










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.78 n.7 Johannesburg Aug. 2023
http://dx.doi.org/10.17159/sadj.v78i07.17070
LITERATURE REVIEW
Restorative considerations in children with congenital dental anomalies
LV MkhonzaI; LM SykesII
IBChD, Dip Implantology (UWC), Dip Dent (UP), Dentist, Department of Prosthodontics, University of Pretoria, South Africa
IIBSc, BDS, MDent, IRENSA, Dip Forensic Path, Dip ESMEA, Head of Department of Prosthodontics, University of Pretoria, South Africa. ORCID: 0000-0002-2002-6238
ABSTRACT
Children with congenital dental manifestations may have to endure challenges due to their abnormal tooth development, altered skeletal growth, compromised masticatory and speech function and poor aesthetics. This may further lead to psychosocial problems. These children may have deficient ridge height and volume in edentulous areas, missing teeth, malformed or malpositioned teeth and often the added complication of xerostomia. These anomalies complicate conventional treatment and have led clinicians to consider alternative restorative treatment options. Recent literature suggests that osseointegrated implant therapy may be a viable option for children with congenital dental defects. However, studies are scarce, with no standardisation of success or survival criteria, and little long-term follow-up results. This paper explores the various restorative options and highlights the need for a multidisciplinary team approach.
INTRODUCTION
Dentofacial aesthetics may influence how individuals are treated by society. In children a deviation from the accepted dentofacial form can lead to bullying from contemporaries1. Dental anomalies may have a psychological effect on the self-esteem of children and adolescents, most notably during this early phase of psychosocial development2. Congenital defects, trauma and conditions causing oligodontia, aplasia and malocclusion can cause functional, aesthetic and psychosocial challenges for growing patients3. Tooth absence, excluding the third molars, can be divided into hypodontia, oligodontia and anodontia. Hypodontia is the absence of less than six teeth, oligodontia is the absence of six or more teeth (excluding the third molars), and anodontia is the complete absence of teeth4,5.
Conditions affecting odontogenesis can also affect the underlying alveolar bone and, in extreme cases, the maxillofacial skeleton4. Oligodontia may be treated with removable complete dentures, partial dentures, overdentures, tooth-supported fixed prostheses or implant-retained prostheses. Conventional treatment to replace missing teeth and restore function and aesthetics may pose difficulties in those cases where patients also have severely resorbed, atrophic or knife-edge alveolar ridges in the edentulous areas. It may thus be pertinent to consider implant therapy in children with congenital dental anomalies as opposed to conventional treatment modalities6.
Growth of the maxilla and mandible
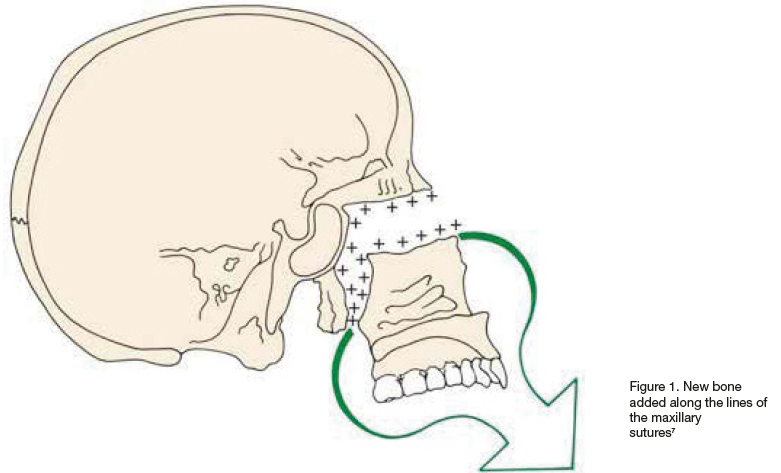
Growth in the maxilla is due to apposition of bone at the sutures that connect the maxilla to the cranium and cranial base and by surface remodelling. This growth moves the maxilla forwards and downwards relative to the cranium and cranial base, with the forward movement facilitated by the growth of the cranial base and downward movement by growth at the sutures. After the age of 7, sutural growth is solely responsible for the growth of the maxilla (Fig 1)7.
