










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.78 n.6 Johannesburg Jul. 2023
http://dx.doi.org/10.17159/sadj.v78i06.16948
RESEARCH
Pulpotomy: An alternative treatment modality to conventional root canal treatment
G StreitI; M VorsterII; PJ van der VyverIII
IBChD [Pret], MSc [Dent] (UWC), PG Dip Aesthetics (Pret), PDD Interceptive Orthodontics (UWC), PG Dip Practice Management (Pret), PG Dip Paedodontics (Pret), PG Dip Prosthodontics (Pret) , PG Dip Endodontics (Pret) ORCID: 0000-0003-2251-7169
IIBChD, PG Dip Dent (Endo), MSc (Pret), PhD (Pret) ORCID: 0000-0003-4470-1530
IIIBChD, PG Dip Dent (Endo), PG Dip Dent (Aesthet Dent), MSc, PhD (Pret) ORCID: 0000-0003-1951-6042
ABSTRACT
INTRODUCTION: Vital pulp therapy is considered a successful treatment modality in primary and immature permanent teeth. The development of bioactive material has led to vital pulp therapy and pulpotomy treatment becoming a popular treatment modality in permanent teeth. This literature review investigates pulpotomy procedures on permanent teeth as a viable option, as opposed to conventional root canal treatment, as presented in the case report included
AIM: The aim of this study is to evaluate literature on the reported success of pulpotomy treatment in mature permanent teeth. For this reason, the study specifically reviewed literature detailing the use of pulpotomies including the materials required for the procedure
METHOD: The literature review is focused on studies using MTA and bioactive alternatives as pulpotomy material. An electronic search was done on EBSCOhost to source 58 articles published from 1979 to 2022
RESULTS: Literature investigated reports that pulpotomy treatment with bioactive materials shows promising results and therefore the possibility exists of it being a suitable treatment option or alternative to conventional root canal treatment
Keywords: Apexification, dental pulp, root canal therapy, partial pulpotomy, vital pulp therapy.
INTRODUCTION
Vital pulp therapy (VPT), as a possible therapeutic intervention in the treatment of both primary and permanent teeth, is well documented.1,2 The long-term health of the dental pulp is reliant on the correct diagnosis and subsequent treatment.3 VPT is a viable treatment option in permanent teeth with normal/healthy pulps or pulpitis (for example: apexogenesis, indirect pulp capping, direct pulp capping, partial pulpotomy and complete pulpotomy).2 The standard treatment options in permanent teeth with irreversible pulpitis or necrotic pulp are regenerative endodontics, conventional root canal treatment and apexification.4,5 It is advised that clinicians familiarise themselves with these pulp therapies, taking into consideration the restorability of the tooth as well as alternative VPT treatment therapies.5
The American Academy of Paediatric Dentistry (AAPD) guidelines define when pulpotomy procedures can be performed: "A pulpotomy is performed in a tooth with extensive caries without evidence of radicular pathology when caries removal results in a carious or mechanical pulp exposure."6
Pulpotomy treatment is indicated in primary teeth with exposed vital pulps or reversible coronal pulpitis. Pulpotomies can also be considered in immature permanent teeth with pulpal exposure due to caries or trauma. This can also be performed as an emergency procedure in permanent mature teeth until such time as root canal treatment can be performed.7 Coronal pulpotomy in comparison to conventional RCT procedures are less costly and not considered as technically demanding and time consuming.
