










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Dental Journal
versão On-line ISSN 0375-1562
versão impressa ISSN 0011-8516
S. Afr. dent. j. vol.78 no.8 Johannesburg Set. 2023
REVIEW
A simplified and evidence-informed approach to designing removable partial dentures - Part 1: Evidence-informed design principles
CP Owen
Professor Emeritus, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
SUMMARY
For many decades the literature has regularly reported that there is a discrepancy between what is taught in dental school and what is practised, especially in the field of removable partial dentures. Not only that, but for more than 60 years reports from around the world have shown that, usually, the majority of clinicians abdicate their responsibility to design a removable partial denture (RPD) and instead leave this to the dental technician, who has no knowledge of the clinical condition of the patient and works only from a cast. Most patients around the world who require RPDs to improve aesthetics and chewing can only afford a removable prosthesis simply because the majority are poor. But RPDs can improve these aspects and contribute to an improved quality of life.
The purpose of this series of articles is to derive the basic, evidence-informed principles of partial denture design and to suggest a simplified explanation and application of those principles in the hope that clinicians will increasingly take responsibility for the design of partial dentures. Part 1 summarises studies revealing what can only be described as the malpractice of abdication of responsibility for design by clinicians, and then explain the evidence-informed basic principles of design; Part 2 will look at the biomechanical basis of those principles in terms of support; Part 3 will do the same for the biomechanical basis of retention; Part 4 will provide a simple seven-step approach to design, applied to an example of an acrylic resin-based and a metal framework-based denture for the same partially edentulous arch; and Part 5 will provide examples of designs for RPDs that have been successfully worn by patients, for each of the Kennedy Classifications of partially dentate arches. Much of this is referenced from an electronic book on the Fundamental of removable partial dentures.1
Keywords: Removable partial denture, design, support, retention, acrylic-based, framework-based
INTRODUCTION TO PART 1
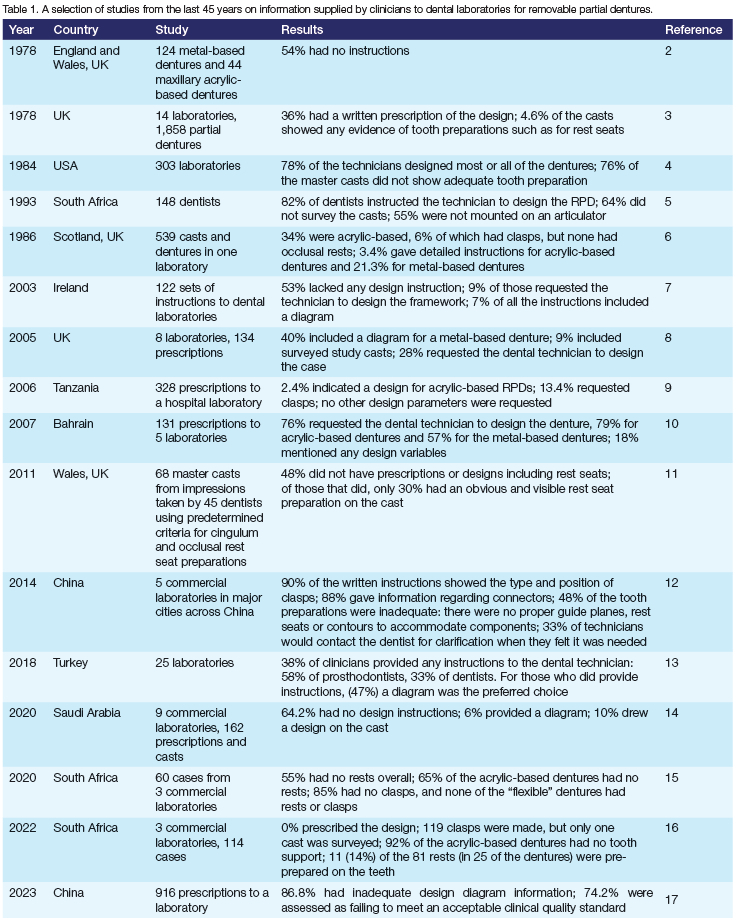
As stated in the summary, many papers have reported on the lack of information prescribed by dentists to the dental technician. Rather than setting these out in narrative form, studies from the last 45 years are summarised in Table 1. The inevitable conclusion from these studies is that little has changed over the last many decades, where there still seems to be an enormous amount of what can only be described as malpractice when clinicians abdicate their responsibility for the design of removable partial dentures. This is the motivation for this series of papers, to try to simplify both the understanding and the application of design principles.