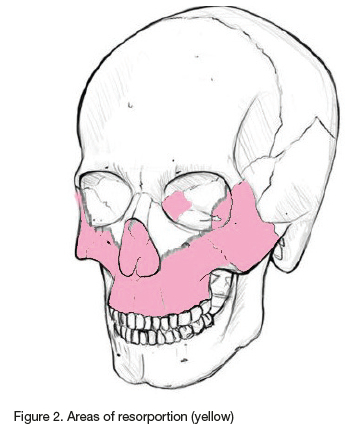
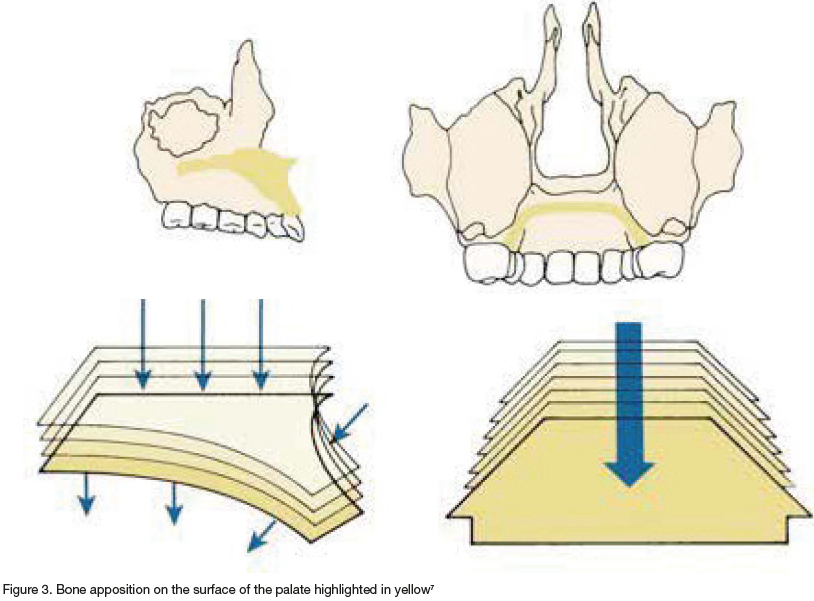
As the maxilla grows forward the anterior part simultaneously gets resorbed, as is highlighted by the yellow areas (Fig 2)8. Simultaneously, remodelling of the palate moves it downwards and widens it. This is achieved by bone removal from the floor of the nose and bone apposition on the surface of the palate (Fig 3)7.
Mandibular growth
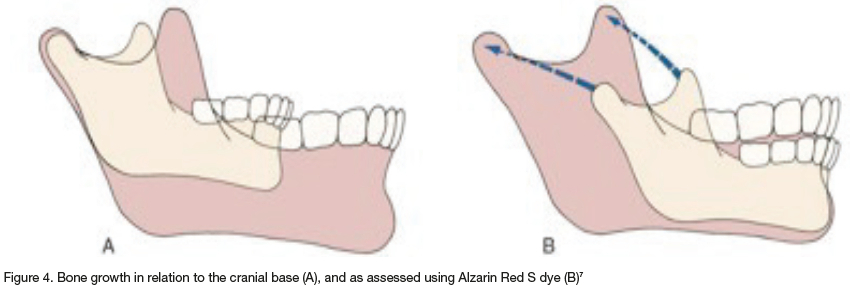
Growth of the mandible was originally described in relation to the cranial base, but has more recently been analysed using data from vital staining experiments. In the latter, 2% Alizarin Red S, a dye with a high affinity for calcium, is injected intraperitoneally or intravenously to reveal areas where there is a high calcium concentration, thus revealing where bone is being deposited and resorbed in the mandible. If the cranial base is used as a reference, then the chin appears to move downwards and forwards (Fig 4A). However, contrary to this theory, vital staining data revealed minimal changes in the body and chin area, with only the ramus, condyle and coronoid processes having substantial growth in the mandible (Fig 4B). Thus, staining suggests that the mandible grows longer by apposition of bone in the posterior part of the ramus, with simultaneous removal of large amounts of bone from the anterior ramus. Essentially the body of the mandible grows longer as the ramus moves away from the chin7. These observations are important to bear in mind if fixed restorations or implants are to be considered in children, as mandibular growth patterns will affect their final position7.