VPT aims to maintain tooth functionality and vitality.8 In the past, VPT has predominantly been used in primary and immature permanent teeth; however, with the development of bioactive materials, the use of these materials in permanent teeth with mature root apices is gaining popularity. Performing a coronal pulpotomy on permanent teeth, which implies the amputation of pulp tissue down to the cervical line with bioactive material, has been suggested as an alternative to a traditional RCT.9
According to the AAPD guidelines, a partial pulpotomy is the treatment of choice following traumatic or carious pulp exposure in immature permanent teeth, whereas coronal pulpotomy is the treatment of choice in immature teeth with pulpal inflammation. The primary objective of performing a pulpotomy is to preserve radicular pulpal tissues that may help to complete apexogenesis in immature permanent teeth.7
Coronal pulpotomy differs from partial pulpotomies whereby only partial removal of coronal pulp is performed. A pulpotomy procedure is performed when the coronal pulp is either inflamed and/or infected and subsequently amputated.10 The remaining radicular dental pulp is then covered with the appropriate material to protect the pulp from further injury and to facilitate healing.7,11
Clinical decision-making and correct diagnosis in considering coronal pulpotomy treatment as an alternative treatment modality over conventional RCT in mature permanent teeth with irreversible pulpitis is paramount.9
Review of literature
Conventional RCT, indicated in permanent mature teeth with pulpal and periradicular diseases, consists of the complete removal of pulp tissue from the root canals of the tooth, the disinfection of canals and final restoration/prosthesis. Root canal treatments are considered to have high overall success rates estimated at 86.02%.12 Results of 86% at 2-3 years, 93% at 4-5 years and 87% at 8-10 years survival rates of endodontically treated teeth have been reported.13 However, considerable loss of tooth structure is one of the negative outcomes of performing RCT. The most common denominator in the failure after root canal treatment is tooth fracture and loss due to compromised remaining tooth structure.8,14,15 Coronal pulpotomy treatment is a more conservative therapy and aids in preserving tooth structure in a minimally invasive manner.9 Pulpotomy treatments are also less technically challenging and demanding than standard root canal treatments.7
Various studies have reported high rates of poor quality of obturation (25-62%) and apical periodontitis (45%) associated with root filled teeth.16,17,18 Healthy pulps are still the best option to All a root canal with and it should not be assumed that just because the pulp is damaged that it will need to be removed completely.19 However, RCT in teeth with pulpal and/or peri-radicular diseases is still considered the standard care.20, 21 Unfortunately, survival rates of these teeth are significantly reduced after root canal treatment compared to vital teeth.14 Plausible causes might include the lack of a proprioceptive mechanism, loss of dental hard tissue and the loss of a damping effect.22,23
Advances in bioactive materials have recently provided an alternative treatment option in teeth with irreversibly inflamed pulps. Most bioactive materials are calcium silicate-based material (ProRoot MTA (Dentsply Sirona, Switzerland), Biodentine (Septodont, Saint-Maur-des-Fossés, France) and calcium-enriched mixture (CEM) (Yekta Zist Dandan Company, Tehran, Iran). Both these materials are biocompatible and capable of inducing cementogenesis, dentinogenesis and osteogenesis.24,25
Due to the biocompatibility and superior sealing ability, mineral trioxide aggregate (MTA) and CEM have been found to produce better success rates than calcium hydroxide.9 Dentine bridge formation and pulpal health were more predictable and successful after MTA pulpotomy treatments.26,27
Since its introduction, MTA has attracted a fair amount of attention from the endodontic field due to many of its advantages compared to traditional endodontic material. This includes its sealing ability, biocompatibility and the ability to form dentine bridges due to the induction and proliferation of pulp cells. Many studies show that MTA is the material of choice for vital pulp therapy, while other studies found no significant differences when comparing MTA to similar material.28-34 Conflicting results exist as to MTA being the material of choice for vital pulp therapy in primary and young permanent teeth.28-34
The use of bioactive material has created a new awareness of pulp regeneration and vascularisation as well as leading to many scholars focusing on alternative treatment options, for example coronal pulpotomy treatment in permanent teeth with reversible pulpitis. Several studies have shown success rates comparable to traditional RCT.35 Studies conducted on coronal pulpotomies also show success rates comparable to traditional root canal treatment in teeth with pulpal disease.36,37,38
A concern with coronal pulpotomies in permanent teeth is the uncertainty of the pulpal status before commencing treatment, as well the unpredictability and lack of long-term scientific evidence regarding success rates of treatment.39 Teeth in which full pulpotomy treatment is considered are generally nonresponsive to sensibility tests.43 The radicular pulp should therefore be considered healthy in the absence of contradicting clinical or radiographic signs. Eghbal et al.40 reported that upon histologic examination, there was no inflammation on pulpal tissue after direct placement of MTA on vital pulp tissue. Additionally, Asgary et al.41 showed similar results in their multicentre trial, comparing coronal pulpotomies using CEM, with RCT in permanent teeth with closed apices and irreversible pulpitis. No differences in success rates were reported between pulpotomies and standard RCT in either 6- or 12-month follow-ups. However, pulpotomies performed better radiographically compared to the RCT group.37 A study done by Alqaderi et al.42, which performed pulpotomies with MTA on permanent teeth in children, indicated for traditional root canal treatment, presented a success rate as high as 90%.43,44 Taha et al.43 reported success rates of 100% at one year and 92.7% success at a period of three years follow-up. Similarly, studies by Simon et al.45 as well as Taha et al.44 reported high clinical and radiographic success in their prospective study in permanent teeth with mature apices and irreversible pulpitis performed by using Biodentine during complete coronal pulpotomy.