THE DESIGN PRINCIPLES
An article that discussed key turning points in RPD philosophy revealed that RPDs have been described in the literature for just over 300 years.18 However, there seems to have been few changes over the last nearly 100 years. While there are no universally accepted principles for the design of RPDs, these can in fact be derived from evidence in the literature.
Tooth support
Early attempts to provide retention were described in the early 19th century as metal bands encircling the teeth. These often extended into the gingival sulcus with somewhat disastrous effects on the periodontium. A fortuitous effect of this was the realisation that tooth support was required, and the first occlusal rest was described in 1817.19 This prevented components such as the bands sinking into the gingiva and mucosa and should have become a universally accepted principle. Sadly, there is much evidence that RPDs are still being made, more than 200 years later, with no tooth support (see Table 1), most notably as acrylic resin-based dentures or, more recently, as the so-called flexible denture.16,20,21
In a study comparing dentures with and without tooth support, it was found that patients who had adequate and sufficient rest seats were more satisfied with their dentures than those whose dentures had inadequate support.22 Adequate support was one of the few criteria that correlated with successful wearing of mandibular Kennedy Class I RPDs.23
Clasps
A century after the concept of a clasp as a band, Roach pioneered the use of wrought wire as a circumferential clasp and as an "infra-bulge" clasp.24 Clasps provide retention by the force exerted against the tooth as they flex while emerging from the undercut below the bulge of the tooth. However, the amount of this force and the ability of all clasp materials to bend many times without distortion has not been fully elucidated. A recent paper has provided some guidelines for cast clasps and stainless steel round wire25 but there are still other casting alloys and pre-formed wrought wire clasps that need to be tested. Pre-formed and cast gingivally-approaching clasps were shown almost 40 years ago to be potentially more damaging to gingival health than circumferential clasps26 so their use will not be advocated here.
Guide planes and guiding surfaces
A guide plane is the prepared surface of a tooth adjacent to to an edentulous space, and a guiding surface is that part of the denture which contacts the guide plane. Close contact of these provides for frictional resistance when the denture moves. It is important to realise that this resistance is least along the path of insertion, and greatest if the denture is removed along any other path, rather like a drawer in a desk. This is a much underestimated contributor to retention, and when the remaining teeth are sufficiently distributed can provide all the retention needed without the use of clasps.27
These three basic design principles govern the features that should be considered for all RPDs. There are, of course, other factors that contribute to the successful use of RPDs. These include minimal gingival coverage wherever possible, and the elimination of redundant components without compromising biomechanical requirements.28,29
THE BIOLOGICAL PRICE OF RPDS
For too long, the observation of increased tooth loss following the wearing of RPDs was attributed to the forces placed on the abutment teeth, as the teeth usually carrying the clasps. This wasn't helped by the theoretical studies of Kratochvil as far back as 1963 in which he surmised that a distal extension base produced a tipping force on the abutment tooth, and advocated an RPI clasp (mesial rest, proximal plate and I-bar) to offset this.30 This was based on the difference between compression of the mucosa under the distal extension and the compression of the periodontal ligament of the abutment tooth. It seemed logical and was followed by purely laboratory studies using photoelastic resin to "prove" the effects that the RPI design was supposed to overcome.31 These are mentioned here because some believe it to this day, but there have never been any clinical studies to show this is indeed the case and it was refuted, also many years ago. 32
So, while it seemed logical that a partial denture gripping an abutment tooth would exert a tipping and torquing force on that tooth, this has never been shown clinically. What has been shown clinically is that abutment teeth are indeed more likely to be lost,3 but the reasons are multifactorial, not least of which is the influence of plaque. This is the severest biological price because a prosthesis provides many more surfaces for plaque to accumulate on, and this changes the ecology of the mouth, resulting in gingival and periodontal disease, root caries and stomatitis, especially in dentures without tooth support.34-38
The common conclusion of all studies is that intensive and meticulous oral hygiene should be a prerequisite for the insertion of RPDs.