Definitions of common congenital tooth abnormalities
Anodontia - is the complete absence of tooth development8
Hypodontia - is the absence of development of less than six teeth, excluding third molars5
Oligodontia - is the absence of development of six or more teeth, excluding third molars8
Malformation - refers to any tooth form outside the normal range of size and shape. It includes macrodontia, microdontia, gemination, fusion and concrescence, among others8
Malposition - is the incorrect buccolingual or mesiodistal tooth position or angulation of a tooth8
Transposition - refers to a normal tooth erupting in an incorrect position8
Delayed eruption - is when the tooth has not emerged within a year of its normal range or when the tooth has not emerged even though 75% of the root has formed8 Impaction - refers to teeth that stop erupting before they fully emerge into the oral cavity8
Ankylosis - is where eruption stops after emergence of a tooth into the oral cavity, but only when this is due to union of the tooth cementum or dentine to the alveolar bone8
Syndromes associated with congenital dental anomalies
Odontogenesis is a complex process between the enamel epithelium, underlying mesenchyme and signalling factors (FGF, SHH, BMP and Wnt). Many factors, including physical obstruction, disruption of the dental lamina, space limitation, functional abnormalities of the dental epithelium, failure of initiation of the underlying mesenchyme and environmental influences such as trauma, infections, ionising radiation, drugs and hormonal influences may affect odontogenesis59. Any interruption in tooth development may affect the morphology, number or differentiation of teeth10,11. Neville et al (2016)8 reported on more than 50 congenital syndromes associated with oral and dental manifestations. However, Bohner et al's 2019 systematic review highlighted cleft palate, congenital aplasia, ectodermal dysplasia and non-syndrome agenesis as the most common disorders associated with congenitally missing teeth3.
Oral characteristics of oligodontia
Dentoalveolar characteristics commonly associated with oligodontia include:
1. Occlusal disturbances such as crossbite, deep bite, steep maxillary incisal inclination, abnormal attrition, narrow alveolar ridge and vertical defects9,12.
2. Loss of vertical dimension due to less growth in the maxilla compared to the mandible, leading to a class III skeletal relationship13.
3. Eruption disturbances including overeruption of teeth opposing edentulous areas, impacted Ds and Es, infraocclusion of Ds and Es, ectopic eruption, delayed eruption, rotation of teeth, multiple diastemas, severe attrition of retained primary teeth, altered tooth morphology, microdontia, conically shaped teeth and any number of other malformations9,12.
Psychological effects of tooth loss in children
Bzoch stated "the development of a child takes place within the context of interactions with others", and that "early developmental events can influence later behaviour". In children with congenital defects, their life experiences may be affected by their disorder as well as the number and types of associated disorders they must bear14. Congenital oro-facial defects can have an impact on growth and development, speech and hearing, mastication, sight and smell and aesthetics. These in turn can affect the mother-child relationship as well as the child's interactions with others. Furthermore, these children often need to attend many visits to hospitals and clinics, where they will encounter a number of strangers and undergo various procedures, which can all be frightening and stressful for them. At the same time, they miss out on normal childhood activities and schooling, which can impact their social and academic development and their oral health related quality of life (OHQoL).
OHQoL can be assessed using the Child Perceptions Questionnaires (CPQ). There is a short and a long version of this questionnaire available. Both questionnaires divide children into age categories from 8-10, 11-14, 15-17 and 18+. And both are subdivided into 4 parts that address oral symptoms, functional limitations, emotional wellbeing and social wellbeing. Each question can be answered on a 5-point Likert scale as either never (=0), once/twice (=1), sometime (=2), often (=3) and everyday/almost every day (=4). Final scores can range from 0-148 and 0-64 in the long and short questionnaires respectively. The higher scores correlate with a higher impact of conditions on OHQoL15. Liang et al (2010) compared the psychosocial impact of hypodontia with moderate to severe dental malocclusion on children. They reported that patients with moderate to severe malocclusion and those with hypodontia both had a similar psychosocial status1. Wogelius et al (2011) found an interesting observation that children with fixed orthodontic treatment had a higher CPQ value (22) than those with healthy oral conditions (9), cleft lip and palate defects (9) and those with rare dental anomalies16.