Asgary et al.41 illustrated a case in which a molar tooth with irreversible pulpitis and condensing osteitis was treated with a coronal pulpotomy using CEM cement. The tooth was clinically asymptomatic, and complete healing of periradicular tissue had taken place at a two-year follow-up investigation. Root canal calcifications were not evident in contrast to calcifications frequently seen in clinical practice using calcium hydroxide pulpotomy.41 Asgary et al.37 compared root canal treatments with coronal pulpotomies (CEM pulpotomy) and showed no significant difference in the success rates during a five-year follow-up between these two treatment modalities. Linsuwanont et al.46 reported a clinical success rate of 87.3% in their study on MTA pulpotomy treatment in 66 carious exposed permanent teeth at a 62-months follow-up evaluation.
Alqaderi et al.42 evaluated the success rate of cervical pulpotomy treatment in mature permanent irreversibly inflamed teeth. Success rates were reported as high as 94% in year one and 92% in year two. Pulpotomies performed using Bioactive materials resulted in higher success rates than those performed using calcium hydroxide. The author of this systematic review proposed coronal pulpotomy as a viable treatment option in irreversibly inflamed permanent teeth.26
Baranwal et al.47 conducted a pulpotomy study and found contradicting results compared to the study done by Asgary41, using Biodentine instead of MTA in the treatment of human permanent molar with irreversible pulpitis. After the first year an overall success rate of 87% was reported using Biodentine. This might be due to its adequate sealing ability, compressive strength and biocompatibility. The additional calcium release of ions in Biodentine compared to MTA and calcium hydroxide-based materials was also evident in this study. When Biodentine is used as a capping material, pulp mesenchymal stem cells develop to odontoblast-like cells, due to the TGF-b1 growth factor release, resulting in tertiary dentine formation. Both partial and complete pulpotomies developed a degree of dentine bridge formation, running the risk of developing root canal calcifications which is less apparent in partial pulpotomies.
A review done by Cushley et al.48 evaluated the clinical success rate of pulpotomies in permanent teeth presenting with symptomatic irreversible pulpitis. The success rate of coronal pulpotomy was found to be 97.4% clinically and 95.4% radiographically at the 12-month follow-up.48
Li et al.49 systematically reviewed the comparison between MTA pulpotomies and calcium hydroxide pulpotomies. Pulpotomies performed using MTA revealed to have a higher clinical and radiographic success rate at one year follow-up than that of calcium hydroxide pulpotomy.
Positive outcomes at two- to three-year follow-up periods have been reported in cases of mature teeth with irreversible pulpitis treated by means of pulpotomy procedures. Defective restorations causing microleakage was reported as the main reason for coronal pulpotomy failures50. Hence, it is crucial for the success of the VPT that there is coronal restoration and satisfactory sealing with bioactive material. Regular evaluations and recalls of restorations are of great importance to ensure marginal integrity and longevity9.