DO THEY REALLY WORK?
This seems at first a strange question to ask, when so many RPDs are made all over the world. But it must be asked, because many papers have reported fairly high levels of dissatisfaction expressed by patients,39 with one retrospective study finding that 39% of the dentures were no longer used after 5 years.40 The adage that all dentures are easy to wear but not all are easy to use certainly applies to RPDs. The conclusion above has implications not only for the need to change patient behaviour but also, and importantly, for the design of the denture so that it can actually be used - and used successfully.
ARE THEY REALLY NEEDED?
This is not a strange question because, as will be shown in Part 4, the first step in designing an RPD is to establish the need. Not all missing teeth need to be replaced. The most common requested needs are to improve aesthetics and chewing ability. Aesthetics is an obvious one, but improving chewing ability may be vital for a number of reasons. The link between chewing ability and food choices has been established through several national surveys of large numbers relating loss of all or some teeth to adverse food choices.41 Such (wrong) food choices place patients at risk of increasing morbidity, and so it would seem logical that improving masticatory ability by replacing missing teeth would also remove those risks of morbidity. Unfortunately, this is not necessarily the case, and merely improving mastication by providing prostheses does not guarantee an improvement in food choices and therefore overall nutrition.42 The answer, therefore, is not to make such assumptions, but to provide, whenever placing a prosthesis for a patient, nutrition analysis and counselling. Unfortunately, this appears to be as rare among practitioners as is the designing of RPDs.
A somewhat still controversial additional reason for improving chewing ability is the link between the ability to chew and cognition, and especially cognitive decline and dementia. Interest in this aspect has increased in the last two decades, with the use of such instruments as functional magnetic resonance imaging and electrical brain activity recordings. A large body of literature now exists on this and it is generally accepted there is indeed an association between loss of teeth and masticatory ability and dementia. The question is, is this just an aspect of dementia in that dementia is a part or maybe a cause of loss of teeth (among other things), or is it the loss of teeth and difficulty with chewing that causes cognitive decline and dementia? The case for the latter is increasingly being made,43,44 which has the potential to make the replacement of teeth, especially in the elderly, a public health measure.
Flying somewhat in the face of these arguments is the concept of the Shortened Dental Arch. Once again there is a large body of literature on this concept, first proposed in 1981, that for a dentition with loss of posterior teeth, bilateral contact on the premolars was sufficient.45 There have been many papers testing this and, recently, some reviews of the clinical studies and while the concept remains somewhat controversial, it is generally considered to be valid, with the proviso that methodological problems with the clinical studies made it difficult to advocate for all cases.46,47 This is a fair conclusion for many aspects of prosthodontics and means that treatment must always be patient-centred. The main problem is that the lack of posterior teeth can affect food choices adversely, so perhaps a nutrition analysis should always be the first step.
There is no doubt that if a prosthesis can be omitted then it should be.
SUMMARY
It is essential that all dentists and dental technicians have a clear understanding of the evidence-informed principles of all aspects of RPD design, and especially of the biological price exacted by these dentures. Meticulous preparation of the mouth prior to treatment is required, so that dentures are placed in a plaque-free environment, and that the patient must be committed to thorough oral hygiene practice and regular recalls.
The next part will deal with the biomechanical basis of support.