Conditions associated with hypodontia or oligodontia may negatively affect the OHQoL in young patients who may fear exposing their removable dentures to their peers, being bullied due to their differences or having a fear of dentists16. Furthermore, as children grow they become more aware of their oral health status, especially girls, who tend to have higher CPQ scores than boys15. Issues of bullying, embarrassment or shame associated with oligodontia affect the psychological and social wellbeing of children, especially in the important adolescent years.
To curb these negative aspects and emotions, treatment of these patients should aspire to improve aesthetics, promote craniofacial growth, improve the profiles, address masticatory and speech function and, to some extent, lead to better psychosocial development17. An added complication is that some conditions that affect odontogenesis may also affect the salivary gland development and function, leading to xerostomia, which has several negative repercussions on the teeth and oral environment. Edentulous areas often have narrow, sharp or deficient ridges. When this is compounded by other dental manifestations including missing teeth and xerostomia, restorative treatment becomes that much more difficult. Once again, this will impact negatively on the child's OHQoL6. In recent years, more clinicians have begun to consider using fixed tooth supported restorations or osseointegrated implant-retained prostheses in children with congenital dental defects. These options may improve self-confidence, perceived quality of life, psychosocial health and alleged social acceptability6,17. Careful consideration of the feasibility, timing of implant placement, future growth and potential restorative or implant failures should be made prior to embarking on any fixed or implant-supported prostheses in children with congenitally dental anomalies.
Treatment considerations
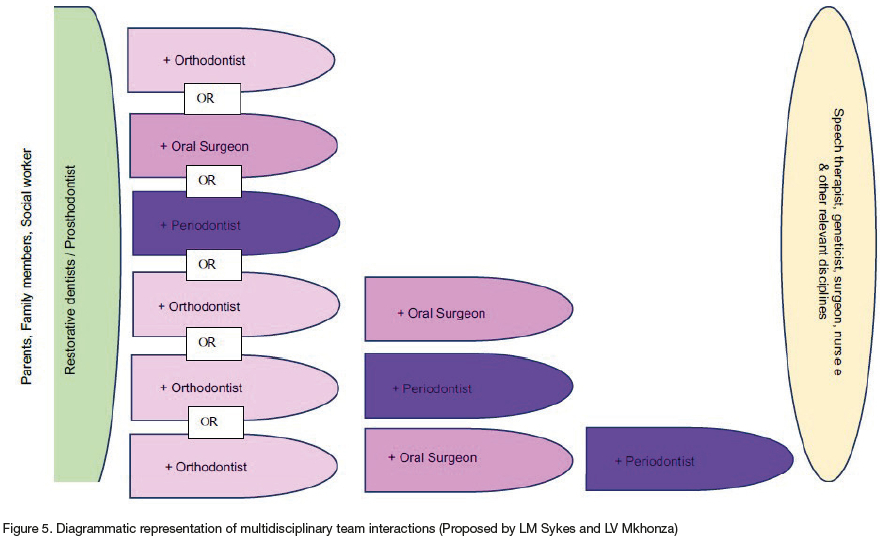
Almost all children with congenital tooth anomalies or absence will need some form of prosthodontic intervention, as well as any number of other treatment modalities. It stands to reason then that the overall management of each child should be coordinated by the treating dentist/ prosthodontist, as part of a multidisciplinary team. The objective of this team approach is to "bring the child to a point where they do not differ significantly from their peers in terms of health, education or ability to interact socially"14. Good communication between the different specialities is essential to ensure the patient gets the appropriate treatment at the correct time to achieve the best possible outcomes in terms of speech, language and hearing, facial appearance, dento-occlusal development and oral function. Each phase of treatment and treatment modality impacts on the others, and thus requires careful co-ordination. For example, in cleft palate patients if timing of surgery is not correctly planned, too early closure of the palatal defect could impede dento-occlusal development and orthognathic growth14. Similarly, dental prostheses may address aesthetics and masticatory concerns but could affect speech and articulation at a crucial time in the child's social development. Thus, all aspects of the treatment regime need to be pre-planned and integrated rather than individually administered. Figure 5 is a diagrammatic representation proposed by the authors of how the various role players may interact. The vertical pillars represent the family; the prosthodontist/restorative dentist and technician; and various crucial allied disciplines including social workers, psychologists, geneticists, speech and hearing therapists, surgeons and nurse aids. The horizontal arms illustrate key dental disciplines that may be needed individually or in combination with each other.
