










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Dental Journal
versión On-line ISSN 0375-1562
versión impresa ISSN 0011-8516
S. Afr. dent. j. vol.78 no.8 Johannesburg sep. 2023
ETHICS
Inaccessible specialised oral health services in South Africa - rationing policy uncertainty
D Pagollang MotlobaI; Pumela Rocky-Queen GwenguII; Pusetso D MoipolaiIII
IMDent (Comm Dent) (Medunsa), MBL (Unisa), Head of Department - Community Dentistry, Sefako Makgatho Healtl Sciences University. ORCID: 0000-0003-1379-7576
IIDip OHOH, BDS, MPH, Mdent (Comm Dent), Head of Department - Operative Dentistry, Sefako Makgatho Health Sciences University
IIIBChD (Leeds, UK), Mdent (Pros)(Wits), Med (Wits), Head of Department - Prosthodontics, Sefako Makgatho Health Sciences University. ORCID: 0000-0003-0388-5898
ABSTRACT
BACKGROUND: Rationing by waiting lists is associated with patient costs such as pain, anxiety and poor health outcomes. Rationing is indicative of a mismatch between the demands and resources to service patients' needs. Long waiting times for specialised oral health services are concerning and unjustifiable. The majority of oral health care services are devoid of an explicit policy and mechanism to address this problem. This paper attempts to provide the ethical basis for waiting times. That is, whether the mechanisms used in the allocation of services (or placing patients on waiting lists) is consistent with ethical principles
METHODOLOGY: The focus of the discussion will be on the theories of justice, which better explicate fairness, especially in the rationing of scarce resources. Among the dominant theories discussed are utilitarianism, egalitarianism and maximin
CONCLUSION: Waiting times for specialised oral health services can be long, arduous and indefinite. This form of rationing can be viewed as unjust given the lack of transparent and objective policies and guidelines. The oral health services must develop and implement appropriate rationing regimes to strengthen equitable access to services and allocation of scarce resources
CONTEXTUALISING WAITING TIMES FOR SPECIALISED ORAL HEALTH SERVICES
Waiting times - epitome of the failed two-tiered health system
Rationing can be defined as denying a potentially beneficial treatment to a patient on the grounds of scarcity.1 Rationing of oral health services includes restrictions in the allocation of treatment options and procedures, especially specialised dental services. Rationing means that restrictions may be imposed on the type of services provided, and when and how often patients would be eligible for care.2 Consequently, patients may not receive the care at point of service; treatment may be postponed or delayed, sometimes indefinitely. The failure to provide critical care impacts clinical outcomes and the quality of life. Long waiting times for dental care indicates the failure of a health system to meet the demands and needs of patients. Long waits, postponement of critical treatment or deferment of services are symptoms of an oral health service that is incapacitated or overburdened or dysfunctional.
Extended waiting times are particularly prevalent in a two-tiered system, which invariably perpetuates health inequality and poor access to care.3 First, the private health sector services a small minority of patients requiring specialised oral health services. For example, and depending on the medical aid cover, patients may not have adequate benefits for orthodontics, prosthodontics or even endodontic treatment. The resultant "dumping" occurs when desperate patients are forced to seek dental care in the public sector, as their dental cover runs out.4 This situation culminates in an overburdened public sector, which further compromises the delivery of services in this sector. The private sector is also prone to overservicing of a few insured individuals. This practice is inefficient, wasteful and perpetuates inequity in oral health.5
Second, the public sector tends to experience overcrowding and long waiting times as it grapples with servicing the uninsured majority (85%).6 With limited resources, decaying infrastructure and poor maintenance, this sector is unable to always provide the required services for all patients, at all times. Additionally, public oral health care in South Africa does not enjoy special dispensation regarding funding and resourcing. Over the years, public funding of this sector has been gradually attenuated. This underresourcing was aggravated by incorporating and amalgamating oral health into other services and programmes. For example, oral health is funded under specialised services and classified under the noncommunicable diseases cluster. This repositioning has resulted in critical funding not being ring-fenced for oral health. This has led to underresourcing and a plethora of adverse outcomes for the sector. Under these circumstances, it is inconceivable how the oral health services will manage the ever-increasing specialised oral health needs. Currently, the oral health services are inundated with the management of pain and sepsis. It is thus incumbent on services to develop innovative policies and interventions to tackle waiting lists and improve access to critical care. Unless such policies are adopted, millions of patients will continue to wait for oral health services in perpetuity.