Conflict of interest
None
REFERENCES
1. Owen CP. Fundamental of removable partial dentures. 5th Ed. Electronic book, available at https://www.appropriatech.com/ Accessed 5 September 2023 [ Links ]
2. Basker RM, Davenport JC. A survey of partial denture design in general dental practice. J Oral Rehabil. 1978;5(3):215-22. doi: 10.1111/j.1365-2842.1978.tb01238.x [ Links ]
3. Schwarz WD, Barsby MJ. Design of partial dentures in dental practice. J Dent. 1978;6(2):166-70. doi: 10.1016/0300-5712(78)90213-0 [ Links ]
4. Dullabh HD, Slabbert JC, Becker PJ. Partial denture prosthodontic procedures employed by practising graduates of the University of the Witwatersrand, Johannesburg. J Dent Assoc S Afr. 1993;48(3):129-34 [ Links ]
5. Owall B, Junggreen L, Yemm R. Removable partial denture production in Scotland. Quintessence Int. 1996;27(12):809-15 [ Links ]
6. Taylor TD, Matthews AC, Aquilino SA, Logan NS. Prosthodontic survey. Part I: Removable prosthodontic laboratory survey. J Prosthet Dent. 1984;52(4):598-601. doi: 10.1016/0022-3913(84)90355-x [ Links ]
7. Lynch CD, Allen PF. A survey of chrome-cobalt RPD design in Ireland. Int J Prosthodont. 2003;16(4):362-4 [ Links ]
8. Lynch CD, Allen PF. Quality of written prescriptions and master impressions for fixed and removable prosthodontics: a comparative study. Br Dent J. 2005;198(1):17-20. doi: 10.1038/sj.bdj.4811947 [ Links ]
9. Carneiro LC. Specifications provided by practitioners for fabrication of removable acrylic prostheses in Tanzania. J Oral Rehabil. 2006;33(9):660-5. doi: 10.1111/j.1365-2842.2005.01611.x [ Links ]
10. Radhi A, Lynch CD, Hannigan A. Quality of written communication and master impressions for fabrication of removable partial prostheses in the Kingdom of Bahrain. J Oral Rehabil. 2007;34(2):153-7. doi: 10.1111/j.1365-2842.2006.01685.x [ Links ]
11. Rice JA, Lynch CD, McAndrew R, Milward PJ. Tooth preparation for rest seats for cobalt-chromium removable partial dentures completed by general dental practitioners. J Oral Rehabil. 2011;38(1):72-8. doi: 10.1111/j.1365-2842.2010.02130.x [ Links ]
12. Sui L, Wu X, Wu S, Gao P, Li R. The quality of written instructions for dental prostheses in China. J Prosthodont. 2014;23(8):602-9. doi: 10.1111/jopr.12163 [ Links ]
13. Cebeci NÖ. Factors associated with insufficient removable partial denture design instructions. Dent Med Probl. 2018;55(2):173-7. doi: 10.17219/dmp/89646 [ Links ]
14. Nassani MZ, AlOtaibi MS. Quality of communicating design features for cobalt chromium removable partial dentures in Riyadh, Saudi Arabia. Eur Oral Res. 2020;54(3):123-9. doi: 10.26650/eor.20200117 [ Links ]
15. Farao W, Geerts G. Conformity of removable partial denture designs to agreed principles based on materials used - A preliminary study. SADJ. 2020;75:253-9 [ Links ]
16. Daya R, Owen CP. Conformity of removable partial denture designs from three laboratories to a set of design principles. SADJ 2022;77(8):459-64 doi: 10.17159/2519-0105/2022/v77no8a1 [ Links ]
17. Zhang N, Mao B, Dai Y, Chen S, You Z, Zhang J, Chen X, Dong H, Yue L, Yu H. Audit to assess the quality of 916 prosthetic prescriptions of removable partial dentures. Hua Xi Kou Qiang Yi Xue Za Zhi. (West China Journal of Stomatology) 2023;41(3):315-22. English, Chinese. doi: 10.7518/hxkq.2023.2021565 [ Links ]