In a study by Kunert et al.51 pulpotomies were performed on 273 teeth using different restorative options. The best results in terms of coronal seal were achieved by using a prosthetic crown, followed by amalgam, while the use of composite yielded poor results.51
Endodontic treatment can be complex and is influenced by various factors such as unusual canal shapes, dilacerations, unusual number of canals as well as root canal calcifications.52 It would be of great advantage to be able to practice a less expensive, and less technically demanding, alternative technique.53 Vital pulp therapy would be such an alternative, as suggested by a recent systematic review.54
The overall success of VPT in caries exposed teeth depends on the technique employed, the extend of pulp tissue inflammation and the period of observation.28 The possibility of failure of vital pulp is far less in younger patients compared to older patients opening new possibilities in endodontics, as observed by Bjorndal et al.55
Case report
An 11-year-old male patient reported with a history of irreversible pulpitis before his previous dentist removed the inflamed coronal pulp tissue from the pulp chamber on his right, maxillary first molar. The tooth was temporarily restored with a polycarboxylate restoration (Figure 1).

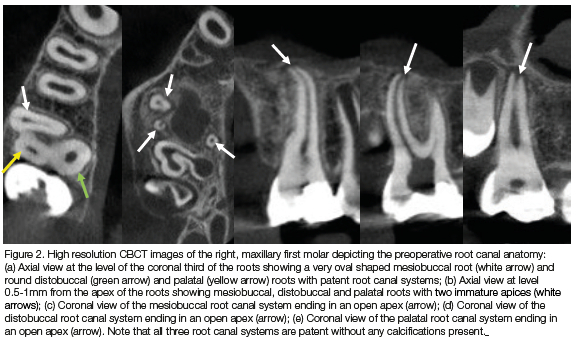
A high resolution CBCT scan revealed patent root canal systems in the mesiobuccal, distobuccal and palatal root canal systems with immature apices (Figure 2).
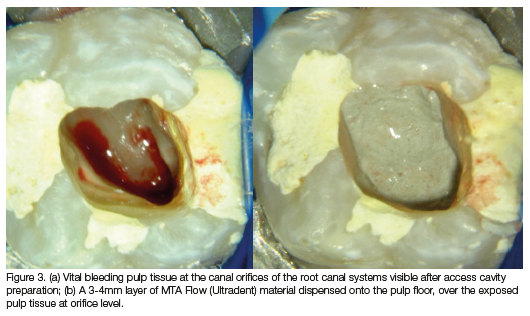
After access cavity preparation it was noted that there was vital bleeding pulp tissue at the canal orifices of the root canal systems (Figure 3a). It was decided to do partial pulpotomy using MTA. A 3.5% sodium hypochlorite solution was used to disinfect the exposed pulp tissue and to control the bleeding from the exposed pulp tissue.56-58 MTA Flow (Ultradent) was mixed and preloaded in a syringe according to the manufacturer's instructions. A 3-4mm layer of the MTA material was dispensed onto the pulp floor, over the exposed pulp tissue at orifice level (Figure 3b).
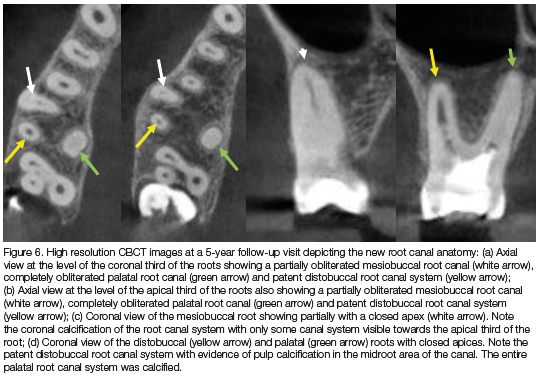
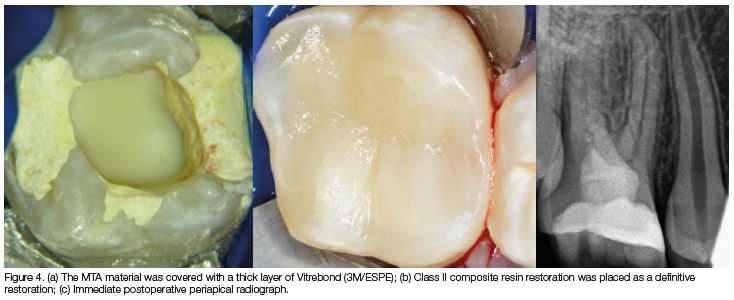
The MTA material was covered with a thick layer of Vitrebond (3M/ESPE) light-cured glass-ionomer cement (Figure 4a) before the rest of the temporary restorative material was removed. A class II composite resin restoration was placed as a definitive restoration (Figure 4b). Figure 4c shows the immediate postoperative periapical radiograph. A periapical radiograph (Figure 5) and CBCT scan (Figure 6) at a five-year follow-up revealed pulp calcification in the root canal systems with mature apices.