Waiting times - dental schools as the last resort
In the context of South Africa, specialised oral health services include procedures ordinarily offered by dental practitioners. For example, basic prosthodontic procedures, minor oral surgery, endodontic treatment and, in some desperate circumstances, basic dental services such as direct restorations are scheduled. For most patients seeking specialised oral health services in South Africa, the dental schools are absolutely the last resort. These institutions are publicly funded and largely use the services of postgraduate clinical candidates to provide essential oral health services as part of their training. Unlike medical schools, dental schools are resource intensive and require dedicated funding to perform optimally. Unfortunately, dental schools remain severely underresourced to provide costly specialised services. A typical dental school employs not more than 100 clinicians to manage an average of 3,000 patients every month. The huge demand for specialised oral health services, additional academic responsibilities of the clinicians, dysfunctional public oral health system and unaffordable private health care are some of the challenges facing the oral health service. This quadruple burden on the staff and services implies that patients will be placed on a waiting list (sometimes indefinitely) or will wait for extended periods of time before receiving the appropriate treatment. For the purpose of this paper, waiting times and waiting lists are used interchangeably.
Aims and objectives
Despite the widespread use of waiting times in the allocation of oral health services, little has been published about the moral justification of these scarce resources. Limited discussions about waiting time focus on problems of application, such as the association of waiting times with social privilege. Focusing only on the application of waiting times misses critical normative questions about the justification of rationing schemes. Consequently, no moral guidance can be incorporated into future allocations using waiting times. The objective of this paper is to explore the ethics of waiting times in oral health services. That is: (i) which moral framework has been adopted in rationing oral health services, if any? ii) whether waiting times or waiting lists policies are adequately designed to usher just and fair rationing of limited resources.
JUSTICE - THE BASIS OF RATIONING POLICY CHOICES
The argument for rationing policy is based on the following premises: (i) health resources are not infinite, and the health needs are ever-increasing (ii) rationing of health care resources is inevitable and necessary, more so in resource-deprived settings; (iii) a just rationing policy is a critical element of a just health system; (iv) equitable health services ought to develop and implement just and explicit rationing policy.
The constitution provides a legal and moral framework for health services to develop and implement explicit and just rationing policy. In practice, however, health services allocate scarce resources based on unclear, unwritten and implicit rationing regimes. Consequently, the services are unable to express (i) clearly and consistently who shall and who shall not receive care; (ii) when, how and what criteria are applied when rationing limited resources. Unclear rationing policies undermine the right to health and compromises the delivery of equitable and accessible health for all.
We premise our moral claim for just rationing regime on (i) Daniels7 argument for a strong right to health care and (ii) Rawls8 justice principle of "fair equality of opportunity". These philosophers purport that the denial of health services increases propensity of disease and disability, and invariably diminish people's "normal species functioning"9 and results in a restriction of the range of opportunities open to them. Waiting times or long waiting lists are tantamount to the denial of health services, which limits the individual's opportunities. Unless the processes and procedures regarding the waiting lists are fair, then the allocation of services cannot be deemed to be just.
Several rationing regimens have demonstrated potential to improve access and allocation of limited health resources: (i) first come first served basis10; (ii) treatment of the worst-off patients11; (iii) prioritisation of those who are able to benefit the most from the intervention12 (ceteris paribus). While some of these regimens have been implemented in health services, their moral underpinnings remain indeterminate. Below are theories of justice that explain the rationing of scarce health resources.
MORAL THEORIES AND WAITING TIMES
a. Utilitarianism
Utilitarianism is a consequentialist approach, rooted in the belief that moral rightness is dependent on the consequences of the act or rule and nothing else. This philosophical view emphasises the maximisation of benefits or outcomes. According to Bentham and Mill, an act or rule is morally right if and only if it results in "the greatest happiness for the greatest number".13,14 Classical utilitarianism is complex, as it seeks to be explicit about the nature and the maximisation of the value of consequence or utility. To fully comprehend the utility of actions, programmes or policies, the nature of the consequence must be clearly defined. Additionally, the utility of the action or programme must be objectively measured. Failure to define and quantify the utility of the policy could invalidate the evaluation of the policy.15
According to utilitarianism, access to care, priority setting,or reduction in waiting times should be based primarily on the actual or anticipated change in health outcomes of the affected patients. Accordingly, (i) the young would be prioritised ahead of the old; (ii) those with the least cost per gain would be chosen; and (iii) those most likely to benefit are selected for care. In so doing the outcomes will result in the maximised benefits and huge returns on the investments (health services provided). The first on the waiting list will be those most likely to increase the utility of the health service and nothing else.