18. Waliszewski MP. Turning points in removable partial denture philosophy. J Prosthodont. 2010;19(7):571-9. doi: 10.1111/j.1532-849X.2010.00622.x [ Links ]
19. Delabarre CF: Discours d'ouverture d'un cours de medicine dentaire. Paris, 1817, 390 pp. Not read in the original: cited by Waliszewski, 2009 [ Links ]
20. Horie N, Ouchi T, Nishiyama R, Usuda S, Morikawa S, Asoda S, Nakagawa T Vertical Displacement in Unilateral Extension Base Flexible Removable Dentures. Bull Tokyo Dent Coll. 2019;60(4):233-9. doi: 10.2209/tdcpublication.2018-0068 [ Links ]
21. Fueki K, Ohkubo C, Yatabe M, Arakawa I, Arita M, Ino S, et al. Clinical application of removable partial dentures using thermoplastic resin-part I: definition and indication of non-metal clasp dentures. J Prosthodont Res. 2014;58(1):3-10. doi: 10.1016/j.jpor.2013.12.002 [ Links ]
22. Koyama S, Sasaki K, Yokoyama M, Sasaki T, Hanawa S. Evaluation of factors affecting the continuing use and patient satisfaction with removable partial dentures over 5 years. J Prosthodont Res. 2010;54:97-101 [ Links ]
23. Frank RP, Brudvik JS, Leroux B, Milgrom P, Hawkins N. Relationship between the standards of removable partial denture construction, clinical acceptability, and patient satisfaction. J Prosthet Dent. 2000;83:521-7 [ Links ]
24. Becker CM, Kaiser DA, Goldfogel MH. Evolution of removable partial denture design. J Prosthodont. 1994;3(3):158-66. doi: 10.1111/j.1532-849x.1994.tb00147.x [ Links ]
25. Owen CP, Naidoo N. Guidelines for the choice of circumferential wrought wire and cast clasp arms for removable partial dentures. Int Dent J. 2022;72(1):58-66. doi: 10.1016/j.identj.2021.01.005 [ Links ]
26. Bazirgan MK, Bates JF. Effect of clasp design on gingival health. J Oral Rehabil. 1987;14(3):271-81. doi: 10.1111/j.1365-2842.1987.tb00719.x [ Links ]
27. Mothopi-Peri M, Owen CP. Guide-Plane Retention in Designing Removable Partial Dentures. Int J Prosthodont. 2018;31(2):145-8. doi: 10.11607/ijp.5525 [ Links ]
28. Runov J, Kroone H, Stoltze K, Maeda T, El Ghamrawy E, Brill N. Host response to two different designs of minor connector. J Oral Rehabil. 1980;7(2):147-53. doi: 10.1111/j.1365-2842.1980.tb00431.x [ Links ]
29. Chandler JA, Brudvik JS. Clinical evaluation of patients eight to nine years after placement of removable partial dentures. J Prosthet Dent. 1984;51(6):736-43. doi: 10.1016/0022-3913(84)90366-4 [ Links ]
30. Kratochvil FJ. Influence of occlusal rest position and clasp design on movement of abutment teeth. J Prosthet Dent. 1963;13(1):114-124 [ Links ]
31. Kratochvil FJ, Caputo AA. Photoelastic analysis of pressure on teeth and bone supporting removable partial dentures. J Prosthet Dent. 1974;32(1):52-61. doi: 10.1016/0022-3913(74)90098-5 [ Links ]
32. Berg E. Periodontal problems associated with use of distal extension removable partial dentures - a matter of construction? J Oral Rehabil. 1985;12(5):369-79. doi: 10.1111/j.1365-2842.1985.tb01542.x [ Links ]
33. Tada S, Ikebe K, Matsuda K, Maeda Y. Multifactorial risk assessment for survival of abutments of removable partial dentures based on practice-based longitudinal study. J Dent. 2013;41(12):1175-80. doi: 10.1016/j.jdent.2013.07.018 [ Links ]