In conclusion, with the use of MTA and other bioactive materials such as Biodentine and CEM, pulpotomies could be a viable alternative to conventional RCT in the management of symptomatic, caries exposed, mature permanent teeth, keeping in mind careful case selection.28
Conflict of interest
The authors have no conflict of interest to declare.
REFERENCES
1. Kratunova E, Silva D. Pulp therapy for primary and immature permanent teeth: An overview. Gen Dent. 2018; 66(6):30-38 [ Links ]
2. Akhlaghi N, Khademi A. Outcomes of vital pulp therapy in permanent teeth with different medicaments based on review of the literature. Dent Res J. 2015;12(5):406-417. doi:10.4103/1735-3327.166187 [ Links ]
3. Wells C, Dulong C, McCormack S. Vital pulp therapy for endodontic treatment of mature teeth: A review of clinical effectiveness, cost-effectiveness, and guidelines (Internet). Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2019 https://www.ncbi.nlm.nih.gov/books/NBK546327/ [ Links ]
4. Lopes LB, Calvão C, Vieira FS, Neves JA, Mendes JJ, Machado V, Botelho J. Vital and nonvital pulp therapy in primary dentition: An umbrella review. J. Clin. Med. 2022; 11(1):85. doi.org/10.3390/jcm11010085 [ Links ]
5. American Academy of Pediatric Dentistry. Pulp therapy for primary and immature permanent teeth. The Reference Manual of Pediatric Dentistry. Chicago, Ill.: AAPD; 2021:399-407 [ Links ]
6. Ricucci D, Siqueira JF Jr, Li Y, Tay FR. Vital pulp therapy: histopathology and histobacteriology-based guidelines to treat teeth with deep caries and pulp exposure. J Dent. 2019; 86:41-52. doi:10.1016/j.jdent.2019.05.022 [ Links ]
7. American Association of Endodontists (AAE). Guide to clinical endodontics. 4th ed. Chicago: AAE; 2004(4) : 9 [ Links ]
8. Caliskan MK. Pulpotomy of carious vital teeth with periapical involvement. Int Endod J. 1995; 28(3):172-6 [ Links ]
9. Sadaf D. Success of coronal pulpotomy in permanent teeth with irreversible pulpitis: An evidence-based review. Cureus. 2020; 12(1):e6747. doi:10.7759/cureus.6747 [ Links ]
10. Cvek M. A clinical report on partial pulpotomy and capping with calcium hydroxide in permanent incisors with complicated crown fracture. J Endod. 1978; 4(8):232-7 [ Links ]
11. Farooq NS, Coll JA, Kuwabara A, Shelton P. Success rates of formocresol pulpotomy and indirect pulp therapy in the treatment of deep dentinal caries in primary teeth. Pediatr Dent. 2000; 22(4):278-86 [ Links ]
12. Elemam RF, Pretty I. Comparison of the success rate of endodontic treatment and implant treatment. ISRN Dent. 2011; 640509. doi:10.5402/2011/640509 [ Links ]
13. Ng YL, Mann V, Gulabivala K. Tooth survival following non-surgical root canal treatment: A systematic review of the literature. Int Endod J. 2010; 43:171-189. doi:10.1111/j.13652591.2009.01671.x [ Links ]
14. Caplan DJ, Cai J, Yin G, White BA. Root canal fille versus non-root canal filled teeth: A retrospective comparison of survival times. J Public Health Dent. 2005; 65:90-96. doi:10.1111/j.1752-7325.2005.tb02792.x [ Links ]
15. Tabassum S, Khan FR. Failure of endodontic treatment: The usual suspects. Eur J Dent. 2016; 10(1):144-147. doi:10.4103/1305-7456.175682 [ Links ]