b. Egalitarianism
The egalitarian theories of justice deal with the question "what should be equal or be distributed equally?" In a resource constrained environment, it is not feasible to distribute everything equally, more so in health care. Hence the question, what specific aspects of health care service should be equal or equalised? Should it be (i) equality of health or in health? That is health outcomes or quality of life; (ii) contribution towards health (including services); and (iii) equality in the use of health services (access). Applying the egalitarian principle of justice to equality of health would mean that (i) all individuals must enjoy the same levels of health; and (ii) the only consideration should be the need. Therefore, the health system should prioritise those with poor health to "restore" to equal health. This state of health can only be achieved by shifting resources away from and to the detriment of those with better health. This concept of "fair earnings" suggests that people above a certain defined health threshold are luckily living on "borrowed health" and have surpassed or extended their health benefits.16,17 Similarly, the persons below this threshold are being denied the opportunity to realise equal or comparable health positions. An egalitarian approach to rationing may not be the most efficient or effective way of achieving the overall goal of health care, which is to improve the health and wellbeing of the population. The application of this moral theory could have unintended consequences for the following reasons: First, the health outcomes of healthier patients could deteriorate due to limited care for this group. Second, the health benefits of interventions might not be fully realised in patients with the worst health status. Ultimately, this system might result in a lose-lose situation. This egalitarian approach has two serious limitations: (i) it is oblivious to antecedent factors and their impact on future health status; (ii) the assumption that healthcare services can completely address, resolve, reverse and equalise the existing differences in health conditions is flawed. Regarding the contribution towards health care, the egalitarians advocate for proportional contribution commensurate with income and the ability to pay. This approach is reflected in modern health system policies such as the National Health Insurance (NHI). Ultimately, the egalitarian view of just health care supports equal access to care and the use of services. Therefore, the costs of care should be reduced or be free for low-income groups.
Regarding waiting times, this framework implies the following:
• equalising access to the same treatment for the same illness;
• similar waiting times irrespective of the type of treatment, and reasons for the intervention; and
• prioritising those with greatest needs to achieve equality of health outcomes.
This framework is not explicit when the costs of treatment and treatment outcomes are comparable between two candidates. Should priority be given to the individual likely to benefit the most from the treatment, the worst-off or on first come first served? Similarly, this moral theory cannot fully explain how justice can be assured when two different patients (demographics, clinical attributes) require similar treatment.
c. Maximin principle (principle of good)
This principle is aimed at maximising liberties or opportunities and minimising inequality or disadvantage.18 This distributive justice principle is premised on the assumption that all rational beings will develop the best solution for any situation provided they: (i) operate behind the veil of ignorance and (ii) their starting point is in the original position. Applied to health care, this theory indicates that priority should be given to maximise outcomes, especially among the worst off. Therefore, the indigent, with the worst economic and social opportunities, need to be prioritised and given more access to care. Furthermore, those who are likely to suffer the worst health outcomes if left untreated should be attended to urgently or promptly. This is tantamount to minimising disadvantage among those with "bad" health outcomes. Simultaneously, those with fair to moderate health are deprioritised. Therefore, one's health must be the worst among the cohort to receive treatment. Those "having bad luck" should not receive further misfortune by not receiving health care. This theoretical stance does not support health promotion and prevention initiatives. In terms of access to care (reduction of waiting times), those likely to have the worst complications should be treated first.