1. Assessment and planning phase
This stage requires cephalometric, panoramic and hand wrist radiographs as well as articulated study casts as diagnostic aids3. During this phase of treatment, the clinician should assess the age and developmental stage of the child, the anatomy of the hard and soft tissue, the number and location of missing teeth, presence of permanent successors, arch shape and the condition the child is suffering from3,18. The quality and quantity of bone available in edentulous areas should also be evaluated as some areas may need bone augmentation to help support a prosthesis or to facilitate implant placement and integration19.
Any previous or currently worn prosthesis should also be examined to visualise arch relations and facial dimensions, and to identify any shortcomings with the hopes of improving these in the future. The assessment phase also includes planning to blueprint a phased approach that will address both functional and aesthetic needs. This will entail use of above-mentioned radiographs and diagnostic wax ups on articulated study casts. These help clinicians explore the various possible treatment options and facilitate communication between patient and clinician, and between members of the treatment team9.
2. Orthodontic phase
Malocclusion, rotated teeth, tilted teeth, microdontia and multiple diastemas are a few common traits seen in patients with oligodontia. These patients may require initial active orthodontic treatment12, and often need prolonged use of retainers4. Orthodontics can help create or maintain space in the arches and correct adverse tooth relationships. Orthognathic surgery may also be needed to correct the jaw relationship6. It is imperative to remember that oral rehabilitation in growing patients must not only focus on immediate restoration of facial dimensions but must also facilitate craniofacial growth to obtain the ultimate ideal jaw relationship - if possible - as this will result in more optimal treatment in the adult patient. Jaw relationships may be improved using maxillary dentures with expansion screws to try to promote sutural growth13.
3. Surgical phase
The goal of this phase is to preserve bone and provide treatment that will benefit the patient immediately and in the future. The most crucial aspect is to try to preserve bone by retaining primary teeth for as long as possible20. This may also be achieved by autotransplantation of teeth when possible. In children this procedure can be successful if the tooth apices are still open as this allows for healing with a functional periodontium. This ligamentous attachment enables the tooth to participate in growth of the alveolar ridge and allows for orthodontic tooth movement21. While auto transplants are only successful in children and adolescents, deciduous teeth may, at times, be retained well into adulthood21. Although implants have not been widely used in children with congenitally missing teeth, Terheyden and Wüsthoff (2015) noted that implant supported prosthesis had a better outcome and higher survival rate than tooth autotransplants. Thus, the possible use of osseointegrated implant therapy warrants further debate21.
4. Prosthetic phase
This phase is important because of the dynamic oral environment, where there are many factors to consider. The first is the arch length. Bu et al (2008) found that in children with oligodontia the maxilla was on average 4.40mm shorter than its dentonormative counterpart, while the mandible was approximately 2.80mm shorter. The next factors are those of prosthesis retention, support, bone loading and follow-up treatment or maintenance. Kearns et al (1999) noted that loading of the basal bone at an early age leads to gradual resorption of the basal bone. Thus, any teeth that could viably be used to retain and support a prosthesis should be considered. Even small, malformed or malaligned teeth may be prepared for telescopic crowns and used to help support an overdenture. In the mandible, these are particularly useful to inhibit tilting of the mandibular denture and make cleaning easier than a fully fixed prosthesis17. Follow up should be every 3-6 months until growth is complete as new dentures may be needed to accommodate the growing jaw22. These appointments should monitor crown discolouration, gingival impingement, occlusal interferences and prosthesis stability16. In addition, radiographs should be taken every 2-3 years, with adjustment of restorations being made when needed, until growth is complete3,4. (Note: The same principles for overdenture abutments will apply with regard to growth, monitoring, adjustment and maintenance when osseointegrated implant retained restorations are to be considered.)
In children with ectodermal dysplasia salivary gland hypoplasia is common leading to xerostomia and difficult adaptation and retention of removable dentures6,21. Conventional treatment poses challenges due to previously mentioned absence of teeth, conical shape of existing teeth, knife-edged alveolar ridges and compounding xerostomia. This all results in poor denture retention, instability, pain on the ridges and mucosa, speech and masticatory difficulty and poor aesthetics23. In these children one may thus begin to explore the possibility of placing endosseous implants. However, Terheyden and Wüsthoff (2015) expressed caution when placing implants in children with ectodermal dysplasia, as they often have delayed development in comparison to their peers and this could lead to an unfavourable final position of the implants.