16. Ribeiro DM, Henckel MD, Mello FW, Felippe MCS, Felippe WT. Radiographic analysis of the obturation's quality in root canal treatment performed by a South Brazilian sample of undergraduate students. RGO - Rev Gaúch Odontol. 2019; 67. doi:10.1590/1981863720190004020180038 [ Links ]
17. Sadaf D, Alsalhy H, Alrothy R, Ahmad M. Prevalence of apical periodontitis in root canal-treated teeth from an urban Saudi female population: influence of root canal fillings and coronal restorations. Int J Oral Health Sci. 2017; 7:82-85. doi:10.4103/ijohs.ijohs_46_17 [ Links ]
18. Kabak Y Abbott PV Prevalence of apical periodontitis and the quality of endodontic treatment in an adult Belarusian population. Int Endod J. 2005; 38:238-245. doi:10.1111/j.13652591.2005.00942.x [ Links ]
19. Pitt-Ford TR, Harty FJ. Harty's endodontics in clinical practice. 5th ed. Edinburgh: Wright; 2004(5): 37-49 [ Links ]
20. Kojima K, Inamoto K, Nagamatsu K et al. Hara A, Nakata K, Morita I, Nakagaki H, Nakamura H. The success rate of endodontic treatment of teeth with vital and nonvital pulps. A meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 97:95-99. doi:10.1016/j.tripleo.2003.07.006 [ Links ]
21. Ng YL, Mann V Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: a systematic review of the literature - Part 2. Influence of clinical factors. Int Endod J. 2008; 41:6-31. doi:10.1111/j.1365-2591.2007.01323.x [ Links ]
22. Randow K, Glantz PO. On cantilever loading of vital and non-vital teeth. An experimental clinical study. Acta Odontol Scand. 1986; 44:271-277. doi:10.3109/00016358609004733 [ Links ]
23. Ou KL, Chang CC, Chang WJ, Lin CT, Chang KJ, Huang HM. Effect of damping properties on fracture resistance of root-filled premolar teeth: a dynamic finite element analysis. Int Endod J. 2009; 42:694-704. doi:10.1111/j.1365-2591.2009.01570.x [ Links ]
24. Asgary S, Eghbal MJ, Ehsani S. Periradicular regeneration after endodontic surgery with calcium-enriched mixture cement in dogs. J Endod. 2010; 36:837-841. doi:10.1016/j.joen.2010.03.005 [ Links ]
25. Nosrat A, Peimani A, Asgary S. A preliminary report on the histological outcome of pulpotomy with endodontic biomaterials vs calcium hydroxide. Restore Dent Endod. 2013; 38:227-233. doi:10.5395/red.2013.38.4.227 [ Links ]
26. Qudeimat MA, Barrieshi-Nusair KM, Owais AI. Calcium hydroxide vs mineral trioxide aggregates for partial pulpotomy of permanent molars with deep caries. Eur Arch Paediatr Dent. 2007; 8(2):99-104 [ Links ]
27. American Academy of Pediatric Dentistry (AAPD). Guideline on pulp therapy for primary and immature permanent teeth; 2022:415-23 available at http://www.aapd.org/media/policies_guidelines/g_pulp.pdf [ Links ]
28. Barngkgei IH, Halboub ES, Alboni RS. Pulpotomy of symptomatic permanent teeth with carious exposure using mineral trioxide aggregate. Iran Endod J. 2013; 8(2):65-68 [ Links ]
29. Karabucak B, Li D, Lim J, Iqbal M. Vital pulp therapy with mineral trioxide aggregate. Dent Traumatol. 2005; 21(4):240-3. doi:10.1111/j.1600-9657.2005.00306.x [ Links ]
30. Nair PN, Duncan HF, Pitt Ford TR, Luder HU. Histological, ultrastructural and quantitative investigations on the response of healthy human pulps to experimental capping with mineral trioxide aggregate: a randomized controlled trial. Int Endod J. 2008; 41(2):128-50. doi:10.1111/j.1365-2591.2007.01329.x [ Links ]
