of participants agreed they have a responsibility to serve the community and become more aware of the community's needs and that it was their responsibility to serve their community. (7, 11) Therefore the supposition that reconnecting with communities, critical thinking in applying their skill and building relationships with people who have authentic challenges is a manner in which OAs assists students accepting responsibility and realizing the need that exits in the underserved communities. (7)
LIMITATIONS
In this retrospective cross-sectional study, students expressed and associated their experiences on OAs based on what they remembered after a period of time had passed and therefore resulting in response bias. The students could have also responded according to what they felt was the correct response rather than the actual occurrences (Response acquiescence). Unfortunately, these are common limitations of cross-sectional survey design studies. No inferential statistics were performed as this was a cross sectional descriptive study.
RECOMMENDATIONS
Defective equipment needs to be assessed, replaced and maintained within budgetary limits. Future studies should be done to evaluate compliance to infection control policies and practices at outreach sites to align to the institution of higher education.
CONC LUSION
Students performed a range of preventive and restorative procedures during the OAs which were in line with their scope of practice and with the dental demand of patients attending these sites. The most common challenges faced on OAs included defective equipment, inadequate materials and a lack of infection control measures. Autonomy to work alone and the exposure to the community encouraged students to develop and improve their independence, accountability, humanitarianism and compassion towards communities and patients through their engagement of service learning on outreach programs.
REFERENCES
1. Aston-Brown RE, Branson B, Gadbury-Amyot CC, Bray KK. Utilizing public health clinics for service-Learning rotations in dental hygiene: a four-year retrospective study. J Dent Educ. 2009;73(3):358-74. [ Links ]
2. Hood JG. Service-learning in dental education: meeting needs and challenges. J Dent Educ. 2009;73(4):454-63. [ Links ]
3. Mofidi M, Strauss R, Pitner LL, Sandler ES. Dental students' reflections on their community-based experiences: the use of critical incidents. J Dent Educ. 2003;67(5):515-23. [ Links ]
4. Finucane D, Nunn J, O'CONNELL A. Paediatric dentistry experience of the first cohort of students to graduate from Dublin Dental School and Hospital under the new curriculum. Int J Paediatr Dent. 2004;14(6):402-8. [ Links ]
5. Smith M, Lennon M, Brook A, Ritucci L, Robinson P. Student perspectives on their recent dental outreach placement experiences. Eur J Dent Educ. 2006;10(2):80-6. [ Links ]
6. Lynch CD, Ash PJ, Chadwick BL, Hannigan A. Effect of community-based clinical teaching programs on student confidence: a view from the United Kingdom. J Dent Educ. 2010;74(5):510-6. [ Links ]
7. Suresan V, Jnaneswar A, Swati S, Jha K, Goutham BS, Kumar G. The impact of outreach programs on academics development, personal development and civic responsibilities of dental students in Bhubaneswar city. Journal of Education and Health Promotion. 2019;8. [ Links ]
8. Health Professions Council of South Africa [Internet]. ACT 56 OF 1974 Regulations relating to the registration of students, undergraduate curricula and professional examinations in Dentistry. [Published under Government Notice R140 in Government Gazette 31886 of 19 February 2009,cited 7 December 2020] CHAPTER 2. Available from:https://www.hpcsa.co.za/Uploads/MDB/Rules%20%26%20Regulations/regulations_gnr_140_2009.pdf [ Links ]
9. Shinnamon AF, Gelmon SB, Holland BA. Methods and strategies for assessing service-learning in the health professions. 1999. [ Links ]
10. Gaeth B. Dental service-learning curriculum and community outreach programs perception vs. practice. 2011. [ Links ]
11. Bhayat A, Mahrous M. Impact of outreach activities at the College of Dentistry, Taibah University. Journal of Taibah University Medical Sciences. 2012;7(1):19-22. [ Links ]
12. Johnson I, Hunter L, Chestnutt IG. Undergraduate students' experiences of outreach placements in dental secondary care settings. Eur J Dent Educ. 2012;16(4):213-7. [ Links ]
13. Stormon N, Beckett D, Gardner S, Keshoor S, Smart K, Wallace L, et al. Empathetic, persistent and female: A snapshot of oral health therapy students in Australia and New Zealand. Eur J Dent Educ. 2022;26(1):206-15. [ Links ]
14. Bhayat A, Vergotine G, Yengopal V, Rudolph MJ. The impact of service-learning on two groups of South African dental students. J Dent Educ. 2011;75(11):1482-8. [ Links ]
15. Bhayat A, Madiba TK, Nkambule NR. A three-year audit of dental services at primary health care facilities in gauteng, south africa: 2017 to 2019. Journal of International Society of Preventive & Community Dentistry. 2020;10(4):452. [ Links ]
16. Schaay N, Sanders D. International perspective on primary health care over the past 30 years: primary health care: in context. South African health review. 2008;2008(1):3-16. [ Links ]
17. Lynch C, Ash P, Chadwick B. Community-based dental hygiene and therapy education. Vital. 2011;9(1):39-43. [ Links ]
18. Rodd HD, Farman M, Albadri S, Mackie IC. Undergraduate experience and selfassessed confidence in paediatric dentistry: comparison of three UK dental schools. Br Dent J. 2010;208(5):221-5. [ Links ]
19. Yardley S, Teunissen PW, Dornan T. Experiential learning: transforming theory into practice. Med Teach. 2012;34(2):161-4. [ Links ]
20. Fitch P. Cultural competence and dental hygiene care delivery: integrating cultural care into the dental hygiene process of care. J Dent Hyg. 2004;78(1). [ Links ]
21. Major N, McQuistan MR, Qian F. Changes in dental students' attitudes about treating underserved populations: a longitudinal study. J Dent Educ. 2016;80(5):517-25. [ Links ]
 Correspondence:
Correspondence:
Ntombizodwa R Nkambule
Department of Community Dentistry, Faculty of Health Science
University of Pretoria
Pretoria, Gauteng, South Africa.
Tel: +27 12 319 2247/ +27 )82 772 5135
E-mail: zodwa.nkambule@up.ac.za
Author contribution
1 . Mrs C Kruger 40% - Identification of topic, literature review, write up and data collection.
2 . Dr NR Nkambule 30% - Introduction, data analysis and writing up of paper.
3 . Prof A Bhayat 30% - Methodology section, discussion and writing up of paper.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}