COMPARISON OF MORAL THEORIES
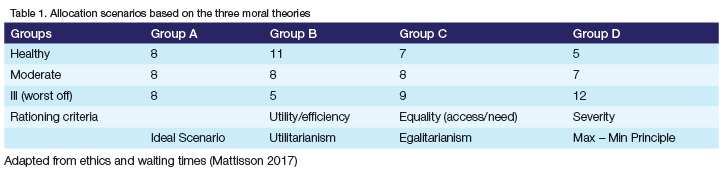
Table 1 illustrates the favoured health outcomes of 24 hypothetical patients under three different moral theories. Group A represents the ideal rationing position, and a fictitious scenario in which resources are allocated equally based on all the theories. This situation does not exist in real life, as health care services are fraught with scarcity of resources. For utilitarianism (Group B), efficacy or net benefit is the goal for rationing at the expense of distributive fairness, equity or capacity to benefit. Therefore, patients who are prioritised for specialised oral health services under this moral theory must have reasonable to good oral health, which is likely to result in greater utility. Patients in this group have comparatively better oral health and may require minimal interaction with the health system. These patients are few and far in between in South Africa, which is inundated with a huge burden of oral diseases. There is a disproportionate prevalence of oral conditions such as dental caries, periodontal diseases and trauma among the uninsured indigent majority.
Egalitarianism (Group C) should ensure the most equal and fair distribution of benefits and costs at the expense of total health. Irrespective of moderating factors, such as income, education etc, patients will enjoy the same level of dental care for the same conditions or needs. Egalitarianism can be viewed as a means of respecting the equal moral worth and dignity of every human being, and avoiding discrimination or unfairness based on factors that are beyond the individual's control. Group D maximises the outcomes for the worst off and neglects equity and efficacy.
The severity of the health condition is the only measure to be considered. Patients with the worst oral health status will receive priority and not be placed on waiting lists whenever possible. All the rationing scenarios that moral theories seek to address exist simultaneously and in varying degrees in the public oral health system.19 Hence the observed hesitancy or unwillingness to develop and implement a singular or combination of these rationing strategies.
DISCUSSION
Waiting time is widely used in health to make resource allocation decisions, yet no general account of the moral significance of waiting time exists. We premise this discussion on the claim that oral services in South Africa do not have a clear and transparent rationing policy. Notwithstanding the legal and constitutional provisions, there ought to be - at the health facility level - some form of a detailed plan to implement the letter of the law regarding the delivery of health care. According to the South African constitution, no patient can be refused care in the public service because of (i) their inability to pay; (ii) their oral health status; (iii) the type of service they need, specifically dental emergencies. However, waiting lists and deferment of oral health care is inevitable in resource-scarce health systems. Subjectively, the essence of the right to health is that it is absolute. Objectively, not as a matter of theory but as a matter of fact, no right, including health, can be absolute. Hence, what a health service can grant or allow is never absolute. However, oral health services should find a way to allocate scarce resources to meet the desired outcomes of the patient.
We argue that, in practice, patients are placed on waiting lists because there is a lack of a clear rationing policy. Clinicians and administrators use their own prerogative in assigning patients spots and places on the waiting lists, a practice that is ill-informed, unethical, unlawful and unjustifiable. Rationing by clinicians is largely informed by the "medical condition" rationale and, in many cases, nothing else. Therefore, other compelling factors outside the medical reasoning are ignored and not explicitly embedded into the rationing formulary. In most circumstances, patients will receive care if and when health officials deem it necessary. Public oral health services generally adhere to public priority-setting guidelines as a rationing tool and reject the market-based utility-maximisation and efficiency paradigm. In other words, publicly funded services have a prima facie preference for egalitarianism and maximin principles than the utilitarian framework. That is, the public service will not consider how removing a patient from a waiting list would then maximise quality-adjusted life-year (QALYs).20,21 This economic measure represents the utilitarian paradigm, which does not support the notion that all citizens contribute to the fiscus and cannot be subjected to market principles. Alternatively, non-utilitarian assumptions such as societal preference should be incorporated into the economic theory for rationing in the public health service to improve its acceptability. We contend that waiting times are not intrinsically morally significant, but how they are used across a range of clinical scenarios is. First, oral health services have a duty of fairness in servicing waiting lists where a sufficiently just queue exists. Second, where patients are in relevantly similar circumstances, the use of waiting times to allocate services is efficient and maximises distribution equality.
Beyond the scope of this paper, further questions relating to rationing should beexplored to get afullergrasp ofthe intricacies of waiting Iists: (i) How can the value of health be measured and objectively quantified'? (ii) What does it mean that a treatment is"good value for money"? (iii) What value is derived from indefinite deferment of health services? (iv) What distributive principles - utilitarian, egalitarian or prioritarian - should be relied on in rationing specialised oral health services?