31. Al-Hiyasat AS, Barrieshi-Nusair KM, Al-Omari MA. The radiographic outcomes of direct pulp-capping procedures performed by dental students: a retrospective study. J Am Dent Assoc. 2006; 137(12):1699-705 [ Links ]
32. Accorinte MLR, Holland R, Reis A, Bortoluzzi MC, Murata SS, Dezan E, Souza V, Alessandro LD. Evaluation of mineral trioxide aggregate and calcium hydroxide cement as pulp-capping agents in human teeth. J Endod. 2008; 34(1):1-6 [ Links ]
33. Qudeimat MA, Barrieshi-Nusair KM, Owais AI. Calcium hydroxide vs mineral trioxide aggregates for partial pulpotomy of permanent molars with deep caries. Eur Arch Paediatr Dent. 2007; 8(2):99-104 [ Links ]
34. Tuna D, Olmez A. Clinical long-term evaluation of MTA as a direct pulp capping material in primary teeth. Int Endod J. 2008; 41(4):273 [ Links ]
35. Solomon RV, Faizuddin U, Karunakar P, Deepthi Sarvani G, Sree Soumya S. Coronal pulpotomy technique analysis as an alternative to pulpectomy for preserving the tooth vitality, in the context of tissue regeneration: a correlated clinical study across 4 adult permanent molars. Case Rep Dent. 2015; 2015:12. doi:10.1155/2015/916060 [ Links ]
36. Asgary S, Eghbal MJ, Fazlyab M, Baghban AA, Ghoddusi J. Five-year results of vital pulp therapy in permanent molars with irreversible pulpitis: a non-inferiority multicenter randomized clinical trial. Clin Oral Investig. 2015; 19:335-341. doi:10.1007/s00784-014-1244-z [ Links ]
37. Asgary S, Eghbal MJ, Ghoddusi J. Two-year results of vital pulp therapy in permanent molars with irreversible pulpitis: An ongoing multicenter randomized clinical trial. Clin Oral Investig. 2014; 18:635-641. doi:10.1007/s00784-013-1003-6 [ Links ]
38. Taha NA, Abdelkhader SZ. Outcome of full pulpotomy using Biodentine in adult patients with symptoms indicative of irreversible pulpitis. Int Endod J. 2018; 51:819828. doi:10.1111/I.12903 [ Links ]
39. Kojima K, Inamoto K, Nagamatsu K, Hara A, Nakata K, Morita I, Nakagaki H, Nakamura H. The success rate of endodontic treatment of teeth with vital and nonvital pulps. A meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 97:95-99. doi:10.1016/j.tripleo.2003.07.006 [ Links ]
40. Eghbal MJ, Asgary S, Baglue RA, Parirokh M, Ghoddusi J. MTA pulpotomy of human permanent molars with irreversible pulpitis. Aust Endod J. 2009; 35:4-8. doi:10.1111/j.17474477.2009.00166.x [ Links ]
41. Asgary S. Calcium-enriched mixture pulpotomy of a human permanent molar with irreversible pulpitis and condensing apical periodontitis. J Conserv Dent. 2011; 14:90-93. doi:10.4103/09720707.80733 [ Links ]
42. Alqaderi HE, Al-Mutawa SA, Qudeimat MA. MTA pulpotomy as an alternative to root canal treatment in children's permanent teeth in a dental public health setting. J Dent. 2014; 42:1390-1395. doi:10.1016/j.jdent.2014.06.007 [ Links ]
43. Taha NA, Abdulkhader SZ. Full pulpotomy with biodentine in symptomatic young permanent teeth with carious exposure. J Endod. 2018; 44:932-937. doi:10.1016/j. joen.2018.03.003 [ Links ]
44 Taha NA, Ahmad MB, Ghanim A. Assessment of mineral trioxide aggregate pulpotomy in mature permanent teeth with carious exposures. Int Endod J. 2017; 50:117-125. doi:10.1111/I.12605 [ Links ]
45. Simon S, Perard M, Zanini M, Smith AJ, Charpentier E, Djole SX, Lumley PJ. Should pulp chamber pulpotomy be seen as a permanent treatment? Some preliminary thoughts. Int Endod J. 2013; 46:79-87. doi:10.1111/j.1365-2591.2012.02113.x [ Links ]