4.1. Considerations for the use of osseointegrated implants in children with congenital dental anomalies
Implant treatment in children has historically only been considered if all other options have been exhausted and have failed24,25. However, with the emergence of many new Implant systems, mini-implants and possibility of custom-made implants, this is an area of dentistry that warrants more research and deliberation. Implant treatment planning needs to consider factors such as gender and age of the patient, skeletal maturation, available supporting and retentive structures, proposed implant location and the current and future needs of the patient24. In the maxilla, growth may cause implants to develop diastema between them, to become infra-occluded, to end up in the sinus or to lose stability due to loss of buccal bone26. It has been advised that 10 years is the minimum age that implants be placed in the anterior maxilla and only after the age of 15 in girls and 17 in boys on the posterior maxilla to help avoid later growth-related implant complications3,24. In the maxilla placement of implants more coronally may help prevent infra-occlusion of implant crowns at a later stage, but could complicate the occlusal and aesthetic needs of the immediate restorations. In patients where the maxilla is unsuitable for implant placement, zygomatic implant placement may even be considered19.
In the mandible, the interforaminal region is the best site for implant placement, as there is little growth in this area after 6 years of age in the dentate mandible and after 3 years in a mandible with an edentulous interforaminal region3,17,19,24. Posterior mandibular implant placement should be avoided until completion of skeletal maturation. This is because of the unpredictable nature of the anteroposterior dimensions of the mandible24. It must also be noted that a high number of implants in children are lost in the healing phase21.
4.2. Contraindications to implant placement
Contraindications include use of implants in children with systemic conditions such as uncontrolled diabetes, vascular conditions, active chemo/radiation therapy and psychiatric disorders; those with metabolic disorders related to wound or bone healing; arches with insufficient bone height or width for implant placement; children with uncontrolled parafunctional habits (for example bruxism, lip or nail biting); uncooperative patients and those who fail to follow and maintain proper oral hygiene practices22.
4.3. Advantages of implant therapy
The main advantage is the perceived improvement in OHQoL due to implant's potential to provide more successful treatment in patients who have had difficulties with conventional treatment1,19.
4.4. Disadvantages of implants in children
In children with congenital dental anomalies the main disadvantage is that implant survival is lower in augmented areas. Vertically augmented bone is particularly susceptible to resorption, development of peri implant pockets and soft tissue recession within the first year after implant placement19. In addition, the survival rate of implants in children is lower than that reported for adults and geriatrics. Furthermore, growth in children can lead to changes in implant position as already mentioned3.
4.5. Possible implant types for use in children
Based on the available space, ridge volume and the age of commencement of treatment, different implant systems can be used. Mini implants have been used in orthodontics to help anchor and support active appliances. Their diameters range from 1.8mm to 2.7mm and were designed to be used in areas where there was limited bone22. Mini implants have a smaller surface area and roughness, and this decreases the likelihood of osseointergration and long-term survival. Their main advantage is that they may be loaded immediately if primary stability is achieved or after 6 months if not initially stable16. These implants should be large enough to provide retention and stability, but small enough to allow bone growth. Literature suggests that mini-implant supported prostheses can be functionally stable for up to 8 years16, but that they should be replaced with standard implants once bone growth is complete27. Further advantages are that due to their small diameter they are easier to insert than standard implants, are cheaper, do not need submerged healing, and can often be immediately loaded13. Some authors also believe that they could preserve alveolar bone volume and may even stimulate remodelling of bone.
Standard implants maybe used for in children if their bone volume is sufficient or if augmentation is possible. Kearns et al (1999) reported high success rates in a series of patients where a total of 36 Titanium plasma-sprayed, press-fit cylindrical implants (3I Implant Innovations) and 5 titanium screw-type implants (Nobelpharma) were placed in the maxillae and mandibles of 6 children23. Worsaae et al (2007) placed 283 Branemark (Nobel Biocare) and Astra (Astra Tech) implants in 46 children, and also showed high success rates (98%)12. Filius et al (2014) successfully placed 8 Strauman SLA implants size 10-14mm in the mandibles of children with congenital defects. All these studies seem to suggest a high survival rate for standard implants in children; however, success and survival criteria were not clearly defined and long-term follow-up results not reported on28.