CONCLUSION
The policies and guidelines used to ration specialiased oral health care servies in South Africa lack transparency and are not underpinned by explicit moral theory. Consequently, eligible and deserving patients might not receive appropriate care at the appropriate time. It is incumbent of oral health services to develop and implement just and explicit policies to allocate scarce resources.
Author's contribution
1. Prof D Pagollang Motloba - 50%
2. Dr Pumela RQ Gwengu - 15%
3. Prof Pusetso D Moipolai - 35%
REFERENCES
1. Moosa MR, Luyckx VA. The realities of rationing in health care. Nature Reviews Nephrology.2021; 17(7): 435-6 [ Links ]
2. Tauber AI. Medicine, public health, and the ethics of rationing. Perspectives in Biology and Medicine.2002; 45(1):16-30. https://doi.org/10.1353/pbm.2002.0018 [ Links ]
3. Human A. A Comparison of Health Care Systems: South Africa vs. Canada. UBC Medical Journal.2010; 2(1): 33 [ Links ]
4. Rice MF, Jones W Jr. The uninsured and patient dumping: recent policy responses in indigent care. J Natl Med Assoc. 1991;83(10):874-80 [ Links ]
5. McQuoid-Mason DJ. 'Over-servicing', 'underservicing' and 'abandonment': What is the law? South African Medical Journal.2015; 105(3):181-182 [ Links ]
6. Moosa S, Carmichael T, Luiz J, Peersman W et al. Insights of private general practitioners in group practice on the introduction of National Health Insurance in South Africa. African Journal of PrimaryHealthCare and Family Medicine.2016; 8(1): 1-6 [ Links ]
7. Daniels, Norman. "Rights to health care and distributive justice: programmatic worries." Health Rights. 2017: 23-40 [ Links ]
8. Alexander LA. Fair equality of opportunity: John Rawls'(best) forgotten principle. Philosophy Research Archives.1985; 11:197-208 [ Links ]
9. Lanoix M. From normal species functioning to capabilities, is it enough? The American Journal of Bioethics. 2013; 13(8): 20-1. https://doi.org/10.1080/15265161.2013.804337 [ Links ]
10. John TM, Millum J. First come, first served? Ethics.2020; 130(2):179-207 [ Links ]
11. Veatch RM. Healthcare rationing through global budgeting: the ethical choices. The Journal of Clinical Ethics.1994; 5(4):291-6 [ Links ]
12. Persad G, Wertheimer A, Emanuel EJ. (2009). Principles for allocation of scarce medical interventions. The Lancet.2009;373(9661):423-31. https://doi.org/10.1016/S0140-6736(09)60137-9 [ Links ]
13. Bentham J. (1830). The greatest happiness of the greatest number. Bentham's political thought.1830: 309-310 [ Links ]
14. Veenhoven R. Greater happiness for a greater number: Is that possible? If so, how. Designing Positive Psychology. 2011: 396-409 [ Links ]
15. Mill JS. Utilitarianism. In Seven Masterpieces of Philosophy.2016: 329-375 [ Links ]
16. Farrant A. The fair innings argument and increasing life spans. Journal of Medical Ethics.2009; 35(1):53-56. http://dx.doi.org/10.1136/jme.2007.023762 [ Links ]
17. Bognar G. Fair innings. Bioethics.2015; 29(4):251-261. https://doi.org/10.1111/bioe.12101 [ Links ]
18. Harsanyi JC. Can the maximin principle serve as a basis for morality? A critique of John Rawls's theory. American Political Science Review. 1975;69(2):594-606. https://doi.org/10.2307/1959090 [ Links ]
19. Savulescu J, Cameron J, Wilkinson D. Equality or utility? Ethics and law of rationing ventilators. British Journal of Anaesthesia.2020;125(1):10-5. https://doi.org/10.1016/j.bja.2020.04.011 [ Links ]
20. Ashcroft RE. Quality of life as the basis of health care resource allocation: a philosopher's perspective on QALYs. AMA Journal of Ethics.2005; 7(2):195-9 [ Links ]
21. Wong DA. Rationing treatments based on their cost per QALY AMA Journal of Ethics.2011;13(3):220-3 [ Links ]
 Correspondence:
Correspondence:
D Pagollang Motloba
Email: pagollang.motloba@smu.ac.za


{kind=link}