46 . Linsuwanont P, Wimonsutthikul K, Pothimoke U, Santiwong B. Treatment outcomes of mineral trioxide aggregate pulpotomy in vital permanent teeth with carious pulp exposure: the retrospective study. J Endod. 2017; 43:225-230. doi:10.1016/j.joen.2016.10.027 [ Links ]
47. Baranwal HC, Mittal N, Yadav J, Rani P, Naveen Kumar PG. Outcome of partial pulpotomy verses full pulpotomy using biodentine in vital mature permanent molar with clinical symptoms indicative of irreversible pulpitis: A randomized clinical trial. J Conserv Dent. 2022 May-Jun;25(3):317-323 [ Links ]
48. Cushley S, Duncan HF, Lappin MJ, Tomson PL, Lundy FT, Cooper P, Clarke M, El Karim IA. Pulpotomy for mature carious teeth with symptoms of irreversible pulpitis: a systematic review. J Dent. 2019; 88:103158. doi:10.1016/j.jdent.2019.06.005 [ Links ]
49. Li Y, Sui B, Dahl C, Bergeron B, Shipman P, Niu L, Chen J, Tay FR. Pulpotomy for carious pulp exposures in permanent teeth: A systematic review and meta-analysis. J Dent. 2019; 84:1-8. doi:10.1016/j.jdent.2019.03.010 [ Links ]
50. Yazdani S, Jadidfard M-P, Tahani B, Kazemian A, Dianat O, Alim Marvasti L. Health technology assessment of CEM pulpotomy in permanent molars with irreversible pulpitis. Iran Endod J. 2014; 9:23-29 [ Links ]
51. Kunert GG, Kunert IR, Da Costa Filho LC, De Figueiredo JAP. Permanent teeth pulpotomy survival analysis: retrospective follow-up. J Dent. 2015; 43:1125-1131. doi:10.1016/j.jdent.2015.06.010 [ Links ]
52. Dorn SO, Gartner AH. Case selection and treatment planning. In: Cohen S, Burns RC, editors. Pathways of the pulp. 6th ed. St. Louis: Mosby; 1994.(6) 60-76 [ Links ]
53. Asgary S, Eghbal MJ, Ghoddusi J, Yazdani S. One-year results of vital pulp therapy in permanent molars with irreversible pulpitis: an ongoing multicenter, randomized, non-inferiority clinical trial. Clin Oral Investig. 2013; 17(2):431-9 [ Links ]
54. Aguilar P, Linsuwanont P. Vital pulp therapy in vital permanent teeth with curiously exposed pulp: A systematic review. J Endod. 2011; 37(5):581-7 [ Links ]
55 Bjorndal L, Reit C, Bruun G, Markvart M, Kjaeldgaard M, Nâsrnan P, Thordrup M, Dige I, Nyvad B, Fransson H, Lager A, Ericson D, Petersson K, Olsson J, Santimano EM, Wennström A, Winkel P, Gluud C. Treatment of deep caries lesions in adults: randomized clinical trials comparing stepwise vs. direct complete excavation, and direct pulp capping vs. partial pulpotomy. Eur J Oral Sci. 2010; 118(3):290-7 [ Links ]
56. Witherspoon DE. Vital pulp therapy with new materials: new directions and treatment perspectives - permanent teeth. J Endod 2008;30(3):220-4 DOI: 10.1016/j.joen.2008.02.030 [ Links ]
57. Hafez AA, Cox CF, Tarim B, Otsuki M, Akimoto N. An in vivo evaluation of haemorrhage control using sodium hypochlorite and direct capping with a one- or two-component adhesive system in exposed nonhuman primate pulps. Quintessence Int 2002; 33: 261-272 [ Links ]
58. Bogen G, Kim JS, Bakland LK. Direct pulp capping with mineral trioxide aggregate: an observational study. J Am Dent Assoc 2008; 139: 305-315 [ Links ]
 Correspondence:
Correspondence:
Dr G Streit
Tel: +264462202
Email: coastal.dental.clinic@gmail.com


{kind=link}