Another rather unconventional type of implant to consider is the Onplant from Nobel Biocare (Fig 6)17. It has a disc-like design that can help overcome bone deficiency in the maxilla. Heuberer et al (2011) used it successfully for anchorage of an upper overdenture17. In 2019, Kamatham et al stated that there was insufficient evidence on the use of implants in children to establish any definitive guidelines29. To date there is still a paucity of literature and long-term follow-up studies reporting on the use of implants in children, most especially those with congenital dental anomalies.
Conclusion
The type and severity of congenital dental defects can influence both the psychosocial development and oral rehabilitation in children. If conventional treatment has been unsuccessful, it may be prudent to consider implant therapy. However, the timing, placement, monitoring and adjustments, and anticipated future needs must all be carefully considered and planned for by a multidisciplinary team. At present there is little literature regarding recommended implant protocols. Neither are there many long-term follow-up studies of survival and success rates, or the psychological impact and benefits that may be derived from their use. There is also very little data on failed implant treatment in children and how these could be addressed. The aim of all dental and restorative treatment in children with congenital dental manifestations should be to restore function and aesthetics and to "bring the child to a point where they do not differ significantly from their peers in terms of health, education or ability to interact socially" -Bozch 199714
REFERENCES
1. Laing E, Cunningham SJ, Jones S, Moles D, Gill D. Psychosocial impact of hypodontia in children. American journal of orthodontics and dentofacial orthopedics. 2010 Jan 1;137(1):35-41 [ Links ]
2. Clarke L, Bowyer L, Noone J, Stevens C, Yates J, Ashley M. Britain's youngest implant patients? - A Case Series of implant treatment in children with ectodermal dysplasia. Oral Surgery. 2020 Aug;13(3):245-51 [ Links ]
3. Bohner L, Hanisch M, Kleinheinz J, Jung S. Dental implants in growing patients: a systematic review. British Journal of Oral and Maxillofacial Surgery. 2019 Jun 1;57(5):397-406 [ Links ]
4. Filius MA, Vissink A, Raghoebar GM, Visser A. Implant-retained overdentures for young children with severe oligodontia: a series of four cases. Journal of Oral and Maxillofacial Surgery. 2014 Sep 1;72(9):1684-90 [ Links ]
5. Bu X, Khalaf K, Hobson RS. Dental arch dimensions in oligodontia patients. American Journal of Orthodontics and Dentofacial Orthopedics. 2008 Dec 1;134(6):768-72 [ Links ]
6. Chrcanovic BR. Dental implants in patients with ectodermal dysplasia: A systematic review. Journal of Cranio-Maxillofacial Surgery. 2018 Aug 1;46(8):1211-7 [ Links ]
7. Proffit WR, Fields HW, Sarver DM, Orthodontics C. Orthodontic treatment planning: From problem list to treatment plan [ Links ]
8. Chi AC, Neville BW, Damm DD, Allen CM. Oral and Maxillofacial Pathology-E-Book. Elsevier Health Sciences; 2017 [ Links ]
9. Tong HJ, Tahmassebi JF. Management of a child with severe hypodontia in the mixed dentition stage of development. European Archives of Paediatric Dentistry. 2014 Dec;15(6):449-54 [ Links ]
10. Matalova E, Fleischmannova J, Sharpe PT, Tucker AS. Tooth agenesis: from molecular genetics to molecular dentistry. Journal of Dental Research. 2008 Jul;87(7):617-23 [ Links ]
11. Qin H, Xu HZ, Xuan K. Clinical and genetic evaluation of a Chinese family with isolated oligodontia. Archives of Oral Biology. 2013 Sep 1;58(9):1180-6 [ Links ]
12. Worsaae N, Jensen BN, Holm B, Holsko JJ. Treatment of severe hypodontia - oligodontia - an interdisciplinary concept. International Journal of Oral and Maxillofacial Surgery. 2007 Jun 1;36(6):473-80 [ Links ]