34. Brill N, Tryde G, Stoltze K, El Ghamrawy EA. Ecologic changes in the oral cavity caused by removable partial dentures. J Prosthet Dent. 1977;38(2):138-48. doi: 10.1016/0022-3913(77)90278-5 [ Links ]
35. do Amaral BA, Barreto AO, Gomes Seabra E, Roncalli AG, da Fonte Porto Carreiro A, de Almeida EO. A clinical follow-up study of the periodontal conditions of RPD abutment and non-abutment teeth. J Oral Rehabil. 2010;37(7):545-52. doi: 10.1111/j.1365-2842.2010.02069.x [ Links ]
36. Emami E, Taraf H, de Grandmont P, Gauthier G, de Koninck L, Lamarche C, de Souza RF. The association of denture stomatitis and partial removable dental prostheses: a systematic review. Int J Prosthodont. 2012;25(2):113-9 [ Links ]
37. Hussain KA, Azzeghaibi SN, Tarakji BRSS, Sirajuddin S, Prabhu SS. Iatrogenic Damage to the Periodontium Caused by Removable Prosthodontic Treatment Procedures: An Overview. Open Dent J. 2015;9:187-9. doi: 10.2174/1874210601509010187 [ Links ]
38. Moldovan O, Rudolph H, Luthardt RG. Biological complications of removable dental prostheses in the moderately reduced dentition: a systematic literature review. Clin Oral Investig. 2018;22(7):2439-61. doi: 10.1007/s00784-018-2522-y [ Links ]
39. Frank RP, Milgrom P, Leroux BG, Hawkins NR. Treatment outcomes with mandibular removable partial dentures: a population-based study of patient satisfaction. J Prosthet Dent. 1998;80(1):36-45. doi: 10.1016/s0022-3913(98)70089-7 [ Links ]
40. Koyama S, Sasaki K, Yokoyama M, Sasaki T, Hanawa S. Evaluation of factors affecting the continuing use and patient satisfaction with Removable Partial Dentures over 5 years. J Prosthodont Res. 2010;54(2):97-101. doi: 10.1016/j.jpor.2009.11.007 [ Links ]
41. Walls AW, Steele JG. The relationship between oral health and nutrition in older people. Mech Ageing Dev. 2004;125(12):853-7. doi: 10.1016/j.mad.2004.07.011 [ Links ]
42. Wöstmann B, Michel K, Brinkert B, Melchheier-Weskott A, Rehmann P, Balkenhol M. Influence of denture improvement on the nutritional status and quality of life of geriatric patients. J Dent. 2008;36(10):816-21. doi: 10.1016/j.jdent.2008.05.017 [ Links ]
43. Ahmed SE, Mohan J, Kalaignan P, Kandasamy S, Raju R, Champakesan B. Influence of Dental Prostheses on Cognitive Functioning in Elderly Population: A Systematic Review. J Pharm Bioallied Sci. 2021;13(Suppl 1):S788-S794. doi: 10.4103/jpbs.JPBS_773_20 [ Links ]
44. Kim MS, Han DH. Does reduced chewing ability efficiency influence cognitive function? Results of a 10-year national cohort study. Medicine (Baltimore). 2022;101(25):e29270. doi: 10.1097/MD.0000000000029270 [ Links ]
45. Käyser AF. Shortened dental arches and oral function. J Oral Rehabil. 1981;8(5):457-62. doi: 10.1111/j.1365-2842.1981.tb00519.x [ Links ]
46. Khan SB, Chikte UM, Omar R. An Overview of Systematic Reviews Related to Aspects of the Shortened Dental Arch and Its Variants in Adults. Int J Prosthodont. 2017;30(4):357-66. doi: 10.11607/ijp.5287 [ Links ]
47. Funke N, Fankhauser N, Mckenna GJ, Srinivasan M. Impact of shortened dental arch therapy on nutritional status and treatment costs in older adults: A systematic review. J Dent. 2023;133:104483. doi: 10.1016/j.jdent.2023.104483 [ Links ]
 Correspondence:
Correspondence:
CP Owen
Tel: +27 83 679 2205; Email: peter.owen@wits.ac.za


{kind=link}