13. Schnabl D, Grunert I, Schmuth M, Kapferer-Seebacher I. Prosthetic rehabilitation of patients with hypohidrotic ectodermal dysplasia: A systematic review. Journal of Oral Rehabilitation. 2018 Jul;45(7):555-70 [ Links ]
14. Bzoch KR, editor. Communicative disorders related to cleft lip and palate. Austin: Pro-ed; 1997 Jan [ Links ]
15. De Stefani A, Bruno G, Irlandese G, Barone M, Costa G, Gracco A. Oral health-related quality of life in children using the child perception questionnaire CPQ11-14: a review. European Archives of Paediatric Dentistry. 2019 Oct;20(5):425-30 [ Links ]
16. Michelogiannakis D, Javed F, Vastardis H. Mini-screw implant-supported pontics for the transitional management of missing permanent maxillary lateral incisors in children and adolescents: a review of currently available evidence. European Archives of Paediatric Dentistry. 2020 Jun;21(3):285-93 [ Links ]
17. Heuberer S, Dvorak G, Zauza K, Watzek G. The use of onplants and implants in children with severe oligodontia: a retrospective evaluation. Clinical oral implants research. 2012 Jul;23(7):827-31 [ Links ]
18. Aarts BE, Convens J, Bronkhorst EM, Kuijpers-Jagtman AM, Fudalej PS. Cessation of facial growth in subjects with short, average, and long facial types - Implications for the timing of implant placement. Journal of Cranio-Maxillofacial Surgery. 2015 Dec 1;43(10):2106-11 [ Links ]
19. Filius MA, Vissink A, Cune MS, Raghoebar GM, Visser A. Long-term implant performance and patients' satisfaction in oligodontia. Journal of Dentistry. 2018 Apr 1;71:18-24. [ Links ]
20. Mankani N, Chowdhary R, Patil BA, Nagaraj E, Madalli P. Osseointegrated dental implants in growing children: a literature review. Journal of Oral Implantology. 2014 Oct;40(5):627-31 [ Links ]
21. Terheyden H, Wusthoff F. Occlusal rehabilitation in patients with congenitally missing teeth - dental implants, conventional prosthetics, tooth autotransplants, and preservation of deciduous teeth - a systematic review. International Journal of Implant Dentistry. 2015 Dec;1(1):1-25 [ Links ]
22. Iyer H, Dixit UB. A review on dental implants in pediatric patients. Indian Journal of Oral Health and Research. 2021 Jul 1;7(2):55 [ Links ]
23. Kearns G, Sharma A, Perrott D, Schmidt B, Kaban L, Vargervik K. Placement of endosseous implants in children and adolescents with hereditary ectodermal dysplasia. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 1999 Jul 1;88(1):5-10 [ Links ]
24. Mishra SK, Chowdhary N, Chowdhary R. Dental implants in growing children. Journal of Indian Society of Pedodontics and Preventive Dentistry. 2013 Jan 1;31(1):3 [ Links ]
25. Percinoto C, de Mello Vieira AE, Megid Barbieri C, LemosMehlado F, Silva Moreira K. Use of dental implants in children: a literature review. Quintessence International. 2001 May 1;32(5) [ Links ]
26. Agarwal N, Kumar D, Anand A, Bahetwar SK. Dental implants in children: A multidisciplinary perspective for long-term success. National journal of maxillofacial surgery. 2016 Jul;7(2):122 [ Links ]
27. Pomini MC, Samra AP, Fischborn AR, Junior VA, Alves FB. The use of mini-implants for provisional prosthetic rehabilitation in growing patients: A critical review. Journal of Prosthodontic Research. 2021:JPOR_2019_338 [ Links ]
28. Filius MA, Cune MS, Raghoebar GM, Vissink A, Visser A. Prosthetic treatment outcome in patients with severe hypodontia: a systematic review. Journal of Oral Rehabilitation. 2016 May;43(5):373-87 [ Links ]
29. Kamatham R, Avisa P, Vinnakota DN, Nuvvula S. Adverse effects of implants in children and adolescents: A systematic review. Journal of Clinical Pediatric Dentistry. 2019;43(2):69-77 [ Links ]
 Correspondence:
Correspondence:
Prof LM Sykes
Email: Leanne.sykes@up.ac.za
Author's contribution
1. L Mkhonza 50%
2. LM Sykes 50%


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}